Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
DEBATE: MEMA μετά την αποσωλήνωση (pro/con) Αθ. Πρεκατές Πνευμονολόγος Δ/ντής ΜΕΘ
 Αθ. Πρεκατές Πνευμονολόγος Δ/ντής ΜΕΘ")
2
Nava S. ICM 2006;32:361-70

3
ΜΕMA TO PREVENT TO AVOID INTUBATION ALTERNATIVE TO INVASIVE VENTILATION

4
DEBATE: MEMA μετά την αποσωλήνωση (pro/con) 15% - 35% 15% - 35% των ασθ. που είναι σε Μ.Α. αποτυγχάνουν στο αρχικό SBT [40% του ολικού τους χρόνου στον ΜΑ δαπανάται για το weaning, (60% σε COPD)] Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):198-208.
] Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):")
5
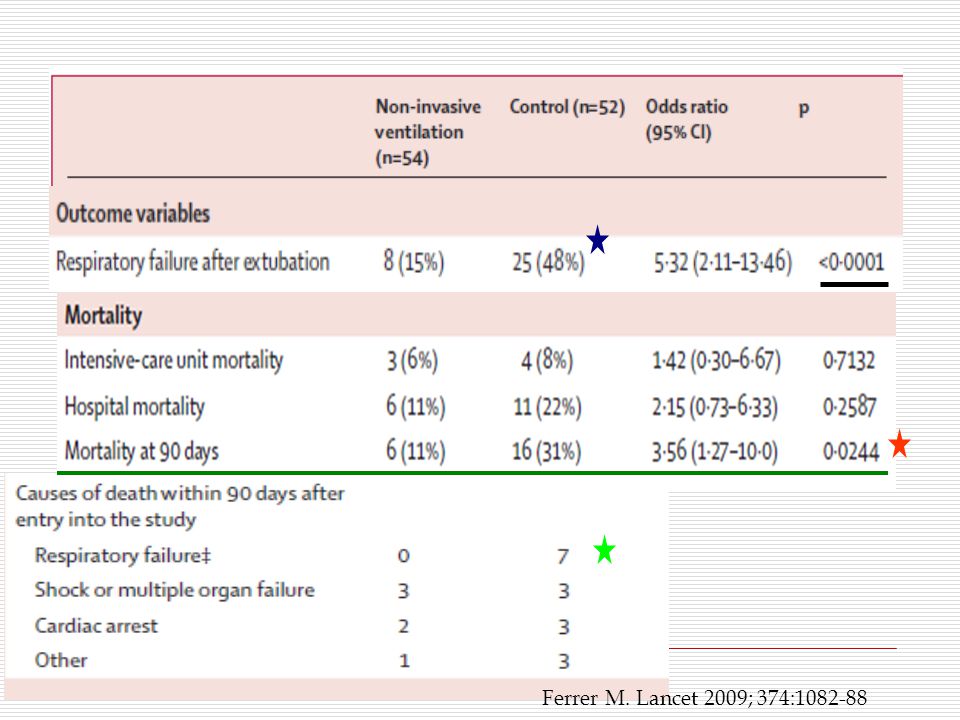
DEBATE: MEMA μετά την αποσωλήνωση (pro/con) Μετά από μία προγραμματισμένη αποσω- λήνωση, η επαναδιασωλήνωση απαντά στο 6-23% των ασθενών, εντός 48-72 ωρών Η επαναδιασωλήνωση αποτελεί από μόνη της ένα ανεξάρτητο παράγοντα κινδύνου Για την ανάπτυξη νοσοκομειακής πνευμονίας Για την αυξημένη θνητότητα και Για την μακρά νοσηλεία στο νοσοκομείο Ferrer M., Lancet 2009; 374: 1082–88
 Μετά από μία προγραμματισμένη αποσω- λήνωση, η επαναδιασωλήνωση απαντά στο 6-23% των ασθενών, εντός ωρών Η επαναδιασωλήνωση αποτελεί από μόνη της ένα ανεξάρτητο παράγοντα κινδύνου Για την ανάπτυξη νοσοκομειακής πνευμονίας Για την αυξημένη θνητότητα και Για την μακρά νοσηλεία στο νοσοκομείο Ferrer M., Lancet 2009; 374: 1082–88")
6
MEMA μετά την αποσωλήνωση A.ΜΕΜΑ για Διευκόλυνση του Δύσκολου weaning και αποδιασωλήνωσης B.ΜΕΜΑ για να θεραπεύσει την αποτυχία της αποδιασωλήνωσης

7
A.ΜΕΜΑ για Διευκόλυνση του Δύσκολου weaning και αποδιασωλήνωσης Διευκόλυνση του Δύσκολου weaning Nava RCT, 50 pts intubated, ARF λόγω COPD. Μετά 48 ώρες σε ΜΑ, απέτυχαν στο Τ-piece trial. Αλλοι αποδιασωληνώθηκαν και τέθηκαν σε NIV και άλλοι συνέχισαν στον ΜΑ και σε κανονικό weaning. Ιn NIV Higher weaning 88% vs 68% Shorter durations of MV (10.2 vs 16.6 days) LOS in ICU (15 vs 24 days) Improved 60-day survival rates (92% vs 72%, p < 0.05) Nava S. Ann Int Med 1998; 128:721-8
 LOS in ICU (15 vs 24 days) Improved 60-day survival rates (92% vs 72%, p < 0.05) Nava S. Ann Int Med 1998; 128:")
8
Nava S. Lancet 2009; 374:250-9

9
106 ασθ. (54 ασθ. σε ΜΕΜΑ και 52 control) Διασωληνώθηκαν για ARF Είχαν αποδεδειγμένα κριτήρια για τη διακοπή του MV, αλλά είχαν ανεπιτυχείς δοκιμές του SBT για 3 διαδοχικές ημέρες ΜΕΜΑ αμέσως μετά την αποδιασωλήνωση vs controls A. ΜΕΜΑ Διευκόλυνση του Δύσκολου weaning και αποδιασωλήνωσης Ferrer M. Lancet 2009; 374:1082-88
 Διασωληνώθηκαν για ARF Είχαν αποδεδειγμένα κριτήρια για τη διακοπή του MV, αλλά είχαν ανεπιτυχείς δοκιμές του SBT για 3 διαδοχικές ημέρες ΜΕΜΑ αμέσως μετά την αποδιασωλήνωση vs controls A. ΜΕΜΑ Διευκόλυνση του Δύσκολου weaning και αποδιασωλήνωσης Ferrer M. Lancet 2009; 374:")
10
A. ΜΕΜΑ Διευκόλυνση του Δύσκολου weaning και αποδιασωλήνωσης Ferrer M. Lancet 2009; 374:1082-88

11
14% 48%

14
A. Διευκόλυνση weaning και αποδιασωλήνωσης Ferrer M. Lancet 2009; 374:1082-88

15
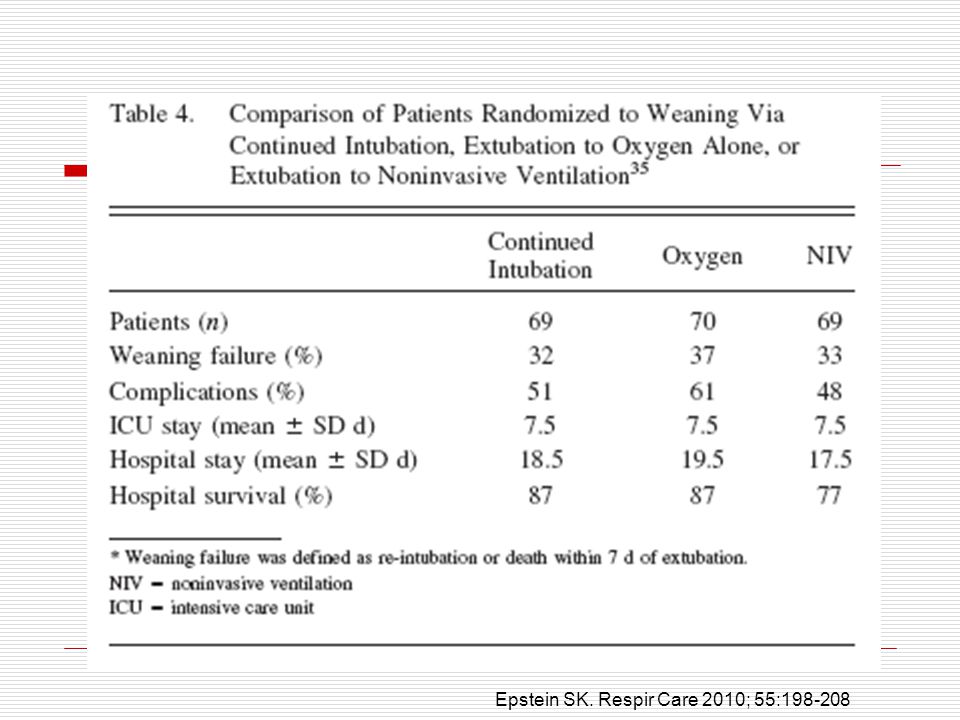
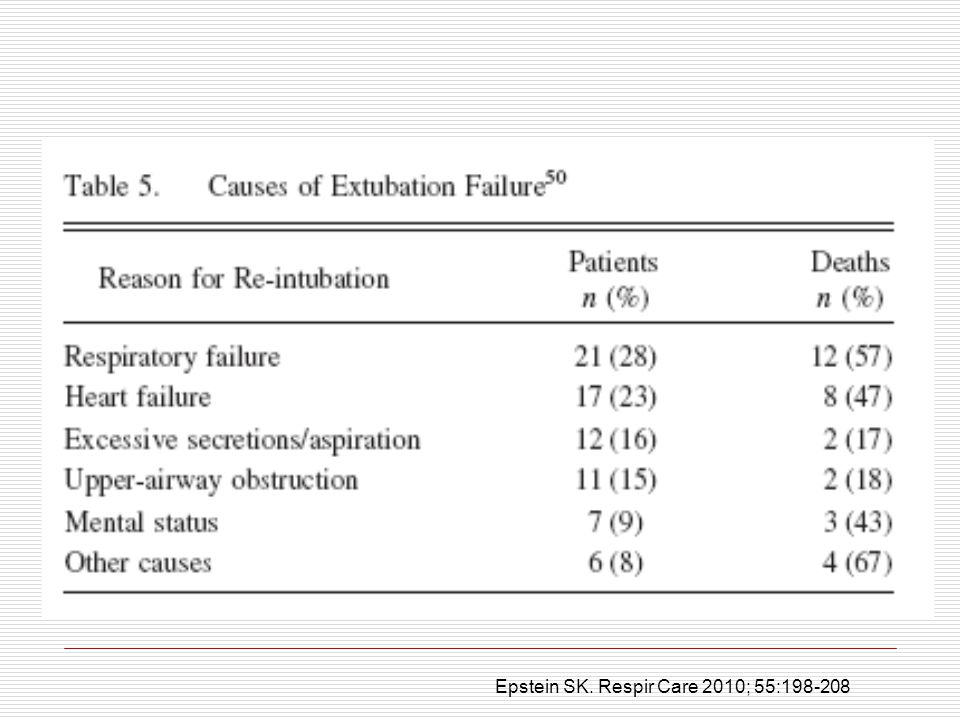
Epstein SK. Respir Care 2010; 55:198-208

16
A. Διευκόλυνση weaning και αποδιασωλήνωσης Διευκόλυνση weaning Girault 33 pts, acute on chronic respiratory failure to remain intubated or to be intubated to NPPV, after failure of a 2- hour T-piece trial Shorter duration of intubation, but total duration of MV was longer in NPPV. Weaning and Mortality rates in ICU and Hospital LOS were similar between the groups Girault C. AJRCCM 1999; 160:86-92

17
Β. ΜΕΜΑ για να θεραπεύσει την αποτυχία της αποδιασωλήνωσης

18
Esteban NEJM 2004; 350:2452-60

19
Esteban NEJM 2004; 350:2452-60

20
Esteban NEJM 2004; 350:2452-60

21
Esteban NEJM 2004; 350:2452-60

23
NIV (114 pts) Control (107 pts) Reintubation48% Rate of death25% Median time from respiratory failure to reintubation12 h 48% 14% (RR=1.78 ; 95 %, 1.03 to 3.20; p=0.048) 2 hs 30 min, p=0.02 ) Esteban NEJM 2004; 350:2452-60
 Control (107 pts) Reintubation48% Rate of death25% Median time from respiratory failure to reintubation12 h 48% 14% (RR=1.78 ; 95 %, 1.03 to 3.20; p=0.048) 2 hs 30 min, p=0.02 ) Esteban NEJM 2004; 350:")
25
Keenan SP. JAMA 2002; 287:3238-44

27
NIVControl

28
Keenan SP. JAMA 2002; 287:3238-3244

29
A RCT by Keenan et al. δεν έδειξε όφελος με την εφαρμογή του ΜΕΜΑ COPDΛιγότερο από το 10 % των ασθ. με ΜΕΜΑ είχαν τη διάγνωση του COPD Καρδιακή νόσος Καρδιακή νόσος ήταν η κύρια διάγνωση, αλλά δεν είναι σαφές αν το καρδιογενές πνευμονικό οίδημα ήταν παρόν ή όχι Keenan SP, et al. JAMA 2002;287:3238-44, Esteban NEJM 2004; 350:2452-60.

30
Con Con – Πλείστοι ασθενείς ήταν COPD Con Con – Οι ασθενείς πρέπει να επιλέγονται πολύ προσεκτικά (καλοί υποψήφιοι για ΜΕΜΑ) Con Con – Ασθενείς που έχουν δύσκολη διασωλήνωση Con Con – οι ασθενείς πρέπει να ανέχονται τα επίπεδα του PSV, που χρησιμοποιούνται μέσω μάσκας μετά τη διασωλήνωση
 Con Con – Ασθενείς που έχουν δύσκολη διασωλήνωση Con Con – οι ασθενείς πρέπει να ανέχονται τα επίπεδα του PSV, που χρησιμοποιούνται μέσω μάσκας μετά τη διασωλήνωση")
31
Con - Η βαρύτητα της νόσου (π.χ. COPD) δεν είναι ομοιογενής - ποικίλει Con - ΜΕΜΑ στη βαριά παρόξυνση του COPD ασθ. βοηθά, αλλά στην ήπια παρόξυνση δεν βοηθά Keenan SP. Ann Int Med 2003; 138:861-870
 δεν είναι ομοιογενής - ποικίλει Con - ΜΕΜΑ στη βαριά παρόξυνση του COPD ασθ. βοηθά, αλλά στην ήπια παρόξυνση δεν βοηθά Keenan SP. Ann Int Med 2003; 138:")
32
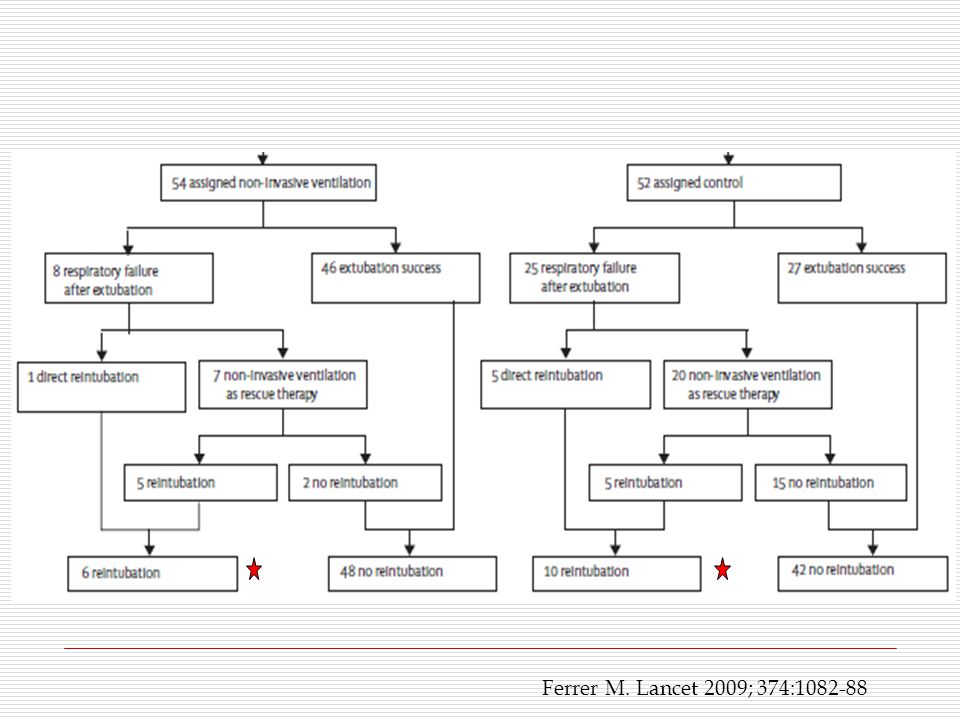
Con Con – Μικρός αριθμός ασθενών (ασθ. που ανέπτυξαν ARF μετά την αποδιασωλήνωση και δεν χρειάστηκαν άμεσα επαναδιασω- λήνωση), ο ΜΕΜΑ σαν rescue θεραπεία απέφυγε την επαναδιασωλήνωση σε 2/7 ασθ. που ήταν στο ΜΕΜΑ και σε 15/20 στο control Con - Crossover to NIV (control group) Ferrer M. Lancet 2009; 374:1082-88
, ο ΜΕΜΑ σαν rescue θεραπεία απέφυγε την επαναδιασωλήνωση σε 2/7 ασθ. που ήταν στο ΜΕΜΑ και σε 15/20 στο control Con - Crossover to NIV (control group) Ferrer M. Lancet 2009; 374:")
33
Con οφέλη Con - Subgroup analysis έδειξε ότι τα οφέλη του ΜΕΜΑ στην αύξηση της επιβίωσης ήταν περιορισμένα στους ασθ. με hypercapnia (PaCO2 >45 mm Hg) κατά τη διάρκεια της SBT πριν την αποσωλήνωση. Σ΄αυτήν την κατηγορία των ασθενών το 98% είχε υποκείμενη χρονία αναπνευστική νόσο Ferrer M. Lancet 2009; 374:1082-88
 κατά τη διάρκεια της SBT πριν την αποσωλήνωση. Σ΄αυτήν την κατηγορία των ασθενών το 98% είχε υποκείμενη χρονία αναπνευστική νόσο Ferrer M. Lancet 2009; 374:")
34
Εpstein SK. AJRCCM 1998; 158(2):489-93 Epstein SK. Respir Care 2010 Feb;55(2):198-208.
: Epstein SK. Respir Care 2010 Feb;55(2):")
35
Predictors of Success during Acute Applications of NIV Νέοι, Low APACHE II score Καλή συνεργασία με τον ασθενή - αναπνευστήρα Μικρή διαφυγή αέρα, καλή οδοντοστοιχία RR μεταξύ 25 – 35 / λεπτό Υπερκαπνία (PaCO2 > 45 αλλά < 92 mm Hg) Οξυαιμία (ΡΗ 7.10) Βελτίωση των αερίων αίματος, HR, RR στην 1 η ή 2 η ώρα του ΜΕΜΑ Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006: 433-471

36
i.a small volume of respiratory secretions ii.low scores on APACHE II iii.synchronous breathing iv.a good initial response in terms of Ph, PaCO2, and RR and v.the ability to protect the airway. Liesching T, et al. Chest 2003;124:699-713. Factors favoring the successful application of NIV

37
Timing of initiation του ΜΕΜΑ Timing of initiation of NIV is a another determinant of success

38
Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006: 433-471

39
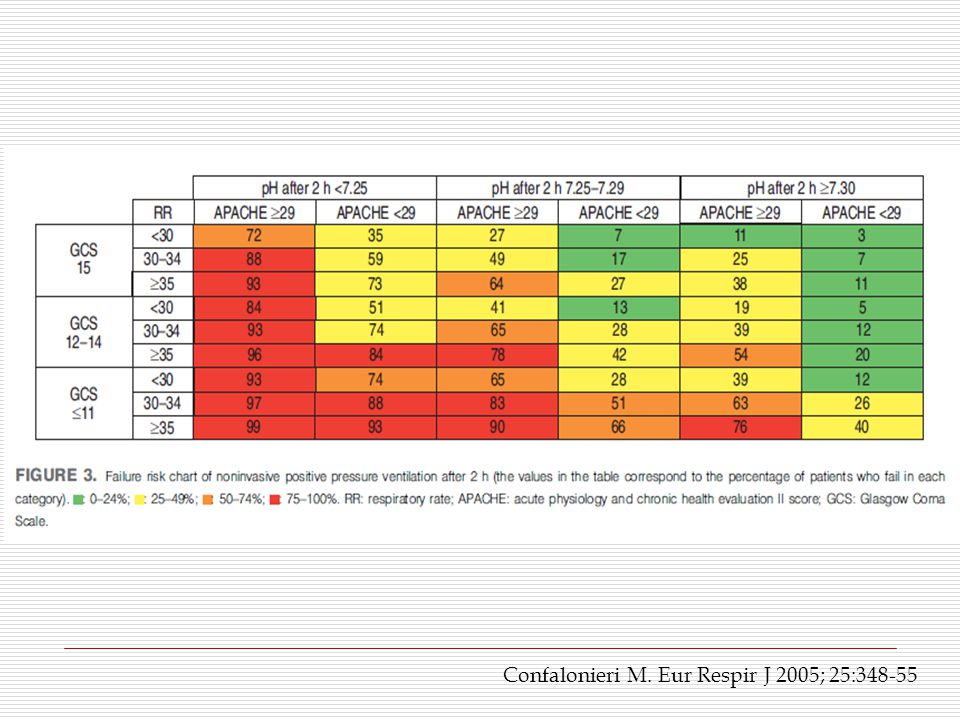
Confalonieri M. Eur Respir J 2005; 25:348-55

40
Κριτήρια Εισόδου στη μελέτη Confalonieri M. Eur Respir J 2005; 25:348-55

44
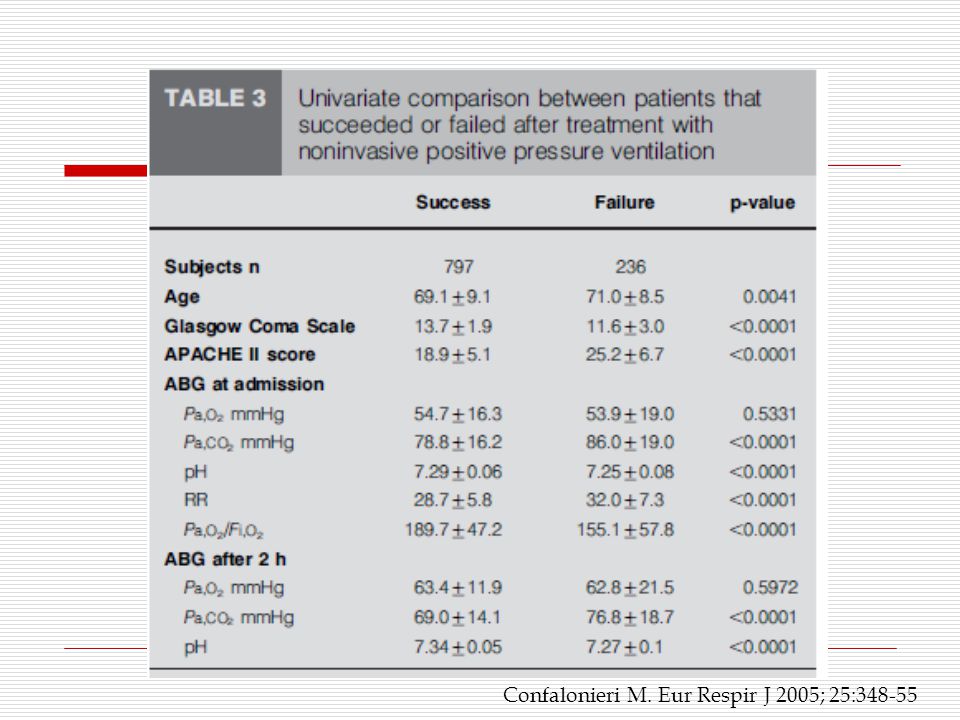
Predictors of Failure during Acute Applications of NIV Στην Εισαγωγή και 1 ή 2 ώρες μετά APACHE II score > 29 GCS < 11 PH < 7.25 RR > 35 / min Αν τα είχε όλα ο ασθενής στην αρχή η πιθανότητα της αποτυχίας στο ΜΕΜΑ ήταν 82% και μετά 2 ώρες ήταν 99% Confalonieri M. Eur Respir J 2005; 25:348-55

45
2 nd part

46
Selection Guidelines: NIV for pts with Acute Respiratory Failure Step 1. Aναγνώρισε αντιστρεπτή αιτία ARF που χρειάζεται βοήθεια (αν/στήρα) Αντιστρεπτή αιτία ARF (ως COPD, ACPO) Συμπτώματα και ενδείξεις οξείας αναπνευστικής δυσχέρειας Μέτρια ή σοβαρή δύσπνοια ή RR > 24 για COPD ή RR > 30 για ARF ή Χρήση επικουρικών μυών Διαταραχές των αερίων αίματος PaCO2 > 45 mmHg, PH < 7.35 PaO2/FiO2 < 200 Mecta S, Hill NS. AJRCCM 2001; 163:540-77
 Αντιστρεπτή αιτία ARF (ως COPD, ACPO) Συμπτώματα και ενδείξεις οξείας αναπνευστικής δυσχέρειας Μέτρια ή σοβαρή δύσπνοια ή RR > 24 για COPD ή RR > 30 για ARF ή Χρήση επικουρικών μυών Διαταραχές των αερίων αίματος PaCO2 > 45 mmHg, PH < 7.35 PaO2/FiO2 < 200 Mecta S, Hill NS. AJRCCM 2001; 163:")
47
Selection Guidelines: NIV for pts with Acute Respiratory Failure Step 2α. Απόλυτες Αντενδείξεις για εφαρμογή NIV Αναπνευστικό arrest Ανίκανος να δεχτεί τη μάσκα Mecta S, Hill NS. AJRCCM 2001; 163:540-77

48
Selection Guidelines: NIV for pts with Acute Respiratory Failure Step 2β. Σχετικές Αντενδείξεις Ασταθής (σόκ, ισχαιμία ή αρρυθμία...) Μη συνεργάσιμος, ανήσυχος Ανίκανος να προστατεύσει τους αεραγωγούς Υπερβολικές εκκρίσεις Πρόσφατο χειρουργείο στους άνω αεραγωγούς ή στο ανώτερο γαστρ/ρικό Mecta S, Hill NS. AJRCCM 2001; 163:540-77
 Μη συνεργάσιμος, ανήσυχος Ανίκανος να προστατεύσει τους αεραγωγούς Υπερβολικές εκκρίσεις Πρόσφατο χειρουργείο στους άνω αεραγωγούς ή στο ανώτερο γαστρ/ρικό Mecta S, Hill NS. AJRCCM 2001; 163:")
49
Βαθμονόμηση του ΝΙV σε Οξεία Αναπνευστική Ανεπάρκεια A. Ισχυρή μαρτυρία - Συνιστάται A.Παρόξυνση της COPD B.Οξύ καρδιογενές πνευμονικό οίδημα C.Ανοσοκαταστολή (αιματολογική κακοήθεια, μεταμόσχευση ΒΜ ή συμπαγούς οργ., AIDS) D.Διευκόλυνση weaning/αποδιασωλήνωσης σε ασθ. με COPD Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006: 433-471
 D.Διευκόλυνση weaning/αποδιασωλήνωσης σε ασθ. με COPD Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006:")
50
B.Ενδιάμεση μαρτυρία – Κατευθυντήριες Οδηγίες A.Ασθμα B.CAP σε ασθ. με COPD C.Aποτυχία αποδιασωλήνωσης σε COPD ασθ. D.Υποξαιμική Αναπνευστική Ανεπάρκεια E.Μη διασωληνωμένοι ασθ. (COPD και CHF) F.Μετεγχειρητική αναπν. ανεπάρκεια Βαθμονόμηση του ΝΙV σε Οξεία Αναπνευστική Ανεπάρκεια Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006: 433-471
 F.Μετεγχειρητική αναπν. ανεπάρκεια Βαθμονόμηση του ΝΙV σε Οξεία Αναπνευστική Ανεπάρκεια Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006:")
51
C.Αδύναμη μαρτυρία – προαιρετική A.ARDS με προσβολή ενός οργάνου B.CAP σε μη COPD ασθενή C.Κυστική ίνωση D.Διευκόλυνση weaning/αποδιασωλήνωσης σε μη COPD E.Νευρομυϊκή νόσος ή παραμόρφωση του θωρακικού τοιχώματος F.Αποφρακτική άπνοια-ύπνου G.Τραύμα, ή Απόφραξη ανωτέρων αεραγωγών Βαθμονόμηση του ΝΙV σε Οξεία Αναπνευστική Ανεπάρκεια Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006: 433-471

52
Βαθμονόμηση του ΝΙV σε Οξεία Αναπνευστική Ανεπάρκεια D.Δεν συνιστάται A.Βαρύ ARDS με ΜΟF B.Οξεία επιδείνωση της UIP τελικού σταδίου C.Μετεγχειρητικά σε εγχείρηση στον οισοφάγο ή στους ανώτερους αεραγωγούς D.Απόφραξη των ανωτέρων αεραγωγών με υψηλό κίνδυνο για απόφραξη Hill NS. Noninvasive Positive-Pressure Ventilation. Ed. Mc Graw Hill. 2 nd Ed. Principles and Practice of Mechanical Ventilation. Tobin MJ. 2006: 433-471

53
DEBATE: MEMA μετά την αποσωλήνωση (pro/con) Η υποκείμενη αιτιολογία και η πιθανή αναστρεψιμότητα Η υποκείμενη αιτιολογία και η πιθανή αναστρεψιμότητα της ARF αποτελούν σπουδαίες ορίζουσες στην επιλογή του ασθενούς και στον τύπο της μηχανικής υποστήριξης της αναπνοής «ΔΕΚΑΝΙΚΙ» (“crutch”), Η αντιστρεπτή αιτιολογία επιτρέπει τη χρήση του ΜΕΜΑ, σαν ένα «ΔΕΚΑΝΙΚΙ» (“crutch”), που βοηθά τον ασθενή, στο κρίσιμο αυτό χρονικό διάστημα (μετά την αποσωλήνωση), να δεχτεί την κατάλληλη θεραπεία για να αντιστρέψει την ARF
 Η υποκείμενη αιτιολογία και η πιθανή αναστρεψιμότητα Η υποκείμενη αιτιολογία και η πιθανή αναστρεψιμότητα της ARF αποτελούν σπουδαίες ορίζουσες στην επιλογή του ασθενούς και στον τύπο της μηχανικής υποστήριξης της αναπνοής «ΔΕΚΑΝΙΚΙ» ( crutch ), Η αντιστρεπτή αιτιολογία επιτρέπει τη χρήση του ΜΕΜΑ, σαν ένα «ΔΕΚΑΝΙΚΙ» ( crutch ), που βοηθά τον ασθενή, στο κρίσιμο αυτό χρονικό διάστημα (μετά την αποσωλήνωση), να δεχτεί την κατάλληλη θεραπεία για να αντιστρέψει την ARF")
54
Successful noninvasive-ventilation strategies require a program that includes a. the availability of well-trained staff b. careful selection of patients, and c. attention to patients’ responses to noninvasive ventilation. Truwit JD, Bernard GR. NEJM 2004; 350:24:2512-14

55
Ευχαριστώ πολύ

58
Noninvasive positive pressure ventilation in unplanned extubation BACKGROUND: Unplanned extubation is quite common in ICU pts receiving MV. The present study aimed to investigate the effectiveness of NIV in pts with unplanned extubation. MATERIALS AND METHODS: A total of 15 pts (12 male, age: 57 +/- 24 years, APACHE II score: 19 +/- 7) monitored at the medical ICU during the year 2004 who developed unplanned extubation were included in the study. NPPV was tried in all of them following unplanned extubation. Indications for admission to the ICU were as follows: 9 pts pneumonia, 3 status epilepticus, 1 with gastrointestinal bleeding, 1 with cardiogenic pulmonary edema and 1 with diffuse alveolar bleeding. RESULTS: 11 pts (74%) were at the weaning period at the time of unplanned extubation. Among these 11 pts, NPPV was successful in 10 (91%) and only one (9%) was reintubated due to the failure of NPPV. The remaining 4 pts (26%) had pneumonia and none of them were at the weaning period at the time of extubation, but their requirement for MV was gradually decreasing. Unfortunately, an NPPV attempt for 6-8 h failed and these patients were reintubated. CONCLUSIONS: Pts with unplanned extubation before the weaning criteria are met should be intubated immediately. On the other hand, when extubation develops during the weaning period, NPPV may be an alternative. The present study was conducted with a small number of patients, and larger studies on the effectiveness of NPPV in unplanned extubation are warranted for firm conclusions. Ervuksel E. Ann Thor Med 2009 Jan;4(1):17-20.
 monitored at the medical ICU during the year 2004 who developed unplanned extubation were included in the study. NPPV was tried in all of them following unplanned extubation. Indications for admission to the ICU were as follows: 9 pts pneumonia, 3 status epilepticus, 1 with gastrointestinal bleeding, 1 with cardiogenic pulmonary edema and 1 with diffuse alveolar bleeding. RESULTS: 11 pts (74%) were at the weaning period at the time of unplanned extubation. Among these 11 pts, NPPV was successful in 10 (91%) and only one (9%) was reintubated due to the failure of NPPV. The remaining 4 pts (26%) had pneumonia and none of them were at the weaning period at the time of extubation, but their requirement for MV was gradually decreasing. Unfortunately, an NPPV attempt for 6-8 h failed and these patients were reintubated. CONCLUSIONS: Pts with unplanned extubation before the weaning criteria are met should be intubated immediately. On the other hand, when extubation develops during the weaning period, NPPV may be an alternative. The present study was conducted with a small number of patients, and larger studies on the effectiveness of NPPV in unplanned extubation are warranted for firm conclusions. Ervuksel E. Ann Thor Med 2009 Jan;4(1):")
59
Factors predicting successful noninvasive ventilation in acute lung injury NIV has potential as an effective therapeutic method in patients with acute lung injury (ALI).The aims of this study were to determine factors predicting the need for endotracheal intubation in ALI patients treated with NIV, and to promote the selection of patients suitable for NIV. Methods. Ι CU of the Nippon Medical School Hospital from 2000 - 2006 with a diagnosis of ALI, in whom NIV was initiated. Results. A total of 47 patients with ALI received NIV, and 33 patients (70%) successfully avoided endotracheal intubation.Pts who required endotracheal intubation had a significantly higher APACHE II score and a signifi cantly higher Simplifi ed Acute Physiology Score (SAPS) II, and a significantly lower arterial pH. The respiratory rate decreased significantly within 1 h of starting NIV only in patients Successfully treated with NIV. An APACHE II score of more than 17 ( P = 0.022) and a respiratory rate of more than 25 breaths·min−1 after 1 h of NIV ( P = 0.024) were independent factors associated with the need for endotracheal intubation. Patients who avoided endotracheal intubation had a signifi cantly lower ICU mortality rate and in-hospital mortality rate than patients who required endotracheal intubation. Conclusion. We determined an APACHE II score of more than 17 and a respiratory rate of more than 25 breaths·min−1 after 1 h of NIV as factors predicting the need for endotracheal intubation in ALI patients treated with NIV. Y. YOSHIDA1. J Anesth (2008) 22:201–206
 successfully avoided endotracheal intubation.Pts who required endotracheal intubation had a significantly higher APACHE II score and a signifi cantly higher Simplifi ed Acute Physiology Score (SAPS) II, and a significantly lower arterial pH. The respiratory rate decreased significantly within 1 h of starting NIV only in patients Successfully treated with NIV. An APACHE II score of more than 17 ( P = 0.022) and a respiratory rate of more than 25 breaths·min−1 after 1 h of NIV ( P = 0.024) were independent factors associated with the need for endotracheal intubation. Patients who avoided endotracheal intubation had a signifi cantly lower ICU mortality rate and in-hospital mortality rate than patients who required endotracheal intubation. Conclusion. We determined an APACHE II score of more than 17 and a respiratory rate of more than 25 breaths·min−1 after 1 h of NIV as factors predicting the need for endotracheal intubation in ALI patients treated with NIV. Y. YOSHIDA1. J Anesth (2008) 22:201–206.")
60
We determined an APACHE II score of more than 17 and a respiratory rate of more than 25 breaths·min−1 after 1 h of NIV as factors predicting the need for endotracheal intubation in ALI patients treated with NIV. Y. YOSHIDA1. J Anesth (2008) 22:201–206
 22:201–206.")
61
The longer re-intubation is delayed, the higher the mortality. In evaluating the impact of re-intubation, a prospective study by Epstein et al found that almost 30% of pts experienced an important complication associated with the re-intubation process The observed complications included development of pneumonia (18%), arrhythmia (4%), atelectasis or lobar collapse (4%), acute myocardial infarction (3%), and stroke (3%) 31 of the 74 re-intubated pts (42%) died, versus 12% of the cohort not re-intubated Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):198-208.
, arrhythmia (4%), atelectasis or lobar collapse (4%), acute myocardial infarction (3%), and stroke (3%) 31 of the 74 re-intubated pts (42%) died, versus 12% of the cohort not re-intubated Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):")
62
Μειονεκτήματα των μελετών Crossover to NIV in the control group and reported “failure” as a surrogate for actual endotracheal intubation HOW and WHERE NIV was applied Interface (nasal vs face mask) Ventilations (volume cycled vs pressure cycled) Ventilators (conventional mechanical ventilators vs ventilators for NIV) Delays of up 24-48 hours from the time of admission to NIV Keenan SP. Ann Int Med 2003; 138:861-870

63
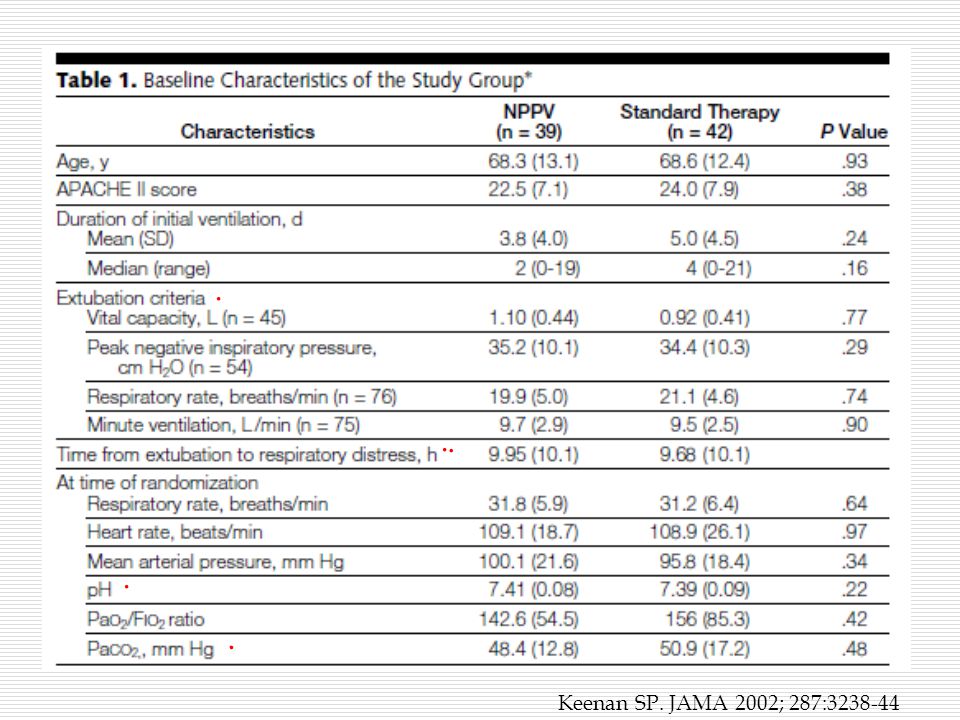
Noninvasive Positive-Pressure Ventilation for Postextubation Respiratory Distress The ICU and hospital lengths of stay and hospital mortality did not differ. This randomized trial suggests that the routine use of NPPV for all patients who develop respiratory distress after Extubation is not effective. Keenan SP. JAMA 2002; 287:3238-3244

64
Successful noninvasive-ventilation strategies require a program that includes a. the availability of well-trained staff b. careful selection of patients, and c. attention to patients’ responses to noninvasive ventilation. Noninvasive ventilation appears best suited to patients with COPD, those with cardiogenic pulmonary edema, those who have just undergone lung surgery, and those who are immunosuppressed and have bilateral infiltrates. Truwit JD, Bernard GR. NEJM 2004; 350:24:2512-14

65
CCM 2008 - Volume 36 (10) pp 2766-2772 Predictors of noninvasive ventilation failure in patients with hematologic malignancy and acute respiratory failure * Adda, Mélanie MD; Coquet, Isaline MD; Darmon, Michaël MD; Thiery, Guillaume MD; Schlemmer, Benoît MD; Azoulay, Élie MD, PhD Abstract Objectives: The current trend to manage critically ill hematologic patients admitted with acute respiratory failure is to perform noninvasive ventilation to avoid endotracheal intubation. However, failure of noninvasive ventilation may lead to an increased mortality. Design: Retrospective study to determine the frequency of NIV failure and identify its determinants.Setting: Medical intensive care unit in a University hospital. Patients: All consecutive pts with hematologic malignancies admitted to the intensive care unit over a 10-yr period who received noninvasive ventilation. Results: 99 pts were studied. SAPS II at admission was 49 (39-57). 53 pts (54%) failed noninvasive ventilation and required endotracheal intubation. Their Pao 2 /Fio 2 ratio was significantly lower (175 [101-236] vs. 248 [134-337]) and their RR under NIV was significantly higher (32 br/min [30-36] vs. 28 [27-30]). 47 pts (89%) who failed noninvasive ventilation required vasopressors. Hospital mortality was 79% in those who failed noninvasive ventilation, and 41% in those who succeeded. Patients who failed noninvasive ventilation had a significantly longer intensive care unit stay (13 days [8-23] vs. 5 [2-8]) and a significantly higher rate of intensive care unit-acquired infections (32% compared with 7%). Factors independently associated with noninvasive ventilation failure by multivariate analysis were respiratory rate under noninvasive ventilation, longer delay between admission and noninvasive ventilation first use, need for vasopressors or renal replacement therapy, and acute respiratory distress syndrome. Conclusions: Failure of noninvasive ventilation occurs in half the critically ill hematologic patients and is associated with an increased mortality. Predictors of noninvasive ventilation failure might be used to guide decisions regarding intubation.
. 53 pts (54%) failed noninvasive ventilation and required endotracheal intubation. Their Pao 2 /Fio 2 ratio was significantly lower (175 [ ] vs. 248 [ ]) and their RR under NIV was significantly higher (32 br/min [30-36] vs. 28 [27-30]). 47 pts (89%) who failed noninvasive ventilation required vasopressors. Hospital mortality was 79% in those who failed noninvasive ventilation, and 41% in those who succeeded. Patients who failed noninvasive ventilation had a significantly longer intensive care unit stay (13 days [8-23] vs. 5 [2-8]) and a significantly higher rate of intensive care unit-acquired infections (32% compared with 7%). Factors independently associated with noninvasive ventilation failure by multivariate analysis were respiratory rate under noninvasive ventilation, longer delay between admission and noninvasive ventilation first use, need for vasopressors or renal replacement therapy, and acute respiratory distress syndrome. Conclusions: Failure of noninvasive ventilation occurs in half the critically ill hematologic patients and is associated with an increased mortality. Predictors of noninvasive ventilation failure might be used to guide decisions regarding intubation..")
66
In pts with respiratory failure, non- invasive ventilation as rescue therapy avoided reintubation in 17 of 27 patients. Non-invasive ventilation was independently associated with a lower risk of respiratory failure after extubation (adjusted odds ratio 0 ⋅ 17 [95% CI 0 ⋅ 06– 0 ⋅ 44]; p<0 ⋅ 0001). 90-day mortality was lower in patients assigned non-invasive ventilation than in those allocated conventional oxygen (p=0 ⋅ 0146).
. 90-day mortality was lower in patients assigned non-invasive ventilation than in those allocated conventional oxygen (p=0 ⋅ 0146)..")
67
Β. NIV να θεραπεύσει την αποτυχία της αποδιασωλήνωσης Patients who fail extubation and undergo re-intubation have longer mechanical ventilation more associated morbidity, and higher mortality than those not requiring reintubation, this may be because they had higher severity of illness at the time of extubation, experienced worsening respiratory failure while extubated, or experienced additional injury associated with the reintubation process Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):198-208.
:")
68
Β. NIV να θεραπεύσει την αποτυχία της αποδιασωλήνωσης Ebstein (-) jiang (-) Esteban (-) keenan
 jiang (-) Esteban (-) keenan.")
70
Some data do support the use of noninvasive ventilation in patients who have acute exace- rbations of asthma, pneumonia, hypoxic respi- ratory failure, trauma, or the acute respiratory distress syndrome and patients who have restrictive lung disease and are acutely ill.1,13 However, because the evidence is insufficient at this time, the use of noninvasive ventilation in these populations cannot be uniformly recommended. Additional selection criteria include moderate-to-severe respiratory distress, tachypnea, accessory-muscle use, asynchronous chest–abdominal muscle use, hypercapnia, and moderate acidosis. Truwit JD, Bernard GR. NEJM 2004; 350:24:2512-14

71
Ferrer M. Lancet 2009; 374:1082-88

72
Many believe that with patients who fairly narrow have acute respiratory distress there is a fairly narrow window of opportunity window of opportunity for the use of noninvasive ventilation; they need to be sick enough for intervention but not sick enough to require immediate intubation. The initial six-to-eight-hour period of noninvasive ventilation is resource-intensive, and failure to intubate a patient who does not have a response is associated with increased mortality. Truwit JD, Bernard GR. NEJM 2004; 350:24:2512-14

73
Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):198-208.
:")
74
Should a patient be extubated and placed on noninvasive ventilation after failing a spontaneous breathing trial? Extubation failure resulting in re- intubation is associated with higher mortality, and this mortality risk increases with delay of re-intubation and may not be prevented by application of NIV. Patients extubated to NIV must have careful monitoring by skilled clinicians able to provide timely re-intubation if the patient shows signs of intolerance or worsening respiratory failure. Epstein SK, Durbin CGJr. Respir Care 2010 Feb;55(2):198-208.
:")
75
Severe hypercapnia or acidemia αποτυχία Στους ασθενείς με Severe hypercapnia or acidemia είναι πολύ πιθανό να συμβεί αποτυχία στην εφαρμογή του ΜΕΜΑ Οι ίδιες μελέτες δείχνουν την έλλειψη βελτίωσης της αναπνευστικής οξέωσης και των RR κατά τη διάρκεια των πρώτων ωρών του ΜΕΜΑ. Thorax 2001; 56:708-12, CCM 1994; 22:1253-61

76
Who May Benefit and Where Should Noninvasive Weaning Be Attempted?

77
Lightoweler et al. BMJ 2003

78
Ferrer M. Lancet 2009; 374:1082-88

79
Epstein SK. Respir Care 2010; 55:198-208

80
Epstein SK. AJRCCM 1998; 158(2):489-93
:489-93")
81
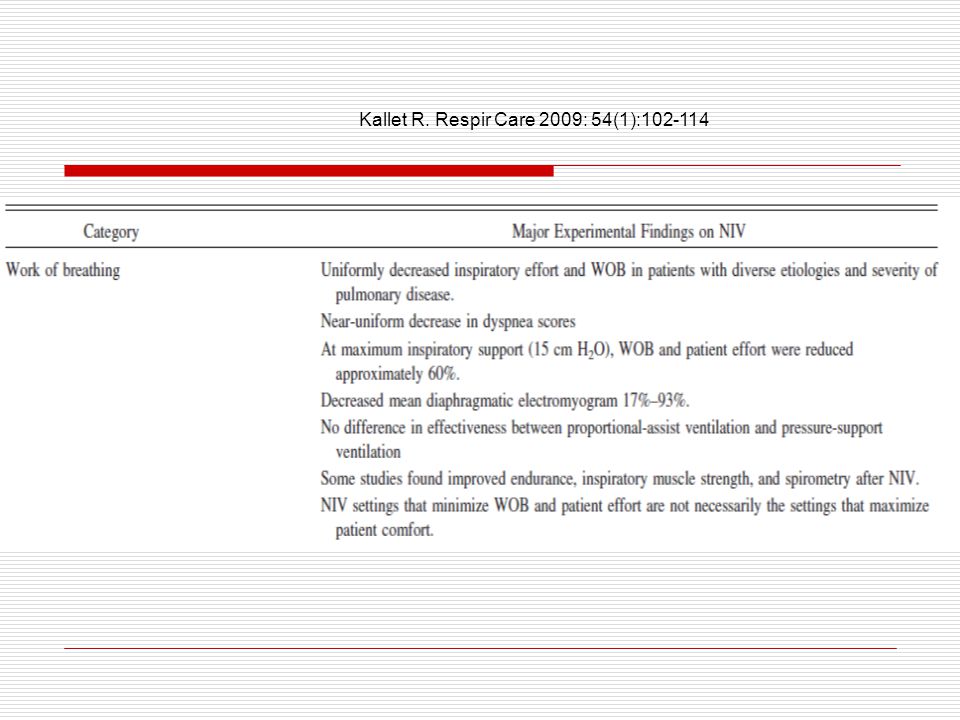
Summary Findings on the Physiologic Effects of Noninvasive Ventilation Category Major Experimental Findings on NIV Work of breathing Uniformly decreased inspiratory effort and WOB in patients with diverse etiologies and severity of pulmonary disease. Near-uniform decrease in dyspnea scores At maximum inspiratory support (15 cm H2O), WOB and patient effort were reduced approximately 60%. Decreased mean diaphragmatic electromyogram 17%–93%. No difference in effectiveness between proportional-assist ventilation and pressure-support ventilation Some studies found improved endurance, inspiratory muscle strength, and spirometry after NIV. NIV settings that minimize WOB and patient effort are not necessarily the settings that maximize patient comfort. Kallet R. Respir Care 2009: 54(1):102-114
, WOB and patient effort were reduced approximately 60%. Decreased mean diaphragmatic electromyogram 17%–93%. No difference in effectiveness between proportional-assist ventilation and pressure-support ventilation Some studies found improved endurance, inspiratory muscle strength, and spirometry after NIV. NIV settings that minimize WOB and patient effort are not necessarily the settings that maximize patient comfort. Kallet R. Respir Care 2009: 54(1):")
83
Summary Findings on the Physiologic Effects of Noninvasive Ventilation Category Major Experimental Findings on NIV Work of breathingUniformly decreased inspiratory effort an WOB in pts with diverse etiologies and severity of lung dis. Near-uniform decrease in dyspnea scores At maximum inspiratory support (15 cm H2O), WOB and pt effort were reduced approximately 60% Decreased mean diaphragmatic electromyogram 17%–93% No difference in effectiveness between proportional-assist ventilation and pressure-support ventilation Some studies found improved endurance, inspiratory muscle strength, and spirometry after NIV NIV settings that minimize WOB and patient effort are not necessarily the settings that maximize patient comfort. Kallet R. Respir Care 2009: 54(1):102-114
, WOB and pt effort were reduced approximately 60% Decreased mean diaphragmatic electromyogram 17%–93% No difference in effectiveness between proportional-assist ventilation and pressure-support ventilation Some studies found improved endurance, inspiratory muscle strength, and spirometry after NIV NIV settings that minimize WOB and patient effort are not necessarily the settings that maximize patient comfort. Kallet R. Respir Care 2009: 54(1):")
84
Breathing pattern Maximal inspiratory support that minimized inspiratory work load increased mean VT 47%. Respiratory-frequency response to maximal NIV support differed in COPD Respiratory frequency typically decreased in patients with acute cardiogenic pulmonary edema. Respiratory-system mechanicsNIV generally increased dynamic lung compliance 17%–50% in pts with COPD, morbid obesity, or restrictive chest-wall disease. During NIV, applied PEEP of 5 cm H2O decreased dynamic intrinsic PEEP in COPD pts High (15 cm H2O) inspiratory support without applied PEEP tends to increase inspiratory dynamic intrinsic PEEP in COPD. Kallet R. Respir Care 2009: 54(1):102-114
 inspiratory support without applied PEEP tends to increase inspiratory dynamic intrinsic PEEP in COPD. Kallet R. Respir Care 2009: 54(1):")
86
Cardiovascular function In healthy subjects, nasal CPAP of 15 cm H2O decreased cardiac output 20%–30%. In patients with stable COPD, high (10–20 cm H2O) pressure-support with low (3–5 cm H2O) PEEP decreased cardiac output approximately 20%. In patients with ALI those NIV levels had negligible effects on cardiac output. In patients with congestive heart failure, NIV often increased cardiac output by decreasing inspiratory effort and left-ventricular afterload. Pulmonary gas-exchange function At settings that minimized WOB, NIV typically increased pH an average 0.06, increased PaO2 8 mm Hg, and decreased PaCO2 9 mm Hg. NIV typically increased PaO2 in patients with acute cardiogenic pulmonary edema, but only decreased PaCO2 in the subgroup of patients with hypercapnia. Kallet R. Respir Care 2009: 54(1):102-114
 pressure-support with low (3–5 cm H2O) PEEP decreased cardiac output approximately 20%. In patients with ALI those NIV levels had negligible effects on cardiac output. In patients with congestive heart failure, NIV often increased cardiac output by decreasing inspiratory effort and left-ventricular afterload. Pulmonary gas-exchange function At settings that minimized WOB, NIV typically increased pH an average 0.06, increased PaO2 8 mm Hg, and decreased PaCO2 9 mm Hg. NIV typically increased PaO2 in patients with acute cardiogenic pulmonary edema, but only decreased PaCO2 in the subgroup of patients with hypercapnia. Kallet R. Respir Care 2009: 54(1):")
87
Respiratory failure after extubation in high risk patients % * Ferrer et al. AJRCCM In press

88
Epstein SK. Respir Care 2010; 55:198-208

91
Non-invasive ventilation is an effective treatment for patients with acute-on-chronic hypercapnic respiratory failure.(Cochrane ) A. Διευκόλυνση weaning και αποδιασωλήνωσης Cochrane systematic review and meta-analysis. BMJ 2003; 326: 185–89.

92
Cochrane Database 2003;(4)Noninvasive positive pressure ventilation as a weaning strategy for intubated adults with respiratory failure. London, Ontario, Canada SEARCH STRATEGY: We searched the Cochrane Central Register of Controlled Trials MEDLINE (Jan 1966 - July 2003) and EMBASE (Jan 1980 - July 2003) for RCT comparing NPPV and IPPV weaning. SELECTION CRITERIA: Randomized and quasi-randomized studies comparing early extubation with immediate application of NPPV to IPPV weaning in intubated adults with respiratory failure. DATA COLLECTION AND ANALYSIS: 2 reviewers independently assessed trial quality and abstracted data according to prespecified criteria. MAIN RESULTS: We identified 11 trials, of which 5 were included, involving 171 participants with predominantly COPD. Overall, the included studies were of moderate to good quality. NPPV strategy decreased mortality (RR 0.41, 95% CI 0.22 to 0.76), the incidence of ventilator associated pneumonia (RR 0.28, 95% CI 0.09 to 0.85), intensive care unit LOS (WMD -6.88 days, 95% CI -12.60 to -1.15), hospital length of stay (WMD -7.33 days, 95%CI -14.05 to -0.61), total duration of mechanical support (WMD -7.33 days, 95% CI -11.45 to -3.22) and the duration of endotracheal mechanical ventilation (WMD -6.79 days, 95% CI -11.70 to -1.87). There was no effect of NPPV on weaning failures or the duration of mechanical support related to weaning and insufficient data to pool adverse events or quality of life. Subgroup analyses suggested that the mortality benefit of the NPPV approach is greater in patients with COPD. REVIEWER'S CONCLUSIONS: Summary estimates from 5 studies of moderate to good quality demonstrated a consistent positive effect on overall mortality. At present, use of NPPV to facilitate weaning in mechanically ventilated patients, with predominantly chronic obstructive lung disease, is associated with promising, although insufficient
 and EMBASE (Jan July 2003) for RCT comparing NPPV and IPPV weaning. SELECTION CRITERIA: Randomized and quasi-randomized studies comparing early extubation with immediate application of NPPV to IPPV weaning in intubated adults with respiratory failure. DATA COLLECTION AND ANALYSIS: 2 reviewers independently assessed trial quality and abstracted data according to prespecified criteria. MAIN RESULTS: We identified 11 trials, of which 5 were included, involving 171 participants with predominantly COPD. Overall, the included studies were of moderate to good quality. NPPV strategy decreased mortality (RR 0.41, 95% CI 0.22 to 0.76), the incidence of ventilator associated pneumonia (RR 0.28, 95% CI 0.09 to 0.85), intensive care unit LOS (WMD days, 95% CI to -1.15), hospital length of stay (WMD days, 95%CI to -0.61), total duration of mechanical support (WMD days, 95% CI to -3.22) and the duration of endotracheal mechanical ventilation (WMD days, 95% CI to -1.87). There was no effect of NPPV on weaning failures or the duration of mechanical support related to weaning and insufficient data to pool adverse events or quality of life. Subgroup analyses suggested that the mortality benefit of the NPPV approach is greater in patients with COPD. REVIEWER S CONCLUSIONS: Summary estimates from 5 studies of moderate to good quality demonstrated a consistent positive effect on overall mortality. At present, use of NPPV to facilitate weaning in mechanically ventilated patients, with predominantly chronic obstructive lung disease, is associated with promising, although insufficient.")
93
In evaluating the prospective NIV weaning trials described above, Burns and colleagues, in their 2 meta-analyses, concluded that NIV is a promising technique for weaning COPD patients but that there is insufficient evidence of benefit to definitively recommend it.

Παρόμοιες παρουσιάσεις




 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")












>")





