Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΣΤΗΝ ΥΠΟΛΙΠΙΔΑΙΜΙΚΗ ΑΓΩΓΗ: ΠΡΟΟΠΤΙΚΕΣ-ΥΠΟΣΧΕΣΕΙΣ
ΜΩΥΣΗΣ ΕΛΙΣΑΦ ΚΑΘΗΓΗΤΗΣ ΠΑΘΟΛΟΓΙΑΣ ΙΑΤΡΙΚΗΣ ΣΧΟΛΗΣ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΙΩΑΝΝΙΝΩΝ

2
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΩΝ ΔΥΣΛΙΠΙΔΑΙΜΙΩΝ (1)
1. ΠΙΤΑΒΑΣΤΑΤΙΝΗ (1,2,4mg) ΑΠΟΤΕΛΕΣΜΑΤΙΚΗ ΣΤΑΤΙΝΗ ΑΥΞΗΣΗ ΤΗΣ ΗDL CHOL ΟΧΙ ΑΛΛΗΛΕΠΙΔΡΑΣΕΙΣ ΜΕ ΑΛΛΑ ΦΑΡΜΑΚΑ ΕΥΝΟΪΚΗ ΕΠΙΔΡΑΣΗ ΣΤΗΝ ΟΜΟΙΟΣΤΑΣΙΑ ΤΩΝ ΥΔΑΤΑΝΘΡΑΚΩΝ
 ΑΠΟΤΕΛΕΣΜΑΤΙΚΗ ΣΤΑΤΙΝΗ. ΑΥΞΗΣΗ ΤΗΣ ΗDL CHOL. ΟΧΙ ΑΛΛΗΛΕΠΙΔΡΑΣΕΙΣ ΜΕ ΑΛΛΑ ΦΑΡΜΑΚΑ. ΕΥΝΟΪΚΗ ΕΠΙΔΡΑΣΗ ΣΤΗΝ ΟΜΟΙΟΣΤΑΣΙΑ ΤΩΝ ΥΔΑΤΑΝΘΡΑΚΩΝ.")
3
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΩΝ ΔΥΣΛΙΠΙΔΑΙΜΙΩΝ (2)
2. ΕΤΟΙΜΟΣ ΣΥΝΔΥΑΣΜΟΣ ΠΡΑΒΑΣΤΑΤΙΝΗΣ (40mg) ME ΦΑΙΝΟΦΙΜΠΡΑΤΗ (160mg) [PRAVAFENIX] 3. ΕΤΟΙΜΟΣ ΣΥΝΔΥΑΣΜΟΣ ΣΙΜΒΑΣΤΑΤΙΝΗΣ (20-40mg) ΜΕ ΦΑΙΝΟΦΙΜΠΡΑΤΗ (145mg) [CHOLIB] ΣΕ ΑΣΘΕΝΕΙΣ ΥΨΗΛΟΥ ΚΙΝΔΥΝΟΥ ME ΑΘΗΡΩΓΟΝΟ ΜΙΚΤΗ ΔΥΣΛΙΠΙΔΑΙΜΙΑ ΥΠΟ ΑΓΩΓΗ ΜΕ ΣΤΑΤΙΝΗ ΠΟΥ ΕΜΦΑΝΙΖΟΥΝ TRG ή / ΚΑΙ HDL CHOL ΥΠΟΛΕΙΠΟΜΕΝΟΣ ΚΑΡΔΙΑΓΓΕΙΑΚΟΣ ΚΙΝΔΥΝΟΣ ΥΠΕΡΤΡΙΓΛΥΚΕΡΙΔΑΙΜΙΑ/ΜΕΙΩΣΗ ΤΗΣ HDL CHOL: ΣΗΜΑΝΤΙΚΟΙ ΠΑΡΑΓΟΝΤΕΣ ΚΙΝΔΥΝΟΥ ΦΑΙΝΟΦΙΜΠΡΑΤΗ ΚΑΙ ΜΕΙΩΣΗ ΤΩΝ ΜΙΚΡΟ ΚΑΙ ΜΑΚΡΟΑΓΓΕΙΑΚΩΝ ΕΠΙΠΛΟΚΩΝ ΤΟΥ ΔΙΑΒΗΤΗ
 ME ΦΑΙΝΟΦΙΜΠΡΑΤΗ (160mg) [PRAVAFENIX] 3. ΕΤΟΙΜΟΣ ΣΥΝΔΥΑΣΜΟΣ ΣΙΜΒΑΣΤΑΤΙΝΗΣ (20-40mg) ΜΕ ΦΑΙΝΟΦΙΜΠΡΑΤΗ (145mg) [CHOLIB] ΣΕ ΑΣΘΕΝΕΙΣ ΥΨΗΛΟΥ ΚΙΝΔΥΝΟΥ ME ΑΘΗΡΩΓΟΝΟ ΜΙΚΤΗ ΔΥΣΛΙΠΙΔΑΙΜΙΑ ΥΠΟ ΑΓΩΓΗ ΜΕ ΣΤΑΤΙΝΗ ΠΟΥ ΕΜΦΑΝΙΖΟΥΝ TRG ή / ΚΑΙ HDL CHOL. ΥΠΟΛΕΙΠΟΜΕΝΟΣ ΚΑΡΔΙΑΓΓΕΙΑΚΟΣ ΚΙΝΔΥΝΟΣ. ΥΠΕΡΤΡΙΓΛΥΚΕΡΙΔΑΙΜΙΑ/ΜΕΙΩΣΗ ΤΗΣ HDL CHOL: ΣΗΜΑΝΤΙΚΟΙ ΠΑΡΑΓΟΝΤΕΣ ΚΙΝΔΥΝΟΥ. ΦΑΙΝΟΦΙΜΠΡΑΤΗ ΚΑΙ ΜΕΙΩΣΗ ΤΩΝ ΜΙΚΡΟ ΚΑΙ ΜΑΚΡΟΑΓΓΕΙΑΚΩΝ ΕΠΙΠΛΟΚΩΝ ΤΟΥ ΔΙΑΒΗΤΗ.")
4
ΥΠΟΛΕΙΠΟΜΕΝΟΣ ΚΑΡΔΙΑΓΓΕΙΑΚΟΣ ΚΙΝΔΥΝΟΣ

5
Data adjusted for age, sex and trial group
Lancet 2014; 384: 626–635 Observational associations between raised concentrations of triglycerides, and CV disease and all-cause mortality, in the Copenhagen City Heart Study and Copenhagen General Population Study combined (left and middle sections) and in the Emerging Risk Factors Collaboration (right section) Data adjusted for age, sex and trial group
 and in the Emerging Risk. Factors Collaboration. (right section) Data adjusted for age, sex and trial group.")
6
Ο συνδυασμός φαινοφιμπράτης – σιμβαστατίνης αύξησε την καρδιαγγειακή προστασία σε ασθενείς με ΣΔτ2 με αυξημένα επίπεδα ΤG και χαμηλά επίπεδα HDL-C Επίδραση της θεραπείας στα κύρια ΚΑ συμβάματα σε ασθενείς με ΣΔτ2, TG ≥204 mg/dL και HDL-C ≤34 mg/dL (κύριο καταληκτικό σημείο, προκαθορισμένη υποομάδα)1 2 4 6 8 10 12 14 16 18 17,32% -31% p=0,03 12,37% Απαιτούμενος αριθμός προς θεραπεία (NNT) για 5 έτη ώστε να προληφθεί ένα καρδιαγγειακό συμβάν 20 Ποσοστό με συμβάν (%) ** NNT: number needed to treat Λόγος κινδύνου 0.69, 95% CI Σιμβαστατίνη Σιμβαστατίνη + Lipidil Ginsberg HN et al. N Engl J Med. 2010;362(17): Cholib® Summary of Product Characteristics. Abbott Laboratories, 2013. FOR INTERNAL USE ONLY
 ,32% -31% p=0,03. 12,37% Απαιτούμενος αριθμός προς θεραπεία (NNT) για 5 έτη ώστε να προληφθεί ένα καρδιαγγειακό συμβάν. 20. Ποσοστό με συμβάν (%) ** NNT: number needed to treat. Λόγος κινδύνου 0.69, 95% CI Σιμβαστατίνη. Σιμβαστατίνη + Lipidil. Ginsberg HN et al. N Engl J Med. 2010;362(17): Cholib® Summary of Product Characteristics. Abbott Laboratories, FOR INTERNAL USE ONLY.")
7
Fibrates: Benefits in atherogenic dyslipidaemia
Reduction of coronary events in atherogenic dyslipidaemia Atherogenic dyslipidaemia Others 35% 4726 Pts with atherogenic dyslipidaemia (defined by ACCORD-LIPID criteria) Sacks et al. N Engl J Med 2010;363:692
 Sacks et al. N Engl J Med 2010;363:692.")
8
Rates of progression of diabetic retinopathy (%)
ACCORD-EYE Lipid Arm Fenofibrate significantly reduced the rate of progression of diabetic retinopathy* by 40% Primary outcome 40% p=0.006 OR 0.60 95% CI ARR = 3.7% NNT = 27 Rates of progression of diabetic retinopathy (%) * 3 step or more progression on the ETDRS scale or development of diabetic retinopathy necessitating laser photocoagulation or vitrectomy 8 The ACCORD Study Group and ACCORD Eye Study Group. N Engl J Med June 29, epub.
 * 3 step or more progression on the ETDRS scale or development of diabetic retinopathy necessitating laser photocoagulation or vitrectomy. 8. The ACCORD Study Group and ACCORD Eye Study Group. N Engl J Med June 29, epub.")
9
Αλγόριθμος φαρμακευτικής θεραπευτικής προσέγγισης ασθενών με δυσλιπιδαιμία
ΔΥΣΛΙΠΙΔΑΙΜΙΑ* ΣΤΑΤΙΝΗ** ΜΗ ΕΠΙΤΕΥΞΗ ΣΤΟΧΟΥ ΓΙΑ ΤΗΝ LDL CHOL ΕΠΙΤΕΥΞΗ ΣΤΟΧΟΥ ΓΙΑ ΤΗΝ LDL CHOL ΤΙΤΛΟΠΟΙΗΣΗ ΤΗΣ ΔΟΣΗΣ ΤΗΣ ΣΤΑΤΙΝΗΣ*** ΦΥΣΙΟΛΟΓΙΚΑ ΤΡΙΓΛΥΚΕΡΙΔΙΑ ΚΑΙ HDL CHOL CHOL ΥΨΗΛΑ ΤΡΙΓΛΥΚΕΡΙΔΙΑ ΚΑΙ ΧΑΜΗΛΗ HDL CHOL Hellenic Journal of Atherosclerosis 2014;5(3): ΜΗ ΕΠΙΤΕΥΞΗ ΣΤΟΧΟΥ ΓΙΑ ΤΗΝ LDL CHOL ΣΤΑΤΙΝΗ + ΦΑΙΝΟΦΙΜΠΡΑΤΗ ΣΤΑΤΙΝΗ + ω-3 ΛΙΠΑΡΑ ΟΞΕΑ ΣΤΑΤΙΝΗ + ΕΖΕΤΙΜΙΜΠΗ ΣΤΑΤΙΝΗ + ΚΟΛΕΣΕΒΕΛΑΜΗ ΕΠΙΤΕΥΞΗ ΣΤΟΧΟΥ ΓΙΑ ΤΗΝ LDL CHOL, ΤΑ ΤΡΙΓΛΥΚΕΡΙΔΙΑ ΚΑΙ ΤΗΝ HDL CHOL ΜΕΓΙΣΤΟ ΚΑΡΔΙΑΓΓΕΙΑΚΟ ΟΦΕΛΟΣ *Αν τριγλυκερίδια νηστείας >500 mg/dL συνιστάται η άμεση χορήγηση μίας φιμπράτης ή/και ω-3 λιπαρών οξέων **Για την επίτευξη του στόχου της αγωγής συνιστάται η χορήγηση μιας στατίνης σε δόση που αναμένεται να επιτύχει το στόχο της θεραπείας ***Κάθε διπλασιασμός της δόσης μίας στατίνης οδηγεί σε 6% περαιτέρω ελάττωση της LDL CHOL
: ΜΗ ΕΠΙΤΕΥΞΗ ΣΤΟΧΟΥ ΓΙΑ ΤΗΝ LDL CHOL. ΣΤΑΤΙΝΗ. + ΦΑΙΝΟΦΙΜΠΡΑΤΗ. ΣΤΑΤΙΝΗ. + ω-3 ΛΙΠΑΡΑ ΟΞΕΑ. ΣΤΑΤΙΝΗ. + ΕΖΕΤΙΜΙΜΠΗ. ΣΤΑΤΙΝΗ. + ΚΟΛΕΣΕΒΕΛΑΜΗ. ΕΠΙΤΕΥΞΗ ΣΤΟΧΟΥ ΓΙΑ ΤΗΝ LDL CHOL, ΤΑ ΤΡΙΓΛΥΚΕΡΙΔΙΑ ΚΑΙ ΤΗΝ HDL CHOL. ΜΕΓΙΣΤΟ ΚΑΡΔΙΑΓΓΕΙΑΚΟ ΟΦΕΛΟΣ. *Αν τριγλυκερίδια νηστείας >500 mg/dL συνιστάται η άμεση χορήγηση μίας φιμπράτης ή/και ω-3 λιπαρών οξέων. **Για την επίτευξη του στόχου της αγωγής συνιστάται η χορήγηση μιας στατίνης σε δόση που αναμένεται να επιτύχει το στόχο της θεραπείας. ***Κάθε διπλασιασμός της δόσης μίας στατίνης οδηγεί σε 6% περαιτέρω ελάττωση της LDL CHOL.")
10
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΩΝ ΔΥΣΛΙΠΙΔΑΙΜΙΩΝ (3)
4. ΕΖΕΤΙΜΙΒΕ KAI ETOIMOI ΣΥΝΔΥΑΣΜΟΙ ΜΕ SIMVA (INEGΥ): LDL CHOL ΚΑΤΑ 44-58% ΜΕ ΑΤΟRVA (ATROZET): LDL CHOL ΚΑΤΑ 50-65% LOWER IS BETTER EVEN LOWER WITH EZETIMIBE IS EVEN BETTER H EZETIMIBE ΜΕΙΩΝΕΙ ΤΑ ΚΑΡΔΙΑΓΓΕΙΑΚΑ ΣΥΜΒΑΜΑΤΑ Η ΕΖΕΤΙΜΙΒΕ ΚΑΙ Η ΕΠΙΘΕΤΙΚΗ ΜΕΙΩΣΗ ΤΗΣ LDL CHOL (50mg/dl) ΕΙΝΑΙ ΑΣΦΑΛΗ Η ΜΕΛΕΤΗ ΙΜΡROVE-IT
: LDL CHOL ΚΑΤΑ 44-58% ΜΕ ΑΤΟRVA (ATROZET): LDL CHOL ΚΑΤΑ 50-65% LOWER IS BETTER. EVEN LOWER WITH EZETIMIBE IS EVEN BETTER. H EZETIMIBE ΜΕΙΩΝΕΙ ΤΑ ΚΑΡΔΙΑΓΓΕΙΑΚΑ ΣΥΜΒΑΜΑΤΑ. Η ΕΖΕΤΙΜΙΒΕ ΚΑΙ Η ΕΠΙΘΕΤΙΚΗ ΜΕΙΩΣΗ ΤΗΣ LDL CHOL (50mg/dl) ΕΙΝΑΙ ΑΣΦΑΛΗ. Η ΜΕΛΕΤΗ ΙΜΡROVE-IT.")
11
Patients stabilized post ACS ≤ 10 days:
Study Design Patients stabilized post ACS ≤ 10 days: LDL-C 50–125*mg/dL (or 50–100**mg/dL if prior lipid-lowering Rx) *3.2mM **2.6mM Standard Medical & Interventional Therapy N=18,144 Uptitrated to Simva 80 mg if LDL-C > 79 (adapted per FDA label 2011) Ezetimibe / Simvastatin 10 / 40 mg Simvastatin 40 mg Follow-up Visit Day 30, every 4 months 90% power to detect ~9% difference Duration: Minimum 2 ½-year follow-up (at least 5250 events) Primary Endpoint: CV death, MI, hospital admission for UA, coronary revascularization (≥ 30 days after randomization), or stroke Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12
 *3.2mM. **2.6mM. Standard Medical & Interventional Therapy. N=18,144. Uptitrated to Simva 80 mg if LDL-C > 79. (adapted per FDA label 2011) Ezetimibe / Simvastatin 10 / 40 mg. Simvastatin 40 mg. Follow-up Visit Day 30, every 4 months. 90% power to detect. ~9% difference. Duration: Minimum 2 ½-year follow-up (at least 5250 events) Primary Endpoint: CV death, MI, hospital admission for UA, coronary revascularization (≥ 30 days after randomization), or stroke. Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:")
12
LDL-C and Lipid Changes
1 Yr Mean LDL-C TC TG HDL hsCRP Simva 69.9 145.1 137.1 48.1 3.8 EZ/Simva 53.2 125.8 120.4 48.7 3.3 Δ in mg/dL -16.7 -19.3 +0.6 -0.5 Median Time avg 69.5 vs mg/dL

13
Primary Endpoint — ITT Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke HR CI (0.887, 0.988) p=0.016 Simva — 34.7% 2742 events NNT= 50 EZ/Simva — 32.7% 2572 events 7-year event rates
, or stroke. HR CI (0.887, 0.988) p= Simva — 34.7% 2742 events. NNT= 50. EZ/Simva — 32.7% 2572 events. 7-year event rates.")
14
Safety — ITT No statistically significant differences in cancer or muscle- or gallbladder-related events Simva n=9077 % EZ/Simva n=9067 p ALT and/or AST≥3x ULN 2.3 2.5 0.43 Cholecystectomy 1.5 0.96 Gallbladder-related AEs 3.5 3.1 0.10 Rhabdomyolysis* 0.2 0.1 0.37 Myopathy* 0.32 Rhabdo, myopathy, myalgia with CK elevation* 0.6 0.64 Cancer* (7-yr KM %) 10.2 0.57 * Adjudicated by Clinical Events Committee % = n/N for the trial duration
 * Adjudicated by Clinical Events Committee. % = n/N for the trial duration.")
15
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΩΝ ΔΥΣΛΙΠΙΔΑΙΜΙΩΝ (4)
5. OI ΑΝΑΣΤΟΛΕΙΣ ΤΗΣ PSCK9 ΣΕ ΣΥΝΔΥΑΣΜΟ ΜΕ ΣΤΑΤΙΝΗ Η ΕΖΕΤΙΜΙΒΕ ΣΕ ΠΟΙΟΥΣ ΑΣΘΕΝΕΙΣ;;: FH/STATIN INTOLERANCE / VERY HIGH RISK (CHD) PATIENTS WITH SEVERE HYPERCHOLESTEROLEMIA ΚΟΣΤΟΣ;;; ΜΑΚΡΟΧΡΟΝΙΑ ΑΣΦΑΛΕΙΑ;;: ΜΕΛΕΤΕΣ ΦΑΣΗΣ ΙΙΙ ΕΠΙΒΕΒΑΙΩΣΑΝ ΤΗΝ ΑΣΦΑΛΕΙΑ
 PATIENTS WITH SEVERE HYPERCHOLESTEROLEMIA. ΚΟΣΤΟΣ;;; ΜΑΚΡΟΧΡΟΝΙΑ ΑΣΦΑΛΕΙΑ;;: ΜΕΛΕΤΕΣ ΦΑΣΗΣ ΙΙΙ ΕΠΙΒΕΒΑΙΩΣΑΝ ΤΗΝ ΑΣΦΑΛΕΙΑ.")
17
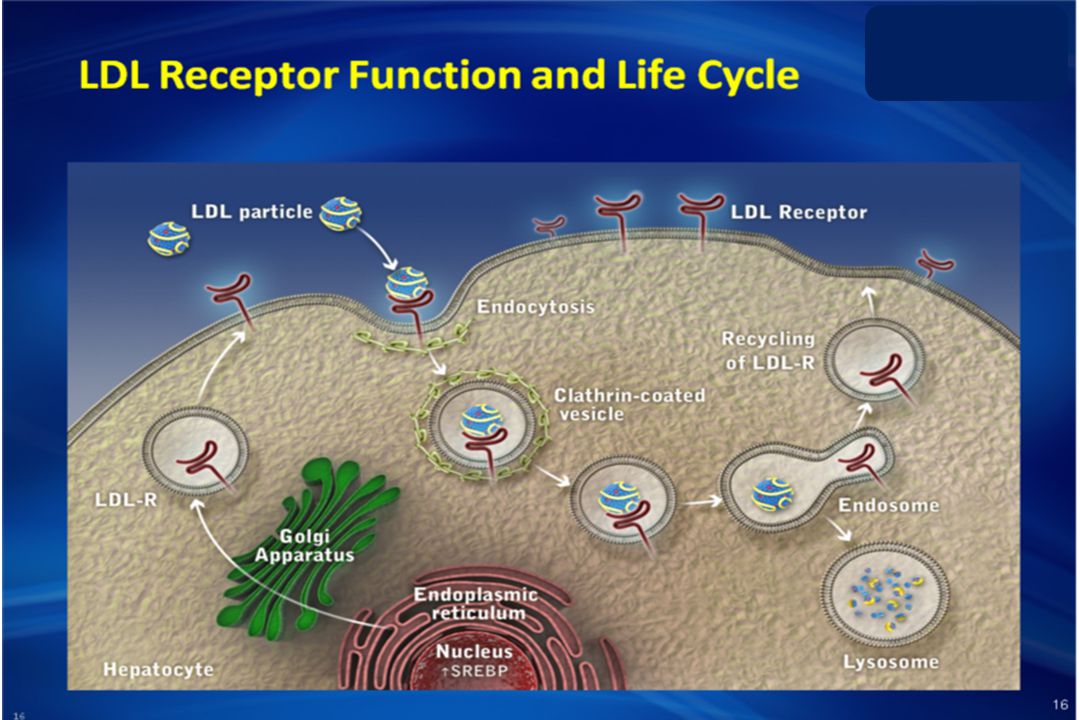
Hepatic LDLRs Play a Central Role in Cholesterol Homeostasis
Main Points: Low-density lipoprotein (LDL) particles consist mostly of cholesteryl esters packaged with a protein moiety called apolipoprotein B (apoB), with 1 apoB molecule in each LDL particle.1 LDL particles are the primary carriers of plasma cholesterol in humans, and high LDL levels have a strong and direct relationship with the development of atherosclerosis.2 The liver is responsible for the clearance and catabolism of plasma LDL, and hepatocyte expression of LDL receptors (LDLRs) are central to this process by binding and removing LDL from the plasma.1 LDL/LDLR complex is internalized into the hepatocyte via clathrin coated vesicles, thereby removing LDL from the blood.3 The affinity of the hepatic LDL receptor for apoB on LDL enables LDLRs to clear the plasma LDL effectively.1 1. Brown MS, et al. Proc Natl Acad Sci 1979;76: 2. Qian YW, et al. J Lipid Res. 2007;48: 3. Steinberg D, et al. Proc Natl Acad Sci U S A. 2009;106: References: Brown MS, Goldstein JL. Receptor-mediated endocytosis: insights from the lipoprotein receptor system. Proc Natl Acad Sci U S A ;76: Qian YW, Schmidt RJ, Zhang Y, et al. Secreted PCSK9 downregulates low density lipoprotein receptor through receptor-mediated endocytosis. J Lipid Res. 2007;48: Steinberg D, Witztum JL. Inhibition of PCSK9: a powerful weapon for achieving ideal LDL cholesterol levels. Proc Natl Acad Sci U S A ;106:
 particles consist mostly of cholesteryl esters packaged with a protein moiety called apolipoprotein B (apoB), with 1 apoB molecule in each LDL particle.1. LDL particles are the primary carriers of plasma cholesterol in humans, and high LDL levels have a strong and direct relationship with the development of atherosclerosis.2. The liver is responsible for the clearance and catabolism of plasma LDL, and hepatocyte expression of LDL receptors (LDLRs) are central to this process by binding and removing LDL from the plasma.1. LDL/LDLR complex is internalized into the hepatocyte via clathrin coated vesicles, thereby removing LDL from the blood.3 The affinity of the hepatic LDL receptor for apoB on LDL enables LDLRs to clear the plasma LDL effectively Brown MS, et al. Proc Natl Acad Sci 1979;76: Qian YW, et al. J Lipid Res. 2007;48: Steinberg D, et al. Proc Natl Acad Sci U S A. 2009;106: References: Brown MS, Goldstein JL. Receptor-mediated endocytosis: insights from the lipoprotein receptor system. Proc Natl Acad Sci U S A. 1979;76: Qian YW, Schmidt RJ, Zhang Y, et al. Secreted PCSK9 downregulates low density lipoprotein receptor through receptor-mediated endocytosis. J Lipid Res. 2007;48: Steinberg D, Witztum JL. Inhibition of PCSK9: a powerful weapon for achieving ideal LDL cholesterol levels. Proc Natl Acad Sci U S A. 2009;106:")
19
Recycling of LDLRs Enables Efficient Clearance of LDL-C Particles
Main Points: Clathrin-coated vesicles containing internalized LDL/LDLR complexes fuse with endosomes, resulting in dissociation of the LDLs from LDLRs due to the acidic environment.1 The free LDLRs then recycle back to the surface of the hepatocyte to bind and clear additional LDL from the blood.1 Free LDL particles in the endosomes are transported to the lysosomes and degraded into lipids and amino acids.1 The ability of hepatic LDLRs to be recycled is a key determinant of hepatic efficacy in lowering plasma LDL.1 1. Brown MS, et al. Proc Natl Acad Sci U S A. 1979;76: 2. Steinberg D, et al. Proc Natl Acad Sci U S A. 2009;106: 3. Goldstein JL, et al. Arterioscler Thromb Vasc Biol. 2009;29: Reference: Goldstein JL, Brown MS. The LDL Receptor. Arterioscler Thromb Vasc Biol. 2009;29:

20
PCSK9 Ένζυμο που συνδέεται με τους LDL υποδοχείς και αυξάνει την αποδόμηση τους Γλυκοπρωτεϊνη (692 αμινοξέα) που ανήκει στην οικογένεια των πρωτεασών της σερίνης που ονομάζονται proprotein convertase (PC) Το γονίδιο που κωδικοποιεί την πρωτεΐνη βρίσκεται στο χρωμόσωμα 1 (1P32) Εκφράζεται σε πολλά όργανα-κυρίως όμως στο ήπαρ
 που ανήκει στην οικογένεια των πρωτεασών της σερίνης που ονομάζονται proprotein convertase (PC) Το γονίδιο που κωδικοποιεί την πρωτεΐνη βρίσκεται στο χρωμόσωμα 1 (1P32) Εκφράζεται σε πολλά όργανα-κυρίως όμως στο ήπαρ.")
21
Αποδόμηση στα λυσοσώματα Σύνδεση με τους LDL υποδοχείς
PCSK9 Σύμπλοκο PCSK9 / LDLR Αποδόμηση στα λυσοσώματα LDL-R LDL CHOL Σύνδεση με τους LDL υποδοχείς

23
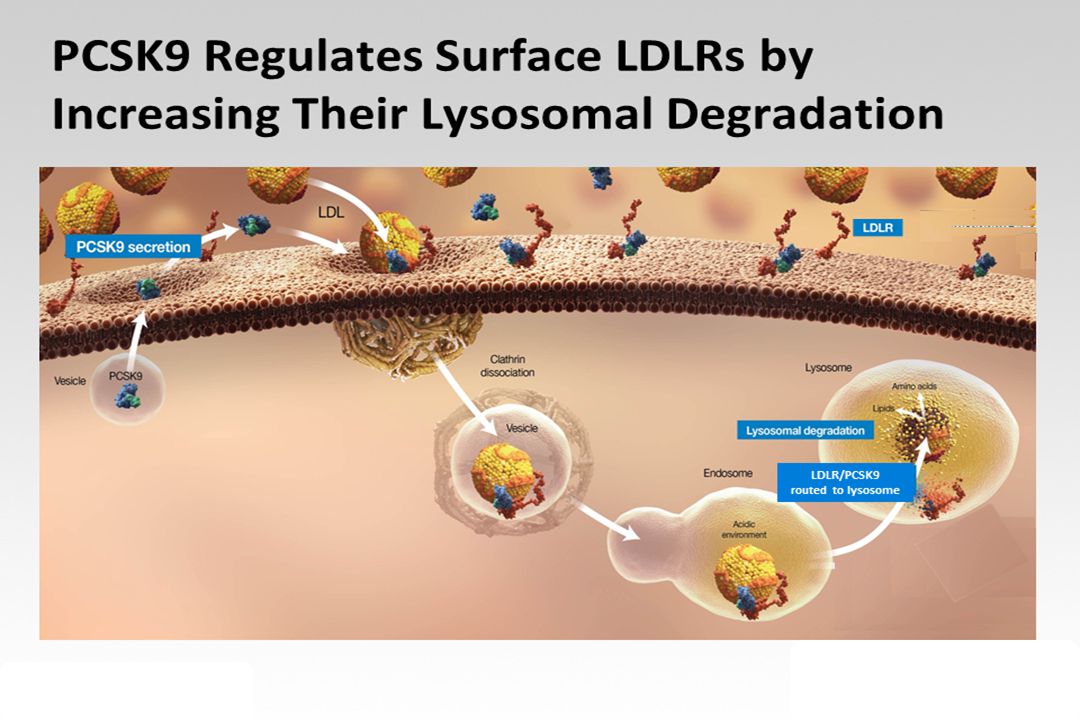
PCSK9 Regulates the Surface Expression of LDLRs by Targeting for Lysosomal Degradation
Main Points: Proprotein convertase subtilisin-like/kexin type 9, or PCSK9, is a proprotein that is produced in hepatocytes, and secreted into the plasma as functional PCSK9.1 Extracellular PCSK9 binds to the LDLR on the surface of the hepatocyte and is internalized within the endosome.2 The LDLR/PCSK9 complex is then routed to the lysosome for degradation, thereby preventing the recycling of LDLR back to the hepatocyte surface. 2 By preventing LDLRs from recycling back to the surface, PCSK9 reduces the concentration of LDLRs on the surface of hepatocytes, resulting in a lower LDL clearance rate and elevated levels of plasma LDL.3 References: Horton JD, Cohen JC, Hobbs HH. PCSK9: a convertase that coordinates LDL catabolism. J Lipid Res. 2009;50(suppl):S172- S177. Zhang DW, Lagace TA, Garuti R, et al. Binding of proprotein convertase subtilisin/kexin type 9 to epidermal growth factor-like repeat A of low density lipoprotein receptor decreases receptor recycling and increases degradation. J Biol Chem ;282: Qian YW, Schmidt RJ, Zhang Y, et al. Secreted PCSK9 downregulates low density lipoprotein receptor through receptor- mediated endocytosis. J Lipid Res. 2007;48: 1. Qian YW, et al. J Lipid Res. 2007;48: 2. Horton JD, et al. J Lipid Res. 2009;50:S172-S177. 3. Zhang DW, et al. J Biol Chem. 2007;282:
:S172- S177. Zhang DW, Lagace TA, Garuti R, et al. Binding of proprotein convertase subtilisin/kexin type 9 to epidermal growth factor-like repeat A of low density lipoprotein receptor decreases receptor recycling and increases degradation. J Biol Chem. 2007;282: Qian YW, Schmidt RJ, Zhang Y, et al. Secreted PCSK9 downregulates low density lipoprotein receptor through receptor- mediated endocytosis. J Lipid Res. 2007;48: Qian YW, et al. J Lipid Res. 2007;48: Horton JD, et al. J Lipid Res. 2009;50:S172-S Zhang DW, et al. J Biol Chem. 2007;282:")
24
Genetic Variants of PCSK9 Demonstrate Its Importance in Regulating LDL Levels
Main Points: The role of PCSK9 in the regulation of plasma LDL levels is supported by a significant amount of genetic evidence. Gain-of-function mutations in PCSK9 result in increased PCSK9 function, which leads to decreased LDLR recycling to the cell surface. 1 This results in an autosomal-dominant hypercholesterolemia with increased plasma LDL levels and increased risk of developing coronary heart disease.1 Mutations in the human PCSK9 gene that lead to a loss of PCSK9 function are found in 1% to 3% of the population. These loss-of-function mutations have been associated with lower levels of circulating PCSK9, lower plasma LDL levels, and a lower incidence of coronary heart disease events, suggesting that inhibiting the interaction between PCSK9 and LDLRs may lower plasma LDL levels.2-4 PCSK9 Gain of Function = Less LDLRs PCSK9 Loss of Function = More LDLRs References: Abifadel M et al. Mutations and Polymorphisms in the Proprotein Convertase Subtilisin Kexin 9 (PCSK9) Gene in Cholesterol Metabolism and Disease. Human Mutation. 2009;30;4:520-9. Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006;354: Lakoski S, et al “Genetic and metabolic determinants of plasma PCSK9 levels” J Clin Endocrinol Metab 94: , 2009. Cohen J, Pertsemlidis A, Kotowski IK, Graham R, Garcia CK, Hobbs HH. Low LDL cholesterol in individuals of African descent resulting from frequent nonsense mutations in PCSK9. Nat Genet 2005;37:
 Gene in Cholesterol Metabolism and Disease. Human Mutation. 2009;30;4: Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006;354: Lakoski S, et al Genetic and metabolic determinants of plasma PCSK9 levels J Clin Endocrinol Metab 94: , Cohen J, Pertsemlidis A, Kotowski IK, Graham R, Garcia CK, Hobbs HH. Low LDL cholesterol in individuals of African descent resulting from frequent nonsense mutations in PCSK9. Nat Genet 2005;37:")
25
Clinical Characteristics
Gain-of-Function Mutations in PCSK9 Cause Autosomal-Dominant Hypercholesterolemia* (ADH) PCSK9 Variant Population Clinical Characteristics D374Y British, Norwegian families, 1 Utah family Premature CHD Tendon xanthomas Severe hypercholesterolemia S127R French, South African, Norwegian families Tendon xanthomas; CHD, early MI, stroke R215H Norwegian family Brother died at 31 from MI; strong family history of CVD Associated with: High serum LDL-C2 Premature CHD and MI2 In vitro testing in many identified mutations show decreased levels of LDLRs3 PCSK9 LDL-R LDL CHOL CHD 1. Abifadel M, et al. Hum Gen. 2009;30: 2. Horton JD, et al. J Lipid Res. 2009;50:S172-S177. 3. Cameron J, et al. Hum Mol Genet. 2006;15: *For a full list of ADH mutations, please see refer to Abifadel reference.
 PCSK9 Variant. Population. Clinical Characteristics. D374Y. British, Norwegian families, 1 Utah family. Premature CHD. Tendon xanthomas. Severe hypercholesterolemia. S127R. French, South African, Norwegian families. Tendon xanthomas; CHD, early MI, stroke. R215H. Norwegian family. Brother died at 31 from MI; strong family history of CVD. Associated with: High serum LDL-C2. Premature CHD and MI2. In vitro testing in many identified mutations show decreased levels of LDLRs3. PCSK9 LDL-R LDL CHOL CHD. 1. Abifadel M, et al. Hum Gen. 2009;30: Horton JD, et al. J Lipid Res. 2009;50:S172-S Cameron J, et al. Hum Mol Genet. 2006;15: *For a full list of ADH mutations, please see refer to Abifadel reference.")
26
Loss-of-Function Mutations in PCSK9 Are Associated With Decreased LDL-C and CHD Risk
PCSK9 Variant Population LDL-C CHD Risk R46L ARIC, DHS ↓ 15%1 ↓ 47%1 Y142X or C679X ↓ 28%-40%1,2 ↓ 88%1 CGPS ↓ 11%3 ↓ 46%3 Heterozygous LOF mutations found in 1% to 3% of population1 Associated with Lower serum LDL-C1 Lower incidence of coronary heart disease1 PCSK9 null individual identified (compound heterozygote for two inactivating mutations) No detectable circulating PCSK9 with strikingly low LDL-C (14 mg/dL)4 Healthy and fertile college graduate in apparent good health4 Inhibiting LDLR/PCSK9 interaction may lower plasma LDL-C levels5 PCSK9 LDL-R LDL CHOL CHD LOF = loss of function. 1. Cohen JC, et al. N Engl J Med. 2006;354: 2. Cohen J, et al. Nat Genet. 2005;37: 3. Benn M, et al. J Am Coll Cardiol. 2010;55: 4. Zhao et al. Am Journal of Hum Gen. 2006;79: 5. Steinberg D, et al. Proc Natl Acad Sci U S A. 2009;106:
 No detectable circulating PCSK9 with strikingly low LDL-C (14 mg/dL)4. Healthy and fertile college graduate in apparent good health4. Inhibiting LDLR/PCSK9 interaction may lower plasma LDL-C levels5. PCSK9 LDL-R LDL CHOL CHD. LOF = loss of function. 1. Cohen JC, et al. N Engl J Med. 2006;354: Cohen J, et al. Nat Genet. 2005;37: Benn M, et al. J Am Coll Cardiol. 2010;55: Zhao et al. Am Journal of Hum Gen. 2006;79: Steinberg D, et al. Proc Natl Acad Sci U S A. 2009;106:")
27
ενδοκυττάριας σύνθεσης χοληστερόλης
ΣΤΑΤΙΝΕΣ ενδοκυττάριας σύνθεσης χοληστερόλης έκφρασης της PCSK9 αποδόμησης των LDL υποδοχέων στα λυσοσώματα LDL υποδοχέων LDL CHOL δραστηριότητας των LDL υποδοχέων καταβολισμού των LDL LDL CHOL Μείωση της δυνατότητας των στατινών να μειώσουν τα επίπεδα της LDL CHOL

28
LDLR and PCSK9 Expression Are Both Upregulated When Intercellular Cholesterol Levels Are Low
Main Point: The expression of LDLRs is also affected by low hepatocyte cholesterol levels, which activate a set of transcription factors called sterol regulatory element-binding proteins (SREBPs). While SREBPs increase the uptake of LDL by increasing the overall expression of LDLRs, they also increase PCSK9 expression, resulting in increased degradation of LDLRs and limited clearance of LDL-cholesterol from the blood.1,2 References: 1. Goldstein JL, Brown MS. The LDL Receptor. Arterioscler Thromb Vasc Biol. 2009;29: 2. Dubuc G, Chamberland A, Wassef H, et al. Statins upregulate PCSK9, the gene encoding the proprotein convertase neural apoptosis-regulated convertase-1 implicated in familial hypercholesterolemia. Arterioscler Thromb Vasc Biol. 2004;24: *[SREBP] = sterol regulatory element-binding protein. 1. Goldstein JL, et al. Arterioscler Thromb Vasc Biol. 2009;29: 2. Dubuc G, et al. Arterioscler Thromb Vasc Biol. 2004;24:
. While SREBPs increase the uptake of LDL by increasing the overall expression of LDLRs, they also increase PCSK9 expression, resulting in increased degradation of LDLRs and limited clearance of LDL-cholesterol from the blood.1,2. References: 1. Goldstein JL, Brown MS. The LDL Receptor. Arterioscler Thromb Vasc Biol. 2009;29: Dubuc G, Chamberland A, Wassef H, et al. Statins upregulate PCSK9, the gene encoding the proprotein convertase neural apoptosis-regulated convertase-1 implicated in familial hypercholesterolemia. Arterioscler Thromb Vasc Biol. 2004;24: *[SREBP] = sterol regulatory element-binding protein. 1. Goldstein JL, et al. Arterioscler Thromb Vasc Biol. 2009;29: Dubuc G, et al. Arterioscler Thromb Vasc Biol. 2004;24:")
29
Οι στατίνες επιτυγχάνουν το στόχο της υπολιπιδαιμικής αγωγής σε ένα σχετικά μικρό ποσοστό ασθενών υψηλού κινδύνου (+FH) –ανάγκη χορήγησης υψηλών δόσεων –δοσοεξαρτώμενες ανεπιθύμητες ενέργειες τους
 –ανάγκη χορήγησης υψηλών δόσεων –δοσοεξαρτώμενες ανεπιθύμητες ενέργειες τους")
30
ΓΙΑ ΤΗΝ ΕΠΙΤΕΥΞΗ ΤΩΝ ΣΤΟΧΩΝ ΤΗΣ ΥΠΟΛΙΠΙΔΑΙΜΙΚΗΣ ΑΓΩΓΗΣ
Ανάγκη χορήγησης υποχοληστερολαιμικών φαρμάκων με διαφορετικό μηχανισμό δράσης

31
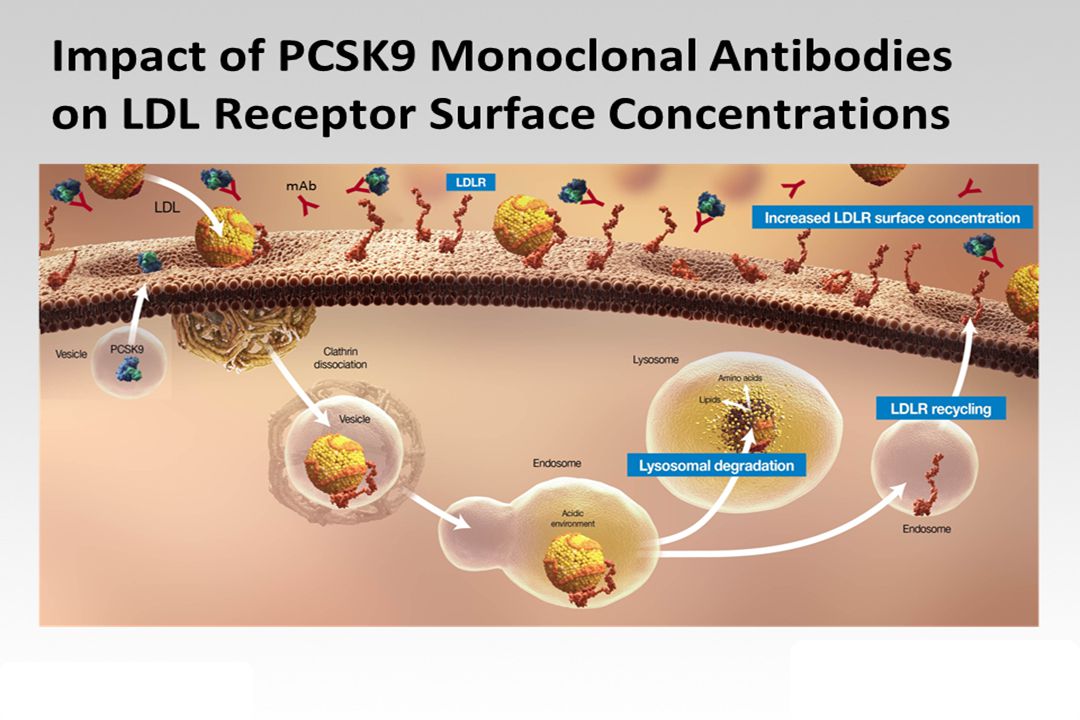
Blockade of PCSK9/LDLR Interaction May Lower LDL Levels
Main Point: Inhibition of circulating PCSK9 in such a way that it blocks the interaction of PCSK9 with cell surface LDLR may lower LDL cholesterol.1 Blocking the interaction of PCSK9 and LDLRs in this manner may allow internalized LDLRs to cycle back to the cell surface instead of being degraded in lysosomes, leading to increased concentrations of LDLRs on the cell surface.1 This may, in turn, result in a higher LDL-cholesterol clearance rate by hepatocytes and an overall reduction in plasma LDL-cholesterol levels.1 1. Chan JC, et al. Proc Natl Acad Sci U S A. 2009;106: Reference: Chan JC, Piper DE, Cao Q, et al. A proprotein convertase subtilisin/kexin type 9 neutralizing antibody reduces serum cholesterol in mice and nonhuman primates. Proc Natl Acad Sci U S A. 2009;106: AMG 145-GRC-AMG October-NP

32
PCSK9 INHIBITORS Μονοκλωνικά αντισώματα που εμποδίζουν την αλληλεπίδραση της PCSK9 (proprotein convertase subtilisin/kexin 9) με τον LDL υποδοχέα
 με τον LDL υποδοχέα.")
34
ΤΗΣ ΥΠΟΛΙΠΙΔΑΙΜΙΚΗΣ ΑΓΩΓΗΣ
ΕΠΙΤΕΥΞΗ ΤΩΝ ΣΤΟΧΩΝ ΤΗΣ ΥΠΟΛΙΠΙΔΑΙΜΙΚΗΣ ΑΓΩΓΗΣ PCSK9 inhibitors + ΣΤΑΤΙΝΗ

35
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΩΝ ΔΥΣΛΙΠΙΔΑΙΜΙΩΝ (5)
OI ΑΝΑΣΤΟΛΕΙΣ ΤΗΣ PSCK9 : EVOLΟCUMAB/ALIROCUMAB ΜΟΝΟΚΛΩΝΙΚΑ ΑΝΤΙΣΩΜΑΤΑ ΚΑΤΑ ΤΗΣ PCSK9

36
Ανεπιθύμητες ενέργειες: ρινοφαρυγγίτιδα, οσφυαλγία, γριπώδης συνδρομή
Ασθενείς υπό αγωγή με ATORVA (10 ή 80mg/d) ή συνδυασμό ATORVA (80mg/d) + ezetimibe (10mg/d) Evolocumab vs placebo (420mg/4 εβδομάδες), n=901 LDL CHOL κατά 57%, p<0.001 Ανεπιθύμητες ενέργειες: ρινοφαρυγγίτιδα, οσφυαλγία, γριπώδης συνδρομή N Engl J Med 2014;370:
 ή συνδυασμό ATORVA (80mg/d) + ezetimibe (10mg/d) Evolocumab vs placebo. (420mg/4 εβδομάδες), n=901. LDL CHOL κατά 57%, p< Ανεπιθύμητες ενέργειες: ρινοφαρυγγίτιδα, οσφυαλγία, γριπώδης συνδρομή. N Engl J Med 2014;370:")
37
EVOLOCUMAB (120mg/2w ή 420mg/4w) ΣΕ ΑΣΘΕΝΕΙΣ ΜΕ ΕΤΕΡΟΖΥΓΗ FH:
Η ΜΕΛΕΤΗ RUTHERFΟRD-2 n=331 LDL CHOL: KATA 59.2% KAI 61.3% LANCET 2014, OCT 1 [EPUB AHEAD OF PRINT]

38
Alirocumab Significantly Reduced LDL-C from Baseline to Week 24 versus Placebo
Primary Endpoint: Percent Change from Baseline to Week 24 in LDL-C All patients on background max-tolerated statin ±other lipid-lowering therapy Alirocumab FH I FH II Placebo N=322 N=163 N=166 N=81 LS mean (SE) % change from baseline to Week 24 43.4% had dose increase at W12 38.6% had dose increase at W12 LS mean difference (SE) vs. placebo: −57.9% (2.7) P<0.0001 −51.4% (3.4) P<0.0001 Intent-to-treat (ITT) Analysis
 % change from baseline to Week % had dose increase at W % had dose increase at W12. LS mean difference (SE) vs. placebo: −57.9% (2.7) P< −51.4% (3.4) P< Intent-to-treat (ITT) Analysis.")
39
Alirocumab Maintained Consistent LDL-C Reductions Over 52 Weeks
Achieved LDL-C Over Time on Background of Maximally-Tolerated Statin ±Other LLT Placebo: FH I Alirocumab: FH I FH II FH II LDL-C, LS mean (SE), mmol/L 3.5 mmol/L 1.8 mmol/L 3.7 mmol/L 1.9 mmol/L mg/dL 1.7 mmol/L 4.0 mmol/L Dose ↑ if LDL-C >70 mg/dL at W8 Week Intent-to-treat (ITT) Analysis LLT = lipid-lowering therapy
, mmol/L. 3.5 mmol/L. 1.8 mmol/L. 3.7 mmol/L. 1.9 mmol/L. mg/dL. 1.7 mmol/L. 4.0 mmol/L. Dose ↑ if LDL-C >70 mg/dL at W8. Week. Intent-to-treat (ITT) Analysis. LLT = lipid-lowering therapy.")
40
ΝΕΩΤΕΡΑ ΦΑΡΜΑΚΑ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΩΝ ΔΥΣΛΙΠΙΔΑΙΜΙΩΝ (6)
6. OI ΑΝΑΣΤΟΛΕΙΣ ΤΗΣ MTP : ΛΟΜΙΤΑΠΙΔΗ ΓΙΑ ΤΗΝ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΗΣ ΟΜΟΖΥΓΗΣ FH

42
Mean % Change in TC, LDL-C, and Apo B Through the Efficacy Phase (ITT, LOCF)
LOPITAPIDE ΣΕ ΑΣΘΕΝΕΙΣ ΜΕ ΟΜΟΖΥΓΗ FH 40% Reduction Mean Change from Baseline (%) Study Week Rader DJ. J Clin Lipid :6(3): ; Data on File, Aegerion Pharmaceuticals
 Study Week. Rader DJ. J Clin Lipid. 2012:6(3): 282-3; Data on File, Aegerion Pharmaceuticals.")
43
Treatment-emergent adverse events
System organ class preferred term Efficacy phase 26 weeks Safety phase >26–78 weeks n % At least one adverse event 27 93 21 91 Gastrointestinal disorders 17 74 Infections and infestations 15 52 10 44 Investigations (e.g. weight loss, lab abnormalities) 13 45 5 22 General disorders and administrative site conditions (e.g. fatigue, malaise) 8 28 7 30 Musculoskeletal and connective tissue disorders Injury, poisoning, and procedural complications (e.g. skin lacerations) 24 Nervous system disorders 6 3 Cardiac disorders 2 9 Hepatobiliary disorders 1 Rader DJ. J Clin Lipid. 2012:6:282–3; Data on File, Aegerion Pharmaceuticals
 General disorders and administrative site conditions (e.g. fatigue, malaise) Musculoskeletal and connective tissue disorders. Injury, poisoning, and procedural complications (e.g. skin lacerations) 24. Nervous system disorders Cardiac disorders Hepatobiliary disorders. 1. Rader DJ. J Clin Lipid. 2012:6:282–3; Data on File, Aegerion Pharmaceuticals.")
44
LOJUXTA, Aegerion Pharmaceuticals

Παρόμοιες παρουσιάσεις

 είναι κυρίως νόσος των ηλικιωμένων. Η μέση ηλικία των ασθενών με ΚΑ είναι τα 75 έτη. Η μέση ηλικία.>")





 νς Ατορβαστατίνης>")












