Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
ΠΡΟΣΕΓΓΙΣΗ ΤΟΥ ΚΑΠΝΙΣΤΗ Ο ΡΟΛΟΣ ΤΟΥ ΚΑΡΔΙΟΛΟΓΟΥ
ΠΡΟΣΕΓΓΙΣΗ ΤΟΥ ΚΑΠΝΙΣΤΗ Ο ΡΟΛΟΣ ΤΟΥ ΚΑΡΔΙΟΛΟΓΟΥ Πέτρος Γ. Καλογερόπουλος Διευθυντής Καρδιολογίας Γ.Ο.Ν.Κ:<<Οι Άγιοι Ανάργυροι >> Ιατρείο Υπέρτασης ΤΖΑΝΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ 14/04/14

2
WHO top ten causes of death3
Smoking Is Related To 5 of the Top 10 Leading Causes of Death Worldwide 1 in 10 adult deaths are smoking-related2 500,000,000 people alive today will die from smoking-related causes2 WHO top ten causes of death3 Smoking has been found to be causally related to 5 of the top 10 leading causes of death worldwide. These 5– Ischemic Heart Disease, Cerebrovascular disease, COPD, Lung Cancer, Stomach Cancer – are highlighted in orange in the graph above. Note – the graph displays overall numbers of deaths, which includes but is not limited to those that are directly attributable to smoking. References US Department of Health and Human Services. The Health Consequences of Smoking. A Report of the Surgeon General. Atlanta, Ga: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. The World Bank Curbing the epidemic: governments and the economics of tobacco control. Washington, D.C. World Health Organization. World Health Report: 2003: Shaping the Future. Causes Related to Smoking 1. Surgeon General’s Report, World Bank, World Health Organization, 2003.

3
WHO top ten risk factors for disability
Smoking: The Leading Risk Factor for Disease and Disability in Developed Countries… Overall, 12% of all disease burden in developed countries is associated with tobacco use WHO top ten risk factors for disability Of the 10 leading risk factors for disease and disability – Tobacco leads in causing the largest burden of disease. Tobacco is the leading risk factor of disease and disability, accounting for about 12% of all disease and injury burden. For both sexes, alcohol and blood pressure account for 9–10% of DALYs, and cholesterol and body mass for 6–7% of DALYs. References World Health Organization, World Health Report: 2002: Reducing Risks, Promoting Healthy Life. 1 DALY = Loss of 1 year of equivalent full health World Health Organization, 2002

4
… And An Increasing Problem in Low Mortality Developing Countries
Tobacco is the third greatest risk factor for disability in developing countries WHO top ten risk factors for disability In developing countries with low child and low adult mortality, tobacco is already the 3rd leading risk factor for disability, behind alcohol and blood pressure. However, the prevalence of smoking is high in these countries compared to industrialized countries and the incidence of smoking in some segments of these populations are increasing. In high mortality developing countries, tobacco is the 9th leading risk factor for disease and disability. As would be expected in such countries, the leading risk factors are underweight, unsafe sex, and unsafe water, sanitation and hygiene. References World Health Organization, World Health Report: 2002: Reducing Risks, Promoting Healthy Life. 1 DALY = Loss of 1 year of equivalent full health World Health Organization, 2002

5
5

6
Deaths from smoking are increasing
Developed Countries Developing Countries 3 2,4 2,4 2,5 2007 3,5 millions deaths/year deaths/day By 2030 10 millions deaths/year Smoking may kill 1 billion people during the 21st century 2 Deaths 1,3 1,5 1 0,5 0,3 0,2 1950 1975 2000 1. Mackay J, Eriksen M. The Tobacco Atlas. World Health Organization; Mackay J, Eriksen M. The Tobacco Atlas. World Health Organization; 2006. 6

7
Endothelial Dysfunction
Oxidative Stress: Endothelial Dysfunction and CAD Risk Factors Homocysteine Estrogen deficiency Smoking LDL Diabetes Hypertension O Endothelial Cells and H2O2 Vascular Smooth Muscle Endothelial Dysfunction Oxidative Stress: Endothelial Dysfunction and CAD/Renal Risk Factors A variety of conditions or insults listed at the top of the illustration that are known risk factors for either coronary artery disease (CAD), progressive renal insufficiency, or both, adversely affect endothelial cell or vascular smooth muscle cell function by increasing the formation of reactive oxygen species such as superoxide anion and hydrogen peroxide. The resultant reduction in the actions of endothelium-derived vasodilators/growth inhibitors such as prostacyclin and nitric oxide with maintenance or increased formation of endothelium-derived vasoconstrictors/growth promoters, such as angiotensin II, endothelin-1, and PAI-1, has significant vascular and renal pathophysiological consequences. Some of the mechanisms by which progressive coronary and renal injury occur include increased apoptosis or programmed cell death that contributes to vascular wall remodeling, activation of cell adhesion molecules resulting in adherence of both mononuclear and polymorphonuclear leukocytes to the vascular wall with subsequent infiltration, deposition of oxidized lipids in the vessel wall, vasoconstriction, both hypertrophy and hyperplasia of vascular smooth muscle cells, and a propensity for thrombus formation. Lipid deposition Apoptosis Thrombosis VSMC growth Leukocyte adhesion Vasoconstriction
, progressive renal insufficiency, or both, adversely affect endothelial cell or vascular smooth muscle cell function by increasing the formation of reactive oxygen species such as superoxide anion and hydrogen peroxide. The resultant reduction in the actions of endothelium-derived vasodilators/growth inhibitors such as prostacyclin and nitric oxide with maintenance or increased formation of endothelium-derived vasoconstrictors/growth promoters, such as angiotensin II, endothelin-1, and PAI-1, has significant vascular and renal pathophysiological consequences. Some of the mechanisms by which progressive coronary and renal injury occur include increased apoptosis or programmed cell death that contributes to vascular wall remodeling, activation of cell adhesion molecules resulting in adherence of both mononuclear and polymorphonuclear leukocytes to the vascular wall with subsequent infiltration, deposition of oxidized lipids in the vessel wall, vasoconstriction, both hypertrophy and hyperplasia of vascular smooth muscle cells, and a propensity for thrombus formation. Lipid. deposition. Apoptosis. Thrombosis. VSMC. growth. Leukocyte. adhesion. Vasoconstriction.")
8
Reduction in CHD mortality
Primary prevention in England and Wales between 1981 and 2000 SPEAKER NOTES The impact of a reduction in 35% of the prevalence of smoking saved nearly 25,000 lives in England and Wales between This is far more lives saved than would have been delivered by cholesterol lowering or blood pressure control For a 35% reduction of smoking prevalence - 4.2% reduction of hypercholesterolemia - 7.7% reduction of high blood pressure in the general population Slide courtesy of D Thomas Adapted from Unal B, Critchley JA, Capewell S. BMJ 2005;331;614-19 8

9
Smoking and MI in younger age
Himonas Ε, Andrikopoulos G, Richter D, et al. ACC 1999 9

10
% of smokers by age and gender
Smoking: The essential and often unique risk factor for acute coronary syndromes in young adults 6,448 patients with STEMI % of smokers by age and gender The prevalence of smoking is very important in myocardial infarction under 50 years ….with the same prevalence among men and women SPEAKER NOTES Smoking is the essential and often unique risk factor for acute coronary syndromes in young adults Between 70-80% of ACS patients under 50 years old admitted to hospitals in France, were smokers 0.97 0.94 0.74 0.83 0.55 0.60 0.68 0.40 0.18 0.25 Global Female/Male prevalence = 0.38 Adapted from Thomas D et al. Poster presented at French Society Cardiology January 2007 10

11
Smoking and Stroke In the long run: favors atherosclerosis
Smoking is the cause for 12% to 14% of all deaths from stroke Risk for Stroke increases by smoking acutely: thrombus formation In the long run: favors atherosclerosis 11

12
Smoking and peripheral arterial disease
20% of smokers > 55 years suffer from PAD Build-up of atherosclerotic plaque in arterial wall Peripheral vascular disease (PVD) affects approximately 20% of adults older than age 55. Approximately half of patients with PVD are asymptomatic. Five to ten percent of asymptomatic patients will progress to symptomatic PVD over 5 years. Patients with symptomatic PVD are at higher risk for concomitant cardiovascular disease as well as cardiovascular mortality. References Hankey GJ, Norman PE, Eikelboom JW. Medical treatment of peripheral arterial disease. JAMA. 2006;295(5): Hooi JD, Kester ADM, Stoffers HEJH, Overdijk M, van Ree JW, Knottnerus JA. Incidence of and risk factors for asymptomatic peripheral arterial occlusive disease: a longitudinal study. Am J Epidemiol. 2001;153(7): Hooi JD, Stoffers HEJH, Knottnerus JA, van Ree JW. The prognosis of non-critical limb ischaemia: a systematic review of population-based evidence. Br J Gen Pract. 1999;49:49-55. Hooi JD, Stoffers HEJH, Kester ADM, et al. Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease: the Limburg PAOD study. Scand J Prim Health Care. 1998;16:
 affects approximately 20% of adults older than age 55. Approximately half of patients with PVD are asymptomatic. Five to ten percent of asymptomatic patients will progress to symptomatic PVD over 5 years. Patients with symptomatic PVD are at higher risk for concomitant cardiovascular disease as well as cardiovascular mortality. References. Hankey GJ, Norman PE, Eikelboom JW. Medical treatment of peripheral arterial disease. JAMA. 2006;295(5): Hooi JD, Kester ADM, Stoffers HEJH, Overdijk M, van Ree JW, Knottnerus JA. Incidence of and risk factors for asymptomatic peripheral arterial occlusive disease: a longitudinal study. Am J Epidemiol. 2001;153(7): Hooi JD, Stoffers HEJH, Knottnerus JA, van Ree JW. The prognosis of non-critical limb ischaemia: a systematic review of population-based evidence. Br J Gen Pract. 1999;49: Hooi JD, Stoffers HEJH, Kester ADM, et al. Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease: the Limburg PAOD study. Scand J Prim Health Care. 1998;16:")
13
Smoking and abdominal aorta aneurysm
Odds Ratio (95% CI)a Key Point Smoking is the most important modifiable risk factor for development of abdominal aortic aneurysm (AAA). Vardulakai et al performed a randomized, controlled trial on 5356 men and women in Chichester, UK, between 1988 and Anteroposterior measurements of the aorta were obtained with an ultrasound, and aneurysm was defined as an aortic diameter of 30 mm or more. Personal and social history were obtained prior to the baseline physical via a self-administered questionnaire. Men were 5.6 times more likely to have an AAA than women. The chart above depicts that the level of risk for AAA increases with the number of cigarettes smoked daily. Risk of AAA ranges from 0.7, 3.0, 2.9, 5.5 for current smokers who smoked 1-9, 10-19, 20-24, and 25 cigarettes daily, respectively. Nonsmokers 1 to 9 10 to 19 20 to 24 25 Cigarettes/Day Current Smokers Vardulaki et al. Br J Surg. 2000;87(2): Reference Vardulaki KA, Walker NM, Day NE, Duffy SW, Ashton AH, Scott RAP. Quantifying the risks of hypertension, age, sex and smoking in patients with abdominal aortic aneurysm. Br J Surg. 2000;87(2): 13
a. Key Point. Smoking is the most important modifiable risk factor for development of abdominal aortic aneurysm (AAA). Vardulakai et al performed a randomized, controlled trial on 5356 men and women in Chichester, UK, between 1988 and Anteroposterior measurements of the aorta were obtained with an ultrasound, and aneurysm was defined as an aortic diameter of 30 mm or more. Personal and social history were obtained prior to the baseline physical via a self-administered questionnaire. Men were 5.6 times more likely to have an AAA than women. The chart above depicts that the level of risk for AAA increases with the number of cigarettes smoked daily. Risk of AAA ranges from 0.7, 3.0, 2.9, 5.5 for current smokers who smoked 1-9, 10-19, 20-24, and 25 cigarettes daily, respectively. Nonsmokers. 1 to to to 24. 25. Cigarettes/Day. Current Smokers. Vardulaki et al. Br J Surg. 2000;87(2): Reference. Vardulaki KA, Walker NM, Day NE, Duffy SW, Ashton AH, Scott RAP. Quantifying the risks of hypertension, age, sex and smoking in patients with abdominal aortic aneurysm. Br J Surg. 2000;87(2):")
15
Εθισμός στη Νικοτίνη Πραγματικός εθισμός σε ναρκωτική ουσία Απαιτεί μακροχρόνια κλινική παρέμβαση, όπως συμβαίνει και με άλλες εθιστικές διαταραχές Η υποτροπή είναι συνήθης και οφείλεται στη φύση του εθισμού, και όχι στην αποτυχία του ατόμου Η μακροχρόνια αποχή από το κάπνισμα για εκείνους που προσπαθούν να το διακόψουν χωρίς βοήθεια είναι 3%–5% Οι περισσότεροι εμφανίζουν υποτροπή εντός των πρώτων 8 ημερών 15

16
Αποτελεσματικές μέθοδοι διακοπής καπνίσματος
Δύο τύποι προσέγγισης είναι αποδεδειγμένα αποτελεσματικοί: Συμβουλευτική Φαρμακοθεραπεία Τα καλύτερα αποτελέσματα επιτυγχάνονται με συνδυασμό των δύο προσεγγίσεων Fiore MC. Treating tobacco use and dependence. Rasp Care 2000;45:1200 West R. Smoking cessation guidelines for health professionals: an update. Thorax 2000;55:987 Simon JA. Smoking cessation counseling (intensive vs. minimal). Am J Med 2003;114(7):555 16 16
. Am J Med 2003;114(7):")
18
Σύνδρομο Στέρησης Σύνδρομο Στέρησης
Ευερεθιστότητα, απογοήτευση ή θυμός (<4 εβδομάδες)2 Αϋπνία / διαταραχές ύπνου (<4 εβδομάδες)2 Αυξημένη όρεξη ή πρόσληψη σωματικού βάρους (>10 εβδομάδες)2 Άγχος (μπορεί να αυξηθεί ή να μειωθεί με τη διακοπή του καπνίσματος)1,2 Δυσφορία ή καταθλιπτική διάθεση (<4 εβδομάδες)2 Νευρικότητα ή ανυπομονησία (<4 εβδομάδες)2 Δυσκολία Συγκέντρωσης (<4 εβδομάδες)2 18
2. Αϋπνία / διαταραχές ύπνου. (<4 εβδομάδες)2. Αυξημένη όρεξη ή πρόσληψη. σωματικού βάρους. (>10 εβδομάδες)2. Άγχος. (μπορεί να αυξηθεί ή να μειωθεί με τη διακοπή του καπνίσματος)1,2. Δυσφορία ή καταθλιπτική διάθεση. (<4 εβδομάδες)2. Νευρικότητα ή. ανυπομονησία. (<4 εβδομάδες)2. Δυσκολία Συγκέντρωσης. (<4 εβδομάδες)")
19
2008 US Department of Health and Human Services Clinical Practice Guidelines for smoking cessation
19

20
Ρωτήστε Σχετικά με τη Χρήση Καπνού
Αναγνωρίστε και τεκμηριώστε την κατάσταση ως προς τη χρήση καπνού για κάθε ασθενή σε κάθε επίσκεψη Εφαρμόστε ένα κοινό για όλο το ιατρείο σας σύστημα, το οποίο θα διασφαλίζει τη διερεύνηση και την τεκμηρίωση της κατάστασης ως προς τη χρήση καπνού Διευρύνετε την τεκμηρίωση των ζωτικών σημείων, ώστε να συμπεριληφθεί η χρήση καπνού Αυτοκόλλητα για τη χρήση καπνού σε διαγράμματα Συστήματα υπενθύμισης ηλεκτρονικού υπολογιστή για τα ηλεκτρονικά ιατρικά αρχεία Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.

21
2008 US Department of Health and Human Services Clinical Practice Guidelines for smoking cessation
21

22
Συμβουλές για τη Διακοπή του Καπνίσματος
ΣΑΦΗΣ “Πιστεύω ότι είναι σημαντικό για σένα να σταματήσεις τώρα το κάπνισμα, και εγώ μπορώ να σε βοηθήσω.” ΚΑΤΗΓΟΡΗΜΑΤΙΚΟΣ “Ως γιατρός σου, πρέπει να σου πω ότι το να κόψεις το κάπνισμα είναι πολύ σημαντικό για την προστασία της υγείας σου, τώρα και στο μέλλον.” ΠΡΟΣΩΠΟΠΟΙΗΜΕΝΟΣ Συνδέστε τη χρήση καπνού με την υγεία/ασθένεια (λόγος επίσκεψης στο ιατρείο), τα κοινωνικά/οικονομικά κόστη, το επίπεδο επιθυμίας, και τον αντίκτυπο στους άλλους (παιδιά) 1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000.
, τα κοινωνικά/οικονομικά κόστη, το επίπεδο επιθυμίας, και τον αντίκτυπο στους άλλους (παιδιά) 1. Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June")
23
2008 US Department of Health and Human Services Clinical Practice Guidelines for smoking cessation
23

24
Πρόκειται για ένα εργαλείο που θα σας βοηθήσει να κατανοήσετε πόσο σημαντικό είναι για εσάς να διακόψετε το κάπνισμα. Καταγράψτε σε έναν κατάλογο όλα όσα απολαμβάνετε στο κάπνισμα. Στη συνέχεια, καταγράψτε σε έναν διαφορετικό κατάλογο όλα όσα απεχθάνεστε στο κάπνισμα. Ποιος από τους δύο καταλόγους είναι μεγαλύτερος; Εάν ο κατάλογος όσων απεχθάνεστε είναι μεγαλύτερος από τον κατάλογο όσων απολαμβάνετε, τότε είστε έτοιμοι να διακόψετε το κάπνισμα. 24

25
2008 US Department of Health and Human Services Clinical Practice Guidelines for smoking cessation
25

26
Η ανάπτυξη ενός Σχεδίου Διακοπής του καπνίσματος
Πριν Μετά Ημερομηνία Διακοπής (κατά τη διάρκεια της προσπάθειας) Και μετά την Ημερομηνία Διακοπής 26
 Και μετά την Ημερομηνία Διακοπής. 26.")
31
Γνωρίζετε τι νά περιμένετε
Αντισταθείτε στήν έντονη επιθυμία νά καπνίσετε (κανόνας τών 5 λεπτών) Εάν παρασυρθείτε και καπνίσετε ένα τσιγάρο, μήν τά παρατήσετε –συνεχίστε την προσπάθεια
 Εάν παρασυρθείτε και καπνίσετε ένα τσιγάρο, μήν τά παρατήσετε –συνεχίστε την προσπάθεια.")
32
2008 US Department of Health and Human Services Clinical Practice Guidelines for smoking cessation
32

33
Κανονίστε Παρακολούθηση
Προγραμματίστε μία επαφή για παρακολούθηση, κατά προτίμηση εντός της πρώτης εβδομάδας μετά την ημερομηνία διακοπής Η παρακολούθηση μπορεί να γίνει είτε με προσωπική συνάντηση είτε μέσω τηλεφώνου Ενέργειες παρακολούθησης Έκφραση συγχαρητηρίων για την επιτυχία Επιθεώρηση των συνθηκών της προσωρινής υποτροπής – διασφάλιση επαναδέσμευσης στην αποχή Αναγνώριση των προκλήσεων και προετοιμασία για αυτές Αξιολόγηση της χρήσης φαρμακοθεραπείας Εξέταση του ενδεχομένου παραπομπής σε πιο εντατική θεραπεία Fiore MC, et al. US Department of Health and Human Services. Public Health Service. June 2000

34
Ομάδες με λιγότερες πιθανότητες να διακόψουν το κάπνισμα
Υψηλότερο επίπεδο εξάρτησης Αριθμός τσιγάρων ανά ημέρα Χρόνος έως το κάπνισμα του πρώτου τσιγάρου μετά το πρωινό ξύπνημα Συμβίωση με ενεργό καπνιστή Λιγότερα εκπαιδευτικά εφόδια Χαμηλότερη κοινωνικοοικονομική τάξη Συνυπάρχουσες ψυχιατρικές διαταραχές Hyland A et al. Nicotine Tob Res. 2004;6(Suppl 3):S363-S369 Chandola T et al. Addiction. 2004;99: Kalman D et al. Am J Addict. 2005;14:106–123
:S363-S369. Chandola T et al. Addiction. 2004;99: Kalman D et al. Am J Addict. 2005;14:106–123.")
35
Effects of smoking cessation on survival
Cessation at age 35-44 Cessation at age 55-64 100 100 Stopped smoking Stopped smoking 80 80 Cigarette smokers Cigarette smokers 60 60 Non smokers % survival from age 60 years Non smokers % survival from age 40 years 40 40 20 20 SPEAKER NOTES Stopping smoking at any age improves life expectancy but the earlier you stop, the greater the benefit 40 50 60 70 80 90 100 40 50 60 70 80 90 100 years years Smoking cessation is always associated with a benefit… …but an early cessation is associated with a greater benefit Doll R, Peto R et al. BMJ 2004; 328: 35

36
ΤΖΑΝΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ 7/04/14
Σας ευχαριστώ για την προσοχή σας ΤΖΑΝΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ 7/04/14

38
Σας ευχαριστώ για την προσοχή σας

39
Cardiovascular Benefits of Cessation: Reduced Risk of Stroke
P for trend <.0001 Relative Risk (95% CI)a Key Point Compared with current smokers, male ex-smokers have a reduced risk of nonfatal stroke. Robbins et al prospectively evaluated 22,071 male physicians in the Physicians’ Health Study, a randomized, double-blind, placebo-controlled study evaluating the effect of low-dose aspirin on cardiovascular disease, as well as the effect of beta-carotene on cancer and cardiovascular disease. Subjects were men aged 40 to 84 years, without history of myocardial infarction (MI), stroke, or transient ischemic attacks. Data regarding smoking habits was derived from a self-completed questionnaire. Smokers were defined as nonsmokers, ex-smokers, current smokers smoking less than 20 cigarettes per day, or current smokers smoking more than 20 cigarettes per day. Every 6 months during the first year, then annually thereafter, subjects completed a questionnaire regarding compliance with the prescribed regimen and incidence of cardiac events (stroke, MI, etc). Follow-up continued either until participants experienced nonfatal or fatal stroke, or any other fatal event. Participants were followed up for an average of 9.7 years. After adjusting for age and treatment assignment, ex-smokers had lower relative risk of total nonfatal stroke (1.2; 95% CI, ) than physicians currently smoking less than 20 and more than 20 cigarettes daily, (2.0, 95% CI, ) and (2.5, 95% CI, ), respectively. Nonsmokers Ex-smokers Current Smokers (<20 cig/d) Current Smokers (≥20 cig/d) aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age and treatment assignment. Robbins et al. Ann Intern Med. 1994;120(6): Reference Robbins AS, Manson JE, Lee I-M, Satterfield S, Hennekens CH. Cigarette smoking and stroke in a cohort of US male physicians. Ann Intern Med. 1994;120(6):
a. Key Point. Compared with current smokers, male ex-smokers have a reduced risk of nonfatal stroke. Robbins et al prospectively evaluated 22,071 male physicians in the Physicians’ Health Study, a randomized, double-blind, placebo-controlled study evaluating the effect of low-dose aspirin on cardiovascular disease, as well as the effect of beta-carotene on cancer and cardiovascular disease. Subjects were men aged 40 to 84 years, without history of myocardial infarction (MI), stroke, or transient ischemic attacks. Data regarding smoking habits was derived from a self-completed questionnaire. Smokers were defined as nonsmokers, ex-smokers, current smokers smoking less than 20 cigarettes per day, or current smokers smoking more than 20 cigarettes per day. Every 6 months during the first year, then annually thereafter, subjects completed a questionnaire regarding compliance with the prescribed regimen and incidence of cardiac events (stroke, MI, etc). Follow-up continued either until participants experienced nonfatal or fatal stroke, or any other fatal event. Participants were followed up for an average of 9.7 years. After adjusting for age and treatment assignment, ex-smokers had lower relative risk of total nonfatal stroke (1.2; 95% CI, ) than physicians currently smoking less than 20 and more than 20 cigarettes daily, (2.0, 95% CI, ) and (2.5, 95% CI, ), respectively. Nonsmokers. Ex-smokers. Current Smokers (<20 cig/d) Current Smokers (≥20 cig/d) aThe probability of an event (developing a disease) occurring in exposed people compared with the probability of the event in nonexposed people. Adjusted for age and treatment assignment. Robbins et al. Ann Intern Med. 1994;120(6): Reference. Robbins AS, Manson JE, Lee I-M, Satterfield S, Hennekens CH. Cigarette smoking and stroke in a cohort of US male physicians. Ann Intern Med. 1994;120(6):")
42
Rest Pain, Cumulative (%)
Cardiovascular Benefits of Cessation: Reduced Progression of Peripheral Vascular Disease 30 Smoking Abstention 20 P=.049 Rest Pain, Cumulative (%) Key Point Smokers with intermittent claudication (IC), who discontinue smoking demonstrate reductions in progression of peripheral vascular disease (PVD). Three hundred forty-three Swedish patients with IC were evaluated at baseline, at follow-up 12 months later, and 7 years after the follow-up exam. Subjects were designated ex-smokers if they had stopped smoking within 6 months before or 12 months after the initial examination. Patients who continued to smoke or stopped more than 12 months after the initial examination were designated as current smokers. At baseline, evidence of PVD was determined based upon the results of a combination of segmental blood pressure measurements as well as Doppler assessment of the velocity and direction of the blood flow in the popliteal and common femoral arteries. Walking tolerance was also estimated by a symptom-limited treadmill test. Rest pain was defined as pain in the leg or foot when the patient was recumbent that was relieved when the leg was lowered. Patients who had stopped smoking within 6 months before or within 12 months after the initial examination were designated nonsmokers. Patients who continued to smoke or stopped smoking more During the 7-year follow-up period, rest pain developed in 26 patients, all of whom were current smokers. None of the ex-smokers developed rest pain. After 7 years, the cumulative proportion of patients with rest pain was 16% among the current smokers (P=.049). 10 2 7 1 6 5 4 3 Years Jonason et al. Acta Med Scand. 1987;221: Reference Jonason T, Bergstrom R. Cessation of smoking in patients with intermittent claudication: effects on the risk of peripheral vascular complications, myocardial infarction and mortality. Acta med Scand. 1987;221:
 Key Point. Smokers with intermittent claudication (IC), who discontinue smoking demonstrate reductions in progression of peripheral vascular disease (PVD). Three hundred forty-three Swedish patients with IC were evaluated at baseline, at follow-up 12 months later, and 7 years after the follow-up exam. Subjects were designated ex-smokers if they had stopped smoking within 6 months before or 12 months after the initial examination. Patients who continued to smoke or stopped more than 12 months after the initial examination were designated as current smokers. At baseline, evidence of PVD was determined based upon the results of a combination of segmental blood pressure measurements as well as Doppler assessment of the velocity and direction of the blood flow in the popliteal and common femoral arteries. Walking tolerance was also estimated by a symptom-limited treadmill test. Rest pain was defined as pain in the leg or foot when the patient was recumbent that was relieved when the leg was lowered. Patients who had stopped smoking within 6 months before or within 12 months after the initial examination were designated nonsmokers. Patients who continued to smoke or stopped smoking more. During the 7-year follow-up period, rest pain developed in 26 patients, all of whom were current smokers. None of the ex-smokers developed rest pain. After 7 years, the cumulative proportion of patients with rest pain was 16% among the current smokers (P=.049) Years. Jonason et al. Acta Med Scand. 1987;221: Reference. Jonason T, Bergstrom R. Cessation of smoking in patients with intermittent claudication: effects on the risk of peripheral vascular complications, myocardial infarction and mortality. Acta med Scand. 1987;221:")
43
Η συσχέτιση της διακοπής του καπνίσματος με την αύξηση του σωματικού βάρους και τον κίνδυνο για καρδιαγγειακή νόσο Οι συγγραφείς καταλήγουν ότι η πρόσληψη σωματικού βάρους που συνοδεύει συχνά τη διακοπή του καπνίσματος δεν μειώνει την ωφέλιμη επίδραση της διακοπής του καπνίσματος στην καρδιαγγειακή νοσηρότητα. (Clair C, Rigotti NA, Porneala B, et al. JAMA 2013;309:

44
The process of stopping smoking
US PHS Guideline – Treating Tobacco Use and Dependence: 2008 Update Ask - Ask about tobacco use at every visit Advise - Advise to quit in a clear, strong, and personalised manner A A Assess A Assess willingness to make a quit attempt A A Assist Arrange Arrange follow-up through personal and telephone contact and continue supporting, encouraging, and treating the patient - Assist in quit attempt with counselling, pharmacotherapy, and social support 1. Raw M, McNeill A, West R. Thorax 1998; 53 (Suppl 5, Pt 1): S1-19.
: S1-19.")
45
Patient Barriers to Treatment Initiation May Be Overcome With Effective Physician-Patient Dialogue
Poor understanding of their condition1 Managing multiple comorbid conditions Lack of perceived benefit from treatment1,2 Deficient knowledge about treatment options3 Lack of self-confidence in managing their condition4 Fears of side effects5 Effective communication may help overcome barriers and improve health outcomes1,4 Patient Barriers Nelson M, et al. Am J Med. 2007;120:S28-S32 George J et al, Chest. 2005;128: Moffat M, et al. Fam Pract. 2007;24:65-70 Naik AD, et al. Circulation. 2008;117: Horne R. Chest. 2006;130:65S-72S. Nelson M, Hamilton HE. Improving in-office discussion of chronic obstructive pulmonary disease: results and recommendations from an in-office linguistic study in chronic obstructive pulmonary disease. Am J Med. 2007;120:S28-S32. George J, Kong DCM, Thoman R, Stewart K. Factors associated with medication nonadherence in patients with COPD. Chest. 2005;128: Moffat M, Cleland J, van der Molen T, Price D. Poor communication may impair optimal asthma care: a qualitative study. Fam Pract. 2007;24:65-70. Naik AD, Kallen MA, Walder A, Street RL. Improving hypertension control in diabetes mellitus: the effects of collaborative and proactive health communication. Circulation. 2008;117: Horne R. Compliance, adherence, and concordance: implications for asthma treatment. Chest. 2006;130:65S-72S. 45

46
3 Essential Skills for Effective and Efficient Physician-Patient Dialogue1,2
Management Goals 1. Assess motivation and readiness to change Understand your patient’s current perspective 2. Share information meaningfully and demonstrate empathy Overcome communication barriers and provide advice tailored to your patient’s needs 3. Jointly develop a treatment plan and build a partnership Encourage patients to participate in shared treatment decisions that may optimise outcomes3 Makoul G, et al. Acad Med. 2001;76: Duffy et al. Acad Med. 2004;79: Heisler et al. J Gen Intern Med. 2003; 18: Makoul G, et al. Essential elements of communication in medical encounters: The Kalamazoo Consensus Statement. Acad Med. 2001;76: Duffy FD, Gordon GH, Whelan G, et al. Assessing competence in communication and interpersonal skills: The Kalamazoo II Report. Acad Med. 2004;79: Heisler M, Vijan S, Anderson RM, et al. When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make?. J Gen Intern Med. 2003; 18: 46

47
47

48
Coronary Artery Disease

50
Summary Tobacco related deaths continue to increase1
Smoking confers significant excess risk to patients with, and without, existing cardiovascular disease2,3 The majority of men and women under 50 years old who have an AMI, smoke4 A reduction in smoking reduces the risk of acute coronary events and CHD mortality5,6 WHO. PLoS Med. 2006; 3: e Qiao Q et al. Eur Heart J 2000; 21: Van Werkhoven JMF et al. Eur Heart J 2011; 32: 365– Thomas D et al. Poster presented at French Society of Cardiology. January D F Mackay, et al Heart 2010; 96: INTERHEART study. Lancet 2006; 368: 647–58 50

51
ΚΑΤΑΝΟΜΗ ΤΗΣ ΝΙΚΟΤΙΝΗΣ (1)
Μετά την απορρόφηση και την είσοδό της στο αίμα, η νικοτίνη κατανέμεται ταχέως σε ολόκληρο τον οργανισμό Μέσα σε sec από την εισπνοή καπνού, φτάνει στους ιστούς του ΚΝΣ Επιδρώντας στον εγκέφαλο, προκαλεί έντονη, ενισχυτική ανταπόκριση, που περιλαμβάνει: Έναν ευχάριστο νικοτινικό βόμβο Χαλάρωση Μείωση του stress Αυξημένη εγρήγορση Βελτιωμένη συγκέντρωση Αλλαγές της διάθεσης Κύρια αίτια για την ανάπτυξη εξάρτησης από τη νικοτίνη! Νικοτινικός βόμβος (nicotine buzz): αίσθημα ευφορίας.
: αίσθημα ευφορίας.")
53
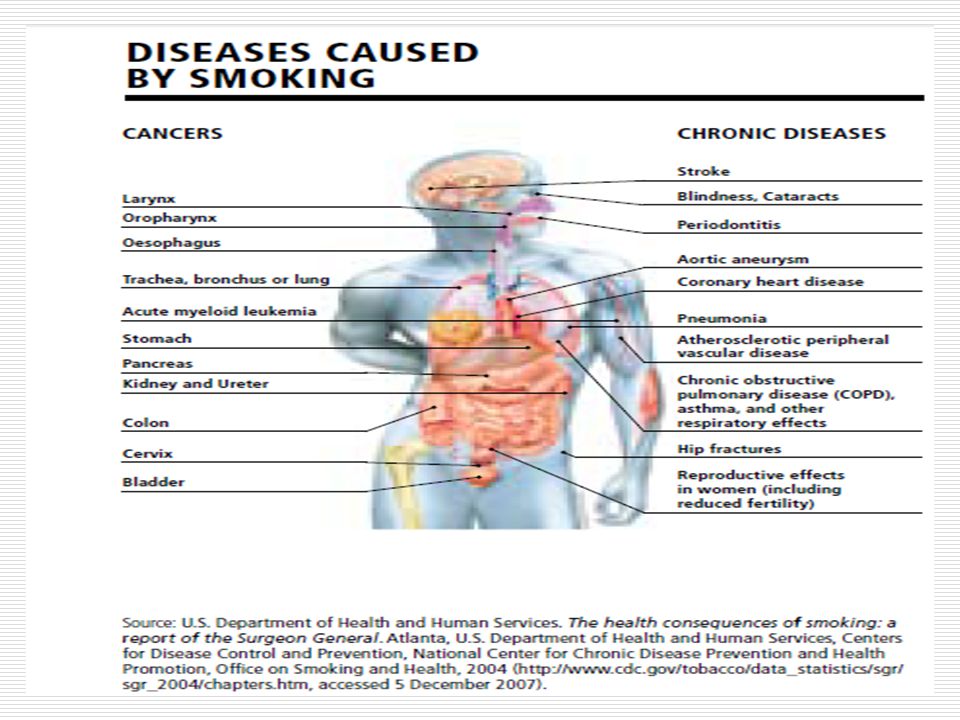
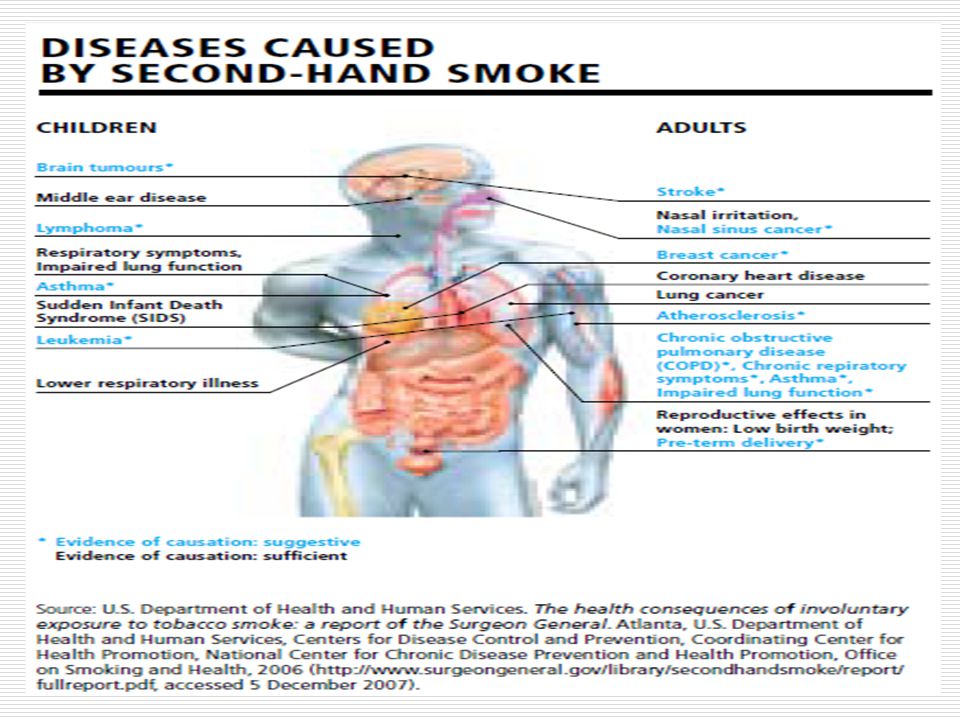
Many Diseases Are Directly Caused By Smoking
Cancer Lung Oral cavity/pharynx Laryngeal Esophageal Stomach Pancreatic Kidney Bladder Cervical Leukemia Cardiovascular Ischemic heart disease Stroke – Vascular dementia2 Peripheral vascular disease3 Abdominal aortic aneurysm Respiratory COPD Pneumonia Poor asthma control Reproductive Low birthweight Pregnancy complications Reduced fertility SIDS Other Adverse surgical outcomes/ wound healing Hip fractures Low bone density Cataract Peptic ulcer disease† Active Smoking Smoking is causally linked to a host of cardiovascular, respiratory, reproductive, and other conditions, as well as many types of cancer. Background In 2004, the US Surgeon General published a report on the health effects of active smoking, focusing specifically on the evidence for a causal relationship between smoking and disease and death. According to the research summarized in the report, many serious conditions are caused by smoking, including cardiovascular, respiratory, reproductive, and other conditions, as well as cancer affecting diverse areas and organs of the body. In addition to the widely-known consequences of lung cancer and respiratory disease, smoking has been causally linked to such diverse morbidities as low bone density, nuclear cataract, bladder cancer, and reduced fertility.1 Other studies have linked smoking to vascular dementia2 and peripheral arterial disease.3 These conditions can affect young and middle-aged smokers and, in general, as a smoker’s age increases, the frequency of smoking-caused diseases rises.1 References US Department of Health and Human Services. The Health Consequences of Smoking. A Report of the Surgeon General. Atlanta, Ga: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. Roman GC. Vascular dementia prevention: a risk factor analysis. Cerebrovasc Dis. 2005;20 (Suppl 2):91–100. Willigendael EM, Teijink JA, Bartelink ML, et al. Influence of smoking on incidence and prevalence of peripheral arterial disease. J Vasc Surg. 2004;40:1158–1165. † In patients who are Helicobacter pylori positive. COPD = chronic obstructive pulmonary disease; SIDS = sudden infant death syndrome. 1. Surgeon General’s Report Roman GC. Cerebrovasc Dis. 2005;20(Suppl 2): Willigendael EM et al. J Vasc Surg. 2004;40:
:91–100. Willigendael EM, Teijink JA, Bartelink ML, et al. Influence of smoking on incidence and prevalence of peripheral arterial disease. J Vasc Surg. 2004;40:1158–1165. † In patients who are Helicobacter pylori positive. COPD = chronic obstructive pulmonary disease; SIDS = sudden infant death syndrome. 1. Surgeon General’s Report Roman GC. Cerebrovasc Dis. 2005;20(Suppl 2): Willigendael EM et al. J Vasc Surg. 2004;40:")
55
Tobacco Dependence Support: «ABC»
The 2007 New Zealand Smoking Cessation Guidelines recommend a modified version of the 5 A’s1 Brief advice to stop smoking Ask about tobacco use at every visit Cessation support to help with the quit attempt Support should use evidence-based techniques McRobbie H, et al. N Z Med J. 2008;121:57-70.

57
Ο Κύκλος του Εθισμού στη Νικοτίνη
Νικοτίνη αύξηση ντοπαμίνης Ντοπαμίνη αισθήματα ευχαρίστησης και ηρεμίας Μείωση ντοπαμίνης μεταξύ των τσιγάρων συμπτώματα στέρησης έντονη επιθυμία για νικοτίνη, ώστε να προκληθεί μεγαλύτερη απελευθέρωση ντοπαμίνης για την αποκατάσταση των αισθημάτων ευχαρίστησης και ηρεμίας Ντοπαμίνη Νικοτίνη Jarvis MJ. BMJ. 2004; 328: Picciotto MR, et al. Nicotine and Tob Res. 1999: Suppl 2:S121-S125 57

58
Εξάρτηση από τον Καπνό και Περιβαλλοντική Ενίσχυση Συμπεριφοράς
Νικοτίνη σωματική εξάρτηση ελαφριά προς μέτρια Περιβαλλοντικά/κοινωνικά ερεθίσματα που έχουν συνδεθεί με το κάπνισμα διαδραματίζουν βασικό ρόλο στην ενίσχυση της εξάρτησης από τη νικοτίνη ψυχολογική εξάρτηση πολύ ισχυρή Caggiula AR et al. Psychol Behavior. 2002;77:683–687 58

59
ΠΡΟΣΕΓΓΙΣΗ ΤΟΥ ΚΑΠΝΙΣΤΗ Ο ΡΟΛΟΣ ΤΟΥ ΚΑΡΔΙΟΛΟΓΟΥ
ΠΡΟΣΕΓΓΙΣΗ ΤΟΥ ΚΑΠΝΙΣΤΗ Ο ΡΟΛΟΣ ΤΟΥ ΚΑΡΔΙΟΛΟΓΟΥ Πέτρος Γ. Καλογερόπουλος Διευθυντής Καρδιολογίας Γ.Ο.Ν.Κ:<<Οι Άγιοι Ανάργυροι >> Ιατρείο Υπέρτασης Πανελλήνιο Καρδιολογικό Συνέδριο 10/10/13 Αθήνα Χίλτον

Παρόμοιες παρουσιάσεις

 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")


















