ΔΙΑΓΝΩΣΤΙΚΗ ΚΑΙ ΘΕΡΑΠΕΥΤΙΚΗ ΠΡΟΣΕΓΓΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΚΑΡΚΙΝΟ
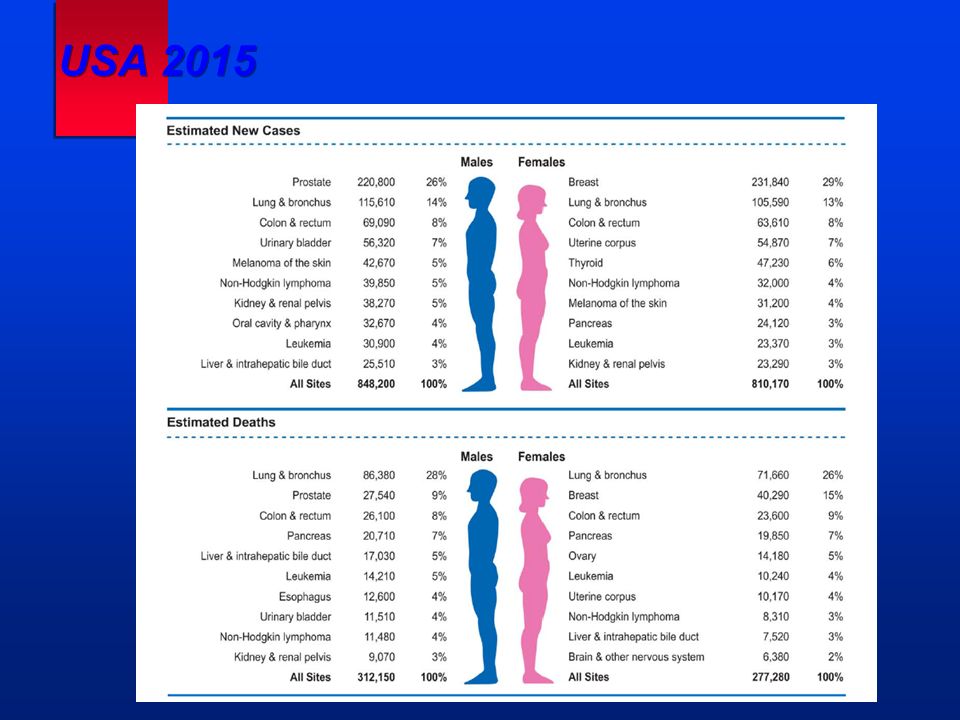
USA 2015
TUMOR GROWTH number of cancer cells diagnosticthreshold(1cm) time undetectablecancer detectablecancer limit of clinicaldetection hostdeath
ΣΥΜΠΤΩΜΑΤΑ ΑΠΟ ΤΟΝ ΚΑΡΚΙΝΟ 1.Τοπική δράση σε ιστούς & όργανα 2.Παρανεοπλασματικές εκδηλώσεις
Θεραπευτική Αντιμετώπιση ΔιάγνωσηΣταδιοποίηση
ΚΑΡΚΙΝΟΣ : ΜΕΘΟΔΟΙ ΔΙΑΓΝΩΣΗΣ & ΣΤΑΔΙΟΠΟΙΗΣΗΣ 1.Ιστορικό 2.Φυσική εξέταση 3.Απεικονιστικές μέθοδοι 4.Ενδοσκοπήσεις ( κυτταρολογική – βιοψία ) 5.Ανοικτή βιοψία, FNA, Pap – test 6.Εργαστηριακές εξετάσεις
Palpable mass ThickeningPain Mass or pain in the axilla Nipple discharge Nipple retraction Edema or erythema of the skin BREAST CANCER/LOCAL MANIFESTATIONS Signs and symptoms at presentation
BREAST CANCER Breast inspection Skin dimpling
BREAST CANCER Breast palpation
BREAST CANCER Regional nodes assessment
BREAST CANCER Spread to lymph nodes Supraclavicular Subclavicular Distal (upper) axillary Central (middle) axillary Proximal (lower) axillary Mediastinal Internal mammary Interpectoral (Rotter’s)
BREAST CANCER Fine-needle aspiration biopsy In Back and Forth EndSuction Suction Out
Lymph nodes SkinLiverKidney BrainPulmonaryBone BREAST CANCER/DISTANT MANIFESTATIONS Signs and symptoms at presentation
TNM CLASSIFICATION T umor N odes M etastasis Good Bad Prognosis
BREAST CANCER Stage IV disease M1 = Distant metastasis (including metastases to ipsilateral supraclavicular, cervical, or contralateral internal mammary lymph nodes) Any T any N M1
BREAST CANCER Distal spread Brain + Skin + Lung Pleura Liver + + Adrenals + + Bone
BREAST CANCER Survival by stage Stage 0 Stage I Stage IIA Stage IIB Stage IIIA Stage IIIB Stage IV Percent surviving Years after diagnosis
BREAST CANCER Survival according to the number of positive nodes Number of positive nodes or more Adapted from Wilson RE et al, 1994 Percent Surviving Years after diagnosis
PRIMARY BREAST CANCER Good prognostic factors Patient’s age:older than 50 years Axillary nodes:not involved Size of tumor:small (< 1 cm) Local extension of tumor:absent Histologic examination:well-differentiated tumor (grade I) Cytologic study:little atypia of nuclei (grade I) EstrogenProgesterone Oncogene amplification:absent receptors: positive (ER + and PR +) receptors: positive (ER + and PR +)
PRIMARY BREAST CANCER Poor prognostic factors Patient’s age:35–40 years Axillary nodes:involved Size of tumor:large (>5 cm) Local extension of tumor:present Histologic examination:anaplastic tumor (grade III) Cytologic study:severe atypia of nuclei (grade III) EstrogenProgesterone HER2 Oncogene amplification: present receptors: negative (ER – and PR – )
LUNG CANCER Signs and symptoms at diagnosis FREQUENCY (%) COUGH DYSPNEA CHEST PAIN HEMOPTYSIS PNEUMONITIS WEIGHT LOSS GENERALIZED ANOREXIA FEVERANEMIA COUGH DYSPNEA CHEST PAIN HEMOPTYSIS PNEUMONITIS WEIGHT LOSS GENERALIZED ANOREXIA FEVERANEMIA WEAKNESS
LUNG CANCER Paraneoplastic syndromes Inappropriate ADH secretion Ectopic ACTH production GynecomastiaEaton-LambertHypercalcemia (nonmetastatic) (nonmetastatic)Hypertrophic osteoarthropathy osteoarthropathyThrombocytosis Hypercoagulable stage SMALL CELLLARGE CELLSQUAMOUSADENOCARCINOMA
LUNG CANCER Incidence of major histologic types EPIDERMOIDCARCINOMA ADENOCARCINOMA LARGE-CELLCARCINOMA SMALL-CELLCARCINOMA OTHERS(Bronchoalveolarmixed) 33% 25% 25% 16% 1%
LUNG CANCER HISTOLOGIC TYPES Smokers vs nonsmokers SQUAMOUS CELL ADENOCARCINOMA LARGE CELL SMALL CELL BRONCHOALVEOLAR Adapted from Rosenow and Carr SMOKER (%)NONSMOKER (%) MALEFEMALE MALEFEMALE
LUNG CANCER Local and distal spread Brain Draining lymph nodes LiverAdrenalsBone
NON–SMALL CELL LUNG CANCER Split by stages Adapted from a lung cancer group survey T1 N0 T1 N1 T2 N0 T2 N1 IIIAResectable IIIAPartiallyResectable IIIBUnresectable 28% 37% 10% 15% 10%
COLON Anatomic segments and vascular supply RIGHTLEFT Ascending colon Descending colon Hepatic flexure Transverse colon Splenic flexure Sigmoid colon Cecum Sup hemorrhoidal a. and v. Sigmoid a. Ileocolic a. R. colic a. Mid. colic a. Sup. mes a. and v. Inf. mes. v. L colic a. Inf. mes. a. Aorta small intestine Internal pudenda a. Middle hemorrhoidal a. Inferior hemorrhoidal a. Rectum
COLORECTAL CANCER Pretreatment evaluation HISTORY — Including familial history of CRC/polyps/other cancersHISTORY — Including familial history of CRC/polyps/other cancers PHYSICAL EXAMINATIONPHYSICAL EXAMINATION — Digital examination of the rectum — Digital examination of the rectum — Hepatomegaly/ascites/lymphadenopathies — Hepatomegaly/ascites/lymphadenopathies — In women: breast/ovarian abnormalities — In women: breast/ovarian abnormalities LABORATORY DATALABORATORY DATA — Blood count, CEA, liver chemistry — Blood count, CEA, liver chemistry GASTROINTESTINAL EXAMINATIONGASTROINTESTINAL EXAMINATION — Full colonoscopy — Full colonoscopy IMAGINGIMAGING — Chest X-ray — Chest X-ray — Abdominal ultrasound for colon cancer — Abdominal pelvic CT scan for rectal cancer — Abdominal ultrasound for colon cancer — Abdominal pelvic CT scan for rectal cancer — Other CT scans as appropriate (metastases) — Other CT scans as appropriate (metastases) --- MRI, … etc if needed … --- MRI, … etc if needed …
RECTAL CANCER Sigmoidoscopy All rights reserved Dr Ligoury, CNRI.
COLORECTAL CANCER Symptomatology and evolution 1) EARLY STAGES No symptomsNo symptoms Abdominal painAbdominal pain FlatulenceFlatulence Minor changes in bowel movementsMinor changes in bowel movements Rectal bleedingRectal bleeding AnemiaAnemia Constipation or diarrheaConstipation or diarrhea Abdominal pain (colicky pain)Abdominal pain (colicky pain) Obstructive symptoms (nausea/vomiting)Obstructive symptoms (nausea/vomiting) 3) LATE STAGE RIGHT-SIDE COLON Vague abdominal achingVague abdominal aching Anemia (iron loss by chronic microscopic bleeding)Anemia (iron loss by chronic microscopic bleeding) WeaknessWeakness Weight lossWeight loss Change in bowel movementsChange in bowel movements Rectal fullnessRectal fullness UrgencyUrgency BleedingBleeding TenesmusTenesmus Pelvic pain (later stage)Pelvic pain (later stage) 4) LATE STAGE RECTUM 2) LATE STAGE LEFT-SIDE COLON
COLORECTAL CANCER Symptoms and their frequency Adapted from Metman EH, Bertrand J, Bouleau PH. Rev Prat. 1979; 29(13): Compared frequency of clinical symptoma- tology of colon cancer (from 180 cancers) Weakness Anemia Bleeding Abdominal mass Occlusion Right-side colon cancer Left-side colon cancer Changes in bowel movements Pain 65% 40% 78% 36% 25.5% 7% 11% 0.8% 7% 88% 6.5% 0% 1.6% 7%
COLORECTAL CANCER TNM classification, definition of T (primary tumor) TisT 1 T 2 T 3 T 4 Extension to an adjacent organ Mucosa Muscularis mucosae Submucosa Muscularis propria SubserosaSerosa
COLORECTAL CANCER Usual prognostic factors StageTNM III-IV Age<40 years Performance statusWHO >2 Symptoms+ Duration of symptoms<6 months Obstruction/perforation+ Location of primary tumorRectum/rectosigmoid HistopathologyMucinous (colloid) and signet-ring adenocarcinomas LDH CEA/Other biomarkers>5 ng/mL PloidyAneuploidy Prognostic factor Bad prognosis
COLORECTAL CANCER 5-year postsurgery follow-up guidelines History/examination Every 3-4 mo for 2y and then every 6 mo for 3y Colonoscopy Preoperatively or mo postoperatively, then every mo Chest X-ray Every 6 mo CEA Every 2-4 mo for 2y then every 6 mo for 2y Liver (US) Same Liver chemistries CT scans (chest, abdo, pelvic) Other scans (liver, spleen, bone) Procedure/TestFrequencyComment As indicated by findings on history, examination, or elevated CEA levels Detects one third of recurrences Every 3 years after free of polyps } CEA, serum carcinoembryonic antigen; CT, computed tomography; US, ultrasound
COLORECTAL CANCER Sites and frequency of distant metastases Adapted from: Kemeny N, Seiter K. Colon and rectal carcinoma. In: Handbook of chemotherapy in clinical oncology. SCI ed.1993: Liver38-60% Abdominal lymph nodes 39% Lung38% Peritoneum28% Ovary18% Adrenal glands14% Pleura11% Brain8% Bone10%
ΟΓΚΟΛΟΓΙΚΟΣ ΑΣΘΕΝΗΣ 1.Θα πρέπει να χορηγηθεί θεραπεία ή όχι ; εάν ναι 2.Τι θεραπεία πρέπει να χορηγηθεί ; και 3.Ποιος είναι ο θεραπευτικός στόχος ; - ριζική εκρίζωση της νόσου - συμπληρωματική μετά την εγχείρηση - ανακουφιστική 4.Πότε ; 5.Χρονική διάρκεια ;
ΘΕΡΑΠΕΙΑ ΑΣΘΕΝΩΝ ΜΕ ΚΑΡΚΙΝΟ 1.Εγχείρηση 2.Χημειοθεραπεία 3.Ορμονοθεραπεία 4.Ακτινοθεραπεία 5.Βιολογικές θεραπείες
ΑΣΘΕΝΕΙΣ ΜΕ ΚΑΡΚΙΝΟ : ΣΧΕΔΙΑΣΜΟΣ ΘΕΡΑΠΕΥΤΙΚΗΣ ΠΡΟΣΕΓΓΙΣΗΣ 1.Επιλογή & αξιολόγηση θεραπευτικών παραγόντων 2.Συνδυασμός ή Μονοθεραπεία ; 3.Χορήγηση των ανώτερων δυνατών δόσεων στο συντομότερο χρονικό διάστημα 4.Αξιολόγηση δραστικότητας έγκαιρα...