Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
ΑΝΤΙΜΥΚΗΤΙΑΣΙΚΑ & ΘΕΡΑΠΕΙΑ ΜΥΚΗΤΙΑΣΙΚΩΝ ΛΟΙΜΩΞΕΩΝ
ΓΕΩΡΓΙΟΣ ΠΑΝΟΣ BSc, CEng, MIET, MD, PhD, DTM&H(Lon), FRCP Αν. Καθηγητής Παθολογίας & Λοιμωδών Νοσημάτων Ιατρική Σχολή Παν/μίου Πατρών ΠΓΝΠ
, FRCP. Αν. Καθηγητής Παθολογίας & Λοιμωδών Νοσημάτων. Ιατρική Σχολή Παν/μίου Πατρών. ΠΓΝΠ.")
2
This slide illustrates 4 possible approaches to antifungal therapy, according to degree of risk and/or certainty of diagnosis In patients at highest risk for invasive fungal infection—allogeneic HSCT recipients, for example—antifungal prophylaxis against Candida infection is standard1 ΠΡΩΙΜΗ Empirical therapy may be warranted in high-risk patients who have persistent fever despite broad-spectrum antibacterial therapy, because systemic fungal infection is one possible explanation of the signs of infection1,2 Initiation of presumptive therapy is recommended as soon as a systemic fungal infection is suspected, at the same time that a diagnostic workup is underway to confirm and further characterize the infection3,4 Specific treatment may be initiated once an infection is confirmed and possibly further characterized1,5 Although knowledge of the infecting species, or even susceptibility testing of an individual isolate, may guide antifungal therapy, host factors are often the more critical determinant of the clinical response to antifungal therapy2 References: 1. Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of candidiasis. Clin Infect Dis ;38: 2. Hayes-Lattin B, Maziarz RT. Update in the epidemiology, prophylaxis, and treatment of fungal infections in patients with hematologic disorders. Leuk Lymphoma. 2004;45: 3. Stevens DA, Kan VL, Judson MA, et al. Practice guidelines for diseases caused by Aspergillus. Clin Infect Dis. 2000;30: 4. Dean DA, Burchard KW. Fungal infection in surgical patients. Am J Surg. 1996;171: 5. Denning DW. Invasive aspergillosis. Clin Infect Dis. 1998;26: 2

3
Η επίδραση της καθυστέρησης της θεραπείας σε ασθενείς με καντιταιμία
45 40 35 30 25 Mortality (%) 20 15 The continuing high mortality rate in SCIs may be due to a delay in the initiation of treatment because of uncertainty in diagnosis. This slide shows results from a study in which delayed treatment resulted in an increase in the risk of mortality.1 There is a need to focus on improved diagnosis of fungal infections, so that they can be treated early and adequately to reduce mortality. Garey KW, et al. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin Infect Dis 2006; 43:25–31. 10 5 Culture day Day 1 Day 2 Day 3 Days to start of fluconazole Garey KW, et al. Clin Infect Dis 2006; 43:25–31; published by the University of Chicago Press
 The continuing high mortality rate in SCIs may be due to a delay in the initiation of treatment because of uncertainty in diagnosis. This slide shows results from a study in which delayed treatment resulted in an increase in the risk of mortality.1. There is a need to focus on improved diagnosis of fungal infections, so that they can be treated early and adequately to reduce mortality. Garey KW, et al. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin Infect Dis 2006; 43:25– Culture day. Day 1. Day 2. Day 3. Days to start of fluconazole. Garey KW, et al. Clin Infect Dis 2006; 43:25–31; published by the University of Chicago Press.")
4
Συσχέτιση μεταξύ νοσοκομειακής θνητότητος και χρόνου έναρξης θεραπείας
35 30 25 20 Hospital mortality (%) 15 This study provides further evidence that delayed treatment results in increased mortality.1 There is a need to focus on improved diagnosis of fungal infections, so that they can be treated early and adequately to reduce mortality. Morrell M, et al. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 2005; 49:3640–3645. 10 5 < 12 12–24 24–48 > 48 Delay in start of antifungal treatment (hours) Morrell M, et al. Antimicrob Agents Chemother 2005; 49:3640–5
 15. This study provides further evidence that delayed treatment results in increased mortality.1. There is a need to focus on improved diagnosis of fungal infections, so that they can be treated early and adequately to reduce mortality. Morrell M, et al. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 2005; 49:3640– < –24. 24–48. > 48. Delay in start of antifungal treatment (hours) Morrell M, et al. Antimicrob Agents Chemother 2005; 49:3640–5.")
5
Θνητότης βακτηριαιμίας
ΗΠΑ

6
Θεραπευτικές επιλογές1
Azoles: fluconazole, itraconazole, voriconazole, posaconazole Polyenes amphotericin B and lipid formulations of amphotericin B Flucytosine Echinocandins caspofungin, micafungin, anidulafungin fluconazole voriconazole amphotericin B anidulafungin caspofungin 1- Eggimann P., Garbino J, Pittet D. Management of Candida species infections in critically ill patients. Lancet Infect Dis. 2003;3(12): 6
:")
7
Στόχοι αντιμυκητιασικών φαρμάκων
Cell membrane Fungi use principally ergosterol instead of cholesterol DNA Synthesis Some compounds may be selectively activated by fungi, arresting DNA synthesis. There are key differences between mammalian and fungal eukaryotic cells. This is the basis of drug selectivity. Cell Wall Unlike mammalian cells, fungi have a cell wall Atlas of fungal Infections, Richard Diamond Ed. 1999 Introduction to Medical Mycology. Merck and Co. 2001

8
Στόχοι Cell membrane DNA/RNA synthesis • Pyrimidine analogues
• Polyene antibiotics • Azole antifungals DNA/RNA synthesis • Pyrimidine analogues - Flucytosine Flucytosine is an anti-metabolite type of antifungal drug. It is a synthetic fluorinated pyrimidine which is available for intravenous infusion or oral administration. It is marketed as Ancotil. Cell wall • Echinocandins

9
Γενικά χαρακτηριστικά των αντιμυκητιασικών φαρμάκων
Αμφοτερικίνη Β Ευρύ φάσμα δραστικότητας Κενά στο φάσμα (ανθεκτικά είδη) Δύσκολη φαρμακοκινητική Αποτελεσματικότητα όχι μεγαλύτερη σε σύγκριση με την βορικοναζόλη και τις εχινοκανδίνες Τοξικότητα από την έγχυση Φαρμακευτική τοξικότης (ηπατική, νεφρική, υποκαλιαιμία) Κόστος 9
 Δύσκολη φαρμακοκινητική. Αποτελεσματικότητα όχι μεγαλύτερη σε σύγκριση με την βορικοναζόλη και τις εχινοκανδίνες. Τοξικότητα από την έγχυση. Φαρμακευτική τοξικότης (ηπατική, νεφρική, υποκαλιαιμία) Κόστος. 9.")
10
Amphotericin B deoxycholate
Αντιμυκητιασική δράση Δυνητικά απειλητικές για την ζωή (ανοσοκατασταλμένοι): aspergillosis, cryptococcosis, North American blastomycosis, systemic candidiasis, coccidioidomycosis, histoplasmosis, sporotrichosis, and zygomycosis including mucormycosis Amphotericin B deoxycholate 10
: aspergillosis, cryptococcosis, North American blastomycosis, systemic candidiasis, coccidioidomycosis, histoplasmosis, sporotrichosis, and zygomycosis including mucormycosis. Amphotericin B deoxycholate. 10.")
11
Lipid Amphotericin B Formulations
Abelcet ® ABLC Amphotec ® ABCD Ambisome ® L-AMB Ribbon-like particles Carrier lipids: DMPC, DMPG Particle size (µm): Disk-like particles Carrier lipids: Cholesteryl sulfate Particle size (µm): Unilaminar liposome Carrier lipids: HSPC, DSPG, cholesterol Particle size (µm) : 0.08
: Disk-like particles. Carrier lipids: Cholesteryl sulfate. Particle size (µm): Unilaminar liposome. Carrier lipids: HSPC, DSPG, cholesterol. Particle size (µm) :")
12
Reference Pathogen(s) Agent Response Survival
Lipid AMB formulations vs. Conventional AMB When Used as First-Line Therapy In Prospective Randomized Trials Outcome Reference Pathogen(s) Agent Response Survival Leenders 1998 Mixed L-AMB Same Leenders 1997 Cryptococcus spp. Anaisse 1995 Candida spp. ABLC Bowden 2002 Aspergillus spp. ABCD Hamill 1999 Cryptococcus spp. Johnson 2002 H. capsulatum Greater Grouping together the lipid formulations of amphotericin as alternatives to conventional amphotericin B for empirical antifungal therapy has been questioned. The best data that address efficacy are from studies that have evaluated the lipid formulations of amphotericin as treatment for documented infection. Six prospective randomized trials have been undertaken in which one of the lipid formulations was compared with conventional amphotericin as treatment for established invasive fungal infection. Unfortunately, some of these studies remain unpublished. This table presents, in brief, data on clinical response rates and overall survival rates from these trials. It shows that none of the lipid formulations has a clear advantage compared with conventional amphotericin B, with 1 exception. In the study performed by Johnson et al 2002, L-AmB was superior to amphotericin B with respect to both clinical response and survival rates in the treatment of histoplasmosis. Wingard. Clin Infect Dis 2002; 35:891-5 12
 Agent Response Survival. Leenders Mixed. L-AMB. Same. Leenders Cryptococcus spp. Anaisse Candida spp. ABLC. Bowden Aspergillus spp. ABCD. Hamill Cryptococcus spp. Johnson H. capsulatum. Greater. Grouping together the lipid formulations of amphotericin as alternatives to conventional amphotericin B for empirical antifungal therapy has been questioned. The best data that address efficacy are from studies that have evaluated the lipid formulations of amphotericin as treatment for documented infection. Six prospective randomized trials have been undertaken in which one of the lipid formulations was compared with conventional amphotericin as treatment for established invasive fungal infection. Unfortunately, some of these studies remain unpublished. This table presents, in brief, data on clinical response rates and overall survival rates from these trials. It shows that none of the lipid formulations has a clear advantage compared with conventional amphotericin B, with 1 exception. In the study performed by Johnson et al 2002, L-AmB was superior to amphotericin B with respect to both clinical response and survival rates in the treatment of histoplasmosis. Wingard. Clin Infect Dis 2002; 35:")
13
Lipid AMB Formulations-Summary
Efficacy Lipid formulation > AMB-deoxy Nephrotoxicity L-AMB < ABLC < ABCD << AMB-deoxy Infusion related toxicity L-AMB < ABLC < ABCD < AMB-deoxy Product cost (AWP) L-AMB > ABLC > ABCD > AMB-deoxy The 3 lipid-based formulations represent a significant advance in antifungal therapy. While superior clinical efficacy of these drugs over AmBD for any fungal disease has not been clearly established, the lower toxicity profile of lipid-based agents is an attractive feature. All 3 drugs are less nephrotoxic than AmBD and 1 of the drugs (L-AmB) is clearly associated with fewer infusion-related adverse events than AmBD. A clear advantage of a lipid based product is where there is poor or no central venous access. The high cost of the lipid-based drugs is the major factor that limits their utilization and well designed pharmacoeconomic studies would be of significant value. The daily treatment costs based on the 1999 average wholesale price for amphotericin B products are as follows: AmBD 1 mg/kg $25, ABLC 5 mg/kg $776, ABCD 4 mg/kg $480, and L-AmB 3 mg/kg $942. As a general rule, these agents should not be used as initial therapy for most patients with the various candida syndromes, cryptococcosis and the endemic mycoses (e.g. blastomycosis, histoplasmosis, coccidioidomycosis) unless the patient has preexisting renal dysfunction, has life-threatening, progressive disease, or is refractory to or intolerant of amphotericin B or azole therapy. If it were not for the 10 to 50-fold higher acquisition cost of lipid formulations of AmB, their first-line use would be widely adopted. Thus, the arrival of these agents onto the market has forced institutions to more closely examine secondary costs associated with antifungal therapy e.g. the management of nephrotoxicity with Amphotericin B. An important goal in determining the cost effectiveness of antifungal therapy is finding a balance between primary (acquisition) and secondary costs. 13
 L-AMB > ABLC > ABCD > AMB-deoxy. The 3 lipid-based formulations represent a significant advance in antifungal therapy. While superior clinical efficacy of these drugs over AmBD for any fungal disease has not been clearly established, the lower toxicity profile of lipid-based agents is an attractive feature. All 3 drugs are less nephrotoxic than AmBD and 1 of the drugs (L-AmB) is clearly associated with fewer infusion-related adverse events than AmBD. A clear advantage of a lipid based product is where there is poor or no central venous access. The high cost of the lipid-based drugs is the major factor that limits their utilization and well designed pharmacoeconomic studies would be of significant value. The daily treatment costs based on the 1999 average wholesale price for amphotericin B products are as follows: AmBD 1 mg/kg $25, ABLC 5 mg/kg $776, ABCD 4 mg/kg $480, and L-AmB 3 mg/kg $942. As a general rule, these agents should not be used as initial therapy for most patients with the various candida syndromes, cryptococcosis and the endemic mycoses (e.g. blastomycosis, histoplasmosis, coccidioidomycosis) unless the patient has preexisting renal dysfunction, has life-threatening, progressive disease, or is refractory to or intolerant of amphotericin B or azole therapy. If it were not for the 10 to 50-fold higher acquisition cost of lipid formulations of AmB, their first-line use would be widely adopted. Thus, the arrival of these agents onto the market has forced institutions to more closely examine secondary costs associated with antifungal therapy e.g. the management of nephrotoxicity with Amphotericin B. An important goal in determining the cost effectiveness of antifungal therapy is finding a balance between primary (acquisition) and secondary costs. 13.")
14
Γενικά χαρακτηριστικά των αντιμυκητιασικών φαρμάκων
Αζόλες Fluconazole Δραστικότης έναντι της Candida albicans Ατοξικότης Δοσοεξαρτώμενη δράση Συσσωρευμένη κλινική εμπειρία Αποτελεσματική στην προφύλαξη Voriconazole Δραστικότης έναντι όλων των ειδών της Candida, Aspergillus, Fusarium, Scedosporium IV, Peros χορήγηση Αδυναμία χορήγησης σε νεφρική ανεπάρκεια (IV) Φαρμακευτικές αλληλεπιδράσεις 14
 Φαρμακευτικές αλληλεπιδράσεις. 14.")
15
Global Comparative Candidemia Study In non-neutropenic patients
Kullberg BJ et al, Lancet 2005;366:1435

16
Primary and Secondary Analyses (MITT Population)
GLOBAL COMPARATIVE CANDIDEMIA STUDY Primary and Secondary Analyses (MITT Population) DRC successes at the last evaluable follow-up study visit Voriconazole (N=248) Amphotericin B fluconazole (N=122) 40.72 40.70 65.48 71.33 Success rate (%) P=0.25 As part of the secondary analysis, we ALSO looked at the success rate not only at 12 weeks but also at successes at any other time point if the 12-week visit was not available, as was done in previous Candidemia studies. The success rate as assessed by the blinded data review committee in this analysis was very similar to those from other published studies, and again, did not differ between the treatment arms. (The prespecified statistical analysis plan for this study allowed the application of confidence intervals to the difference in response rates in the primary efficacy analysis only.) Kullberg BJ et al, Lancet 2005;366:1435
 DRC successes at the last evaluable follow-up study visit. Voriconazole (N=248) Amphotericin B fluconazole (N=122) Success rate (%) P=0.25. As part of the secondary analysis, we ALSO looked at the success rate not only at 12 weeks but also at successes at any other time point if the 12-week visit was not available, as was done in previous Candidemia studies. The success rate as assessed by the blinded data review committee in this analysis was very similar to those from other published studies, and again, did not differ between the treatment arms. (The prespecified statistical analysis plan for this study allowed the application of confidence intervals to the difference in response rates in the primary efficacy analysis only.) Kullberg BJ et al, Lancet 2005;366:1435.")
17
Success by Baseline Pathogen
Voriconazole (N=248) Amphotericin B/fluconazole (N=122) 32.1 33.3 33.3 These are the DRC-assessed success rates at the 12-week timepoint, according to Candida species at baseline. 6.3 Kullberg BJ et al, Lancet 2005;366:1435
 Amphotericin B/fluconazole (N=122) These are the DRC-assessed success rates at the 12-week timepoint, according to Candida species at baseline Kullberg BJ et al, Lancet 2005;366:1435.")
18
Kaplan-Meier Survival Curve (MITT Population)
Attributable mortality (deaths caused by candidemia) was 10.9% (27/248) in the voriconazole arm compared with 11.5% (14/122) in the amphotericin B/fluconazole arm 1.0 0.8 0.6 0.4 0.2 0.0 Probability of survival Voriconazole Amphotericin B/fluconazole This Kaplan-Meier plot illustrates that there were more deaths in the amphotericin B arm and the hazard ratio of suggests that there was a trend toward improved survival for patients in the voriconazole arm. The DRC-assessed attributable mortality (deaths caused by candidemia) was 10.9% (27/248) in the voriconazole arm and 11.5% (14/122) in the amphotericin B/fluconazole arm. Hazard Ratio=0.822 95% CI: (0.582, 1.161) 14 13 12 11 10 9 8 7 6 5 4 3 2 1 Time (weeks) Note: the hazard ratio is stratified by region.
 was 10.9% (27/248) in the voriconazole arm compared with 11.5% (14/122) in the amphotericin B/fluconazole arm Probability of survival. Voriconazole. Amphotericin B/fluconazole. This Kaplan-Meier plot illustrates that there were more deaths in the amphotericin B arm and the hazard ratio of suggests that there was a trend toward improved survival for patients in the voriconazole arm. The DRC-assessed attributable mortality (deaths caused by candidemia) was 10.9% (27/248) in the voriconazole arm and 11.5% (14/122) in the amphotericin B/fluconazole arm. Hazard Ratio= % CI: (0.582, 1.161) Time (weeks) Note: the hazard ratio is stratified by region.")
19
Γενικά χαρακτηριστικά αντιμυκητιασικών φαρμάκων Flucytosine
Περιορισμένο φάσμα παρενέργειες Επίκτητη αντοχή > μονοθεραπεία > ταχεία εμφάνιση Flucytosine is active against a limited range of systemic fungal infections, being effective mainly in those caused by yeast. It has activity against Candida spp., C. neoformans and some fungi causing chromoblastomycosis. While flucytosine is in clinical use for these few specific indications, its use alone in treatment frequently results in emergence of resistance. This rapid de-novo resistance occurring during therapy has effectively limited its use in the treatment of candida infections (approx 10% of Candida albicans isolates are resistant before treatment starts), and is a major drawback for this compound. In principle, resistance to 5FC may result from decreased uptake (loss of permease activity) or loss of enzymatic activity responsible for conversion to FUMP. Although resistance due to decreased 5FC uptake has been found in S. cerevisiae and C. glabrata, this mechanism does not seem to be important in C. albicans or Cryptococcus neoformans. The most common cause of resistance appears to be loss of cytosine deaminase or UMP pyrophosphorylase activity.
, and is a major drawback for this compound. In principle, resistance to 5FC may result from decreased uptake (loss of permease activity) or loss of enzymatic activity responsible for conversion to FUMP. Although resistance due to decreased 5FC uptake has been found in S. cerevisiae and C. glabrata, this mechanism does not seem to be important in C. albicans or Cryptococcus neoformans. The most common cause of resistance appears to be loss of cytosine deaminase or UMP pyrophosphorylase activity.")
20
Flucytosine – Κλινική χρήση
μονοθεραπεία : περιορισμένη } Candidiasis Cryptococcosis ?Aspergillosis Σε συνδυασμό με amphotericin B or fluconazole. 5-FC monotherapy is effective in treating infections caused by C. neoformans, Candida spp., and C. glabrata and in chromoblastomycosis. However, the use of 5-FC as a single agent is limited, because of the prevalence of intrinsically resistant strains and the frequent development of resistance during treatment. Monotherapy with 5-FC is now only used in some cases of chromoblastomycosis and in uncomplicated lower urinary tract candidiasis and vaginal candidiasis. In all other cases, 5-FC is used together with other agents, usually amphotericin B, for the treatment of systemic mycoses. Used in combination, these antifungals are more effective. The underlying reason for this synergistic action is not clear. However, it is possible that when using amphotericin B, flucytosine penetration through amphotericin B-damaged fungal cell membranes is increased.

21
Γενικά χαρακτηριστικά των αντιμυκητιασικών φαρμάκων
Eχινοκανδίνες Αντιμυκητιασικό φάσμα έναντι των συνηθεστέρων μυκήτων της καθημερινής κλινικής πράξης Ατοξικότης Όχι σημαντικές αλληλεπιδράσεις Όχι ανάγκη προσαρμογής δοσολογίας 21

22
Echinocandins-Spectrum vs. Yeast and Moulds
Fungicidal vs. Candida spp. including many fluconazole-resistant species C. albicans = C. tropicalis = C. glabrata = C. krusei < C. parapsilosis = C. lusitaniae Active against Aspergillus species No activity against C. neoformans, zygomycetes The optimal first-line treatment for serious candida infections is a controversial issue. Amphotericin B has served as standard treatment for five decades, but toxic effects often limit its use. Prospective, randomized studies have shown that fluconazole is as effective as amphotericin B, with superior safety, for the treatment of candida infections. However, certain non-albicans candida species, which account for over half the cases, are less susceptible to fluconazole. The need remains for new agents to treat serious candida infections. One alternative is caspofungin. The next few slides show results of studies investigating the effectiveness of caspofungin against: Planktonic candida albicans Biofilm candida albicans Mucosal candida albicans Invasive aspergillosis Invasive candida albicans (compared to AmB) The mode of action of the echinocandins means they possess an unusual extended spectrum of activity. They are active against Candida spp. isolates that are resistant to the azoles and amphotericin B. About 10 % of Candida species are not killed by echinocandins and Candida parapsilosis, C.guilliermondii and C. lusitaniae are slightly less susceptible then other species. They are not active at all against Cryptococcus neoformans, since this pathogen has little or no β(1,3)- -D-glucan synthase enzyme. On the other hand, they are very active against Pneumocystis carinii. (unlike other antifungal agents) because the wall of the ‘cyst’ form of this fungus contains β(1,3)- -D-glucan synthase. They have a fungicidal action. Kuhn et al used confocal scanning laser microscopy (CSLM) to image the effects, on cell structure, of drug exposure on planktonic (free floating) C. albicans cells. These images utilize CAAF and FUN-1 staining. FUN-1 is a fluorescent dye taken up by fungal cells; in the presence of metabolic viability it is converted from a diffuse yellow cytoplasmic stain to red, rod-like dye aggregates. However, it remains yellow in metabolically inactive, nonviable cells. Concanavalin A-alexa fluor 488 conjugate (CAAF) selectively binds to polysaccharides. Therefore, green CAAF staining highlights blastospore cell walls. Cells in slide B had been exposed to caspofungin for 24 hrs. Slide A shows untreated control cells. Caspofungin-treated cells exhibit grossly distorted cell walls, with minimal cytoplasmic staining and no evidence of viability. i.e. echinocandins are effective against planktonic Candida spp. Kuhn et al. Antimicrob Agent Chemother 2002;46: 22
 The mode of action of the echinocandins means they possess an unusual extended spectrum of activity. They are active against Candida spp. isolates that are resistant to the azoles and amphotericin B. About 10 % of Candida species are not killed by echinocandins and Candida parapsilosis, C.guilliermondii and C. lusitaniae are slightly less susceptible then other species. They are not active at all against Cryptococcus neoformans, since this pathogen has little or no β(1,3)- -D-glucan synthase enzyme. On the other hand, they are very active against Pneumocystis carinii. (unlike other antifungal agents) because the wall of the ‘cyst’ form of this fungus contains β(1,3)- -D-glucan synthase. They have a fungicidal action. Kuhn et al used confocal scanning laser microscopy (CSLM) to image the effects, on cell structure, of drug exposure on planktonic (free floating) C. albicans cells. These images utilize CAAF and FUN-1 staining. FUN-1 is a fluorescent dye taken up by fungal cells; in the presence of metabolic viability it is converted from a diffuse yellow cytoplasmic stain to red, rod-like dye aggregates. However, it remains yellow in metabolically inactive, nonviable cells. Concanavalin A-alexa fluor 488 conjugate (CAAF) selectively binds to polysaccharides. Therefore, green CAAF staining highlights blastospore cell walls. Cells in slide B had been exposed to caspofungin for 24 hrs. Slide A shows untreated control cells. Caspofungin-treated cells exhibit grossly distorted cell walls, with minimal cytoplasmic staining and no evidence of viability. i.e. echinocandins are effective against planktonic Candida spp. Kuhn et al. Antimicrob Agent Chemother 2002;46:")
23
In vitro δραστικότης μυκητοκτόνος δράση εναντίον των ειδών Candida
- Candida albicans, Candida glabrata, Candida tropicalis, and Candida krusei (MIC90 ≤ 0.12 µg/mL) - Candida parapsilosis, Candida lusitaniae (MIC90, 0.5 µg/ml to 2.0 µg/ml) - (Στελέχη ανθεκτικά στη φλουκοναζόλη) 1- Pfaller M.A., Boyken L., Hollis R.J., Messer S.A., Tendolkar S., Diekema D.J. In vitro activities of anidulafungin against more than 2,500 clinical isolates of Candida spp., including 315 isolates resistant to fluconazole. J Clin Microbiol. 2005;43: 23
 - Candida parapsilosis, Candida lusitaniae (MIC90, 0.5 µg/ml to 2.0 µg/ml) - (Στελέχη ανθεκτικά στη φλουκοναζόλη) 1- Pfaller M.A., Boyken L., Hollis R.J., Messer S.A., Tendolkar S., Diekema D.J. In vitro activities of anidulafungin against more than 2,500 clinical isolates of Candida spp., including 315 isolates resistant to fluconazole. J Clin Microbiol. 2005;43:")
24
Caspofungin vs. Amphotericin B Deoxycholate in the Treatment of Invasive Candidiasis in Neutropenic and Non-Neutropenic Patients Caspofungin 70 mg day #1, then 50 mg QD vs. AMB-D mg/kg/q24h CAS [95% CI] AMB Difference adjusted for stratification MITT 71/115 (74%) [65-82] 71/115 (62%) [53-71] 12.7% [ ] End of Therapy response * 71/88 (81%) [72-89] 63/97 (65%) [55-75] 15.4% [ ] A double-blind trial to compare caspofungin with amphotericin B deoxycholate for the primary treatment of invasive candidiasis was performed. The presence or absence of neutropenia was assessed and patients were randomly assigned to receive either intravenous caspofungin or amphotericin B. Of the 239 patients enrolled, 224 were included in the modified intention-to-treat analysis. A modified intention-to-treat analysis showed that the efficacy of caspofungin was similar to that of amphotericin B, with successful outcomes in 73.4 percent of the patients treated with caspofungin and in 61.7 percent of those treated with amphotericin B (difference after adjustment for APACHE II score and neutropenic status, 12.7 percentage points). An analysis of patients who met pre-specified criteria for evaluation showed that caspofungin was superior, with a favorable response in 80.7 percent of patients, as compared with 64.9 percent of those who received amphotericin B (difference, 15.4 percentage points) There were significantly fewer drug-related adverse events in the caspofungin group than in the amphotericin B group. * P < 0.05, secondary analysis Mora-Duarte et al. NEJM Volume 348:
 [65-82] 71/115 (62%) [53-71] 12.7% [ ] End of Therapy response * 71/88 (81%) [72-89] 63/97 (65%) [55-75] 15.4% [ ] A double-blind trial to compare caspofungin with amphotericin B deoxycholate for the primary treatment of invasive candidiasis was performed. The presence or absence of neutropenia was assessed and patients were randomly assigned to receive either intravenous caspofungin or amphotericin B. Of the 239 patients enrolled, 224 were included in the modified intention-to-treat analysis. A modified intention-to-treat analysis showed that the efficacy of caspofungin was similar to that of amphotericin B, with successful outcomes in 73.4 percent of the patients treated with caspofungin and in 61.7 percent of those treated with amphotericin B (difference after adjustment for APACHE II score and neutropenic status, 12.7 percentage points). An analysis of patients who met pre-specified criteria for evaluation showed that caspofungin was superior, with a favorable response in 80.7 percent of patients, as compared with 64.9 percent of those who received amphotericin B (difference, 15.4 percentage points) There were significantly fewer drug-related adverse events in the caspofungin group than in the amphotericin B group. * P < 0.05, secondary analysis. Mora-Duarte et al. NEJM Volume 348:")
25
Νεότερα αντιμυκητιασικά φάρμακα
Πολυένια ABLC, ABCD, AmBisome liposomal nystatin inhaled amphotericin B Αζόλες itraconazole (i.v.) voriconazole posaconazole ravuconazole BAL 8557/4815 Εχινοκανδίνες caspofungin micafungin anidulafungin Aminocandin
 voriconazole. posaconazole. ravuconazole. BAL 8557/4815. Εχινοκανδίνες. caspofungin. micafungin. anidulafungin. Aminocandin.")
26
Chemical structures of the licensed and new azoles and echinocandins
Pasqualotto, A. C. et al. J. Antimicrob. Chemother :i19-30i; Copyright restrictions may apply.

27
Posaconazole

28
Posaconazole Προφύλαξη In vitro δραστικότης παρόμοια με voriconazole
Όχι ένδειξη για συστηματική καντιντίαση Μόνο στοματοφαρυγγική καντιντίαση 200 mg X4 400 mg X2

29
Posaconazole Salvage Therapy for Invasive Aspergillosis
Open, salvage therapy; historical controls refractory or intolerant of standard therapy Posaconazole: Oral solution (200mg qid X 2 wk/400mg bid) Adverse events: 4-10% (Headache, abdominal pain, nausea, liver enzyme elevations) Aspergillus species Posaconazole (n) Historical Controls (n) All Aspergillus 42% (107) 26% (86) A. fumigatus 41% (29) 35% (34) A. flavus 53% (19) 19% (16) A. terreus 29% (14) 18% (11) Raad I, et al. ICAAC 2004 (Abstract M-669)
 Adverse events: 4-10% (Headache, abdominal pain, nausea, liver enzyme elevations) Aspergillus species. Posaconazole (n) Historical Controls (n) All Aspergillus. 42% (107) 26% (86) A. fumigatus. 41% (29) 35% (34) A. flavus. 53% (19) 19% (16) A. terreus. 29% (14) 18% (11) Raad I, et al. ICAAC 2004 (Abstract M-669)")
30
In vitro activity1 Minimum inhibitory concentrations of the echinocandins against Candida species Anidulafungin Micafungin* Caspofungin Candida species MIC50 (µg/ml) MIC90 albicans 0.03 0.06-1 glabrata 0.13 0.03-1 0.06-2 tropicalis 0.06 0.25-1 dubliniensis 0.033 0.5 krusei 0.12-2 0.25-2 lusitaniae 0.25 2 0.5-1 1-2 parapsilosis 1 1-4 guilliermondii ND 2 -> 8 * Micafungin has not yet been approved in the EU. 1- Cappelletty D. et al. Reviews of therapeutics : the echinocandins Pharmacotherapy 2007, 27(3): 30
 MIC90. albicans glabrata tropicalis dubliniensis krusei lusitaniae parapsilosis guilliermondii. ND. 2 -> 8. * Micafungin has not yet been approved in the EU. 1- Cappelletty D. et al. Reviews of therapeutics : the echinocandins Pharmacotherapy 2007, 27(3):")
31
Aνιντουλαφουνγκίνη Θεραπεία της εν τω βάθει Καντιντίασης

32
Anidulafungin – Χαρακτηριστικά
Το νεώτερο αντιμυκητιασικό Επιθυμητή φαρμακοκινητική Δραστικό εναντίον της Candida albicans και ειδών non- albicans 1 Όχι ηπατικός ή νεφρικός μεταβολισμός 1 Όχι προσαρμογή δοσολογίας σε ηπατική ή νεφρική ανεπάρκεια1 Δεν αναφέρονται φαρμακευτικές αλληλεπιδράσεις1 1- Ecalta SPC. 2-Reboli A.C., Rotstein C., Pappas P.G., Chapman S.W., Kett D.H., Kumar D., Betts R., Wible M., Goldstein B.P., Schranz J., Krause D.S., Walsh T.J. Anidulafungin Study Group. Anidulafungin versus fluconazole for invasive candidiasis. N Engl J Med. 2007;356(24): 32
:")
33
Μηχανισμός δράσης1-4 Anidulafungin: Αναστολή της σύνθεσης της 1,3-β-D – γλυκάνης 4 Glucan is essential to fungal cell wall integrity2-4 Without it, fungal cells are osmotically fragile and easily lysed4 1- ECALTA® SPC. 2- Odds F.C., Brown A.J.P., Gow N.A.R. Antifungal agents: mechanism of action. Trends Microbiol. 2003;11: Debono M., Turner W.W., LaGrandeur L. et al. Semisynthetic chemical modification of the antifungal lipopeptide echinocandin B (ECB): structure-activity studies of the lipophilic and geometric parameters of polyarylated acyl analogs of ECB. J Med Chem. 1995;38(17): Raasch R.H. Anidulafungin: review of a new echinocandin antifungal agent. Expert Rev Anti Infect Ther. 2004;2: 33
: structure-activity studies of the lipophilic and geometric parameters of polyarylated acyl analogs of ECB. J Med Chem. 1995;38(17): Raasch R.H. Anidulafungin: review of a new echinocandin antifungal agent. Expert Rev Anti Infect Ther. 2004;2:")
34
In vitro δραστικότης Anidulafungin : μυκητοκτόνος δράση εναντίον των ειδών Candida - Candida albicans, Candida glabrata, Candida tropicalis, and Candida krusei (MIC90 ≤ 0.12 µg/mL) - Candida parapsilosis, Candida lusitaniae (MIC90, 0.5 µg/ml to 2.0 µg/ml) - (Στελέχη ανθεκτικά στη φλουκοναζόλη) 1- Pfaller M.A., Boyken L., Hollis R.J., Messer S.A., Tendolkar S., Diekema D.J. In vitro activities of anidulafungin against more than 2,500 clinical isolates of Candida spp., including 315 isolates resistant to fluconazole. J Clin Microbiol. 2005;43: 34
 - Candida parapsilosis, Candida lusitaniae (MIC90, 0.5 µg/ml to 2.0 µg/ml) - (Στελέχη ανθεκτικά στη φλουκοναζόλη) 1- Pfaller M.A., Boyken L., Hollis R.J., Messer S.A., Tendolkar S., Diekema D.J. In vitro activities of anidulafungin against more than 2,500 clinical isolates of Candida spp., including 315 isolates resistant to fluconazole. J Clin Microbiol. 2005;43:")
36
Primary endpoint1 Global success at the end of IV therapy
Anidulafungin demonstrated superiority vs fluconazole: Significantly greater response rate in the anidulafungin group Difference: 15.4% (95% CI: 3.9% to 27.0%) Mean (median) duration of IV therapy: fluconazole: (11) days anidulafungin: (14) days 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:
 Mean (median) duration of IV therapy: fluconazole: 12.1 (11) days. anidulafungin: 13.5 (14) days. 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:")
37
Secondary endpoint1 (2) Global per-pathogen success at the end of IV therapy 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:

38
Secondary endpoint1 (3) At the end of intravenous therapy, persistent infection was documented in: 8 patients (6.3%) in the anidulafungin group 17 patients (14.4%) in the fluconazole group (P = 0.06) Kaplan–Meier estimates of survival The median time to death was 21 days in the anidulafungin group 14 days in the fluconazole group More patients died in the fluconazole group (37 of 118: 31.4%) than in the anidulafungin group (29 of 127: 22.8% (P = 0.13) 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:
 in the fluconazole group (P = 0.06) Kaplan–Meier estimates of survival. The median time to death was. 21 days in the anidulafungin group. 14 days in the fluconazole group. More patients died in the fluconazole group (37 of 118: 31.4%) than in the anidulafungin group (29 of 127: 22.8% (P = 0.13) 1- Reboli A.C., Rotstein C., Pappas P.G. et al. Anidulafungin versus Fluconazole for Invasive Candidiasis. N Engl J Med 2007;356:")
39
Μικαφουνγκίνη REVIEWS OF ANTI-INFECTIVE AGENTS • CID 2006:42 (15 April) • 1171
 • 1171")
40
Micafungin MYCAMINE® (micafungin sodium)
")
41
Mechanism of action Micafungin inhibits 1,3-β-D-glucan synthesis
1,3-β-D-glucan forms helically intertwined chains that are essential to cell wall rigidity Inhibition of 1,3-β-D-glucan synthesis results in destabilisation of the cell wall, eventually causing cell lysis Depletion of 1,3-β-D-glucan resulting in cell wall destabilisation As an echinocandin, micafungin targets the cell wall of fungi. Micafungin acts by inhibiting the enzyme 1,3-β-D-glucan synthase. The normal function of this enzyme is the synthesis of 1,3-β-D-glucan, a polymer of glucose that forms fibrils comprised of three helically intertwined polysaccharide chains. These fibrils are essential to the rigidity of the cell wall.1,2 Inhibition of 1,3-β-D-glucan synthase prevents assembly of these fibrils and the resulting changes in the composition of the cell wall cause destabilisation of the cell wall structure and, eventually, cell lysis.3 Groll AH, et al. Micafungin: pharmacology, experimental therapeutics and clinical applications. Expert Opin Investig Drugs 2005; 14:489–509. Kurtz MB & Douglas CM. Lipopeptide inhibitors of fungal glucan synthase. J Med Vet Mycol 1997; 35:79–86. Ghannoum MA & Rice LB. Antifungal agents: mode of action, mechanisms of resistance, and correlation of these mechanisms with bacterial resistance. Clin Microbiol Rev 1999; 12:501–517. Inhibition of 1,3-β-D-glucan synthase Micafungin

42
Structure of the 1,3-β-D-glucan synthase enzyme, revealing the site of action of micafungin
Catalytic subunit (Fks) 1,3-β-D-glucan Exoplasm Plasma membrane As shown on this slide, the 1,3-β-D-glucan synthase enzyme is a complex of at least two different components: the catalytic subunit Fks1p/Fks2p and the soluble regulatory subunit Rho1GTPase.1,2 It is not known exactly how micafungin interacts with the enzyme complex but it is hypothesised that the drug interacts with the Fks1p subunit, since mutations in the FKS1 gene have been linked with micafungin resistance.3 The exact mode of action may be either inhibition of the priming reaction for initiation of 1,3-β-D-glucan synthesis or prevention of chain elongation once synthesis has begun.1 Inhibition of 1,3-β-D-glucan synthase is unlikely to result in mechanism-based toxicity, since this enzyme is not found in mammals. Kurtz MB & Douglas CM. Lipopeptide inhibitors of fungal glucan synthase. J Med Vet Mycol 1997; 35:79–86. Denning DW. Echinocandin antifungal drugs. Lancet 2003; 362:1142–1151. Laverdiere M, et al. Progressive loss of echinocandin activity following prolonged use for treatment of Candida albicans oesophagitis. J Antimicrob Chemother 2006; 57:705–708. UDP Soluble regulatory subunit (Rho1) Micafungin blocks this reaction Cytoplasm Kurtz MB & Douglas CM. J Med Vet Mycology 1997; 35:79–86 UDP = uridine diphosphate
 1,3-β-D-glucan. Exoplasm. Plasma membrane. As shown on this slide, the 1,3-β-D-glucan synthase enzyme is a complex of at least two different components: the catalytic subunit Fks1p/Fks2p and the soluble regulatory subunit Rho1GTPase.1,2. It is not known exactly how micafungin interacts with the enzyme complex but it is hypothesised that the drug interacts with the Fks1p subunit, since mutations in the FKS1 gene have been linked with micafungin resistance.3. The exact mode of action may be either inhibition of the priming reaction for initiation of 1,3-β-D-glucan synthesis or prevention of chain elongation once synthesis has begun.1. Inhibition of 1,3-β-D-glucan synthase is unlikely to result in mechanism-based toxicity, since this enzyme is not found in mammals. Kurtz MB & Douglas CM. Lipopeptide inhibitors of fungal glucan synthase. J Med Vet Mycol 1997; 35:79–86. Denning DW. Echinocandin antifungal drugs. Lancet 2003; 362:1142–1151. Laverdiere M, et al. Progressive loss of echinocandin activity following prolonged use for treatment of Candida albicans oesophagitis. J Antimicrob Chemother 2006; 57:705–708. UDP. Soluble regulatory subunit (Rho1) Micafungin blocks this reaction. Cytoplasm. Kurtz MB & Douglas CM. J Med Vet Mycology 1997; 35:79–86. UDP = uridine diphosphate.")
43
In vitro activity of micafungin against Candida spp.
Organism Study 1* Study 2† No. of isolates MIC50 (µg/ml) MIC90 (µg/ml) C. albicans 2,869 0.015 0.03 404 0.06 C. glabrata 747 157 C. tropicalis 625 62 0.125 C. parapsilosis 759 1 2 109 C. krusei 136 0.12 21 0.25 C. kefyr 37 C. guilliermondii 61 0.5 27 C. lusitaniae 58 12 C. famata 24 – C. haemulonii C. fermentati 10 Candida spp. 30 Total 5,346 862 In two separate studies, micafungin has demonstrated potent in vitro activity against Candida spp., including both C. albicans and non-albicans Candida species.1,2 Pfaller MA, et al. In vitro susceptibility of invasive isolates of Candida spp. to anidulafungin, caspofungin, and micafungin: six years of global surveillance. J Clin Microbiol 2008; 46:150–156. Dannaoui E, et al. Comparative in vitro activities of caspofungin and micafungin, determined using the method of the European Committee on Antimicrobial Susceptibility Testing, against yeasts isolates obtained in France in Antimicrob Agents Chemother 2008; 52:778–781. *Pfaller MA, et al. J Clin Microbiol 2008; 46:150–6; †Dannaoui E, et al. Antimicrob Agents Chemother 2008; 52:778–81
 MIC90 (µg/ml) C. albicans. 2, C. glabrata C. tropicalis C. parapsilosis C. krusei C. kefyr. 37. C. guilliermondii C. lusitaniae C. famata. 24. – C. haemulonii. C. fermentati. 10. Candida spp. 30. Total. 5, In two separate studies, micafungin has demonstrated potent in vitro activity against Candida spp., including both C. albicans and non-albicans Candida species.1,2. Pfaller MA, et al. In vitro susceptibility of invasive isolates of Candida spp. to anidulafungin, caspofungin, and micafungin: six years of global surveillance. J Clin Microbiol 2008; 46:150–156. Dannaoui E, et al. Comparative in vitro activities of caspofungin and micafungin, determined using the method of the European Committee on Antimicrobial Susceptibility Testing, against yeasts isolates obtained in France in Antimicrob Agents Chemother 2008; 52:778–781. *Pfaller MA, et al. J Clin Microbiol 2008; 46:150–6; †Dannaoui E, et al. Antimicrob Agents Chemother 2008; 52:778–81.")
44
In vitro activity of micafungin against Candida spp
In vitro activity of micafungin against Candida spp. – comparison with other echinocandins Organism MIC90 (µg/ml) Number of isolates Micafungin Caspofungin Anidulafungin C. albicans 2,869 0.03 0.06 C. parapsilosis 759 2 1 C. glabrata 747 0.015 0.12 C. tropicalis 625 C. krusei 136 0.25 C. guilliermondii 61 C. lusitaniae 58 0.5 C. kefyr 37 C. famata 24 Candida spp. 30 Total 5,346 Micafungin is more potent in vitro than both caspofungin and anidulafungin against C. glabrata and remained active against a strain of C. glabrata that was non-susceptible to both anidulafungin and caspofungin.1 Micafungin has also been shown to be active against isolates with acquired or inherent resistance to polyenes and azoles.1 Pfaller MA, et al. In vitro susceptibility of invasive isolates of Candida spp. to anidulafungin, caspofungin, and micafungin: six years of global surveillance. J Clin Microbiol 2008; 46:150–156. Pfaller MA, et al. J Clin Microbiol 2008; 46:150–6
 Number of isolates. Micafungin. Caspofungin. Anidulafungin. C. albicans. 2, C. parapsilosis C. glabrata C. tropicalis C. krusei C. guilliermondii. 61. C. lusitaniae C. kefyr. 37. C. famata. 24. Candida spp. 30. Total. 5,346. Micafungin is more potent in vitro than both caspofungin and anidulafungin against C. glabrata and remained active against a strain of C. glabrata that was non-susceptible to both anidulafungin and caspofungin.1. Micafungin has also been shown to be active against isolates with acquired or inherent resistance to polyenes and azoles.1. Pfaller MA, et al. In vitro susceptibility of invasive isolates of Candida spp. to anidulafungin, caspofungin, and micafungin: six years of global surveillance. J Clin Microbiol 2008; 46:150–156. Pfaller MA, et al. J Clin Microbiol 2008; 46:150–6.")
45
Micafungin licensed indications
The indications of micafungin can be summarised as follows: In adults and children (including infants < 12 months of age and premature neonates) for: the treatment of invasive candidiasis prophylaxis of Candida infection in patients undergoing allogeneic haematopoietic stem cell transplantation or patients who are expected to have neutropenia (absolute neutrophil count < 500 cells/µl) for ≥ 10 days It is also approved for the treatment of oesophageal candidiasis in adult patients (including adolescents ≥ 16 years of age and the elderly) for whom intravenous therapy is appropriate Micafungin is now approved for use in adults and children (including infants < 12 months of age and premature neonates) for the treatment of invasive candidiasis and for prophylaxis of Candida infection in patients undergoing allogeneic haematopoietic stem cell transplantation (HSCT) or patients who are expected to have neutropenia (absolute neutrophil count < 500 cells/µl) for ≥ 10 days. Micafungin is also approved in adults (including adolescents ≥ 16 years of age and the elderly) for the treatment of oesophageal candidiasis in patients for whom intravenous therapy is appropriate. The decision to use micafungin should take into account a potential risk for the development of liver tumours (rat finding). Micafungin should therefore only be used if other antifungals are not appropriate. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September 2008. MYCAMINE® (micafungin sodium) for injection SmPC. Astellas Pharma Europe Ltd., September 2008
 for: the treatment of invasive candidiasis. prophylaxis of Candida infection in patients undergoing allogeneic haematopoietic stem cell transplantation or patients who are expected to have neutropenia (absolute neutrophil count < 500 cells/µl) for ≥ 10 days. It is also approved for the treatment of oesophageal candidiasis in adult patients (including adolescents ≥ 16 years of age and the elderly) for whom intravenous therapy is appropriate. Micafungin is now approved for use in adults and children (including infants < 12 months of age and premature neonates) for the treatment of invasive candidiasis and for prophylaxis of Candida infection in patients undergoing allogeneic haematopoietic stem cell transplantation (HSCT) or patients who are expected to have neutropenia (absolute neutrophil count < 500 cells/µl) for ≥ 10 days. Micafungin is also approved in adults (including adolescents ≥ 16 years of age and the elderly) for the treatment of oesophageal candidiasis in patients for whom intravenous therapy is appropriate. The decision to use micafungin should take into account a potential risk for the development of liver tumours (rat finding). Micafungin should therefore only be used if other antifungals are not appropriate. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September MYCAMINE® (micafungin sodium) for injection SmPC. Astellas Pharma Europe Ltd., September")
46
Comparison of approved indications in Europe for the echinocandins
Micafungin1* Caspofungin2 Anidulafungin3 Invasive candidiasis Yes Yes† Neutropenic patients No Paediatric patients Yes‡ ≥ 12 months Neonates Prophylaxis in HSCT patients or expected neutropenic patients Adults Oesophageal candidiasis in adult patients Invasive aspergillosis Salvage Empiric therapy in febrile neutropenia This table provides a comparison of the approved indications within Europe for micafungin compared with the other approved echinocandins, caspofungin and anidulafungin. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September 2008. CANCIDAS (caspofungin) Summary of Product Characteristics. Merck Sharp & Dohme Ltd., November 2008. ECALTA® (anidulafungin) Summary of Product Characteristics. Pfizer Ltd., October 2007. *The decision to use micafungin should take into account a potential risk for the development of liver tumours (rat finding). Micafungin should therefore only be used if other antifungals are not appropriate.1 †Anidulafungin was studied primarily in patients with candidaemia and only in a limited number of patients with deep tissue Candida infections or abscess-forming disease. ‡Including infants < 12 months of age and premature neonates. 1. MYCAMINE® (micafungin sodium) for injection SmPC. Astellas Pharma Europe Ltd., September 2008; 2. CANCIDAS (caspofungin) SmPC. Merck Sharp & Dohme Ltd, November 2008; 3. ECALTA® (anidulafungin) SmPC. Pfizer Ltd., October 2007
 for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September CANCIDAS (caspofungin) Summary of Product Characteristics. Merck Sharp & Dohme Ltd., November ECALTA® (anidulafungin) Summary of Product Characteristics. Pfizer Ltd., October *The decision to use micafungin should take into account a potential risk for the development of liver tumours (rat finding). Micafungin should therefore only be used if other antifungals are not appropriate.1 †Anidulafungin was studied primarily in patients with candidaemia and only in a limited number of patients with deep tissue Candida infections or abscess-forming disease. ‡Including infants < 12 months of age and premature neonates. 1. MYCAMINE® (micafungin sodium) for injection SmPC. Astellas Pharma Europe Ltd., September 2008; 2. CANCIDAS (caspofungin) SmPC. Merck Sharp & Dohme Ltd, November 2008; 3. ECALTA® (anidulafungin) SmPC. Pfizer Ltd., October")
47
Πλεονεκτήματα του φαρμάκου

48
Micafungin activity against biofilms
Micafungin showed excellent activity against both intermediate- and mature-phase biofilms of two separate Candida albicans strains: ATCC 3153 ATCC 66396 Caspofungin 2 mg/l Micafungin 5 mg/l (a) C. albicans ATCC 3155 (b) C. albicans ATCC 66396 100 100 90 80 70 60 50 40 30 20 10 24h 48h 72h 90 80 Micafungin has excellent activity against Candida species when growing as biofilms, which are commonly found on intravascular catheters and which frequently act as a source of candidaemia.1 A study examined the effects of an antifungal lock strategy (defined as static instillation of a concentrated antifungal solution into the catheter lumen for an extended period) on Candida biofilms. Micafungin solution (5 mg/l) was found to substantially reduce the metabolic activity of both young (12‑hour incubation) and mature (5-day incubation) biofilms of two separate strains of C. albicans. Growth inhibition was maintained for up to 72 hours against young biofilms and for up to 48 hours against mature biofilms.1 Cateau E, et al. In vitro efficacies of caspofungin or micafungin catheter lock solutions on Candida albicans biofilm growth. J Antimicrob Chemother 2008; 62:153–155. 70 60 Biofilm growth inhibition (%) Biofilm growth inhibition (%) 50 40 30 20 10 24h 48h 72h 24h 48h 12 h old biofilm 5 day old biofilm 12 h old biofilm 5 day old biofilm Cateau E, et al. J Antimicrob Chemother 2008; 62:153–5
 C. albicans ATCC (b) C. albicans ATCC h. 48h. 72h Micafungin has excellent activity against Candida species when growing as biofilms, which are commonly found on intravascular catheters and which frequently act as a source of candidaemia.1. A study examined the effects of an antifungal lock strategy (defined as static instillation of a concentrated antifungal solution into the catheter lumen for an extended period) on Candida biofilms. Micafungin solution (5 mg/l) was found to substantially reduce the metabolic activity of both young (12‑hour incubation) and mature (5-day incubation) biofilms of two separate strains of C. albicans. Growth inhibition was maintained for up to 72 hours against young biofilms and for up to 48 hours against mature biofilms.1. Cateau E, et al. In vitro efficacies of caspofungin or micafungin catheter lock solutions on Candida albicans biofilm growth. J Antimicrob Chemother 2008; 62:153– Biofilm growth inhibition (%) Biofilm growth inhibition (%) h. 48h. 72h. 24h. 48h. 12 h old biofilm. 5 day old biofilm. 12 h old biofilm. 5 day old biofilm. Cateau E, et al. J Antimicrob Chemother 2008; 62:153–5.")
49
In vivo drug–drug interaction studies with micafungin in healthy subjects
Class Effect of micafungin on metabolism of co-administered drug Effect of co-administered drug on metabolism of micafungin Mycophenolate mofetil1 Cyclosporin1 Tacrolimus2 Immunosuppressant None Prednisolone1 Corticosteroid Ritonavir1 Antiviral Rifampicin1 Antibacterial Amphotericin B3 Voriconazole4 Fluconazole1 Antifungals Nifedipine1 Calcium channel blocker When co-administered with micafungin: monitor for toxicity reduce dose (if necessary) Sirolimus1 Itraconazole5 Antifungal Patients with invasive fungal infections are often seriously ill, with many underlying conditions, and are likely to be receiving treatment with several concomitant medications of different classes. It is therefore important to consider the drug–drug interaction profile of an antifungal drug. Echinocandins are poor substrates for CYP450 enzymes and do not inhibit P-glycoprotein. This results in a lower potential for drug–drug interactions than is observed with other antifungal drug, particularly the triazoles.1 Several studies have been conducted to examine possible drug–drug interactions between micafungin and a range of other therapeutic agents. These are summarised in the table. No drug–drug interactions have been reported between micafungin and other highly protein-bound drugs such as warfarin, diazepam, salicylic acid or methotrexate.1 No drug–drug interactions that alter the PK of micafungin have been reported in studies including immunosuppressants, corticosteroids, calcium channel blockers, antivirals, antifungals and antibacterials.2–6 Steady-state concentrations of micafungin are associated with small increases in the area under the concentration-time curve (AUC) of itraconazole, sirolimus and nifedipine (22%, 21% and 18%, respectively).2,3 Patients receiving sirolimus, nifedipine or itraconazole in combination with micafungin should be monitored for sirolimus, nifedipine or itraconazole toxicity and the sirolimus, nifedipine or itraconazole dosage should be reduced if necessary.2 Denning DW. Echinocandin antifungal drugs. Lancet 2003; 362:1142–1151. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd. September 2008. Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009). Hiemenz J, et al. Pharmacokinetic and maximum tolerated dose study of micafungin in combination with fluconazole versus fluconazole alone for prophylaxis of fungal infections in adult patients undergoing a bone marrow or peripheral stem cell transplant. Antimicrob Agents Chemother 2005; 49:1331–1336. Keirns J, et al. Steady-state pharmacokinetics of micafungin and voriconazole after separate and concomitant dosing in healthy adults. Antimicrob Agents Chemother 2007; 51:787–790. Undre N, et al. Amphotericin B does not affect the pharmacokinetics of micafungin (FK463). 17th European Congress of Clinical Microbiology and Infectious Diseases. Munich, Germany, 31 March–3 April 2007; Poster P971. Undre N, et al. Itraconazole does not affect the pharmacokinetics of micafungin (FK463). 17th European Congress of Clinical Microbiology and Infectious Diseases. Munich, Germany, 31 March–3 April 2007; Poster P970. 1. Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009); 2. Hebert MF, et al. J Clin Pharmacol 2005; 45:1018–24; 3. Undre N, et al. 17th ECCMID. Munich, Germany, 31 Mar–3 Apr 2007; Poster P971; 4. Keirns J, et al. Antimicrob Agents Chemother 2007; 51:787–90; 5. Undre N, et al. 17th ECCMID. Munich, Germany, 31 Mar–3 Apr 2007; Poster P970
 Sirolimus1. Itraconazole5. Antifungal. Patients with invasive fungal infections are often seriously ill, with many underlying conditions, and are likely to be receiving treatment with several concomitant medications of different classes. It is therefore important to consider the drug–drug interaction profile of an antifungal drug. Echinocandins are poor substrates for CYP450 enzymes and do not inhibit P-glycoprotein. This results in a lower potential for drug–drug interactions than is observed with other antifungal drug, particularly the triazoles.1. Several studies have been conducted to examine possible drug–drug interactions between micafungin and a range of other therapeutic agents. These are summarised in the table. No drug–drug interactions have been reported between micafungin and other highly protein-bound drugs such as warfarin, diazepam, salicylic acid or methotrexate.1. No drug–drug interactions that alter the PK of micafungin have been reported in studies including immunosuppressants, corticosteroids, calcium channel blockers, antivirals, antifungals and antibacterials.2–6. Steady-state concentrations of micafungin are associated with small increases in the area under the concentration-time curve (AUC) of itraconazole, sirolimus and nifedipine (22%, 21% and 18%, respectively).2,3 Patients receiving sirolimus, nifedipine or itraconazole in combination with micafungin should be monitored for sirolimus, nifedipine or itraconazole toxicity and the sirolimus, nifedipine or itraconazole dosage should be reduced if necessary.2. Denning DW. Echinocandin antifungal drugs. Lancet 2003; 362:1142–1151. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd. September Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009). Hiemenz J, et al. Pharmacokinetic and maximum tolerated dose study of micafungin in combination with fluconazole versus fluconazole alone for prophylaxis of fungal infections in adult patients undergoing a bone marrow or peripheral stem cell transplant. Antimicrob Agents Chemother 2005; 49:1331–1336. Keirns J, et al. Steady-state pharmacokinetics of micafungin and voriconazole after separate and concomitant dosing in healthy adults. Antimicrob Agents Chemother 2007; 51:787–790. Undre N, et al. Amphotericin B does not affect the pharmacokinetics of micafungin (FK463). 17th European Congress of Clinical Microbiology and Infectious Diseases. Munich, Germany, 31 March–3 April 2007; Poster P971. Undre N, et al. Itraconazole does not affect the pharmacokinetics of micafungin (FK463). 17th European Congress of Clinical Microbiology and Infectious Diseases. Munich, Germany, 31 March–3 April 2007; Poster P Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009); 2. Hebert MF, et al. J Clin Pharmacol 2005; 45:1018–24; 3. Undre N, et al. 17th ECCMID. Munich, Germany, 31 Mar–3 Apr 2007; Poster P971; 4. Keirns J, et al. Antimicrob Agents Chemother 2007; 51:787–90; 5. Undre N, et al. 17th ECCMID. Munich, Germany, 31 Mar–3 Apr 2007; Poster P970.")
50
Administration to special populations
There is no requirement for micafungin dose adjustments in special populations Age Gender Renal impairment Mild-to-moderate hepatic impairment1–3 Micafungin has not been studied in patients with severe hepatic impairment2,4 No dose adjustments are required for micafungin with regard to race, gender, renal impairment or mild-to-moderate hepatic impairment.1–3 Micafungin has not been studied in patients with severe hepatic impairment and its use is not recommended in these patients.2,4 Groll AH, et al. Micafungin: pharmacology, experimental therapeutics and clinical applications. Expert Opin Investig Drugs 2005; 14:489–509. Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009). Hebert MF, et al. Concomitant tacrolimus and micafungin pharmacokinetics in healthy volunteers. J Clin Pharmacol 2005; 45:1018–1024. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September 2008. 1. Groll AH, et al. Expert Opin Investig Drugs 2005; 14:489–509; 2. Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009); 3. Hebert MF, et al. J Clin Pharmacol 2005; 45:1018–24; MYCAMINE® (micafungin sodium) for injection SmPC. Astellas Pharma Europe Ltd., September 2008
 for injection US Prescribing Information Available at: (accessed February 2009). Hebert MF, et al. Concomitant tacrolimus and micafungin pharmacokinetics in healthy volunteers. J Clin Pharmacol 2005; 45:1018–1024. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September Groll AH, et al. Expert Opin Investig Drugs 2005; 14:489–509; 2. Astellas Pharma US, Inc. MYCAMINE® (micafungin sodium) for injection US Prescribing Information Available at: (accessed February 2009); 3. Hebert MF, et al. J Clin Pharmacol 2005; 45:1018–24; MYCAMINE® (micafungin sodium) for injection SmPC. Astellas Pharma Europe Ltd., September")
51
Oesophageal candidiasis

52
Summary of micafungin clinical data in oesophageal candidiasis
Study design Comparator Patients Doses Key efficacy results Open-label, dose-finding1 – 120 patients with endoscopically proven oesophagitis 12.5–100 mg/day Clear dose–response pattern with improved efficacy at higher doses Randomised, double-blind, dose–response2 Fluconazole (IV) 245 patients; 185 treated with micafungin and 60 treated with fluconazole Micafungin: 50 mg/day (n = 64); 100 mg/day (n = 62); 150 mg/day (n = 59) Fluconazole: 200 mg/day (n = 60) Endoscopic cure rate: micafungin (pooled 100 mg/day mg/day) 83.5%; fluconazole 86.7% Randomised, double-blind, comparative, non-inferiority, Phase III3 518 patients; 260 treated with micafungin and 258 treated with fluconazole Micafungin: 150 mg/day Fluconazole: 200 mg/day Endoscopic cure rate: micafungin 87.7%; fluconazole 88.0% Micafungin has been evaluated in a number of clinical trials in oesophageal candidiasis.1–3 In an open-label, non-comparative, dose-finding trial, micafungin was effective in clearing or providing improvement in symptoms over a range of doses from 12.5–100 mg and there was a clear dose-response pattern, with higher doses resulting in improved efficacy.1 In a randomised, double-blind, parallel-group, dose–response study of micafungin compared with IV fluconazole in HIV patients with oesophageal candidiasis, the pooled endoscopic cure rate for micafungin doses of 100 mg/day and 150 mg/day was 83.5%; (n = 121) which was equivalent to that seen with fluconazole 200 mg/day (86.7%; n = 60).2 A further, larger, randomised, double-blind, non-inferiority study versus IV fluconazole found that micafungin (150 mg/day) was associated with an endoscopic cure rate of 87.7%, compared with 88.0% with fluconazole. Endoscopic cure rates of 87.7% and 88.0% were recorded for micafungin and fluconazole, respectively.3 Pettengell K, et al. Successful treatment of oesophageal candidiasis by micafungin: a novel systemic antifungal agent. Aliment Pharmacol Ther 2004; 20:475–481. de Wet N, et al. A randomized, double-blind, parallel-group, dose-response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV-positive patients. Clin Infect Dis 2004; 39:842–849. de Wet NT, et al. A randomized, double blind, comparative trial of micafungin (FK463) vs. fluconazole for the treatment of oesophageal candidiasis. Aliment Pharmacol Ther 2005; 21:899–907. 1. Pettengell K, et al. Aliment Pharmacol Ther 2004; 20:475–81; 2. de Wet N, et al. Clin Infect Dis 2004; 39:842–9; 3. de Wet NT, et al. Aliment Pharmacol Ther 2005; 21:899–907
 245 patients; 185 treated with micafungin and 60 treated with fluconazole. Micafungin: 50 mg/day (n = 64); 100 mg/day (n = 62); 150 mg/day (n = 59) Fluconazole: 200 mg/day (n = 60) Endoscopic cure rate: micafungin (pooled 100 mg/day mg/day) 83.5%; fluconazole 86.7% Randomised, double-blind, comparative, non-inferiority, Phase III patients; 260 treated with micafungin and 258 treated with fluconazole. Micafungin: 150 mg/day. Fluconazole: 200 mg/day. Endoscopic cure rate: micafungin 87.7%; fluconazole 88.0% Micafungin has been evaluated in a number of clinical trials in oesophageal candidiasis.1–3. In an open-label, non-comparative, dose-finding trial, micafungin was effective in clearing or providing improvement in symptoms over a range of doses from 12.5–100 mg and there was a clear dose-response pattern, with higher doses resulting in improved efficacy.1. In a randomised, double-blind, parallel-group, dose–response study of micafungin compared with IV fluconazole in HIV patients with oesophageal candidiasis, the pooled endoscopic cure rate for micafungin doses of 100 mg/day and 150 mg/day was 83.5%; (n = 121) which was equivalent to that seen with fluconazole 200 mg/day (86.7%; n = 60).2. A further, larger, randomised, double-blind, non-inferiority study versus IV fluconazole found that micafungin (150 mg/day) was associated with an endoscopic cure rate of 87.7%, compared with 88.0% with fluconazole. Endoscopic cure rates of 87.7% and 88.0% were recorded for micafungin and fluconazole, respectively.3. Pettengell K, et al. Successful treatment of oesophageal candidiasis by micafungin: a novel systemic antifungal agent. Aliment Pharmacol Ther 2004; 20:475–481. de Wet N, et al. A randomized, double-blind, parallel-group, dose-response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV-positive patients. Clin Infect Dis 2004; 39:842–849. de Wet NT, et al. A randomized, double blind, comparative trial of micafungin (FK463) vs. fluconazole for the treatment of oesophageal candidiasis. Aliment Pharmacol Ther 2005; 21:899– Pettengell K, et al. Aliment Pharmacol Ther 2004; 20:475–81; 2. de Wet N, et al. Clin Infect Dis 2004; 39:842–9; 3. de Wet NT, et al. Aliment Pharmacol Ther 2005; 21:899–907.")
53
Systemic Candida infections

54
Phase II micafungin study: global response rate
Efficacy failure patients 90 87.5 80 83.3 79.3 76.0 70 60 50 Response rate (%) 40 30 This study showed treatment success in 105 of 126 (83.3%) patients, with 95 (75.4%) experiencing a complete response (eradication of bloodstream infection and resolution of attributable signs and symptoms). Micafungin was also active in both de novo and efficacy failure patients receiving micafungin alone, with treatment success in 63 of 72 (87.5%) and 19 of 25 (76.0%) patients, respectively. This Phase II trial also demonstrated that treatment success was similar in C. albicans and non-albicans Candida species, including C. glabrata, C. parapsilosis, C. tropicalis and C. krusei. Importantly, > 90% of patients who received 75–150 mg/day micafungin responded to therapy. Ostrosky-Zeichner L, et al. International, open-label, noncomparative, clinical trial of micafungin alone and in combination for treatment of newly diagnosed and refractory candidemia. Eur J Clin Microbiol Infect Dis 2005; 24:654–661. 20 10 De novo patients Micafungin Micafungin Total in combination alone Ostrosky-Zeichner L, et al. Eur J Clin Microbiol Infect Dis 2005; 24:654–61 PP population
 This study showed treatment success in 105 of 126 (83.3%) patients, with 95 (75.4%) experiencing a complete response (eradication of bloodstream infection and resolution of attributable signs and symptoms). Micafungin was also active in both de novo and efficacy failure patients receiving micafungin alone, with treatment success in 63 of 72 (87.5%) and 19 of 25 (76.0%) patients, respectively. This Phase II trial also demonstrated that treatment success was similar in C. albicans and non-albicans Candida species, including C. glabrata, C. parapsilosis, C. tropicalis and C. krusei. Importantly, > 90% of patients who received 75–150 mg/day micafungin responded to therapy. Ostrosky-Zeichner L, et al. International, open-label, noncomparative, clinical trial of micafungin alone and in combination for treatment of newly diagnosed and refractory candidemia. Eur J Clin Microbiol Infect Dis 2005; 24:654– De novo patients Micafungin Micafungin Total in combination alone. Ostrosky-Zeichner L, et al. Eur J Clin Microbiol Infect Dis 2005; 24:654–61. PP population.")
55
Phase III study micafungin vs
Phase III study micafungin vs. L-AmB: overall treatment success by infection site Micafungin L-AmB 100 90.6 90.8 80 84.4 81.5 60 Treatment success rate (%) 40 The efficacy of micafungin was independent of infection site, with high overall treatment response rates in both candidaemia and invasive candidiasis (i.e. an infection at a site other than the bloodstream). Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519–1527. 20 n = 170 n = 32 n = 170 163 32 27 Candidaemia Invasive candidiasis Kuse ER, et al. Lancet 2007; 369:1519–27 PP population
 40. The efficacy of micafungin was independent of infection site, with high overall treatment response rates in both candidaemia and invasive candidiasis (i.e. an infection at a site other than the bloodstream). Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519– n = 170. n = 32. n = Candidaemia. Invasive candidiasis. Kuse ER, et al. Lancet 2007; 369:1519–27. PP population.")
56
Phase III study micafungin vs
Phase III study micafungin vs. L-AmB: overall treatment success by Candida species Micafungin L-AmB 100 95.3 92.3 89.3 88.4 89.7 89.3 89.2 80 86.7 85.7 82.6 83.3 80.0 60 Treatment success rate (%) 40 This slide shows that micafungin was successful in the treatment of both C. albicans and non-albicans Candida species, particularly C. glabrata, C. parapsilosis and C. krusei. Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519–1527. 20 n = 86 84 126 112 23 15 52 43 37 30 6 7 C. albicans Any non- albicans C. glabrata C. tropicalis C. parapsilosis C. krusei Non-albicans Candida spp. Kuse ER, et al. Lancet 2007; 369:1519–27 PP population
 40. This slide shows that micafungin was successful in the treatment of both C. albicans and non-albicans Candida species, particularly C. glabrata, C. parapsilosis and C. krusei. Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519– n = C. albicans. Any non- albicans. C. glabrata. C. tropicalis. C. parapsilosis. C. krusei. Non-albicans Candida spp. Kuse ER, et al. Lancet 2007; 369:1519–27. PP population.")
57
Phase III study micafungin vs
Phase III study micafungin vs. L-AmB: treatment success by neutropenic status Overall Non-neutropenic Neutropenic 100 80 89.6 91.6 89.5 90.3 80.0 74.1 76.3 75.0 60 69.6 71.2 Treatment success rate (%) 59.4 56.0 40 This slide shows the treatment success rates when stratified by neutropenic status. Although no statistical comparison was made of the effect of neutropenia on efficacy, treatment success rates were broadly similar across all patient groups. In the mITT population, 59.4% of neutropenic patients receiving micafungin achieved success versus 56.0% of neutropenic patients receiving L-AmB. the difference in proportions for treatment success between the two treatments was 4.9% (95% CI: –3.0 to 12.8). In the PP population, 75.0% of neutropenic patients who received micafungin achieved treatment success, compared with 80.0% in the L-AmB arm. the difference in proportions for treatment success between the two treatments was only 0.7% (95% CI: –5.3 to 6.7). Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519–1527. 20 n = 247 215 32 247 222 25 202 178 24 190 175 15 Micafungin L-AmB Micafungin L-AmB mITT PP Kuse ER, et al. Lancet 2007; 369:1519–27 mITT = modified intent-to-treat; PP = per-protocol set
 This slide shows the treatment success rates when stratified by neutropenic status. Although no statistical comparison was made of the effect of neutropenia on efficacy, treatment success rates were broadly similar across all patient groups. In the mITT population, 59.4% of neutropenic patients receiving micafungin achieved success versus 56.0% of neutropenic patients receiving L-AmB. the difference in proportions for treatment success between the two treatments was 4.9% (95% CI: –3.0 to 12.8). In the PP population, 75.0% of neutropenic patients who received micafungin achieved treatment success, compared with 80.0% in the L-AmB arm. the difference in proportions for treatment success between the two treatments was only 0.7% (95% CI: –5.3 to 6.7). Kuse ER, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007; 369:1519– n = Micafungin. L-AmB. Micafungin. L-AmB. mITT. PP. Kuse ER, et al. Lancet 2007; 369:1519–27. mITT = modified intent-to-treat; PP = per-protocol set.")
58
Phase III study micafungin vs. caspofungin: treatment success
80 76.4 71.4 72.3 60 Treatment success rate (%) 40 Analysis of the primary efficacy endpoint showed that treatment success rates were comparable between micafungin 100 mg/day, micafungin 150 mg/day and caspofungin, demonstrating similar efficacy across all three treatment arms. Micafungin was associated with treatment success in both candidaemia and deep invasive Candida infections. In the statistical analysis, the 95% CIs for the treatment difference between caspofungin and both micafungin 100 and micafungin 150 had lower bounds that were higher than –15%, the predefined limit of non-inferiority, and were therefore both non-inferior to caspofungin. On the secondary efficacy endpoints, there were no significant differences between the three treatment arms in terms of site of infection or incidence of recurrent invasive fungal infections (relapse) during the post-treatment period. As the lower daily dose of 100 mg/day was as effective as the higher 150 mg dose, 100 mg/day was selected as the dose of choice for the treatment of adult patients with SCIs. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. 20 n = 191 n = 199 n = 188 n = 191 199 188 Micafungin 100 mg/day Micafungin 150 mg/day Caspofungin 50 mg/day* Pappas PG, et al. Clin Infect Dis 2007; 45:883–93 *Loading dose 70 mg; mITT population
 40. Analysis of the primary efficacy endpoint showed that treatment success rates were comparable between micafungin 100 mg/day, micafungin 150 mg/day and caspofungin, demonstrating similar efficacy across all three treatment arms. Micafungin was associated with treatment success in both candidaemia and deep invasive Candida infections. In the statistical analysis, the 95% CIs for the treatment difference between caspofungin and both micafungin 100 and micafungin 150 had lower bounds that were higher than –15%, the predefined limit of non-inferiority, and were therefore both non-inferior to caspofungin. On the secondary efficacy endpoints, there were no significant differences between the three treatment arms in terms of site of infection or incidence of recurrent invasive fungal infections (relapse) during the post-treatment period. As the lower daily dose of 100 mg/day was as effective as the higher 150 mg dose, 100 mg/day was selected as the dose of choice for the treatment of adult patients with SCIs. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883– n = 191. n = 199. n = 188. n = Micafungin 100 mg/day. Micafungin 150 mg/day. Caspofungin 50 mg/day* Pappas PG, et al. Clin Infect Dis 2007; 45:883–93. *Loading dose 70 mg; mITT population.")
59
Phase III study micafungin vs
Phase III study micafungin vs. caspofungin: treatment success by Candida species Micafungin 100 mg/day (n = 191) Micafungin 150 mg/day (n = 199) Caspofungin 50 mg/day* (n = 188) p = 0.07 (NS) 100 90 p = NS p = NS p = NS p = NS p = NS 85.7 88.2 80 77.2 75.9 70 73.5 75.0 75.0 75.0 75.0 69.6 71.6 71.1 71.4 66.7 67.7 60 64.3 60.6 62.5 Treatment success rate (%) 50 40 Micafungin was at least as effective as caspofungin in both C. albicans and non-albicans Candida species and a trend towards higher treatment success rates both in C. glabrata (p = 0.07) and in C. parapsilosis was also observed. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. 30 20 10 n = C. albicans Any non- C. glabrata C. tropicalis C. parapsilosis C. krusei albicans Non-albicans Candida spp. Pappas PG, et al. Clin Infect Dis 2007; 45:883–93 *Loading dose 70 mg; mITT population
 Micafungin 150 mg/day (n = 199) Caspofungin 50 mg/day* (n = 188) p = 0.07 (NS) p = NS. p = NS. p = NS. p = NS. p = NS Treatment success rate (%) Micafungin was at least as effective as caspofungin in both C. albicans and non-albicans Candida species and a trend towards higher treatment success rates both in C. glabrata (p = 0.07) and in C. parapsilosis was also observed. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883– n = C. albicans Any non- C. glabrata C. tropicalis C. parapsilosis C. krusei albicans. Non-albicans Candida spp. Pappas PG, et al. Clin Infect Dis 2007; 45:883–93. *Loading dose 70 mg; mITT population.")
60
Phase III study micafungin vs
Phase III study micafungin vs. caspofungin: treatment success by neutropenic status Overall Non-neutropenic Neutropenic 100 80 81.8 76.4 75.7 73.1 72.3 72.9 60 71.4 63.6 Treatment success rate (%) 52.9 40 No significant differences in treatment success were observed between either dose of micafungin or caspofungin in neutropenic patients. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883–893. 20 n = 191 169 22 199 182 17 188 177 11 Micafungin 100 mg/day Micafungin 150 mg/day Caspofungin 50 mg/day* Pappas PG, et al. Clin Infect Dis 2007; 45:883-93 *Loading dose 70 mg; mITT population
 No significant differences in treatment success were observed between either dose of micafungin or caspofungin in neutropenic patients. Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007; 45:883– n = Micafungin 100 mg/day. Micafungin 150 mg/day. Caspofungin 50 mg/day* Pappas PG, et al. Clin Infect Dis 2007; 45: *Loading dose 70 mg; mITT population.")
61
Paediatric sub-study micafungin vs
Paediatric sub-study micafungin vs. L-AmB: treatment success by primary infection site Micafungin L-AmB 100 80 60 40 20 75.0 76.6 66.7 Treatment success rate (%) The efficacy of micafungin was independent of infection site, with equivalent efficacy to L-AmB in both candidaemia and invasive candidiasis. Queiroz-Telles F, et al. Micafungin versus liposomal amphotericin B for pediatric patients with invasive candidiasis in a randomized double-blind trial. Pediatr Infect Dis J 2008; 27:820–826. 50.0 n = 44 47 4 3 Candidaemia Invasive candidiasis Adapted from Queiroz-Telles F, et al. Pediatr Infect Dis J 2008; 27:820–6 mITT population
 The efficacy of micafungin was independent of infection site, with equivalent efficacy to L-AmB in both candidaemia and invasive candidiasis. Queiroz-Telles F, et al. Micafungin versus liposomal amphotericin B for pediatric patients with invasive candidiasis in a randomized double-blind trial. Pediatr Infect Dis J 2008; 27:820– n = Candidaemia. Invasive candidiasis. Adapted from Queiroz-Telles F, et al. Pediatr Infect Dis J 2008; 27:820–6. mITT population.")
62
Paediatric sub-study micafungin vs
Paediatric sub-study micafungin vs. L-AmB: treatment success by neutropenic status Overall Non-neutropenic Neutropenic 100 80 60 40 20 83 76 77 73 76 72 Treatment success rate (%) The study demonstrated that micafungin was equivalent to L-AmB, with overall treatment success rates on the mITT analysis of 72.9% and 76.0%, respectively. Micafungin showed equivalent efficacy to L-AmB in both neutropenic and non-neutropenic patients. Micafungin showed equivalence to L-AmB across all age groups, including neonates. Micafungin also demonstrated equivalence to L-AmB against all Candida species, including non-albicans Candida species. Queiroz-Telles F, et al. Micafungin versus liposomal amphotericin B for pediatric patients with invasive candidiasis in a randomized double-blind trial. Pediatr Infect Dis J 2008; 27:820–826. n = 48 42 6 50 37 13 Micafungin L-AmB Queiroz-Telles F, et al. Pediatr Infect Dis J 2008; 27:820–6 mITT population
 The study demonstrated that micafungin was equivalent to L-AmB, with overall treatment success rates on the mITT analysis of 72.9% and 76.0%, respectively. Micafungin showed equivalent efficacy to L-AmB in both neutropenic and non-neutropenic patients. Micafungin showed equivalence to L-AmB across all age groups, including neonates. Micafungin also demonstrated equivalence to L-AmB against all Candida species, including non-albicans Candida species. Queiroz-Telles F, et al. Micafungin versus liposomal amphotericin B for pediatric patients with invasive candidiasis in a randomized double-blind trial. Pediatr Infect Dis J 2008; 27:820–826. n = Micafungin. L-AmB. Queiroz-Telles F, et al. Pediatr Infect Dis J 2008; 27:820–6. mITT population.")
63
Paediatric subset of Phase III trial micafungin vs
Paediatric subset of Phase III trial micafungin vs. fluconazole: treatment success 80 Micafungin Fluconazole 70 69.2 60 50 53.3 Treatment success rate (%) 40 30 The Phase III trial of micafungin compared with fluconazole as prophylaxis against invasive fungal infections in adults also included a small number of paediatric patients, of whom 39 received micafungin and 45 received fluconazole.1 Micafungin was associated with a higher percentage of treatment success than fluconazole (69.2% versus 53.3%), although the difference did not reach statistical significance because of the small number of patients.1,2 van Burik JA, et al. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004; 39:1407–1416. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September 2008. 20 10 n = 39 45 Micafungin Fluconazole van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16
 The Phase III trial of micafungin compared with fluconazole as prophylaxis against invasive fungal infections in adults also included a small number of paediatric patients, of whom 39 received micafungin and 45 received fluconazole.1. Micafungin was associated with a higher percentage of treatment success than fluconazole (69.2% versus 53.3%), although the difference did not reach statistical significance because of the small number of patients.1,2. van Burik JA, et al. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004; 39:1407–1416. MYCAMINE® (micafungin sodium) for injection Summary of Product Characteristics. Astellas Pharma Europe Ltd., September n = Micafungin. Fluconazole. van Burik JA, et al. Clin Infect Dis 2004; 39:1407–16.")
64
Θεραπευτικές προσεγγίσεις μυκητιασικών λοιμώξεων

65
Θεραπευτικές προσεγγίσεις μυκητιασικών λοιμώξεων candida spp
Polyenes Amphotericin B, including lipid formulations Azoles Older agents: fluconazole, itraconazole Newer agents: voriconazole, posaconazole Echinocandins Micafungin Caspofungin Anidulafungin There are a number of different classes of antifungal agents available for the treatment of SCIs; these agents can be classified according to their mechanism of action: Polyenes – these agents were the first antifungals developed Azoles – this class includes fluconazole, itraconazole, voriconazole and posaconazole Echinocandins – this is the newest major class of antifungal agents and includes caspofungin, anidulafungin and micafungin.

66
Micafungin Antifungal agents indicated for first-line therapy of candidemia include: amphotericin B (AMB) deoxycholate, anidulafungin, fluconazole, caspofungin, and voriconazole1-5 Anidulafungin is indicated for the treatment of candidemia and other Candida infections (intra-abdominal abscess and peritonitis), based on a randomized double-blind trial versus fluconazole4 Caspofungin is indicated for the treatment of candidemia and other forms of Candida infections (intra-abdominal abscess and peritonitis) based on a double-blind, randomized trial versus amphotericin B deoxycholate5 Fluconazole’s indications for Candida urinary tract infections, peritonitis, and systemic Candida infections, including candidemia, disseminated candidiasis, and pneumonia, were approved on the basis of noncomparative, open studies in relatively small numbers of patients,3 before more robust data were available from large-scale, randomized, comparative studies in patients with candidemia Voriconazole is indicated for the treatment of candidemia in nonneutropenic patients, disseminated Candida infections in skin, and Candida infections in the abdomen, kidney, bladder wall, and wounds, based on an open-label randomized trial versus amphotericin B followed by fluconazole1 The salvage Candida indication for liposomal AMB (L-AMB) is based on a compassionate-use study of 133 patients with various systemic fungal infections who were refractory to, or intolerant of, AMB deoxycholate or had preexisting renal insufficiency.6 For AMB lipid complex (ABLC), the indication is based on pooled data from 3 open-label studies, which included 87 evaluable patients with invasive candidiasis who were judged by their physicians to be refractory to, or intolerant of, AMB deoxycholate, or who had preexisting nephrotoxicity7 Only voriconazole and fluconazole are available in both oral and IV formulations1,3 References: 1. VFEND [package insert]. New York, NY: Pfizer Inc; March 2006. 2. Fungizone Intravenous [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2001. 3. Diflucan [package insert]. New York, NY: Pfizer Inc; 2004. 4. Eraxis [package insert]. New York, NY: Pfizer Inc; March 2006. 5. Cancidas for Injection [package insert]. Whitehouse Station, NJ: Merck & Co, Inc; 2005. 6. AmBisome for Injection [package insert]. San Dimas, Calif: Gilead Sciences, Inc; 2005. 7. Abelcet Injection [package insert]. Piscataway, NJ: Enzon Pharmaceuticals; 2002. 66
 deoxycholate, anidulafungin, fluconazole, caspofungin, and voriconazole1-5. Anidulafungin is indicated for the treatment of candidemia and other Candida infections (intra-abdominal abscess and peritonitis), based on a randomized double-blind trial versus fluconazole4. Caspofungin is indicated for the treatment of candidemia and other forms of Candida infections (intra-abdominal abscess and peritonitis) based on a double-blind, randomized trial versus amphotericin B deoxycholate5. Fluconazole’s indications for Candida urinary tract infections, peritonitis, and systemic Candida infections, including candidemia, disseminated candidiasis, and pneumonia, were approved on the basis of noncomparative, open studies in relatively small numbers of patients,3 before more robust data were available from large-scale, randomized, comparative studies in patients with candidemia. Voriconazole is indicated for the treatment of candidemia in nonneutropenic patients, disseminated Candida infections in skin, and Candida infections in the abdomen, kidney, bladder wall, and wounds, based on an open-label randomized trial versus amphotericin B followed by fluconazole1. The salvage Candida indication for liposomal AMB (L-AMB) is based on a compassionate-use study of 133 patients with various systemic fungal infections who were refractory to, or intolerant of, AMB deoxycholate or had preexisting renal insufficiency.6 For AMB lipid complex (ABLC), the indication is based on pooled data from 3 open-label studies, which included 87 evaluable patients with invasive candidiasis who were judged by their physicians to be refractory to, or intolerant of, AMB deoxycholate, or who had preexisting nephrotoxicity7. Only voriconazole and fluconazole are available in both oral and IV formulations1,3. References: 1. VFEND [package insert]. New York, NY: Pfizer Inc; March Fungizone Intravenous [package insert]. Princeton, NJ: Bristol-Myers Squibb Company; Diflucan [package insert]. New York, NY: Pfizer Inc; Eraxis [package insert]. New York, NY: Pfizer Inc; March Cancidas for Injection [package insert]. Whitehouse Station, NJ: Merck & Co, Inc; AmBisome for Injection [package insert]. San Dimas, Calif: Gilead Sciences, Inc; Abelcet Injection [package insert]. Piscataway, NJ: Enzon Pharmaceuticals;")
67
Guidelines for the treatment of patients with SCIs: Europe 2007
Several groups within Europe have published individual recommendations for the treatment of SCIs, including FUNGINOS, DGHO, SAEI and ECIL1–6 Patient type First choice Alternatives Non-neutropenic Fluconazole (800 mg/d loading, then 400 mg/d)*1,2 Amphotericin B deoxycholate (AmB-d) or caspofungin†1 AmB-d or caspofungin or voriconazole*1,2 Liposomal amphotericin B (L‑AmB)†1 Neutropenic AmB-d1,2 Caspofungin or L-AmB1 Fluconazole or L-AmB2 Severe sepsis/ septic shock Caspofungin1,2 or AmB-d2 L-AmB1,2 or voriconazole1 Haemato-oncology Echinocandin or L-AmB or, if patient is non- neutropenic, voriconazole3 Fluconazole is reserved for patients who are stable, non-neutropenic, with no prior azole exposure and with a susceptible Candida species3 Caspofungin or L-AmB4 L-AmB or ABLC3 Several groups within Europe have published recommendations for the treatment of patients with SCIs, including: The Fungal Infection Network of Switzerland (FUNGINOS)1 The Andalusian Society of Infectious Diseases (SAEI)2 The Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO)3 The British Committee for Standards in Haematology at the British Society for Haematology4 The European Conference on Infections in Leukaemia (ECIL).5,6 These recommendations are summarised in the table. Flückiger U, et al. Treatment options of invasive fungal infections in adults. Swiss Med Wkly 2006; 136:447–463. Pachon J, et al. [Treatment of invasive fungal infections Andalusian Infectious Disease Society.]. Enferm Infecc Microbiol Clin 2006; 24:254–263. Böhme A, et al. Treatment of invasive fungal infections in cancer patients--recommendations of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol 2009; 88:97–110. Prentice AG, et al. British Committee for Standards in Haematology. Guidelines on the management of invasive fungal infection during therapy for haematological malignancy. London; British Society for Haematology, 2008. Marchetti O, et al. Empirical antifungal therapy in neutropaenic cancer patients with persistent fever. Eur Journal of Cancer Suppl 2007; 5:32–42. Herbrecht R, et al. Treatment of invasive Candida and invasive Aspergillus infections in adult haematological patients. Eur J of Cancer Suppl 2007; 5:49–59. *No prior azole exposure; †Prior azole exposure; ABLC = amphotericin B lipid complex 1. Fluckiger U. Swiss Med Wkly 2006; 136:447–63; 2. Pachon J, et al. Enferm Infecc Microbiol Clin 2006; 24:254–63; 3. Böhme A, et al. Ann Hematol 2009; 88:97–110; 4. Prentice AG, et al. British Committee for Standards in Haematology. London; British Society for Haematology; 5. Marchetti O, et al. Eur J Cancer Suppl 2007; 5:32–42; 6. Herbrecht R, et al. Eur J Cancer Suppl 2007; 5:49–59 67
*1,2. Amphotericin B deoxycholate (AmB-d) or caspofungin†1. AmB-d or caspofungin or voriconazole*1,2. Liposomal amphotericin B (L‑AmB)†1. Neutropenic. AmB-d1,2. Caspofungin or L-AmB1. Fluconazole or L-AmB2. Severe sepsis/ septic shock. Caspofungin1,2 or AmB-d2. L-AmB1,2 or voriconazole1. Haemato-oncology. Echinocandin or L-AmB or, if patient is non- neutropenic, voriconazole3. Fluconazole is reserved for patients who are stable, non-neutropenic, with no prior azole exposure and with a susceptible Candida species3. Caspofungin or L-AmB4. L-AmB or ABLC3. Several groups within Europe have published recommendations for the treatment of patients with SCIs, including: The Fungal Infection Network of Switzerland (FUNGINOS)1. The Andalusian Society of Infectious Diseases (SAEI)2. The Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO)3. The British Committee for Standards in Haematology at the British Society for Haematology4. The European Conference on Infections in Leukaemia (ECIL).5,6. These recommendations are summarised in the table. Flückiger U, et al. Treatment options of invasive fungal infections in adults. Swiss Med Wkly 2006; 136:447–463. Pachon J, et al. [Treatment of invasive fungal infections Andalusian Infectious Disease Society.]. Enferm Infecc Microbiol Clin 2006; 24:254–263. Böhme A, et al. Treatment of invasive fungal infections in cancer patients--recommendations of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol 2009; 88:97–110. Prentice AG, et al. British Committee for Standards in Haematology. Guidelines on the management of invasive fungal infection during therapy for haematological malignancy. London; British Society for Haematology, Marchetti O, et al. Empirical antifungal therapy in neutropaenic cancer patients with persistent fever. Eur Journal of Cancer Suppl 2007; 5:32–42. Herbrecht R, et al. Treatment of invasive Candida and invasive Aspergillus infections in adult haematological patients. Eur J of Cancer Suppl 2007; 5:49–59. *No prior azole exposure; †Prior azole exposure; ABLC = amphotericin B lipid complex. 1. Fluckiger U. Swiss Med Wkly 2006; 136:447–63; 2. Pachon J, et al. Enferm Infecc Microbiol Clin 2006; 24:254–63; 3. Böhme A, et al. Ann Hematol 2009; 88:97–110; 4. Prentice AG, et al. British Committee for Standards in Haematology. London; British Society for Haematology; 5. Marchetti O, et al. Eur J Cancer Suppl 2007; 5:32–42; 6. Herbrecht R, et al. Eur J Cancer Suppl 2007; 5:49–")
68
Guidelines for the treatment of invasive candidiasis: IDSA
Condition or treatment group Therapy Primary Alternative Recommendation Rank* Non-neutropenic patients Candidaemia (targeted therapy) Fluconazole or an echinocandin† A-I Lipid formulation of AmB (LFAmB) or AmB-d or voriconazole Suspected candidiasis (empirical therapy‡) As for candidaemia; echinocandin or fluconazole preferred† B-III LFAmB or AmB-d Neutropenic patients Echinocandin or LFAmB A-II Fluconazole§ or voriconazole LFAmB or caspofungin or voriconazole A-I (B-I for voriconazole) Fluconazole¶ or itraconazole¶ B-I In the absence of pan-European guidelines, the treatment guidelines produced by the Infectious Diseases Society of America (IDSA) are held in high regard. The most recent version of these guidelines was published in February 2009; the key recommendations are summarised in the table.1 Pappas PG, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis 2009; 48:503–535. *See following slide for definitions. †An echinocandin is favoured for moderately severe to severe illness and in patients with recent azole exposure, and as initial therapy in patients with or suspected to have C. glabrata infection; fluconazole is preferred as initial therapy in patients with or suspected to have C. parapsilosis infection, if no prior azole exposure. ‡Empirical therapy should be initiated following ≥ 4 days’ fever despite antibiotics. §Fluconazole should be reserved for patients without prior azole exposure who are not critically ill. ¶Azoles should not be used for empirical therapy in patients who have received an azole for prophylaxis Pappas PG, et al. Clin Infect Dis 2009; 48:503–35
 Fluconazole or an echinocandin† A-I. Lipid formulation of AmB (LFAmB) or AmB-d or voriconazole. Suspected candidiasis (empirical therapy‡) As for candidaemia; echinocandin or fluconazole preferred† B-III. LFAmB or AmB-d. Neutropenic patients. Echinocandin or LFAmB. A-II. Fluconazole§ or voriconazole. LFAmB or caspofungin or voriconazole. A-I (B-I for voriconazole) Fluconazole¶ or itraconazole¶ B-I. In the absence of pan-European guidelines, the treatment guidelines produced by the Infectious Diseases Society of America (IDSA) are held in high regard. The most recent version of these guidelines was published in February 2009; the key recommendations are summarised in the table.1. Pappas PG, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis 2009; 48:503–535. *See following slide for definitions. †An echinocandin is favoured for moderately severe to severe illness and in patients with recent azole exposure, and as initial therapy in patients with or suspected to have C. glabrata infection; fluconazole is preferred as initial therapy in patients with or suspected to have C. parapsilosis infection, if no prior azole exposure. ‡Empirical therapy should be initiated following ≥ 4 days’ fever despite antibiotics. §Fluconazole should be reserved for patients without prior azole exposure who are not critically ill. ¶Azoles should not be used for empirical therapy in patients who have received an azole for prophylaxis. Pappas PG, et al. Clin Infect Dis 2009; 48:503–35.")
69
ΠΡΟΦΥΛΑΞΗ ΜΥΚΗΤΙΑΣΕΩΝ ΠΟΥ ΚΑΙ ΠΟΤΕ

70
ΓΙΑΤΙ; ΔΙΟΤΙ : Υπάρχουν καλά καθορισμένοι πληθυσμοί ασθενών που διατρέχουν ψηλό κίνδυνο να παρουσιάσουν Διηθητικές Μυκητιασικές Λοιμώξεις (ΔΜΛ) ΠΟΙΕΣ ΛΟΙΜΩΞΕΙΣ; 1. Από ζυμομύκητες (Yeast infections) ΚΑΙ κυρίως από Candida spp (Candida albicans αποτελεί κύριο εκπρόσωπο) 2. Σε δεύτερο χρόνο, από υφομύκητες (Mould infections) ΚΑΙ κυρίως από Aspergillus spp
 ΚΑΙ κυρίως από Candida spp (Candida albicans αποτελεί κύριο εκπρόσωπο) 2. Σε δεύτερο χρόνο, από υφομύκητες (Mould infections) ΚΑΙ κυρίως από Aspergillus spp.")
71
ΠΛΗΘΥΣΜΟΙ: Α. ΧΑΜΗΛΟΥ ΚΙΝΔΥΝΟΥ Β. ΥΨΗΛΟΥ ΚΙΝΔΥΝΟΥ

72
Πληθυσμοί χαμηλού κινδύνου:
Ασθενείς με λέμφωμα που λαμβάνουν ‘standard’ χημειοθεραπεία Ασθενείς που υπόκεινται σε αυτόλογη μεταμόσχευση αρχέγονων κυττάρων μετά από χημειοθεραπεία υψηλών δόσεων ΚΑΙ ΔΕΝ έχουν λάβει πρόσφατα πουρινικά ανάλογα που καταστέλλουν τα Τ κύτταρα Ασθενείς που υπόκεινται σε μεταμόσχευση παγκρέατος (χωρίς χαρακτηριστικά υψηλού κινδύνου) Ασθενείς που υπόκεινται σε μεταμόσχευση ήπατος και ΔΕΝ χαρακτηρίζονται ως υψηλού κινδύνου Ασθενείς που υπόκεινται σε μεταμόσχευση νεφρού ή καρδίας (θεωρούνται ΠΟΛΥ Χαμηλού κινδύνου)
 Ασθενείς που υπόκεινται σε μεταμόσχευση ήπατος και ΔΕΝ χαρακτηρίζονται ως υψηλού κινδύνου. Ασθενείς που υπόκεινται σε μεταμόσχευση νεφρού ή καρδίας (θεωρούνται ΠΟΛΥ Χαμηλού κινδύνου)")
73
Πληθυσμοί υψηλού κινδύνου
Ουδετεροπενία επι κακοήθων αιματολογικών νόσων (Neutropenia in malignant haematological diseases) Δέκτες αλλογενούς μεταμόσχευσης αρχέγονων κυττάρων (Allogenic stem cell transplant recipients) Δέκτες συμπαγών οργάνων μετά μεταμόσχευση (Solid organ transplant recipients) Ορισμένοι ασθενείς σε ΜΕΘ (Intensive care patients) Ασθενείς με AIDS και CD4 <50 κύτ/μl ??????
 Δέκτες αλλογενούς μεταμόσχευσης αρχέγονων κυττάρων (Allogenic stem cell transplant recipients) Δέκτες συμπαγών οργάνων μετά μεταμόσχευση (Solid organ transplant recipients) Ορισμένοι ασθενείς σε ΜΕΘ (Intensive care patients) Ασθενείς με AIDS και CD4 <50 κύτ/μl")
85
ευχαριστώ

Παρόμοιες παρουσιάσεις

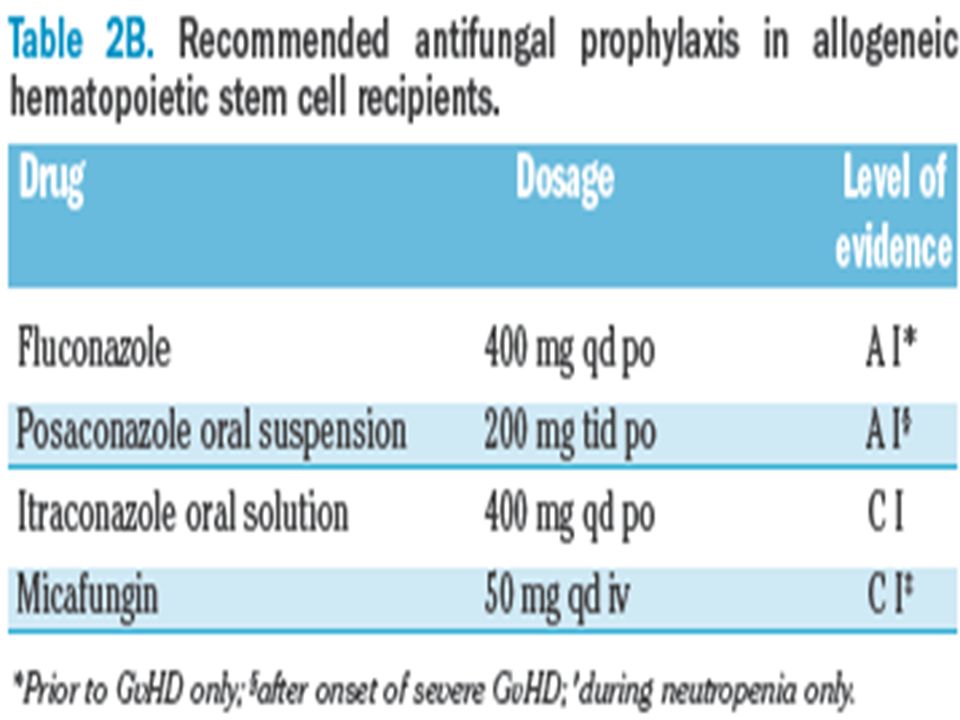
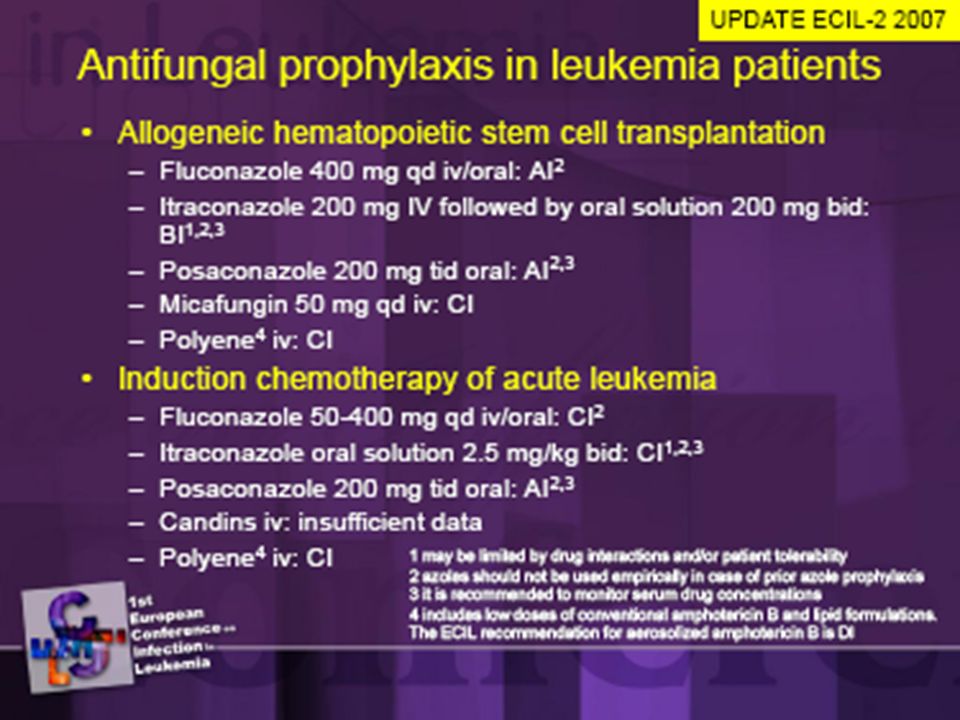
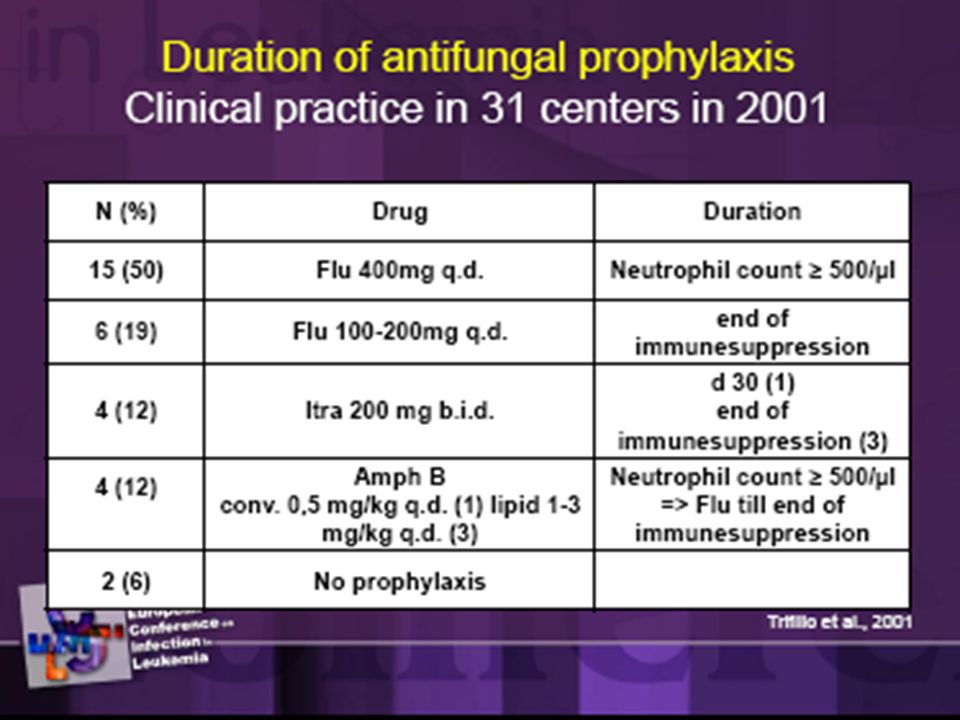












>")












 ωφελέειν ή μη βλάπτειν ωφελέειν = θεραπευτική παρέμβαση μη βλάπτειν = ασφάλεια ασθενών.>")




