Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

2
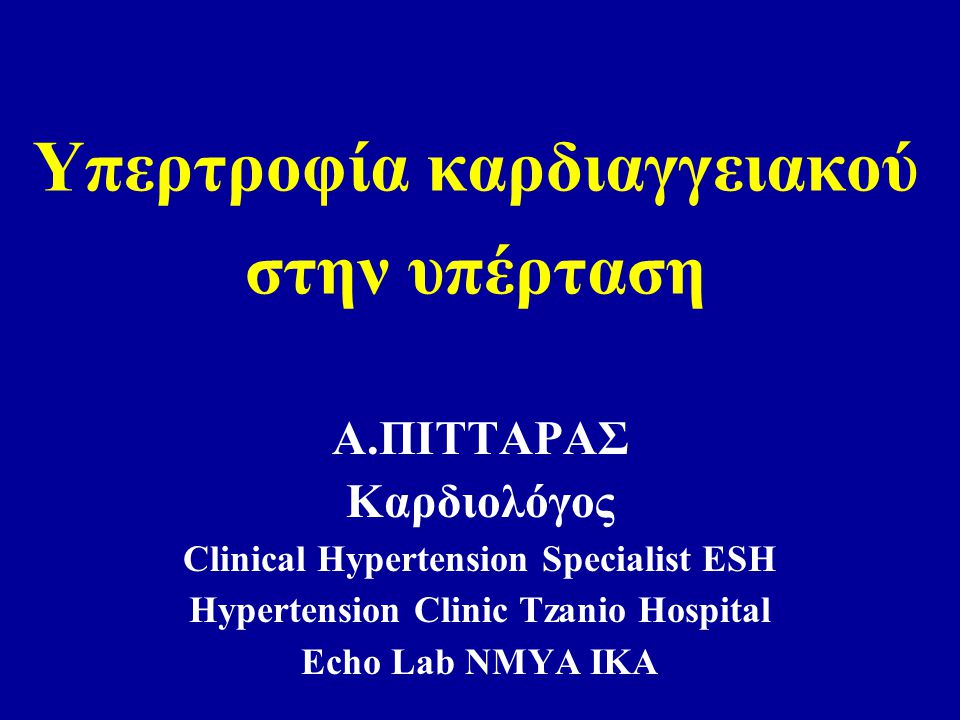
Υπερτροφία καρδιαγγειακού στην υπέρταση Α.ΠΙΤΤΑΡΑΣ Καρδιολόγος Clinical Hypertension Specialist ESH Hypertension Clinic Tzanio Hospital Echo Lab ΝΜΥΑ ΙΚΑ

5
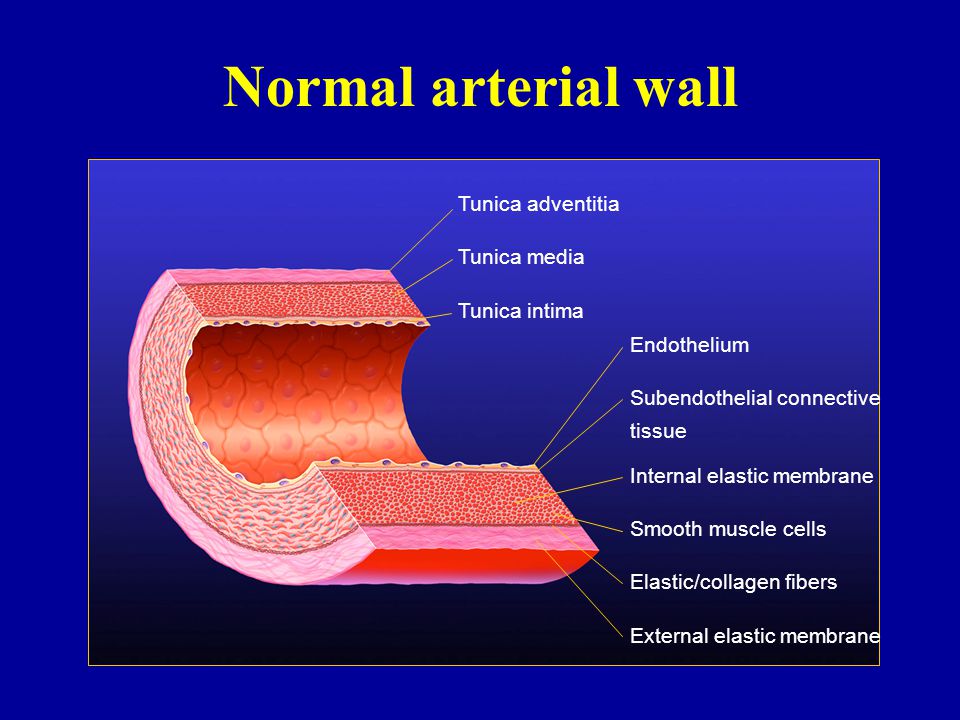
Normal arterial wall Tunica adventitia Tunica media Tunica intima Endothelium Subendothelial connective tissue Internal elastic membrane Smooth muscle cells Elastic/collagen fibers External elastic membrane

10
Main steps in the atherosclerotic process (in vivo) a Normal intima (rabbit)Thickened intima (rabbit) Soma et al, 1994
 a Normal intima (rabbit)Thickened intima (rabbit) Soma et al, 1994")
11
Growth factors Endothelin Vascular smooth muscle cell (SMC) a Hypertension hypertrophy of the media Atherosclerosis cell proliferation and migration into the intima Hypertension and atherosclerosis: common factors
 a Hypertension hypertrophy of the media Atherosclerosis cell proliferation and migration into the intima Hypertension and atherosclerosis: common factors")
12
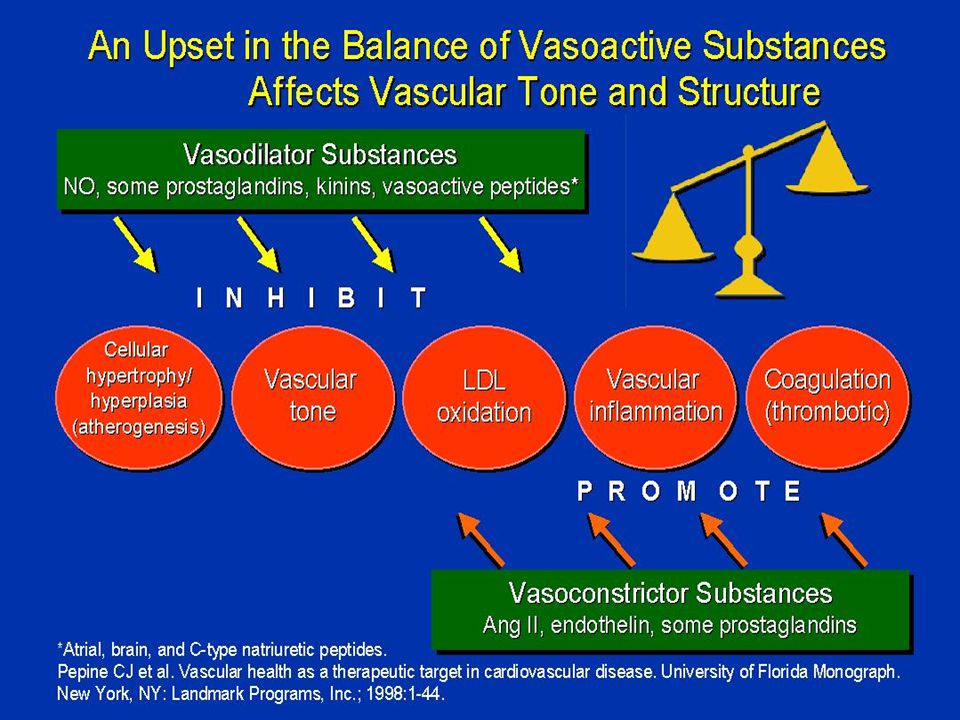
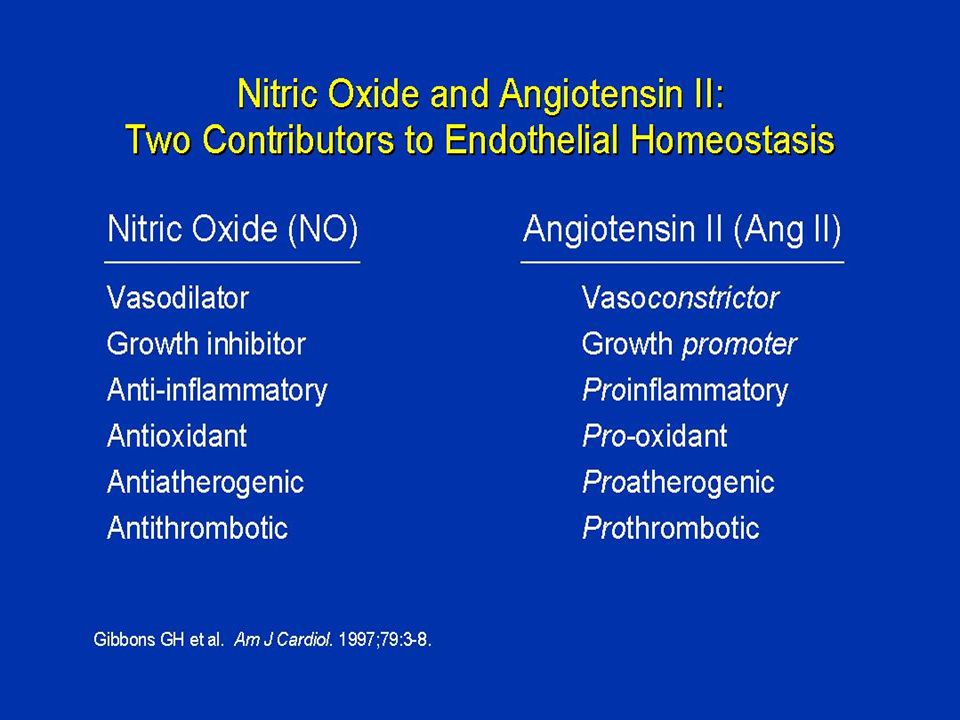
Διατήρηση Ενδοθηλιακής Λειτουργίας Endothelin I Angiotensin II Thromboxane A 2 Oxygen Nitric oxide Prostaglandin I 2 Vascular constriction Proliferation of vascular smooth muscle cells RISK FACTORS hypertension smoking hyperlipidemia glucose intolerance diabetes + – Vascular dilatation Anti-proliferation of vascular smooth muscle cells

13
Main steps in the atherosclerotic process (atherogenesis) a Smooth cell proliferation... and migration into the intima

15
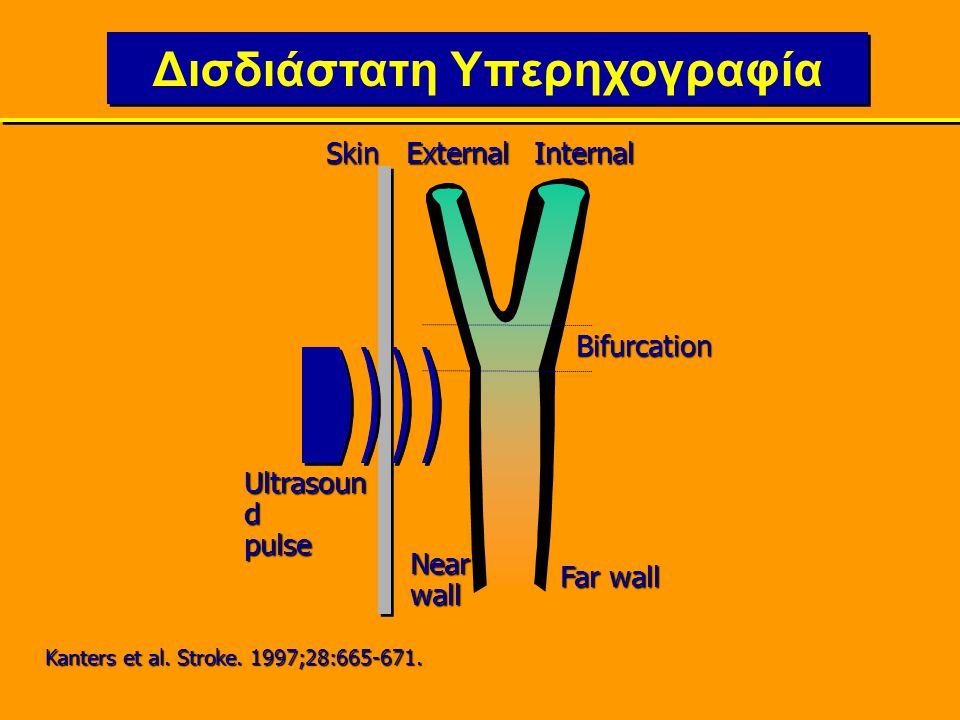
Δισδιάστατη Υπερηχογραφία SkinΕxternalInternal Bifurcation Nearwall Far wall Ultrasoun d pulse Κanters et al. Stroke. 1997;28:665-671.

16
Έσω καρωτίδα (IC)Έξω καρωτίδα (EC) Δέρμα Κοντινό τοίχωμα Μακρινό τοίχωμα 1.0 cm 0.5-1.0 cm 1.0 cm CBM max Μέσος όρος του μέγιστου IMT από 4 μακρινά τοιχώματα (+ 4 κοντινά τοιχώματα) σε CC και Bif, αμφοτερόπλευρα Διχασμός (Bif) Κοινή καρωτίδα (CC) Ορισμός του πάχους του έσω –μεσου χιτωνα (ΙΜΤ)
Έξω καρωτίδα (EC) Δέρμα Κοντινό τοίχωμα Μακρινό τοίχωμα 1.0 cm cm 1.0 cm CBM max Μέσος όρος του μέγιστου IMT από 4 μακρινά τοιχώματα (+ 4 κοντινά τοιχώματα) σε CC και Bif, αμφοτερόπλευρα Διχασμός (Bif) Κοινή καρωτίδα (CC) Ορισμός του πάχους του έσω –μεσου χιτωνα (ΙΜΤ)")
17
Συσχέτιση μεταξύ ΟΕΜ ή ΑΕΕ και πάχους της καρωτίδας 0 5 10 15 20 25 30 35 40 45 12345 Πάχος έσω-μέσου χιτώνα (IMT), πεμπτημόρια (quintiles) (συνδυασμένη μέτρηση των μέγιστων CCA και ICA) Ποσοστό εμφράγματος του μυοκαρδίου ή Α.Ε.Ε. ανά 1000 έτη ασθενών 13.6 18.4 22.2 40.9 O’Leary et al, 1999 7.8

18
Μελέτη PREVENT PART-2 SECURE BCAPS MIDAS ns VHAS ns INSIGHT DAPHNE ELSA Ασθένεια CHD VD Υψ.Κίνδ. VD HT Θεραπευτικές αγωγές Αμλοδιπίνη έναντι Placebo Ραμιπρίλη έναντι Placebo Μετοπρολόλη έναντι Placebo Ισραδιπίνη έναντι HCTZ Βεραπαμίλη έναντι Χλωροθαλιδόνης Νιφεδιπίνη GITS έναντι Cο-Αμιλοζίδης Δοξαζοσίνη έναντι HCTZ Λασιδιπινη - Ατενολολη Μέτρηση IMT M max CC-IMT M max Bif M max CC-IMT C + Fem IMT-CBM Ασθενείς (n) 373 617 732 793 833 498 324 80 2255 Πρόσφατες Μελέτες Αντιυπερτασικών Παραγόντων στο Καρωτιδικό IMT
 Πρόσφατες Μελέτες Αντιυπερτασικών Παραγόντων στο Καρωτιδικό IMT.")
19
Επιδράσεις των CCB στις Αγγειακές Μεταβολές και στα Κλινικά Επεισόδια: Αρχική Μελέτη Υπολογισμούτου Πάχους IMT των Καρωτίδων IMT = intimal-medial thickness. Borhani et al. JAMA. 1996;276:785-791. MIDAS 1996 Isradipine (5-10 mg/day) vs hydrochlorothiazide (25-50 mg/day) Early (6 mo) slowing of IMT thickening with isradipine, but no difference between treatment groups in change in carotid IMT at 3 y 883 3 y StudyNFollow-up Vascular Changes Trend toward major vascular events with isradipine Coronary Events
 vs hydrochlorothiazide (25-50 mg/day) Early (6 mo) slowing of IMT thickening with isradipine, but no difference between treatment groups in change in carotid IMT at 3 y y StudyNFollow-up Vascular Changes Trend toward major vascular events with isradipine Coronary Events.")
20
PREVENT: Επίδραση Αμλοδιπίνης στο ΙΜΤ των Καρωτίδων-0.10 -0.05 0.00 0.05 0.10 AmlodipinePlacebo P=.007 Μean Change (mm) at 3 Years Pitt et al.Circulation. 2000;102:1503-1510.

21
PREVENT: Επιδράσεις της Αμλοδιπίνης στην Καρδιαγγειακή Νοσηρότητα και Θνησιμότητα RRR 95% Αναλογική RRR 95% Αναλογική *Amlo + Pl%HR ‡ CI ‡ P ‡ διαφορά *Amlo + Pl%HR ‡ CI ‡ P ‡ διαφορά Θνησιμότητα από όλα τα αίτια 6 8260,74 0,26-2,120,57 Μείζονα αγγειακά επεισόδια 2328180,82 0,47-1,420,47 Αλλα πιστοποιηθέντα μη θανατηφόρα καρδιαγγειακά επεισόδια (CHF, ασταθής στηθάγχη) 6188350,65 0,47-0,910,01 Μείζονες αγγειακές επεμβάσεις § 53 86 4 3 0,57 0,41-0,8 0,001 Οποιοδήποτε πιστοποιηθέν μείζον αγγειακό επεισόδιο ή επέμβαση86116310,69 0,52-0,920,01 *Amlo = Amlodipine, n=417; +Pl=Placebo, n=408; ‡ From proportional hazards models; P values presented only for prespecified composite event outcomes; § Includes angioplasties, stents, and atherectomies. Pitt et al. Circulation. 2000; 102:1503-1510. 0,0 0,5 1,0 1,5 2,0 2,5

22
Πανεπιστήμια των Μιλάνο Πάδοβα Μπρέσια Μπολώνια Αγκώνα Πίζα Ρώμη Νάπολη Μαδρίτη Βαρκελώνη Αθήνα Γλασκώβη Σέφιλντ Μόναχο Βερολίνο Φραγκφούρτη Mένστερ Αμβούργο Παρίσι Γκρενόμπλ Νανσύ Στοκχόλμη Λουντ H κλινική μελέτη ELSA Κέντρα αναφοράς (n = 23)
")
23
Αποτελέσματα Πρωταρχικού Τελικού Σημείου (4 ετής εξέλιξη CBM Max ) 0 0.01 0.02 0.03 0.04 0.05 Μέση μεταβολή (mm) Ατενολόλη Λασιδιπίνη P<0,001 Ασθενείς που ολοκλήρωσαν την μελέτη 0.06 ELSA
 Μέση μεταβολή (mm) Ατενολόλη Λασιδιπίνη P<0,001 Ασθενείς που ολοκλήρωσαν την μελέτη 0.06 ELSA")
24
Αποτελέσματα Πρωταρχικού Τελικού Σημείου (ετήσια εξέλιξη CBM Max ) 0.0145 0.0087 0 0.005 0.01 0.015 0.02 0.025 mm Ατενολόλη Λασιδιπίνη p=0,0073 Ασθενείς που ολοκλήρωσαν την μελέτη
 mm Ατενολόλη Λασιδιπίνη p=0,0073 Ασθενείς που ολοκλήρωσαν την μελέτη")
25
ELSA:Ανάλυση συμβαμάτων Myocardial infarction Relative risk of adverse events in lacidipine- and atenolol-treated patients Stroke All death Hospitalised angina Other minor CV events All serious AEs Events (N) LacidipineAtenolol 17 14 33 17 11 30 Major CV events CV death 8 201 18 9 27 4 13 17 27 186 Lacidipine betterAtenolol better 1.0 Relative risk (95% CI) 0.10.20.30.52.04.0
 LacidipineAtenolol Major CV events CV death Lacidipine betterAtenolol better 1.0 Relative risk (95% CI)")
26
INSIGHT: Η επίδραση της Νιφεδιπίνης στο IMT Follow-up (years) IMT Change from baseline (mm) 0 -0.010 0 0.010 0.020 0.030 0.040 1234 HCTZ/ Amiloride Nifedipine GITS πρόοδος υποστροφή Simon et al. Circulation (June, 2001)
.")
27
Συμπεράσματα από την μελέτη INSIGHT/IMT * σε σύγκριση με την 0.010 mm/έτος φυσιολογική εξέλιξη του IMT από την EVA study Simon et al. Circulation (June, 2001) Η νιφεδιπίνη GITS εμποδίζει την εξέλιξη του intima-media thickness ενώ τα διουρητικά φαίνονται ότι απλώς την καθυστερούν *. Η προστατευτική δράση της νιφεδιπίνης GITS (συγκρινόμενη με τα διουρητικά) δεν μπορεί αποδοθεί σε διαφορές ως προς τον έλεγχο της ΑΠ. Πιθανοί μηχανισμοί: - Aντιαθηρωτική δράση στο intima - Aντιπολλαπλασιαστική δράση στο media
 Η νιφεδιπίνη GITS εμποδίζει την εξέλιξη του intima-media thickness ενώ τα διουρητικά φαίνονται ότι απλώς την καθυστερούν *. Η προστατευτική δράση της νιφεδιπίνης GITS (συγκρινόμενη με τα διουρητικά) δεν μπορεί αποδοθεί σε διαφορές ως προς τον έλεγχο της ΑΠ. Πιθανοί μηχανισμοί: - Aντιαθηρωτική δράση στο intima - Aντιπολλαπλασιαστική δράση στο media.")
28
SECURE (ramipril) - primary outcome Lonn E ACC 49 th Session, Anaheim, USA, March 2000 p = 0.028
 - primary outcome Lonn E ACC 49 th Session, Anaheim, USA, March 2000 p = 0.028")
29
SECURE (ramipril) - secondary outcomes &Single maximum IMT regression slope in the ramipril 10 mg group significantly lower than in the placebo group (p = 0.055). &Trend towards fewer CV events (composite endpoint of MI/stroke/CV death) in ramipril group. Lonn E ACC 49 th Session, Anaheim, USA, March 2000
 in ramipril group. Lonn E ACC 49 th Session, Anaheim, USA, March")
33
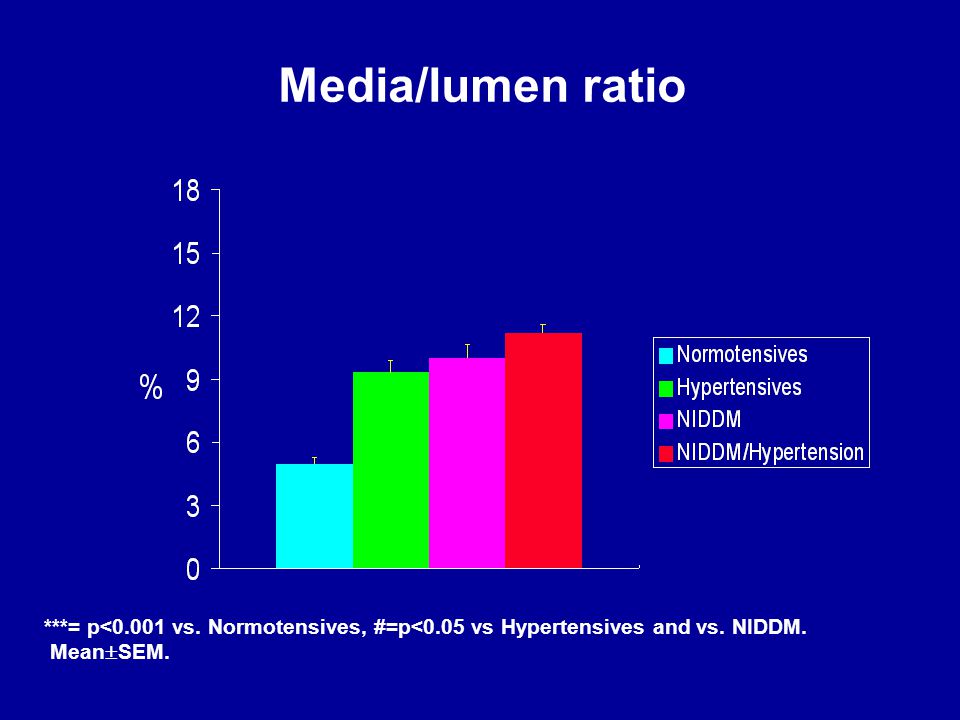
Media/lumen ratio ***= p<0.001 vs. Normotensives, #=p<0.05 vs Hypertensives and vs. NIDDM. Mean SEM. *** ***# Rizzoni et al, J Circulation 2001

35
Arteriolar vasoconstrictionArteriolar vasoconstriction Increase in wall : lumen ratioIncrease in wall : lumen ratio RarefactionRarefaction MECHANISMS OF INCREASE IN PERIPHERAL RESISTANCE

36
CAPILLARY RAREFACTION IN HUMAN HYPERTENSION Normotensive Sullivan et al. Hypertension 1983;5:844 Hypertensive

37
Incident Wave Ventricular ejection Pulse wave velocity at a given resistance Reflected Wave Pulse wave velocity Reflection points closer to the heart HEART RESISTANCE VESSELS

39
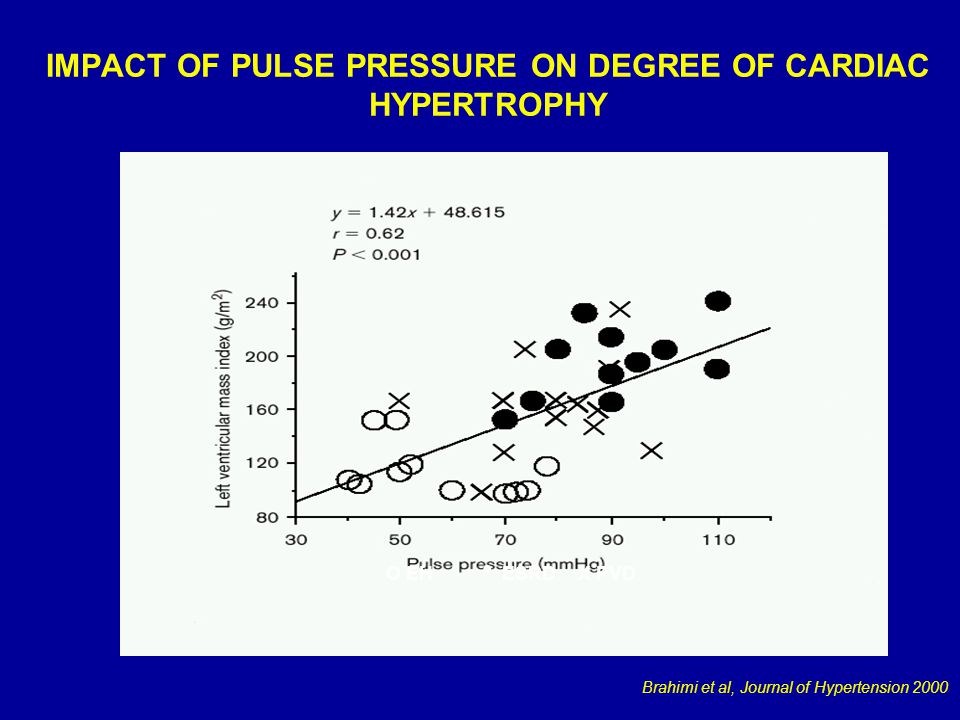
IMPACT OF PULSE PRESSURE ON DEGREE OF CARDIAC HYPERTROPHY O EH ESRDX PVD Brahimi et al, Journal of Hypertension 2000

40
Aortic Pulse Wave Velocity Predicts Cardiovascular Mortality in Subjects > 70 Years of Age Arterioscler Thromb Vasc Biol. 2001;21:2046-2050

47
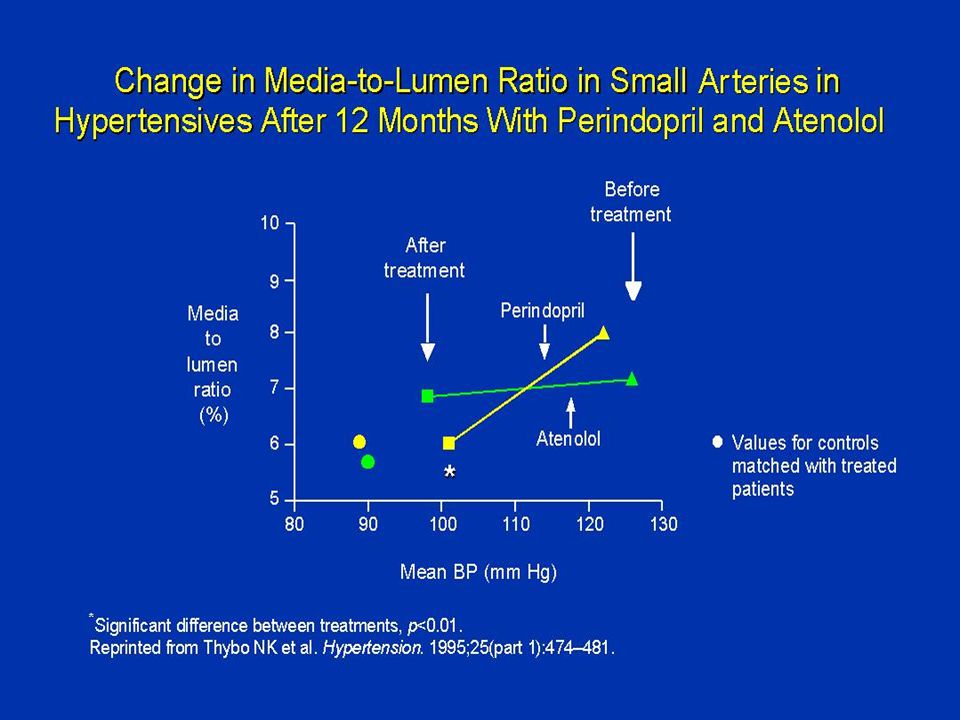
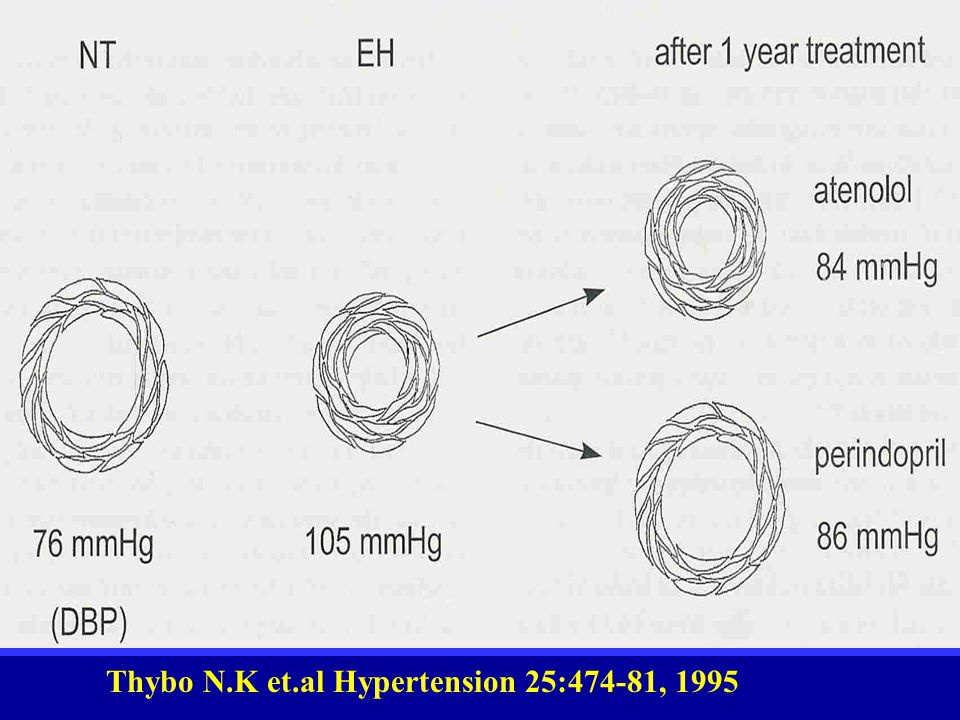
Thybo N.K et.al Hypertension 25:474-81, 1995

52
LVH: Ορισμός LVH is the major cardiac alteration associated with systemic arterial hypertension, in which left ventricular mass and wall thickness increase in response to the progressive overload and increased left ventricular wall stress that are imposed by the higher arterial pressure and total peripheral resistance (Adapted from Frohlich ED, Re RN Hurst’s the Heart. 1998:1635-1650)
.")
53
ΥΑΚ: Ορισμός ΥΑΚ είναι η κύρια καρδιακή μεταβολή που σχετίζεται με την υπέρταση. Η μάζα και το πάχος των τοιχωμάτων της αριστερής κοιλίας αυξάνουν σαν προσαρμογή στην προοδευτική υπερφόρτιση και αυξανόμενη τοιχωματική τάση που επέρχονται από την υψηλή ΑΠ και υψηλές περιφερικές αντιστάσεις. (Adapted from Frohlich ED, Re RN Hurst’s the Heart. 1998:1635-1650)
.")
54
Determinants for LV Hypertrophy Υπόβαθρο Ηλικία Φύλο Φυλή Παχυσαρκία Αλάτι Αλκοόλ Λοιπές παθήσεις Αιμοδυναμικές παράμετροι Αρτ. Πίεση Φόρτιση όγκου Αρτηριακή δομή Γλοιότητα αίματος Μη-αιμοδυναμικές παράμετροι Τροφικοί παράγοντες: -Συμπαθητικό ΝΣ -RAAS -Ινσουλίνη Γενετικοί παράγοντες και άλλα ενδοκυττάρια σήματα

55
LVH: Causative Factors Genetic/ environmental factors Age Gender Race Other illness Hemodynamic load Volume Pressure Trophic factors Angiotensin II Aldosterone Catecholamines Insulin

56
Processes Underlying Diastolic Dysfunction Hypertension Aging Arteriosclerosis Diabetes Blood vessels Hypertrophy Altered elastin & collagen Calcification Endothelial dysfunction Loss of compliance Myocardium Hypertrophy Fibrosis/altered collagen Apoptosis Infarction/ischemia Cellular dysfunction Loss of compliance Impaired relaxation Heart failure Death, MI, ACS, heart failure, arrhythmias, stroke

57
Processes Underlying Diastolic Dysfunction Hypertension Aging Atherosclerosis Diabetes Blood Vessels Hypertrophy Altered elastin & collagen Calcification Endothelial dysfunction Loss of compliance Myocardium Hypertrophy (LVH) Fibrosis Cellular dysfunction Ischemia Increased stiffness Impaired relaxation Diastolic Dysfunction Heart Failure with Preserved Systolic Function
 Fibrosis Cellular dysfunction Ischemia Increased stiffness Impaired relaxation Diastolic Dysfunction Heart Failure with Preserved Systolic Function")
58
Παράγοντες σχετιζόμενοι με LVH I Blood Pressure ++++ Wall stress ++++ Stroke volume ++++ Obesity ++++ IGF-1 ++ FGF ++ Gender ++ Race ++ Age ++

59
Παράγοντες σχετιζόμενοι με LVH II Intracellular Ca Insulin resistance Angiotensin II PDGF Shear stress Circuferential/Axial stretch Estrogen Pulse Pressure Aortic Stiffness

60
Association Between Left Ventricular Mass and Hemodynamic and Nonhemodynamic Factors : Strength of Evidence Supporting a Causal Role (b) Association Between Left Ventricular Mass and Hemodynamic and Nonhemodynamic Factors : Strength of Evidence Supporting a Causal Role (b) FactorAlcohol Intrinsic myocardial contractility Blood viscosity Parathyroid hormone Aldosterone (collagen synthesis) Sodium intake Na + /H + exchanger and Na + -K+ - CI - cotransport system Polymorphism of the ACE gene Plasma renin activity Norepinephrine Na + /Li + exchanger βARK FactorAlcohol Intrinsic myocardial contractility Blood viscosity Parathyroid hormone Aldosterone (collagen synthesis) Sodium intake Na + /H + exchanger and Na + -K+ - CI - cotransport system Polymorphism of the ACE gene Plasma renin activity Norepinephrine Na + /Li + exchanger βARK Evidence Needs confirmation ControversialControversialControversialControversialControversialEvidence ControversialControversialControversialControversialControversial
 Association Between Left Ventricular Mass and Hemodynamic and Nonhemodynamic Factors : Strength of Evidence Supporting a Causal Role (b) FactorAlcohol Intrinsic myocardial contractility Blood viscosity Parathyroid hormone Aldosterone (collagen synthesis) Sodium intake Na + /H + exchanger and Na + -K+ - CI - cotransport system Polymorphism of the ACE gene Plasma renin activity Norepinephrine Na + /Li + exchanger βARK FactorAlcohol Intrinsic myocardial contractility Blood viscosity Parathyroid hormone Aldosterone (collagen synthesis) Sodium intake Na + /H + exchanger and Na + -K+ - CI - cotransport system Polymorphism of the ACE gene Plasma renin activity Norepinephrine Na + /Li + exchanger βARK Evidence Needs confirmation ControversialControversialControversialControversialControversialEvidence ControversialControversialControversialControversialControversial")
61
ΓΟΝΙΔΙΑ ΣΧΕΤΙΖΟΜΕΝΑ ΜΕ LVH ΦΑΙΝΟΤΥΠΟ ΣΥΣΤΟΛΙΚΗ & ΔΙΑΣΤΟΛΙΚΗ ΔΥΣΛΕΙΤΟΥΡΓΙΑ ΓΟΝΙΔΙΑ ΣΧΕΤΙΖΟΜΕΝΑ ΜΕ LVH ΦΑΙΝΟΤΥΠΟ ΣΥΣΤΟΛΙΚΗ & ΔΙΑΣΤΟΛΙΚΗ ΔΥΣΛΕΙΤΟΥΡΓΙΑ ΓΟΝΙΔΙΑ ΡΥΘΜΙΣΗΣ ΑΙΜΟΔΥΝ/ΚΟΥ ΦΟΡΤΙΟΥ α-, β-adrenergic receptors Renin-angiotensin system Sodium sensitivity Insulin resistance Endothelial function ΓΟΝΙΔΙΑ ΡΥΘΜΙΣΗΣ ΑΙΜΟΔΥΝ/ΚΟΥ ΦΟΡΤΙΟΥ α-, β-adrenergic receptors Renin-angiotensin system Sodium sensitivity Insulin resistance Endothelial function ΓΟΝΙΔΙΑ ΡΥΘΜΙΣΗΣ ΚΑΤΑΣΚΕΥΗΣ ΑΡΙΣ. ΚΟΙΛΙΑΣ Sarcomeric proteins Thick filaments Cardiac α-, βmyosin heavy chain Thin filame Cardiac, skeletal actin Troponin I, C, or T Tropomyosin Titin Myosin binding- protein C Extracellular Matrix Collagen a Types I, III Fibrillin ΓΟΝΙΔΙΑ ΡΥΘΜΙΣΗΣ ΚΑΤΑΣΚΕΥΗΣ ΑΡΙΣ. ΚΟΙΛΙΑΣ Sarcomeric proteins Thick filaments Cardiac α-, βmyosin heavy chain Thin filame Cardiac, skeletal actin Troponin I, C, or T Tropomyosin Titin Myosin binding- protein C Extracellular Matrix Collagen a Types I, III Fibrillin Genes regulating hormones, growth factors, and cell signaling Renin-angiotensin system β-adrenergic receptors Natriuretic peptides (atrial, brain) Mitogen-activated protein kinases Guanine (g) nucleotide binding proteins Insulin growth factor Transforming growthfactor-β Fibroblast growth factor Genes regulating hormones, growth factors, and cell signaling Renin-angiotensin system β-adrenergic receptors Natriuretic peptides (atrial, brain) Mitogen-activated protein kinases Guanine (g) nucleotide binding proteins Insulin growth factor Transforming growthfactor-β Fibroblast growth factor Genes regulating calcium transport, binding, and signaling Na + -Ca ++ exchanger Ryanodine receptors Calmodulin Calcineurin NF-AT 3 SERCA 2 Phospholamban Genes regulating calcium transport, binding, and signaling Na + -Ca ++ exchanger Ryanodine receptors Calmodulin Calcineurin NF-AT 3 SERCA 2 Phospholamban Left ventricular hypertrophy
 Mitogen-activated protein kinases Guanine (g) nucleotide binding proteins Insulin growth factor Transforming growthfactor-β Fibroblast growth factor Genes regulating hormones, growth factors, and cell signaling Renin-angiotensin system β-adrenergic receptors Natriuretic peptides (atrial, brain) Mitogen-activated protein kinases Guanine (g) nucleotide binding proteins Insulin growth factor Transforming growthfactor-β Fibroblast growth factor Genes regulating calcium transport, binding, and signaling Na + -Ca ++ exchanger Ryanodine receptors Calmodulin Calcineurin NF-AT 3 SERCA 2 Phospholamban Genes regulating calcium transport, binding, and signaling Na + -Ca ++ exchanger Ryanodine receptors Calmodulin Calcineurin NF-AT 3 SERCA 2 Phospholamban Left ventricular hypertrophy.")
62
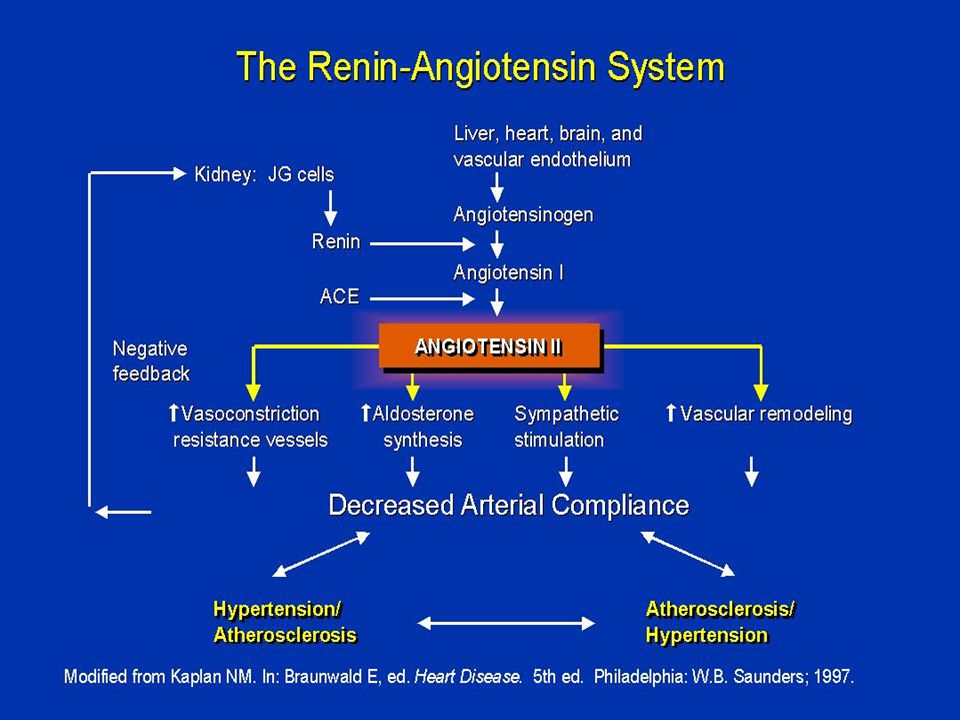
Η Αγγειοτασίνη II Διαδραματίζει Πρωταρχικό Ρόλο στη Βλάβη των Οργάνων Adapted from Willenheimer R et al Eur Heart J 1999; 20(14): 997 1008, Dahlöf B J Hum Hypertens 1995; 9(suppl 5): S37 S44, Daugherty A et al J Clin Invest 2000; 105(11): 1605 1612, Fyhrquist F et al J Hum Hypertens 1995; 9(suppl 5): S19 S24, Booz GW, Baker KM Heart Fail Rev 1998; 3: 125 130, Beers MH, Berkow R, eds. The Merck Manual of Diagnosis and Therapy. 17th ed. Whitehouse Station, NJ: Merck Research Laboratories 1999: 1682 1704, Anderson S Exp Nephrol 1996; 4(suppl 1): 34 40, Fogo AB Am J Kidney Dis 2000; 35(2): 179 188 Αιι ΑΤ1 υποδοχέας Αθηροσκλήρυνση* Αγγειοσύσπαση Αγγειακή υπερτροφία Δυσλειτουργία ενδοθηλίου Υπερτροφία αριστεράς κοιλίας Ίνωση Αναδιαμόρφωση Απόπτωση Εγκεφαλικό Θάνατος Υπέρταση Καρδιακή ανεπάρκεια Έμφραγμα μυοκαρδίου Νεφρική ανεπάρκεια Ρυθμός σπειραματικής διήθησης Πρωτεϊνουρία Απελευθέρωση αλδοστερόνης Σπειραματική σκλήρυνση *Προκλινικά δεδομένα
: 34 40, Fogo AB Am J Kidney Dis 2000; 35(2): 179 188 Αιι ΑΤ1 υποδοχέας Αθηροσκλήρυνση* Αγγειοσύσπαση Αγγειακή υπερτροφία Δυσλειτουργία ενδοθηλίου Υπερτροφία αριστεράς κοιλίας Ίνωση Αναδιαμόρφωση Απόπτωση Εγκεφαλικό Θάνατος Υπέρταση Καρδιακή ανεπάρκεια Έμφραγμα μυοκαρδίου Νεφρική ανεπάρκεια Ρυθμός σπειραματικής διήθησης Πρωτεϊνουρία Απελευθέρωση αλδοστερόνης Σπειραματική σκλήρυνση *Προκλινικά δεδομένα.")
63
Abnormal Exercise Blood Pressure Predicts Left Ventricular Mass in Pre- Hypertensive, Middle-aged Men and Women Andreas Pittaras, P.F.Kokkinos A.J. Manolis, D. Manjoros, P. Narayan, V. Papademetriou, and S. Singh Mediton Greece, VA & Georgetown University Medical Centers, Washington, DC,Tzanio Hospital, Piraeus AHA 2004

64
LVMI Predictors for Pre-HTN (Multiple Regression) R 2 p-value Men SBP @ 6 min 0.48 0.000 Age0.50 0.000 T-Time0.52 0.006 Women SBP @ 6 min 0.49 0.000 T-Time0.51 0.002 Age0.53 0.006
 R 2 p-value Men 6 min Age T-Time Women 6 min T-Time Age")
65
Exercise SBP Threshold for LVH (Cut-off Analysis) SBP threshold for LVH – Men: SBP >165 mm Hg – Women: SBP >170 mm Hg Achieved at a workload of approximately 6-7 METS.
 SBP threshold for LVH – Men: SBP >165 mm Hg – Women: SBP >170 mm Hg Achieved at a workload of approximately 6-7 METS.")
66
Logistics Regression Findings MEN BetaSEWaldExp(B)95% CIP-value 6-min SBP0.170.02360.11.1941.14-1.20.000 WOMEN 6-min SBP0.1060.01280.01.1141.0-1.30.000 The likelihood of having LVH increases by about 6-fold in men for every 10 mmHg increase in SBP above the threshold (1.194 10 =5.88) and 3-fold for women (1.114 10 =2.9).
95% CIP-value 6-min SBP WOMEN 6-min SBP The likelihood of having LVH increases by about 6-fold in men for every 10 mmHg increase in SBP above the threshold ( =5.88) and 3-fold for women ( =2.9).")
67
LVMI & Exercise SBP in Pre-HTN Men * p<0.01 Normal BP Ex-HTN * *

68
LVMI & Exercise SBP in Pre- Hypertensive Women * p<0.01 Normal BP Ex-HTN * *

69
EXERCISE BLOOD PRESSURE THRESHOLD FOR LEFT VENTRICULAR HYPERTROPHY IN NORMOTENSIVE AND HYPERTENSIVE MIDDLE-AGED MEN Pittaras, Kokkinos,et al J.Hypertension vol20;2002

70
LVMI Predictors for Normotensive Men (Multiple Regression) R-squared p-Value Normotensive –SBP @ 6 min 0.49 0.000 Hypertensive –SBP @ 6 min 0.41 0.000
 R-squared p-Value Normotensive 6 min Hypertensive 6 min")
71
LVMI & Exercise SBP in Hypertensive Men 95 120 145 170 195 SBPLVMI * p<0.01 Ex-HNT( -) Ex-HTN * *
 Ex-HTN * *")
72
LVMI & Exercise SBP in Normotensive Men 80 105 130 155 180 SBPLVMI * p<0.01 Ex-HNT( -) Ex-HTN * *
 Ex-HTN * *")
73
Correlates of LVMI for Normotensive & Hypertensive Men NormotensiveHypertensive Variables r_ r_ SBP @ 6 min 0.70 0.64 Max SBP 0.64 0.50 SBP @ 3 min0.54 0.41 RSBP 0.37 0.48 Ex. Time -0.29 - 0.24 Age 0.13 0.28

74
Other Predictors of LVMI Normotensive R-squaredp-Value –Max SBP0.41 0.000 –SBP @ 3 min 0.29 0.000 –Pulse Pressure-60.26 0.000 Hypertensive –SBP @3 min0.30 0.000 –Max SBP0.25 0.000 –Pulse pressure-60.24 0.000 –Pulse Pressure-3 0.10 0.000

75
Conclusions Systolic BP at 6 minutes of exercise is the strongest predictor of LV mass in normotensive and hypertensive men. The SBP threshold for LVH is a SBP >167 mm Hg for normotensive and >160 mm Hg for hypertensive men achieved at a workload of approximately 6-7 METS.

76
LOWER LEFT VENTRICULAR MASS, 24-HR BLOOD PRESSURE AND EXERCISE BLOOD PRESSURE IN FIT VS UNFIT MIDDLE-AGED MEN AND WOMEN Α.Pittaras et al ASH 2003 NY

77
ΓΥΝΑΙΚΕΣ (η=480) * ** Διαφορά μεταξύ όλων των ομάδων * Low-Fit vs Moderate and High-Fit
 * ** Διαφορά μεταξύ όλων των ομάδων * Low-Fit vs Moderate and High-Fit")
78
ΑΝΔΡΕΣ (η=385) * ** Διαφορά μεταξύ όλων των ομάδων * Low-Fit vs Moderate and High-Fit
 * ** Διαφορά μεταξύ όλων των ομάδων * Low-Fit vs Moderate and High-Fit")
79
Ambulatory Blood Pressure Predicts Left Ventricular Hypertrophy in Pre-Hypertensive Women Andreas Pittaras, P.F.Kokkinos, Demosthenes Panagiotakos, Athanasios Manolis, Puneet Narayan, Vasilios Papademetriou, and Steven Singh, Veterans Affairs Medical Center, Washington, DC, Georgetown University Medical Center, Washington, DC ACC 2004

80
Background: The JNC 7 report points to elevated cardiovascular (CV) risk even at systolic blood pressure (SBP) levels of 120-139 mm Hg or diastolic (DBP) of 80-89 mm Hg, classified as prehypertension. Left ventricular hypertrophy (LVH) in an independent CV risk factor and it is more closely related to 24-hour BP than office BP. We assessed 24-hour BP and cardiac parameters in prehypertensive women to determine if they have elevated 24-hour BP and increased left ventricular mass (LVM).
 in an independent CV risk factor and it is more closely related to 24-hour BP than office BP. We assessed 24-hour BP and cardiac parameters in prehypertensive women to determine if they have elevated 24-hour BP and increased left ventricular mass (LVM)..")
81
Methods: Two-hundred twenty, pre- hypertensive women (age=54±10 yrs) with resting BP=130±78 mm Hg and free of overt heart disease were consented to undergo an exercise tolerance test, echocardiographic assessment and 24hour BP monitoring. LVH was considered as LVM index >105 g/m2.

82
Results Age-specific prevalence of LVH The prevalence of LVH was 54.5%. Characteristics of the participants by LVH status. Age, and 24-hour BP were significantly higher in women with LVH versus those without (p < 0.01).
..")
83
LVM index and BP levels Significant correlations were noted between LVM index, 24-hour, daytime and nighttime BP.

84
Ambulatory BP values were significantly higher in pre- hypertensive women with LVH versus without.

85
ABP for Pre-hypertensive Women No LVHLVH Daytime SBP136±9150±11 Daytime DBP 81±890±9 Nighttime SBP118±9133±13 Nighttime DBP 69±8 80±10 24-hr SBP131±8143±10 24-hr DBP76±886±9

86
Multiple logistic regression analysis revealed that SBP, nighttime DBP, age and BMI were the strongest predictors of LVH Odds Ratio95% CIP Day SBP1.151.1 - 1.20.001 Night DBP1.081.0 - 1.10.002 Age1.061.02 - 1.10.004 BMI0.880.8 - 0.90.02

87
Cut-off analysis revealed that the daytime SBP threshold for LVH was 145 mm Hg.

88
LVH and daytime SBP There was a 4- fold increase in the likelihood of having LVH for every 10 mm Hg increase in daytime SBP above this threshold.

89
Conclusions: The prevalence of LVH is 54.5% in pre-hypertensive women. Daytime SBP is the strongest predicts of LVH in pre-hypertensive women. The threshold for LVH is >145 mm Hg The likelihood of having LVH increases by 4-fold for every 10 mm Hg increase above this threshold.

90
Nondippers Have Higher Incidence of Abnormal Exercise Blood Pressure Response Left Ventricular Hypertrophy and Diastolic Dysfunction in Pre-Hypertensive and Hypertensive Men Andreas Pittaras, P.Kokkinos, A J Manolis, P. Narayan V. Papademetriou, and S. Singh Mediton Clinic, Greece, VA & Georgetown University Medical Centers, Washington, DC, USA and Tzanio Hospital, Greece. ESH 2005 (Highlights)
.")
91
ALL MEN (n=563) I Dippers (443)Non-Dippers (120) P Age50±1154±8*0.000 BMI27.1 2.726.9 2.60.413 RSBP133±10138±8*0.000 SBP3150±15156±18*0.000 SBP6170±21179±17*0.000 SBPmax192±21202±19*0.000 DBP383±987±8*0.001 DBP687±990±8*0.001 DBPmax91±894±9*0.000 SBPmea n 138±12143±13*0.000 DBPmea n 83±10.486.16 ±11.4*0.004
 I Dippers (443)Non-Dippers (120) P Age50±1154±8*0.000 BMI RSBP133±10138±8*0.000 SBP3150±15156±18*0.000 SBP6170±21179±17*0.000 SBPmax192±21202±19*0.000 DBP383±987±8*0.001 DBP687±990±8*0.001 DBPmax91±894±9*0.000 SBPmea n 138±12143±13*0.000 DBPmea n 83± ±11.4*0.004")
92
ALL MEN (n=563) II Dippers (443)Non-Dippers (120) P LVMI122±29130±25*0.015 LVDD49±350±3*0.001 IVS10.6±1.111±1.1*0.005 PW10.2±1.210.5±1.1*0.034 AO31.2±2.532.1±2.2*0.000 LA36.8±2.337.3±2.3*0.05 Time(sec) 609±115589±770.080 Awave0.61±0.110.68±0.13*0.000 E/A1.1±0.360.97±0.36*0.001 DT229±23232±26*0.041
 II Dippers (443)Non-Dippers (120) P LVMI122±29130±25*0.015 LVDD49±350±3*0.001 IVS10.6±1.111±1.1*0.005 PW10.2± ±1.1*0.034 AO31.2± ±2.2*0.000 LA36.8± ±2.3*0.05 Time(sec) 609±115589± Awave0.61± ±0.13*0.000 E/A1.1± ±0.36*0.001 DT229±23232±26*0.041")
93
Pre-Hypertensives (n=316) I Dippers (263)Non-Dippers (53) P Age47.3±1155.5±8*0.000 BMI26.8± 2.726.1±2.70.079 RSBP127.3±7.8131.9±6.1*0.000 SBP3140.6±9.4148.2±7.6*0.000 SBP6156.6±12166.8±13*0.000 SBPmax179.6±14188.9±15*0.000 DBP377.5±6.781.1±7*0.001 DBP681.1±6.584.1±6.7*0.003 DBPmax85.9±688.2±6.6*0.015 SBPmean131.3±9133.3±7.40.139 DBPmean77.4±7.879.8 ±9*0.047
 I Dippers (263)Non-Dippers (53) P Age47.3±1155.5±8*0.000 BMI26.8± ± RSBP127.3± ±6.1*0.000 SBP3140.6± ±7.6*0.000 SBP6156.6± ±13*0.000 SBPmax179.6± ±15*0.000 DBP377.5± ±7*0.001 DBP681.1± ±6.7*0.003 DBPmax85.9±688.2±6.6*0.015 SBPmean131.3±9133.3± DBPmean77.4± ±9*0.047")
94
Pre-Hypertensives (n=316) II Dippers (263)Non-Dippers (53) P LVMI105.8±20112.8±21*0.023 LVDD48.2±2.449.1±3.1*0.020 IVS10±0.7810.3±0.84*0.028 PW9.58±0.89.7±0.950.275 AO30.3±2.231.5±2.3*0.000 LA35.8±2.0436.1±2.30.484 Time(sec)644±93594±62*0.000 Awave0.55±0.80.64±0.13*0.000 E/A1.29±0.291.19±0.38*0.029 DT218±18216±220.056
 II Dippers (263)Non-Dippers (53) P LVMI105.8± ±21*0.023 LVDD48.2± ±3.1*0.020 IVS10± ±0.84*0.028 PW9.58±0.89.7± AO30.3± ±2.3*0.000 LA35.8± ± Time(sec)644±93594±62*0.000 Awave0.55± ±0.13*0.000 E/A1.29± ±0.38*0.029 DT218±18216±")
95
Γενικά ΗΚΓφικά ευρήματα Η ΥΑΚ μπορεί να προκαλέσει 5 μείζονες ΗΚΓφικες μεταβολές: 1. Αύξηση QRS voltage 2. Αύξηση διάρκειας QRS 3. Αριστερή στροφή του άξονα 4. Διαταραχές επαναπολώσεως (ST-Τ) 5. Διαταραχές αριστερού κόλπου
 5. Διαταραχές αριστερού κόλπου.")
96
ΗΚΓφικά ΚΡΙΤΗΡΙΑ Sokolow R I +S III 2.5mV 21% - 89% Estes 5 points 15%- 100% Framingham LV strain+1vcriter 9% -100% LV strain 16%- 98% Cornell volt S V3 +R aVL> 2.8/2.0mV 16%- 97% Minnesota 3-1 Voltage 15%- 92% SV3+RaVL>2.4/2.0mV or LV strain or Estes>5 34%- 93% Schillaci G. Am.J.Card. 1994;74 Ευαισθ. Ειδικότ.

98
Epidemiology of LVH Prevalence varies widely depending on method of assessment and hypertension severity –Electrocardiographic LVH: 1 to 8% –Echocardiographic LVH: up to 60% (Adapted from Vasan RS, Levy D. Arch Intern Med. 1996:156:1789-1796. Mitchell GF et al Med Clin N. Am 1997:81(5);1247-1271)
; ).")
99
ΕΠΙΠΤΩΣΗ ΗΚΓ LVH ΣΤΗ ΜΕΛΕΤΗ FRAMINGHAM Kannel W. Am.J.Card.1987

100
Prevalence of LVH as a Function of 30- Year Average Systolic Blood Pressure Lauer MS et al. J Am Coll Cardiol. 1991;18:1287-1294. 0 0.2 0.4 <120120-129130-139140+ 30-Year Average Systolic Blood Pressure Age-adjusted Prevalence of LVH Women Men

101
12% Stage of HTN Stage of HTN Stage 1: SBP = 140–159; DBP = 90–99 8% Stage 3: SBP 180; DBP 110 Stage 2: BP = 160–179/100–110 10 20 30 80 90 100 3% Hypertensive patients (%) 90% 30% Prevalence of LVH in hypertension Tedesco MA et al. Clin Cardiol 2001;24:603–7. Schmieder RE et al. J Hum Hyperten 2000;14:597–604. Kahan T. J Hypertens 1998;16(suppl 7):23–29. Tedesco MA et al. Clin Cardiol 2001;24:603–7. Schmieder RE et al. J Hum Hyperten 2000;14:597–604. Kahan T. J Hypertens 1998;16(suppl 7):23–29.
:23–29. Tedesco MA et al. Clin Cardiol 2001;24:603–7. Schmieder RE et al. J Hum Hyperten 2000;14:597–604. Kahan T. J Hypertens 1998;16(suppl 7):23–29..")
104
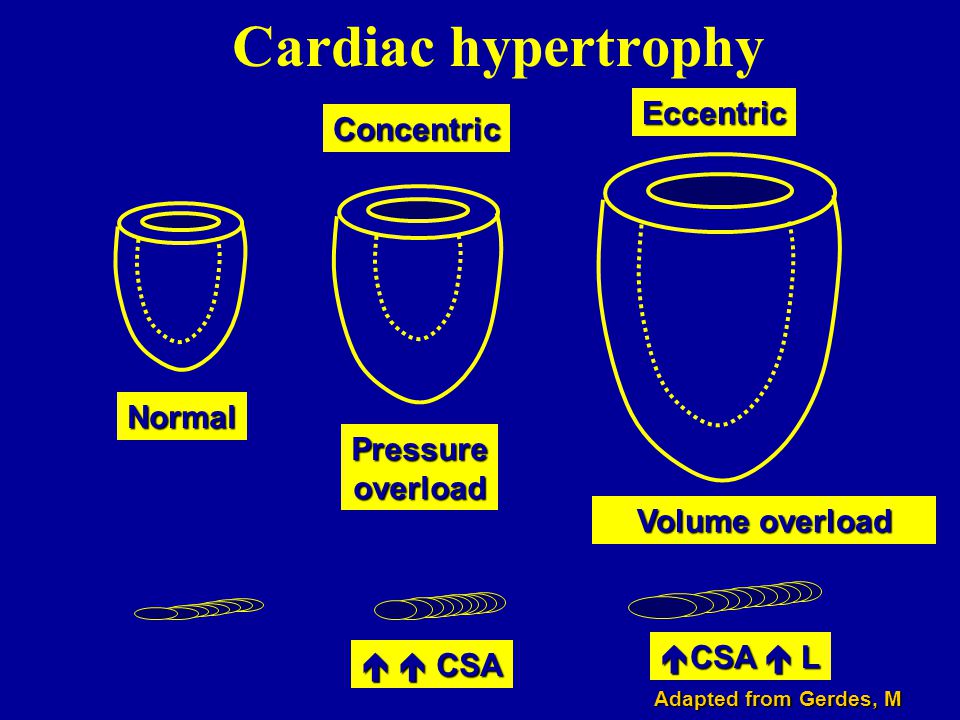
Cardiac hypertrophy Concentric Eccentric Normal Pressure overload Volume overload CSA CSA L Adapted from Gerdes, M

105
Aortic Stiffness Is an Independent Predictor of Primary Coronary Events in Hypertensive Patients Hypertension. 2002;39:10-15

106
Diastolic filling by Doppler echocardiography

107
LVH &Διαστολική Δυσλειτουργία E A Ε:0.86 ± 0.16 m/s Α:0.56 ±0.13 m/s Ε/Α:1.6 ± 0.5 DT:199 ± 32 ms IVRT:73 ± 13 ms

109
Progression from Hypertension to HF Years Normal LV Subclinical Clinical heart LV structure remodeling LV dysfunction failure & function Heart failure Obesity Diabetes HTN Smoking Dyslipidemia Diabetes Adapted from Vasan RS et al. Arch Intern Med. 1996,156:1789-1796. MI LVH Diastolic dysfunction Years/months Systolic dysfunction Death

110
LV Dysfunction: Mechanisms LV Pressure LV Volume Diastolic dysfunction Hypertension aging LVH Concentric remodeling Systolic dysfunction MI, CM, volume overload Hypertension Eccentric remodeling Mediators: angiotensin II, aldosterone, catecholamines, cytokines

111
Coronary Artery Disease (Ischemic Heart): Differentiation Between Hypertension and Atherosclerosis HypertensionAtherosclerosis LEFT VENTRICULAR HYPERTROPHYMYOCARDIAL ISCHEMIA Arteriolar Constriction Increased Afterload Coronary Insufficiency (Demand) Coronary Insufficiency (Demand) Sudden Death (Dysrhythmia) ( Acute LV Failure ) Sudden Death (Dysrhythmia) ( Acute LV Failure ) Congestive Heart Failure Congestive Heart Failure Myocardial Infarction Myocardial Infarction Sudden Death (Dysrhythmia) ( Acute Occlusion ) Sudden Death (Dysrhythmia) ( Acute Occlusion ) Coronary Insufficiency (Supply) Coronary Insufficiency (Supply) Lipid Deposition Arterial Occlusion (Adapted from Frohlich ED, Re RN Hurst’s the Heart. 1998:1635-1650, Frohlich ED et al N. Engl J Med. 1992:327(14):998-1008)
: ).")
112
Compensated concentric or eccentric hypertrophy Sustained pressure overload Mechanical stretch neurohormonal signalling Geneticfactors Co-morbidities MicrovascularabnormalitiesApoptosisnecrosis Ischaemia Cell loss Diastolicdysfunction Heart Failure Altered expression of contractilityregulatinggenes Systolicdysfunction Decompensated concentric hypertrophy Decompensated eccentric hypertrophy Development of heart failure in the hypertensive patient

113
Στεφανιαία Εφεδρεία & Αγγειακό Remodeling σε ΗΤΝ & LVH Στεφανιαία Εφεδρεία & Αγγειακό Remodeling σε ΗΤΝ & LVH Coronary Hemodynamic Characteristics n=68 48.1 ±3.2 2.8 ±0.1 2.9 ±0.2 69.8 ±6.8 56.1 ±13.1 -12.3 ±4.2 n=30 56.5 ±6.2 2.7 ±0.1 2.7 ±0.3 78.1 ±11.5 46.9 ±20.2 -11.3 ±5.4 n=13 81.1 ±9.9*† 2.3 ±0.2*† 1.7 ±0.3*‡ 99.3 ±29.0 1.5 ±20.5† -31.6 ±9.5 No.of patients CBF at baseline(ml/min) Coronary flow reserve to adenosine Coronary vascular resistance (mm Hg min/ml) CBF change induced by acetylcholine (min/ml) % change of CBF induced by Acetylcholine (%) % change of CAD induced by Acetylcholine (%) Group 3 Normotensive Group 2 Hypertensive Without LVH Group 1 Hypertensive With LVH Values are mean ± SE. CAD = coronary artery diameter; CBF = coronary blood flow; LVH = left ventricular hypertrophy. *p < 0.05 versus group 2; †p < 0.01; ‡<0.05 versus group 3. Hamasaki S. et al. J Am Coll Cardiol 2000.

114
8-Year Incidence of STROKE and TIA by LV Mass (Gr/m) MEN I: <98 II: 98-118 III: 119-144 IV: >144 WOMEN I: <76 II: 76-92 III: 93-112 IV: >112 Bikkina M. JAMA 1994;272:33-36

115
Incidence of CHF According to LVH Status Cupples LA et al. In: Kannel WB et al, eds. The Framingham Study. NHLBI; 1987: NIH Publication No. 87-2703. 0 10 20 30 40 50 60 No LVHBorderline LVH Definite LVH Age 35-64 Annual Rate/1000 Pts Men Women 0 10 20 30 40 50 60 No LVHBorderline LVH Definite LVH Age 65-94 Annual Rate/1000 Pts Men Women

116
Levy et al, Circulation, 1994: 90;1786-1793 Baseline Repolarization Abnormalities Two-year age-adjusted Incidence (%) 24 0 5 10 15 20 25 NoneMildSevere 5 6 10 9 14 Men Women CV Events as a Function of LVH
 NoneMildSevere Men Women CV Events as a Function of LVH")
117
ΣΥΜΒΑΜΑΤΑ & ΓΕΩΜΕΤΡΙΑ ΑΡΙΣΤΕΡΗΣ ΚΟΙΛΙΑΣ LVMI Relative wall thickness Event Rate Koren Ann.Intern.Med 1991;114:345

118
Cardiovascular events-free survival curves for patients divided into tertiles LVMI, according to the presence of concentric or eccentric geometry Muiesan, Agabiti Rosei et al, Hypertension 2004 in press )
")
119
0 40 10 20 30 1 tertile (LVMI < 91 g/m2) 2 tertile (LVMI 91-117 g/m2) 3 tertile (LVMI > 117 g/m2) 149+32 g/m2 75+11 g/m2 79+9 g/m2 104 + 7 g/m2 104 + 8 g/m2 141+21 g/m2 CV ev (%) RWT < 0.44 RWT > 0.44 * * § CV events according to LV geometry changes n° of patients 424; Follow-up 2-18 yrs, mean 6.4 yrs Muiesan, Agabiti Rosei et al, Hypertension 2004 in press * § § * vs eccentric geometry; § vs 1st tertile eccentric geometry
 2 tertile (LVMI g/m2) 3 tertile (LVMI > 117 g/m2) g/m g/m g/m g/m g/m g/m2 CV ev (%) RWT < 0.44 RWT > 0.44 * * § CV events according to LV geometry changes n° of patients 424; Follow-up 2-18 yrs, mean 6.4 yrs Muiesan, Agabiti Rosei et al, Hypertension 2004 in press * § § * vs eccentric geometry; § vs 1st tertile eccentric geometry")
120
Incidence of CV events (n/100pts/yr) Ganau A et al. J Am Coll Cardiol 1992
 Ganau A et al. J Am Coll Cardiol 1992")
121
LVH & Καρδιαγγειακά συμβάματα ΜελέτηΝLVH g/m²LVH(+)LVH(-) Casale 1986 140>1254.61.2 Levy 1989 3220>1162-3.30.8-1.4 Koren 1991 280>1251.4-6.30.1-2.2 Silberberg 1989 119>12515.29.6 Partrey 1990 104 IVS>1.4cm 15.34.8 Pittaras 2000,2004 812>125RR: 2.0
LVH(-) Casale > Levy > Koren > Silberberg > Partrey IVS>1.4cm Pittaras 2000, >125RR: 2.0")
122
Survival of Patients with and Without LVH N=812, Follow-up: 10 years No LVH LVH RR=2.0; p=0.0001 N=812 A.Pittaras et.al.Eur.Heart J.vol21,2000

123
Επίπτωση NSVT σε υπερτασικούς με LVH Loaldi 61 10% Aronow 196 15% Papademetriou 125 19% Mclenahon 50 28% Pringle 90 12% Μελέτη Ν NSVT Σύνολο 522 15.3%

124
Mild LVH in HTN: Is it really arrhythmogenic? Mild LVH in HTN: Is it really arrhythmogenic? Mild LVH among ambulatory hypertensives does not carry an additive arrhythmogenic risk and can be successfully reversed with the appropriate antihypertensive therapy, with no need of additional antiarrhythmic management. Gatzoulis K. et.al Am.J.Hypertension 2000

125
ΥΠΟΣΤΡΕΦΕΙ Η ΥΑΚ ΜΕ ΦΑΡΜΑΚΟΛΟΓΙΚΕΣ Η ΜΗ ΠΑΡΕΜΒΑΣΕΙΣ?

126
Υποστροφή LVH με αερόβια άσκηση * * p<0.05 Baseline16 weeks g/m2 Kokkinos,Narayan, Pittaras et al. N Engl J Med 1995;333:1462-7

128
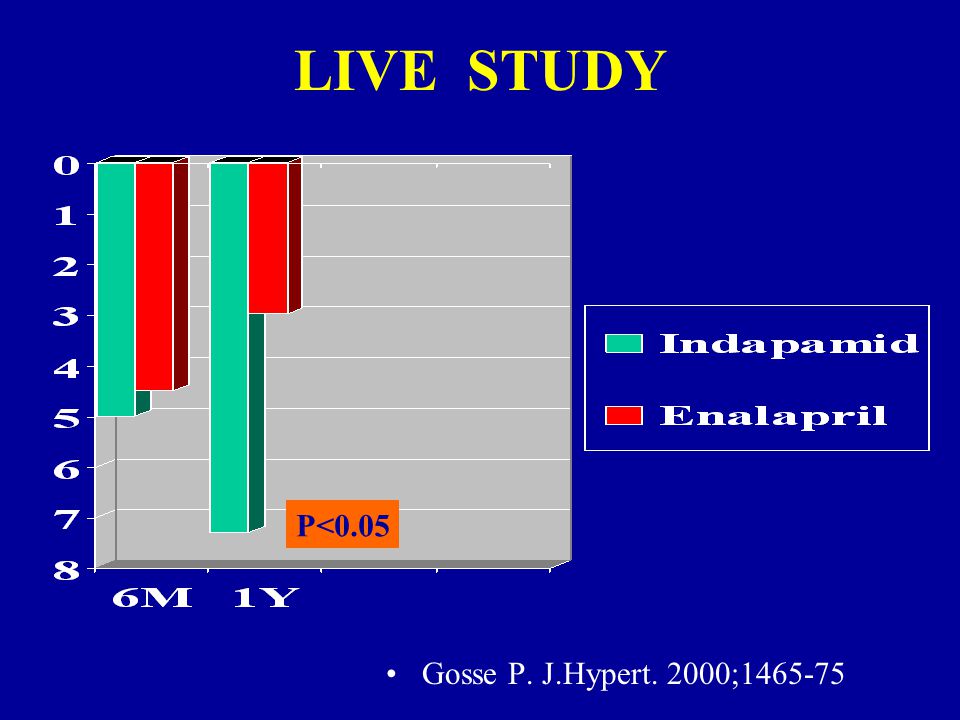
LIVE STUDY Gosse P. J.Hypert. 2000;1465-75 P<0.05

129
Μετανάλυση Μελετών Υποστροφής LVH στην Υπέρταση Schmieder 2001

130
Meta-analysis of randomized, controlled trials of LV hypertrophy regression in essential hypertension Schmieder RE et al. Am J Med 2003; 115:41-6. -16 -14 -12 -10 -8 -6 -4 -2 0 0 Diuretics -blockers Ca- antagonist Ca- antagonist ACE- inhibitors ACE- inhibitors ARBs -8% -6% -11% -10% -13% LV mass reduction (%) LV mass reduction (%) 80 randomized controlled trials; 4,113 patients
 LV mass reduction (%) 80 randomized controlled trials; 4,113 patients.")
131
Percent reduction of relative wall thickness during antihypertensive treatment Values are adjusted for differences between studies aDhlof B, Pennert K, Hansson L Am J H 1992; 5:95-110

132
ΥΠΟΣΤΡΟΦΗ ΥΑΚ ΚΑΙ ΚΑΡΔΙΑΓΓΕΙΑΚΑ ΣΥΜΒΑΜΑΤΑ Koren et al Am J Hypertens. 1991 Yurenev et al Am J Hypertens. 1992 Levy et al Circulation 1994 Muiesan et al Hypertension 1995 Devereux et al Am J Hypertens. 1996 Miser et al JACC 1996 Koren et al Am J Hypertens. 1991 Yurenev et al Am J Hypertens. 1992 Levy et al Circulation 1994 Muiesan et al Hypertension 1995 Devereux et al Am J Hypertens. 1996 Miser et al JACC 1996

133
Καρδιαγγειακά συμβάματα 2 χρόνων με ΗΚΓφικές αλλαγές LVH change Levy D. Circulation 1994;90:1786-93

134
Time to event (weeks) Verdecchia P et al. Circulation 1998;97:48–54. Probability of event-free survival (%) Probability of event-free survival (%) Regressors Non- Regressors Non- Regressors 40 50 60 70 80 90 100 0 0 200 300 400 500 Non-regressors (n = 60) Regressors (n = 52) p = 0.002 1 1 2 2 3 3 4 4 5 5 6 6 7 7 0 0 Rate of events (per 100 patient-years) Rate of events (per 100 patient-years) Regression of LVH predicts prognosis
 Probability of event-free survival (%) Regressors Non- Regressors Non- Regressors Non-regressors (n = 60) Regressors (n = 52) p = Rate of events (per 100 patient-years) Rate of events (per 100 patient-years) Regression of LVH predicts prognosis.")
135
Prognostic Value of Serial Changes in LV Mass (Echo) No LVH LVH LVHLVH Persistently Normal LV Mass LV Hypertrophy RegressionPersistently Increased LV Mass Koran M. et al 5/98 (5,1%) 1/28 (3,6%) 4/16 (25%) Mulasan ML. et al 4/78 (5,1%) 4/32 (12,5%) 13/34 (23%) Verdcchia P. et al 15/278 (5,4%) 3/48 (6,2%) 12/68 (21%) Cipriano C. et al 6/125 (4,8%) 5/52 (9,6%) 16/109 (15%) Total 30/579 (5,2%) 13/160(8,1%)45/217(20,7%)
 1/28 (3,6%) 4/16 (25%) Mulasan ML. et al 4/78 (5,1%) 4/32 (12,5%) 13/34 (23%) Verdcchia P. et al 15/278 (5,4%) 3/48 (6,2%) 12/68 (21%) Cipriano C. et al 6/125 (4,8%) 5/52 (9,6%) 16/109 (15%) Total 30/579 (5,2%) 13/160(8,1%)45/217(20,7%).")
136
Prognostic Value of Serial ECG Changes in the HOPE Study Κύρια συμβάματα Αιφνίδιος θάνατος Συγκοπή Κύρια και δευτερεύοντα συμβάματα Καρδιακή ανεπάρκεια

137
Impact of Changes in LVH on Development of Heart Failure in HOPE Comparison study of ramipril (n=336) vs placebo (n=406). Mathew J et al. Circulation. 2001;104:1615-1621. Days of Follow-Up P<.0001. 0.05.10.15.20.25 0500100015002000 Heart Failure Development/persistence of LVH Regression/prevention of LVH

138
Υποστροφή LVH και Αρρυθμίες Μείωση Αρρυθμιών Gonzales-Fernadez et al Am J Hypert. 1993 Χωρίς μεταβολές Mayet et al Am J Hypert. 1997 Manolis et al Am J Hypert. 1998

139
The L osartan I ntervention F or E ndpoint Reduction in Hypertension Study Dahlöf B et al Lancet 2002;359:995-1003. Steering Committee Chair: Co-chair: B. Dahlöf R.B. Devereux

140
Παρόμοιες Μειώσεις στην Αρτηριακή Πίεση 061218243036424854 Μήνες 40 50 60 70 80 90 100 110 120 130 140 150 160 170 180 Συστολική Διαστολική Μέση Πίεση mmHg Atenolol 145.4 mmHg Losartan 144.1 mmHg Atenolol 80.9 mmHg Losartan 81.3 mmHg Dahlöf B et al Lancet 2002;359:995-1003. Atenolol 102.4 mmHg Losartan 102.2 mmHg

141
Υποστροφή LVH Συγκριτικά με τις Αρχικές Τιμές -18 -16 -14 -12 -10 -8 -6 -4 -2 0 Cornell ProductSokolow-Lyon Μέση μεταβολή από τις αρχικές τιμές (%) LosartanAtenolol p<0.0001 Dahlöf B et al Lancet 2002;359:995-1003. 10.2 % 9.0 % 15.3 % 4.4 % p<0.0001

142
0 2 4 6 8 10 12 14 16 Ποσοστό ασθενών που εμφάνισαν το πρώτο σύμβααμα (%) Συνδυασμός καρδιαγγειακού θανάτου, εγκεφαλικού επεισοδίου και εμφράγματος του μυοκαρδίου Losartan Atenolol Συνολικός Πρωταρχικός Στόχος Μήνες0612182430364248546066 Losartan (n)46054524446043924312424741894112404738971889901 Atenolol (n)45884494441443494289420541354066399238211854876 Με Στατιστική Προσαρμογή 13.0% p=0.021 Χωρίς Στατιστική Προσαρμογή 14.6%, p=0.009 Dahlöf B et al Lancet 2002;359:995- 1003. Αριθμός Ασθενών σε Κίνδυνο

143
Εγκεφαλικά Επεισόδια Losartan Atenolol Με Στατιστική Προσαρμογή 24.9%, p=0.001 Χωρίς Στατιστική Προσαρμογή 25.8%, p=0.0006 Μήνες 0612182430364248546066 0 1 2 3 4 5 6 7 8 Dahlöf B et al Lancet 2002;359:995- 1003. Losartan 4605 4528 4469 4408 4332 4273 4224 4166 4117 3974 1928 925 Atenolol 4588 4490 4424 4372 4317 4245 4180 4119 4055 3894 1901 897 Θανατηφόρα και μη θανατηφόρα εγκεφαλικά επεισόδια Ποσοστό ασθενών που εμφάνισαν το πρώτο σύμβααμα (%) Αριθμός ασθενών σε κίνδυνο
 Αριθμός ασθενών σε κίνδυνο.")
144
Proportion of patients with first event (%) Proportion of patients with first event (%) 0 0 2 2 4 4 6 6 8 8 10 12 14 16 0 0 6 6 12 18 24 30 36 42 48 54 60 66 Adjusted Risk Reduction: 13.0%, p = 0.021 Time (months) Change from baseline (%) in LVH determined by electrocardiography Change from baseline (%) in LVH determined by electrocardiography -18 -16 -14 -12 -10 -8 -6 -4 -2 0 0 p < 0.0001 4.4% 10.2% 15.3% 9.0% Atenolol Losartan Atenolol Losartan Dahlöf B et al. Lancet 2002;359:995–1003. LIFE: LVH regression and primary endpoint Atenolol Losartan Cornell Voltage-Duration Product Sokolow-Lyon Voltage Composite of CV Death, stroke and MI

145
Losartan Intervention For End Point Prevention (LIFE) Echocardiographic Substudy N=960
 Echocardiographic Substudy N=960")
146
LVM in Patients with or without Composite End-Point: LIFE Year in LIFE LV Mass (g) All p<0.05 to <0.001
 All p<0.05 to <0.001")
147
LVM in Patients with or without Cardiovascular Death: LIFE Year in LIFE LV Mass (g) All p<0.05 to p=0.001 except year 4
 All p<0.05 to p=0.001 except year 4")
148
LVM σε ασθενείς καρδιαγγειακό θάνατο : LIFE STUDY Year in LIFE LV Mass (g) All p<0.05 to p=0.001 except year 4
 All p<0.05 to p=0.001 except year 4")
149
LV Mass in Patients with or without STROKE : LIFE Year in LIFE * LV Mass (g) P=0.11 p=0.17 p=0.20 p=0.11 p=0.02
 P=0.11 p=0.17 p=0.20 p=0.11 p=0.02")
150
Change in diastolic LV filling in the LIFE study Watchell et al Circulation 2002

151
Progression from Hypertension to HF Years Normal LV Subclinical Clinical heart LV structure remodeling LV dysfunction failure & function Heart failure Obesity Diabetes HTN Smoking Dyslipidemia Diabetes Adapted from Vasan RS et al. Arch Intern Med. 1996,156:1789-1796. MI LVH Diastolic dysfunction Years/months Systolic dysfunction Death

152
Υπέρταση : ένας μείζων παράγοντας κινδύνου για Συμφορητική Καρδιακή Ανεπάρκεια (CHF) ΥπέρτασηΥπέρταση LVH ΟΕΜ ΔιαστολικήΔυσλ/ργία ΣυστολικήΔυσλ/ργία CHF Θάνατος Θάνατος Αναδιαμόρφωση (Remodelling) της Αριστ.Κοιλίας Υποκλινική δυσλειτουργί α της Αρ.Κοιλίας Έκδηλη Καρδ.Ανεπάρκεια Χρόνος : δεκαετίες Χρόνος : μήνες ΚάπνισμαΔυσλιπιδαιμίαΔιαβήτης Παχυσαρκία Σ. Διαβήτης

153
A GROWING BURDEN Source: Vital Statistics of the United States, National Center for Health Statistics ΘΑΝΑΤΟΙ ΑΠΟ ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ 1979-1997 (USA)
")
154
ΚΟΣΤΟΣ ΚΑ ΣΕ ΝΟΣΗΛΕΙΕΣ 1997: 957,000 Νοσηλείες για ΚΑ $52.6 billion * (U.S. Health & Human Services, Vital and Health Statistics: National Hospital Discharge Survey: Annual Summary, 1997. Series 13: No.144. December 1999) (Health Care Financing Administration. Health Care Financing Review, Statistical Supplement: 1999. Cited by: American Heart Association. 2001 Heart and Stroke Statistical Update. Dallas, Texas: AHA, 2000) *Based on average Medicare payment per beneficiary of $5,501 per discharge.
 (Health Care Financing Administration. Health Care Financing Review, Statistical Supplement: Cited by: American Heart Association Heart and Stroke Statistical Update. Dallas, Texas: AHA, 2000) *Based on average Medicare payment per beneficiary of $5,501 per discharge..")
155
E. FREIS 1912-2005 The father of the first multicenter, double- blinded, random trial of cardiovascular drugs, VA Cooperative Study on Antihypertensive Agents

156
The VA Cooperative Study, 1967: ΣΥΜΒΑΜΑΤΑ Placebo n=70 Active Rx* n=73 Accelerated hypertension120 Stroke41 Coronary event20 CHF20 Renal damage20 Deaths40 VA Cooperative Study Group. JAMA. 1967;202:1028-1034. *P<0.001 active drug therapy vs placebo

157
Placebo n=194 Active Rx* n=186 Accelerated hypertension40 Stroke205 Total coronary event1311 Fatal coronary event116 ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ110 Renal damage30 Deaths198 The VA Cooperative Study, 1970: ΣΥΜΒΑΝΤΑ VA Cooperative Study Group. JAMA. 1970;213:1143-1152. *P<0.001 active drug therapy vs placebo

158
Major hypertension outcome trials Relative Risk of Event (%) in comparison to Placebo Mean BP at entry, mmHg Isolated systolic hypertension Age range No. of patient s Trial name EWPHE STOP I MRC STONE Strok e CAD CHF All CV 840 1627 4396 1632 > 60 70 – 84 65 – 74 60 – 79 182/101 195/102 185/ 91 169/ 98 64 53 75 43 82 87 81 86 78 49 – 32 71 60 83 41 Systolic and diastolic hypertension SHEP4736 4695 60 – 79 > 60 170/ 77 174/ 86 63 58 75 70 – 71 68 71

159
UKPDS :ΣΥΓΚΡΙΣΗ ΕΝΤΑΤΙΚΗΣ ΜΕ ΧΑΛΑΡΗ ΡΥΘΜΙΣΗ ΑΠ Endpoint % Relative risk reduction P value Any diabetes-related endpoint Diabetes-related deaths 24 32 0.005 0.02 ΚΑΡΔ. ΑΝΕΠΑΡΚΕΙΑ Stroke Myocardial infarction 56 44 21 0.004 0.01 NS Microvascular complications Retinopathy progression Deterioration of vision 37 34 47 0.009 0.004 *n=758 (mean achieved blood pressure of 144/82 mmHg) † n=390 (mean achieved blood pressure of 154/87 mmHg) UKPDS Group. BMJ. 1998;317:703–713.
 † n=390 (mean achieved blood pressure of 154/87 mmHg) UKPDS Group. BMJ. 1998;317:703–713..")
160
Cumulative CHF Rate Years to HF 01234567 0.03.06.09.12.15 Cumulative Event Rates for Heart Failure by ALLHAT Treatment Group HR (95% CI)p value A v C 1.38 (1.25-1.52)<.001 L v C 1.19 (1.07-1.31)<.001 ALLHAT Chlorthalidone Amlodipine Lisinopril
p value A v C 1.38 ( )<.001 L v C 1.19 ( )<.001 ALLHAT Chlorthalidone Amlodipine Lisinopril")
Παρόμοιες παρουσιάσεις




 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")




>")













