Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Λέκτορας Πνευμονολογίας
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ Παρασκευή Κατσαούνου Λέκτορας Πνευμονολογίας Ιατρική Σχολή Αθηνών ΓΝ ΕΥΑΓΓΕΛΙΣΜΟΣ

2
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ Environmental tobacco smoke (ETS)
“second-hand smoke” “involuntary smoking” The smoke inhaled by the smoker first, and then exhaled, is called mainstream smoke. The smoke that goes directly into the air from the end of a burning cigarette is called sidestream smoke. ETS is composed of side-stream smoke from smouldering cigarettes and from mainstream smoke exhaled by smokers.

3
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ- ΕΤS
Αποτελεί σημαντικό και απόλυτα αναγνωρισμένο ρύπο των εσωτερικών χώρων. 4.000 χημικά 100 τοξικά 50 καρκινογόνα Η έκθεση ενός μη καπνιστή που συμβιώνει με καπνιστή είναι ισοδύναμη περίπου με το 1% της έκθεσης ενεργητικού καπνιστή 20 τσιγάρων την ημέρα.

4
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ- ΝΟΥΜΕΡΑ
Tο 2004 εκτέθηκαν σε παθητικό κάπνισμα: 40% των παιδιών. 33% των μη καπνιστών αντρών. 35% των μη καπνιστών γυναικών.

5
ΕΚΘΕΣΗ ΣΕ ETS ΣΤΗ ΔΟΥΛΕΙΑ

6
ΕΚΘΕΣΗ ΣΕ ETS ΣΤΗ ΔΟΥΛΕΙΑ
17% στην Ευρωπαϊκή ένωση 60% στην Ελλάδα 47% στη Βουλγαρία 41% στη Λιθουανία, Κύπρο <10% στην Αγγλία, Γαλλία, Σουηδία Συχνότερα σε: -άντρες -χαμηλή εκπαίδευση - εργάτες - ηλικία άνω των 54 - αυτοαπασχολούμενοι

7
ΕΚΘΕΣΗ ΣΕ ETS ΣΤΟ ΣΠΙΤΙ

8
ΕΚΘΕΣΗ ΣΕ ETS ΣΤΟ ΣΠΙΤΙ

9
ΕΚΘΕΣΗ ΣΕ ETS ΣΤΟ ΣΠΙΤΙ

10
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΑΙΔΙΑ
Λοιμώξεις κατώτερου αναπνευστικού (LRI) Συχνές σε παιδιά 0-2 ετών βρογχίτις, βρογχιολίτις, πνευμονία Συχνές εισαγωγές στο νοσοκομείο για LRI
 Συχνές σε παιδιά 0-2 ετών. βρογχίτις, βρογχιολίτις, πνευμονία. Συχνές εισαγωγές στο νοσοκομείο για LRI.")
11
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΑΙΔΙΑ

13
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΑΙΔΙΑ
Συμπτώματα Συριγμός Βήχας Απόχρεμψη Δύσπνοια ⇑ ΒΗR Aτοπία

14
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΑΙΔΙΑ
ΝΟΣΟΙ ΜΕΣΟΥ ΩΤΟΣ Οξεία μέση ωτίτιδα Υποτροπιάζουσα μέση ωτίτιδα Συλλογές μέσου ωτός

15
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΑΙΔΙΑ ΣΥΝΔΟΜΟ ΑΙΦΝΙΔΙΟΥ ΘΑΝΑΤΟΥ ΒΡΕΦΩΝ-
SUDDEN INFANT DEATH SYNDROME Kατά τη διάρκεια της κύησης και μετά. Χαλαρότερη πρόσφυση των κυψελίδων στους αεραγωγούς, με αποτέλεσμα περισσότερο ευένδοτους αεραγωγούς, ιδιαίτερα μετά από έκθεση σε ερεθίσματα που προκαλούν ελάττωση της διαμέτρου τους. Περισσότερα απνοϊκά επισόδεια κυρίως αποφρακτικού τύπου και πιθανώς υψηλότερο ουδό αφύπνισης μετά τα απνοίκά επισόδεια.

16
ΑΣΘΜΑ ΠΑΙΔΙΚΗΣ ΗΛΙΚΙΑΣ ΚΑΙ ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ
Πρόκληση βρογχικού άσθματος; Επιδείνωση της σοβαρότητας και της πρόγνωσης του βρογχικού άσθματος Περισσότερα συμπτώματα και παροξύνσεις. Πιο σοβαροί παροξυσμοί που μπορεί να οδηγήσουν και σε θάνατο

17
ΚΥΗΣΗ ΚΑΙ ΚΑΠΝΙΣΜΑ Η νικοτίνη επιδρά αρνητικά στην κυκλοφορία πλακούντα-μήτρας ⇓ διαφοροποίηση εμβρυïκής καρδιακής συχνότητας ⇑ αντίσταση ομφάλιας αρτηρίας Το κάπνισμα σχετίζεται με: ⇓ διαστάσεις αγγείων πλακούντα ⇑ αυτόματες αποβολές ⇓ ενδομήτρια ανάπτυξη ⇑ κίνδυνος έκτοπης κύησης (δοσοεξαρτώμενος) ⇑ κίνδυνο αποκόλλησης πλακούντα Καθυστερημένη ενδομήτρια ανάπτυξη Αυτόματη αποβολή 1ου τριμήνου Εμβρυïκή θνησιμότητα Πρώϊμη ρήξη υμένων Πρώïμος τοκετός Πρόδρομος πλακούντας ⇑ht εμβρύου Παιδικό άσθμα Διαταραχές ανάπτυξης ΚΝΣ Women who smoke have a higher rate of placenta previa, abruptio placenta, preterm delivery, ectopic pregnancy and PPROM. Smoking also contributes to higher infant mortality, low birth weight, and intrauterine growth restriction. The fetal complications associated with smoking include reduced placental capillary dimensions, increased risk of fetal death and preterm birth, and increased fetal hematocrit. Smoking during pregnancy has also been correlated to an increased risk of childhood asthma.
 ⇑ κίνδυνο αποκόλλησης πλακούντα. Καθυστερημένη ενδομήτρια ανάπτυξη. Αυτόματη αποβολή 1ου τριμήνου. Εμβρυïκή θνησιμότητα. Πρώϊμη ρήξη υμένων. Πρώïμος τοκετός. Πρόδρομος πλακούντας. ⇑ht εμβρύου. Παιδικό άσθμα. Διαταραχές ανάπτυξης ΚΝΣ. Women who smoke have a higher rate of placenta previa, abruptio placenta, preterm delivery, ectopic pregnancy and PPROM. Smoking also contributes to higher infant mortality, low birth weight, and intrauterine growth restriction. The fetal complications associated with smoking include reduced placental capillary dimensions, increased risk of fetal death and preterm birth, and increased fetal hematocrit. Smoking during pregnancy has also been correlated to an increased risk of childhood asthma.")
18
ENΔΟΜΗΤΡΙΑ ΕΚΘΕΣΗ ΣΕ ΚΑΠΝΟ ΤΣΙΓΑΡΟΥ
Μητρικό κάπνισμα σχετίζεται με αυξημένο oξειδωτικό stress στο 3 μηνών νεογνό (Noakes P. et al, Τhorax 2007). Eνδομήτρια έκθεση σε καπνό επιτείνει την αλλεργική απόκριση σε αλλεργιογόνα σε ποντίκια (Penn A. et al, Env Heal Perc 2007). Μητρικό κάπνισμα (κατά την κύηση και στη συνέχεια) σχετίζεται με wheezing {OR:1.24 [ ]} και άσθμα {OR:1.22 [ ]}(Raherison C et al, Resp Med 2006). Guilliand FD, AJRCCM 2003
. Eνδομήτρια έκθεση σε καπνό επιτείνει την αλλεργική απόκριση σε αλλεργιογόνα σε ποντίκια (Penn A. et al, Env Heal Perc 2007). Μητρικό κάπνισμα (κατά την κύηση και στη συνέχεια) σχετίζεται με wheezing {OR:1.24 [ ]} και άσθμα {OR:1.22 [ ]}(Raherison C et al, Resp Med 2006). Guilliand FD, AJRCCM")
19
ΚΑΠΝΙΣΜΑ ΣΤΗΝ ΚΥΗΣΗ ΚΑΙ ΑΣΘΜΑ ΣΤΗΝ ΠΑΙΔΙΚΗ ΗΛΙΚΙΑ
Το κάπνισμα κατά την εμβρυική ηλικία σχετίζεται με υψηλότερη επίπτωση άσθματος στα παιδιά. Ανάλυση 60 μελετών ανέδειξε ότι ο κίνδυνος εμφάνισης άσθματος στην παιδική ηλικία είναι αυξημένος όταν οι γονείς καπνίζουν. Odds Ratio (OR)a=1.21 (95% CI, ). Το κάπνισμα της μητέρας είχε μεγαλύτερη επίπτωση από το κάπνισμα του πατέρα στα παιδιά. Key Point The risk of asthma in school-aged children is increased if either parent smokes. Cook and Strachan performed a meta-analysis on 60 studies to assess the effects of parental smoking on the prevalence of asthma and respiratory symptoms in school-age children. The authors determined that the pooled OR for either parent smoking was 1.21 (95% CI, ) for asthma, 1.24 (95% CI, ) for wheezing, and 1.4 (95% CI, ) for chronic cough. Cook et al also found that although maternal smoking had a greater effect than paternal smoking, the effect of paternal smoking alone was also important, suggesting that the postnatal effect is significant as well. aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Cook et al. Thorax. 1997;52(12): ; Reference Cook DG, Strachan DP. Health effects of passive smoking, 3: parental smoking and prevalence of respiratory symptoms and asthma in school age children. Thorax. 1997;52(12):
a=1.21 (95% CI, ). Το κάπνισμα της μητέρας είχε μεγαλύτερη επίπτωση από το κάπνισμα του πατέρα στα παιδιά. Key Point. The risk of asthma in school-aged children is increased if either parent smokes. Cook and Strachan performed a meta-analysis on 60 studies to assess the effects of parental smoking on the prevalence of asthma and respiratory symptoms in school-age children. The authors determined that the pooled OR for either parent smoking was 1.21 (95% CI, ) for asthma, 1.24 (95% CI, ) for wheezing, and 1.4 (95% CI, ) for chronic cough. Cook et al also found that although maternal smoking had a greater effect than paternal smoking, the effect of paternal smoking alone was also important, suggesting that the postnatal effect is significant as well. aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Cook et al. Thorax. 1997;52(12): ; Reference. Cook DG, Strachan DP. Health effects of passive smoking, 3: parental smoking and prevalence of respiratory symptoms and asthma in school age children. Thorax. 1997;52(12):")
20
ΚΑΠΝΙΣΜΑ ΣΤΗΝ ΚΥΗΣΗ ΚΑΙ ΑΣΘΜΑ ΣΤΗΝ ΠΑΙΔΙΚΗ ΗΛΙΚΙΑ
Η έκθεση σε καπνό τσιγάρου πριν και μετά τη γέννηση σχετίζεται με αυξημένο κίνδυνο άσθματος. ΧΩΡΙΣ ΕΚΘΕΣΗ ΣΕ ΚΑΠΝΟ ΕΚΘΕΣΗ ΣΕ ΚΑΠΝΟ ΛΟΓΩ ΜΗΤΕΡΑΣ Odds Ratio (95% CI)a Key Point Exposure to pre- and postnatal smoking carries a substantial risk for developing adult asthma. Skorge et al evaluated the effects of pre- or postnatal passive smoking on the adult incidence of asthma and respiratory symptoms. An 11-year community cohort study was conducted between 1985 and 1996/1997 in western Norway. The final cohort included 2819 subjects (those who responded to both surveys) aged 15 to 70 years who responded to a mailed questionnaire that consisted of 40 questions about respiratory health, allergies, smoking habits, and occupational exposure. The follow-up survey was conducted between September 1996 and May The questionnaire was expanded to 58 questions and included questions on education and exposure to passive smoking. At follow-up the subjects also were asked the following 3 questions about their parents’ smoking habits: Did your mother smoke when she was pregnant with you? Did your mother smoke when you were a child? Did others in the household smoke when you were a child? Participants reporting smoking exposure in utero had a significantly higher risk for the adult incidence of asthma, even after extensive adjustment for confounders. A similar but weaker trend was seen with exposure to maternal smoking in childhood. With the combined variable, it is apparent that the association between maternal smoking and adult incidence of asthma and respiratory symptoms is strongest with prenatal exposure. ΠΡΙΝ ΤΗ ΓΕΝΝΗΣΗ ΜΕΤΑ ΤΗ ΓΕΝΝΗΣΗ ΠΡΙΝ ΚΑΙ ΜΕΤΑ ΤΗ ΓΕΝΝΗΣΗ Adjusted for sex, age, educational level, active smoking in terms of both smoking habits and pack/years, occupational exposure, and hay fever. In addition, when estimating the ORs for the 3 maternal smoking variables, adjustment was made for exposure to smoking from other household members. Skorge et al. Am J Resp Crit Care Med. 2005;172(1):61-66. Reference Skorge TD, Eagan TML, Eide GE, Gulsvik A, Bakke PS. The adult incidence of asthma and respiratory symptoms by passive smoking in utero or in childhood. Am J Respir Crit Care Med. 2005;172(1):61-66.
a. Key Point. Exposure to pre- and postnatal smoking carries a substantial risk for developing adult asthma. Skorge et al evaluated the effects of pre- or postnatal passive smoking on the adult incidence of asthma and respiratory symptoms. An 11-year community cohort study was conducted between 1985 and 1996/1997 in western Norway. The final cohort included 2819 subjects (those who responded to both surveys) aged 15 to 70 years who responded to a mailed questionnaire that consisted of 40 questions about respiratory health, allergies, smoking habits, and occupational exposure. The follow-up survey was conducted between September 1996 and May The questionnaire was expanded to 58 questions and included questions on education and exposure to passive smoking. At follow-up the subjects also were asked the following 3 questions about their parents’ smoking habits: Did your mother smoke when she was pregnant with you Did your mother smoke when you were a child Did others in the household smoke when you were a child Participants reporting smoking exposure in utero had a significantly higher risk for the adult incidence of asthma, even after extensive adjustment for confounders. A similar but weaker trend was seen with exposure to maternal smoking in childhood. With the combined variable, it is apparent that the association between maternal smoking and adult incidence of asthma and respiratory symptoms is strongest with prenatal exposure. ΠΡΙΝ ΤΗ ΓΕΝΝΗΣΗ. ΜΕΤΑ ΤΗ ΓΕΝΝΗΣΗ. ΠΡΙΝ ΚΑΙ ΜΕΤΑ ΤΗ ΓΕΝΝΗΣΗ. Adjusted for sex, age, educational level, active smoking in terms of both smoking habits and pack/years, occupational exposure, and hay fever. In addition, when estimating the ORs for the 3 maternal smoking variables, adjustment was made for exposure to smoking from other household members. Skorge et al. Am J Resp Crit Care Med. 2005;172(1): Reference. Skorge TD, Eagan TML, Eide GE, Gulsvik A, Bakke PS. The adult incidence of asthma and respiratory symptoms by passive smoking in utero or in childhood. Am J Respir Crit Care Med. 2005;172(1):")
21
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΑΙΔΙΑ
Μικρή αλλά στατιστικά σημαντική επίδραση στην ανάπτυξη του πνεύμονα, όπως αυτή εκφράζεται από τους σπιρομετρικούς δείκτες FEV1, FVC, MEFR. Μηχανισμοί: ΟΞΕΩΣ Ερεθισμός υποδοχέων Οίδημα βλεννογόνου ⇓βλεννοκρωσσωτή κάθαρση υπερτροφία καλυκοειδών κυττάρων Υπερέκκριση βλέννας Υπερπλασία αδενοειδών εκβλαστήσεων Φλεγμονή βρογχικού βλεννογόνου Επιβράδυνση της ανάπτυξης του πνεύμονα κατά τη γέννηση ΧΡΟΝΙΩΣ - Επιβράδυνση εμβρυϊκής ανάπτυξης

22
ΣΥΝΔΡΟΜΟ ΑΙΦΝΙΔΙΟΥ ΘΑΝΑΤΟΥ ΤΩΝ ΒΡΕΦΩΝ- SUDDEN INFANT DEATH SYNDROME
Δοσοεξαρτώμενη συσχέτιση μεταξύ καπνίσματος της μητέρας και βεφικού θανάτου, τόσο κατά τη διάρκεια της κύησης, όσο και μετά τον τοκετό. και μόνο μετά τον τοκετό ⇑⇑ κίνδυνο για SIDS. το κάπνισμα μόνο του πατέρα ⇑κίνδυνο για SIDS.

23
ΚΑΠΝΙΣΜΑ ΚΑΙ ΚΥΗΣΗ Η νικοτίνη είναι λιποδιαλυτή και διαχέεται εύκολα μέσω των βιολογικών μεμβρανών. Κατά τη διάρκεια της κύησης μεταφέρεται μέσω του πλακούντα και εναποτίθεται στους εμβυϊκούς ιστούς. Οι επιπτώσεις της νικοτίνης στην κύηση οφείλονται κυρίως στα παρακάτω: - αγγειοδιασταλτικές ιδιότητές της νικοτίνης - ⇑ επίπεδα κατεχολαμινών και καρβοξυαιμο-σφαιρίνης εμβρύου. - ⇑ καρδιακή συχνότητα και αρτηριακή πίεση

24
ΕΠΙΠΕΔΑ ΚΟΤΙΝΙΝΗΣ ΣΤΑ ΑΜΝΙΑΚΑ ΥΓΡΑ
Η έκθεση στη νικοτίνη μπορεί να μετρηθεί έμμεσα με τη μέτρηση της κοτινίνης. Η κοτινίνη είναι καλύτερος δείκτης έκθεσης στον καπνό απ’ ότι η νικοτίνη. Η κοτινίνη εναποτίθεται ήδη από την 7η εβδομάδα στην κυκλοφο-ρία του εμβρύου. Υπάρχει γραμμική συνάρτηση μεταξύ των επιπέδων κοτινίνης της μητέρας και του εμβρύου. Key Point Cotinine, the main metabolite of nicotine, accumulates in fetal compartments early in gestation in women with measurable cotinine concentrations in their serum. Cotinine is the main metabolite of nicotine. It is a better indicator of tobacco use because of its longer half-life, and can be found in maternal serum, urine, and saliva. Jauniaux et al measured maternal cotinine concentrations in women presenting for termination in their first or second trimesters. These included 26 smokers, 19 women chronically exposed to environmental tobacco smoke, and 40 nonsmokers. Coelomic (n=23) and amniotic fluid (n=25) cotinine concentrations were obtained at 7 to 11 weeks’ gestation, and if the procedure was being done between 11 and 17 weeks, amniotic fluid (n=58) and fetal serum (n=46) concentrations were measured. The correlation between concentrations in different compartments and number of cigarettes per day was calculated using the least squares method and the F ratio test. In women exposed to environmental tobacco smoke, mean cotinine levels were higher in fetal than maternal serum. There was a positive linear correlation between maternal and fetal serum cotinine concentrations in active smokers (r=0.97; SEM=39; F=59, n=25; P<.001). This study demonstrates that cotinine accumulates in the early fetal circulation and fluids in measurable concentrations. Jauniaux et al. Obstet Gynecol. 1999;93(1):25-29; Reference Jauniaux E, Gulbis B, Acharya G, Thiry P, Rodeck C. Maternal tobacco exposure and cotinine levels in fetal fluids in the first half of pregnancy. Obstet Gynecol. 1999;93(1):25-29.
 and amniotic fluid (n=25) cotinine concentrations were obtained at 7 to 11 weeks’ gestation, and if the procedure was being done between 11 and 17 weeks, amniotic fluid (n=58) and fetal serum (n=46) concentrations were measured. The correlation between concentrations in different compartments and number of cigarettes per day was calculated using the least squares method and the F ratio test. In women exposed to environmental tobacco smoke, mean cotinine levels were higher in fetal than maternal serum. There was a positive linear correlation between maternal and fetal serum cotinine concentrations in active smokers (r=0.97; SEM=39; F=59, n=25; P<.001). This study demonstrates that cotinine accumulates in the early fetal circulation and fluids in measurable concentrations. Jauniaux et al. Obstet Gynecol. 1999;93(1):25-29; Reference. Jauniaux E, Gulbis B, Acharya G, Thiry P, Rodeck C. Maternal tobacco exposure and cotinine levels in fetal fluids in the first half of pregnancy. Obstet Gynecol. 1999;93(1):")
25
Η ΕΠΙΔΡΑΣΗ ΤΗΣ ΝΙΚΟΤΙΝΗΣ ΣΤΗΝ ΕΜΒΡΥΙΚΗ ΚΥΚΛΟΦΟΡΙΑ
⇓ αιματική ροή πλακούντα-μήτρας. ⇑αντίσταση στην αιματική ροή μέσης εγκεφαλικής. ⇓ διαφοροποίηση εμβρυïκής καρδιακής συχνότητας (ΝST) Key Point Maternal cigarette smoking has a significant impact on both maternal-fetal and fetal hemodynamics Effects of maternal tobacco smoking on fetal outcome are potentially mediated by restricted blood flow in the vascular beds of the placenta and the fetus. Acute repeated smoking reduces fetal heart rate reactivity, and increases umbilical, uterine, and fetal middle cerebral arterial resistance to blood flow. Εμβρυϊκή κυκλοφορία (Directional Color Doppler) Oncken et al. Obstet Gynecol 2002;99: Albuquerque et al. Early Hum Dev. 2004;80:31-42. References Albuquerque CA, Smith KR, Johnson C, Chao R, Harding R. Influence of maternal tobacco smoking during pregnancy on uterine, umbilical and fetal cerebral artery blood flows. Early Hum Dev. 2004;80:31-42. Oncken C, Kranzler H, O’Malley P, et al. The effect of cigarette smoking on fetal heart rate characteristics. Obstet Gynecol. 2002;99:
 Key Point. Maternal cigarette smoking has a significant impact on both maternal-fetal and fetal hemodynamics. Effects of maternal tobacco smoking on fetal outcome are potentially mediated by restricted blood flow in the vascular beds of the placenta and the fetus. Acute repeated smoking reduces fetal heart rate reactivity, and increases umbilical, uterine, and fetal middle cerebral arterial resistance to blood flow. Εμβρυϊκή κυκλοφορία. (Directional Color Doppler) Oncken et al. Obstet Gynecol 2002;99: Albuquerque et al. Early Hum Dev. 2004;80: References. Albuquerque CA, Smith KR, Johnson C, Chao R, Harding R. Influence of maternal tobacco smoking during pregnancy on uterine, umbilical and fetal cerebral artery blood flows. Early Hum Dev. 2004;80: Oncken C, Kranzler H, O’Malley P, et al. The effect of cigarette smoking on fetal heart rate characteristics. Obstet Gynecol. 2002;99:")
26
Η ΕΠΙΔΡΑΣΗ ΤΟΥ ΚΑΠΝΙΣΜΑΤΟΣ ΣΤΗΝ ΚΥΚΛΟΦΟΡΙΑ ΤΟΥ ΠΛΑΚΟΥΝΤΑ
ΥΠΑΡΞΗ ΔΙΑΣΤΟΛΙΚΟΥ ΗΧΟΥ ΑΡΤΗΡΙΑΣ ΜΗΤΡΑΣ Notch P<.05 Umbilical S/D (Median)a ΜΗ ΚΑΠΝΙΣΤΕΣ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Key Point Maternal smoking causes reduced blood-flow velocity in the maternal-fetal circulation resulting from increased vascular resistance. In a study of 143 women in their 34th to 35th week of pregnancy, 74 current smokers and 69 nonsmokers, Alburquerque et al measured blood-flow velocity of the uterine, umbilical, and fetal middle cerebral arteries (MCA) using Doppler analysis. The current smokers were also divided into heavy (at least 10 cigarettes/day) and light (less than 10 cigarettes/day) smokers. Mean S/D ratios (the ratio of time-averaged maximal systolic and diastolic blood flow velocities) were calculated from the mean of 3 successive Doppler waveforms. Data were expressed as mean and standard error of the mean (SEM). The Mann-Whitney U-test was used to analyze the difference between the groups, and the 2 test was used in the analysis of uterine artery notching. In the uterine artery, a diastolic notch was present in significantly more smokers than nonsmokers, 21 and 6, respectively (P<.05), suggestive of a greater resistance in uterine vasculature. The presence of a diastolic notch in the uterine artery flow profile has been interpreted as being due to an elevated diastolic resistance, and is consistent with smokers being found to have a poorer utero-placental perfusion In the umbilical artery, the current smokers had significantly greater S/D ratios (2.76 vs 2.40) than the nonsmokers (P<.05), suggestive of a greater resistance in umbilical vasculature. aS/D=systolic/diastolic ratio, the ratio of time-averaged maximal systolic and diastolic blood flow velocities. Albuquerque et al. Early Hum Dev. 2004;80:31-42. P<.05 Number of Patients ΜΗ ΚΑΠΝΙΣΤΕΣ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Reference Albuquerque CA, Smith KR, Johnson C, Chao R, Harding R. Influence of maternal tobacco smoking during pregnancy on uterine, umbilical and fetal cerebral artery blood flows. Early Hum Dev. 2004;80:31-42.
a. ΜΗ ΚΑΠΝΙΣΤΕΣ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Key Point. Maternal smoking causes reduced blood-flow velocity in the maternal-fetal circulation resulting from increased vascular resistance. In a study of 143 women in their 34th to 35th week of pregnancy, 74 current smokers and 69 nonsmokers, Alburquerque et al measured blood-flow velocity of the uterine, umbilical, and fetal middle cerebral arteries (MCA) using Doppler analysis. The current smokers were also divided into heavy (at least 10 cigarettes/day) and light (less than 10 cigarettes/day) smokers. Mean S/D ratios (the ratio of time-averaged maximal systolic and diastolic blood flow velocities) were calculated from the mean of 3 successive Doppler waveforms. Data were expressed as mean and standard error of the mean (SEM). The Mann-Whitney U-test was used to analyze the difference between the groups, and the 2 test was used in the analysis of uterine artery notching. In the uterine artery, a diastolic notch was present in significantly more smokers than nonsmokers, 21 and 6, respectively (P<.05), suggestive of a greater resistance in uterine vasculature. The presence of a diastolic notch in the uterine artery flow profile has been interpreted as being due to an elevated diastolic resistance, and is consistent with smokers being found to have a poorer utero-placental perfusion. In the umbilical artery, the current smokers had significantly greater S/D ratios (2.76 vs 2.40) than the nonsmokers (P<.05), suggestive of a greater resistance in umbilical vasculature. aS/D=systolic/diastolic ratio, the ratio of time-averaged maximal systolic and diastolic blood flow velocities. Albuquerque et al. Early Hum Dev. 2004;80: P<.05. Number of Patients. ΜΗ ΚΑΠΝΙΣΤΕΣ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Reference. Albuquerque CA, Smith KR, Johnson C, Chao R, Harding R. Influence of maternal tobacco smoking during pregnancy on uterine, umbilical and fetal cerebral artery blood flows. Early Hum Dev. 2004;80:")
27
ΠΕΡΙΓΕΝΝΗΤΙΚΕΣ ΕΠΙΠΛΟΚΕΣ ΣΧΕΤΙΖΟΜΕΝΕΣ ΜΕ ΤΗ ΧΡΗΣΗ ΚΑΠΝΟΥ
Αποκόλληση πλακούντα Καθυστερημένη ενδομήτρια ανάπτυξη Αυτόματη αποβολή 1ου τριμήνου Εμβρυïκή θνησιμότητα Πρωίμη ρήξη υμένων Πρώïμος τοκετός Πρόδρομος πλακούντας ⇑ht εμβρύου Παιδικό άσθμα Διαταραχές ανάπτυξης ΚΝΣ (εγκεφαλική λειτουργία, συμπεριφορά, γνώση) Although negative effects of smoking during pregnancy have been well publicized, 15% to 20% of women still continue to smoke while pregnant. Nicotine and its metabolites do enter the maternal-fetal unit, and smoking is associated with multiple significant perinatal complications. Andres et al. Semin Neonatol. 2000;5: ; Cnattingius. Nicotine Tob Res. 2004;6(suppl 2):S125-S140. References Andres RL, Day M-C. Perinatal complications associated with maternal tobacco use. Semin Neonatol. 2000;5: Cnattingius S. The epidemiology of smoking during pregnancy: smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob Res. 2004;6(suppl 2):S125-S140.
 Although negative effects of smoking during pregnancy have been well publicized, 15% to 20% of women still continue to smoke while pregnant. Nicotine and its metabolites do enter the maternal-fetal unit, and smoking is associated with multiple significant perinatal complications. Andres et al. Semin Neonatol. 2000;5: ; Cnattingius. Nicotine Tob Res. 2004;6(suppl 2):S125-S140. References. Andres RL, Day M-C. Perinatal complications associated with maternal tobacco use. Semin Neonatol. 2000;5: Cnattingius S. The epidemiology of smoking during pregnancy: smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob Res. 2004;6(suppl 2):S125-S140.")
28
ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ Πρώιμη αποκόλληση φυσιολογικά εμφυτεμένου πλακούντα πριν τον τοκετό. 0.8%-1.0% των κυήσεων. Δυνητικά επαπειλεί την ζωή εμβρύου-μητέρας. Μπορεί να οδηγήσει σε πρώιμο τοκετό, με βραχυ και μακροχρόνιες συνέπειες. Abruption FH Bl Placental abruption is defined as the premature separation of a normally implanted placenta before delivery. It occurs in 0.8% to 1.0% of all pregnancies. Placental abruption can cause preterm labor, fetal and maternal hemorrhage, and fetal death. FB FB=fetal body; Bl=bladder; FH=fetal head; Health Education Assets Library. Accessed October 19, 2007; Cunningham et al. In: Williams Obstetrics. 19th ed. 1993: ; Ananth et al. Obstet Gynecol. 1999;93: References Ananth CV, Smulian JC, Vintzileos AM. Incidence of placental abruption in relation to cigarette smoking and hypertensive disorders during pregnancy: a meta-analysis of observational studies. Obstet Gynecol. 1999;93: Cunningham FC, MacDonald PC, Gant NF, Leveno KJ, Gilstep LC. Obstetrical hemorrhage. In: Williams Obstetrics. 19th ed. Norwalk, CT: Appleton & Lange; 1993:

29
ΚΑΠΝΙΣΜΑ ΚΑΙ ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ
Οι καπνίστριες έχουν διπλάσιο κίνδυνο για αποκόλληση πλακούντα Σχετικός κίνδυνος OR Key Point Smokers have a 2-fold risk of placental abruption compared with nonsmokers. Ananth et al conducted a prospective study in 26 hospitals in Nova Scotia, Canada, between 1986 and 1993 to investigate the possibility that smoking increases the risk of placental abruption. A total of 81,826 pregnancies were analyzed, of which 26,325 (33%) were in women who smoked. Adjusted relative risk (RR) was determined using logistic regression models based on generalized estimating equations (which adjust the variance estimates for the inherent correlation that arises due to repeat pregnancies in the same woman). Data were adjusted for hospital type, year of delivery, marital status, age, parity, chronic hypertension, and mild and severe preeclampsia. More smokers, 1.52%, experienced placental abruption than nonsmokers, 0.73%, which translated into a 2-fold greater risk for smokers than nonsmokers (RR, 2.05; 95% CI, ). ΜΗ ΚΑΠΝΙΣΤΕΣ ΝΥΝ ΚΑΠΝΙΣΤΕΣ ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ Ananth et al. Am J Epidemiol. 1996;144(9): Reference Ananth CV, Savitz DA, Luther ER. Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol. 1996;144(9):
 were in women who smoked. Adjusted relative risk (RR) was determined using logistic regression models based on generalized estimating equations (which adjust the variance estimates for the inherent correlation that arises due to repeat pregnancies in the same woman). Data were adjusted for hospital type, year of delivery, marital status, age, parity, chronic hypertension, and mild and severe preeclampsia. More smokers, 1.52%, experienced placental abruption than nonsmokers, 0.73%, which translated into a 2-fold greater risk for smokers than nonsmokers (RR, 2.05; 95% CI, ). ΜΗ ΚΑΠΝΙΣΤΕΣ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ. Ananth et al. Am J Epidemiol. 1996;144(9): Reference. Ananth CV, Savitz DA, Luther ER. Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol. 1996;144(9):")
30
ΚΑΠΝΙΣΜΑ ΚΑΙ ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ ΣΥΣΧΕΤΙΣΗ ΜΕ ΠΟΣΟΤΗΤΑ ΚΑΠΝΟΥ
Odds Ratio (95% CI)a Key Point Smoking increases the risk of placental abruption in a dose-dependent manner. Cnattingius analyzed data from 1,057,711 births occurring in Sweden from 1983 to The mothers’ smoking habits were determined at the first prenatal visit and were categorized by extent of smoking: 25% of the mothers were smokers, 10% were heavy smokers (10 or more cigarettes/day), and 15% were moderate smokers (<10/day). Multiple logistic regression analysis controlling for parity and family situation was performed to determine the effect of smoking on placental abruption. The placental abruption rate for nonsmokers was 4 per 1000 live births. In contrast, the rate for moderate smokers was 7.8/1000, and for heavy smokers, 9.9/ This translated into an adjusted odds ratio (OR) of 2.0 for moderate smokers (95% CI, ) and 2.5 for heavy smokers (95% CI, ). ΜΗ ΚΑΠΝΙΣΤΕΣ b 1-9 10 ΤΣΙΓΑΡΑ / ΗΜΕΡΑ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Cnattingius. Am J Epidemiol. 1997;145(4): Reference Cnattingius S. Maternal age modifies the effect of maternal smoking on intrauterine growth retardation but not on late fetal death and placental abruption. Am J Epidemiol. 1997;145(4):
a. Key Point. Smoking increases the risk of placental abruption in a dose-dependent manner. Cnattingius analyzed data from 1,057,711 births occurring in Sweden from 1983 to The mothers’ smoking habits were determined at the first prenatal visit and were categorized by extent of smoking: 25% of the mothers were smokers, 10% were heavy smokers (10 or more cigarettes/day), and 15% were moderate smokers (<10/day). Multiple logistic regression analysis controlling for parity and family situation was performed to determine the effect of smoking on placental abruption. The placental abruption rate for nonsmokers was 4 per 1000 live births. In contrast, the rate for moderate smokers was 7.8/1000, and for heavy smokers, 9.9/1000. This translated into an adjusted odds ratio (OR) of 2.0 for moderate smokers (95% CI, ) and 2.5 for heavy smokers (95% CI, ). ΜΗ ΚΑΠΝΙΣΤΕΣ. b 10. ΤΣΙΓΑΡΑ / ΗΜΕΡΑ ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Cnattingius. Am J Epidemiol. 1997;145(4): Reference. Cnattingius S. Maternal age modifies the effect of maternal smoking on intrauterine growth retardation but not on late fetal death and placental abruption. Am J Epidemiol. 1997;145(4):")
31
ΚΑΠΝΙΣΜΑ ΚΑΙ ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ
15%- 25% των αποκολλήσεων του πλακούντα θα είχαν αποφευχθεί εάν οι γυναίκες διέκοπταν το κάπνισμα κατά τη διάρκεια της κύησης. ΑΠΟΔΙΔΟΜΕΝΕΣ ΣΤΟ ΚΑΠΝΙΣΜΑ Key Point Fifteen to twenty-five percent of placental abruption episodes could be prevented if women stopped smoking cigarettes during their pregnancies. Ananth et al conducted a meta-analysis of 13 observational studies conducted between 1966 and 1997, which included a total of 1,358,083 pregnancies. They assessed the risk of placental abruption that could be attributable to cigarette smoking by calculating the population attributable risk percentage, and concluded that 25% of placental abruption is due to cigarette smoking. ΑΠΟΚΟΛΛΗΣΗ ΠΛΑΚΟΥΝΤΑ Ananth et al. Obstet Gynecol. 1999;93: Reference Ananth CV, Smulian JC, Vintzileos AM. Incidence of placental abruption in relation to cigarette smoking and hypertensive disorders during pregnancy: a meta-analysis of observational studies. Obstet Gynecol. 1999;93:

32
ΚΑΠΝΙΣΜΑ ΚΑΙ ΑΥΤΟΜΑΤΗ ΑΠΟΒΟΛΗ 1ου ΤΡΙΜΗΝΟΥ
9% των αυτόματων αποβολών μπορεί να αποδοθούν στο κάπνισμα P for trend <.001 Odds Ratio (95% CI)a Key Point Compared with nonsmokers, women who smoked more than 10 cigarettes per day in the first trimester experienced a higher rate of spontaneous abortion. To determine the effects of smoking on spontaneous abortion rates, Chatenoud et al conducted a case-controlled study of women at the Clinica Luigi Mangiagalli in Milan, Italy, starting in The study included 1543 randomly selected women who delivered healthy infants and 782 women who experienced a spontaneous abortion within the first 12 weeks of gestation. The women were interviewed about smoking habits and other possible risk factors. Data were analyzed by computing odds ratios and using unconditional multiple logistic regression analysis, which included terms for center, age, education, marital status, maternal family history of spontaneous abortion, history of miscarriages, nausea, and alcohol and coffee drinking habits during the first trimester. Women who smoked at least 10 cigarettes per day had a greater risk of spontaneous abortion than nonsmokers (OR, 1.4; 95% CI, ). 10 ΤΣΙΓΑΡΑ / ΗΜΕΡΑ TΟ 1ο ΤΡΙΜΗΝΟ ΤΗΣ ΚΥΗΣΗΣ Logistic regression estimates include the following covariates: center, age, marital status, maternal family history of spontaneous abortion, education, history of miscarriages, nausea, and alcohol and coffee intake in the first trimester of pregnancy. Chatenoud et al. Ann Epidemiol. 1998;8(8): Reference Chatenoud L, Parazzini F, di Cintio E, et al. Paternal and maternal smoking habits before conception and during the first trimester: relation to spontaneous abortion. Ann Epidemiol. 1998;8(8):
a. Key Point. Compared with nonsmokers, women who smoked more than 10 cigarettes per day in the first trimester experienced a higher rate of spontaneous abortion. To determine the effects of smoking on spontaneous abortion rates, Chatenoud et al conducted a case-controlled study of women at the Clinica Luigi Mangiagalli in Milan, Italy, starting in The study included 1543 randomly selected women who delivered healthy infants and 782 women who experienced a spontaneous abortion within the first 12 weeks of gestation. The women were interviewed about smoking habits and other possible risk factors. Data were analyzed by computing odds ratios and using unconditional multiple logistic regression analysis, which included terms for center, age, education, marital status, maternal family history of spontaneous abortion, history of miscarriages, nausea, and alcohol and coffee drinking habits during the first trimester. Women who smoked at least 10 cigarettes per day had a greater risk of spontaneous abortion than nonsmokers (OR, 1.4; 95% CI, ). 10. ΤΣΙΓΑΡΑ / ΗΜΕΡΑ TΟ 1ο ΤΡΙΜΗΝΟ ΤΗΣ ΚΥΗΣΗΣ. Logistic regression estimates include the following covariates: center, age, marital status, maternal family history of spontaneous abortion, education, history of miscarriages, nausea, and alcohol and coffee intake in the first trimester of pregnancy. Chatenoud et al. Ann Epidemiol. 1998;8(8): Reference. Chatenoud L, Parazzini F, di Cintio E, et al. Paternal and maternal smoking habits before conception and during the first trimester: relation to spontaneous abortion. Ann Epidemiol. 1998;8(8):")
33
ΕΠΙΔΡΑΣΗ ΤΟΥ ΚΑΠΝΙΣΜΑΤΟΣ ΣΤΟΝ ΠΛΑΚΟΥΝΤΑ
Cigarette smoking during pregnancy Reduced dimensions of the fetal capillaries in villi Modify placental blood flow Diminish the area for exchange of gasses and nutrients between the mother and the fetus Key Point Capillary dimensions are reduced in infants of mothers who smoke. This could contribute to their lower birth weights. Larsen et al studied the placental vasculature of smoking and nonsmoking mothers after delivery. Placentas were fixed and vertical sections were cut for measurement of the vasculature. In addition, neonatal data were recorded, including birth weight. Seventy-two placentas were analyzed: 25 from nonsmokers, 15 from light smokers (5-10/cigarettes/day), 16 from heavy smokers (11-20/day), and 16 from very heavy smokers (>20/day). Data were expressed as median and range, and the Kurskal-Wallis test was used to determine significance (P<.05). Median birth weights of the infants decreased significantly in those born to heavy smokers: nonsmokers (NS): 3480 g ( ); light smokers (LS): 3690 g ( ); heavy smokers (HS): 3325 g ( ); very heavy smokers (VHS): 3175 g ( ) (P=.009). Placental capillary volume, surface area, length, and volume fraction all decreased similarly in all 3 groups of smokers; for example, capillary surface area (m2): NS: 23.0 ( ), LS: 15.7 ( ), HS: 15.9 ( ), VHS: 16.5 ( )(P=.003). The reduced dimensions of the placental capillaries could modify placental blood flow and diminish the area for exchange of gasses and nutrients between the mother and fetus. This could contribute to the observed reduction in birth weights of infants born to smoking mothers. Reduction in birth weight of infants delivered by smoking mothers Adapted from Larsen et al. Am J Obstet Gynecol. 2002;186: Reference Larsen LG, Clausen HV, Jonsson L. Stereologic examination of placentas from mothers who smoke during pregnancy. Am J Obstet Gynecol. 2002;186:
, 16 from heavy smokers (11-20/day), and 16 from very heavy smokers (>20/day). Data were expressed as median and range, and the Kurskal-Wallis test was used to determine significance (P<.05). Median birth weights of the infants decreased significantly in those born to heavy smokers: nonsmokers (NS): 3480 g ( ); light smokers (LS): 3690 g ( ); heavy smokers (HS): 3325 g ( ); very heavy smokers (VHS): 3175 g ( ) (P=.009). Placental capillary volume, surface area, length, and volume fraction all decreased similarly in all 3 groups of smokers; for example, capillary surface area (m2): NS: 23.0 ( ), LS: 15.7 ( ), HS: 15.9 ( ), VHS: 16.5 ( )(P=.003). The reduced dimensions of the placental capillaries could modify placental blood flow and diminish the area for exchange of gasses and nutrients between the mother and fetus. This could contribute to the observed reduction in birth weights of infants born to smoking mothers. Reduction in birth weight of infants delivered by smoking mothers. Adapted from Larsen et al. Am J Obstet Gynecol. 2002;186: Reference. Larsen LG, Clausen HV, Jonsson L. Stereologic examination of placentas from mothers who smoke during pregnancy. Am J Obstet Gynecol. 2002;186:")
34
ΕΠΙΔΡΑΣΗ ΤΟΥ ΚΑΠΝΙΣΜΑΤΟΣ ΣΤΗΝ ΕΜΒΡΥΪΚΗ ΑΝΑΠΤΥΞΗ
Δοσοεξαρτώμενη σχέση μεταξύ μητρικού καπνίσματος και χαμηλού βάρους εμβρύου για την ηλικία του. Odds Ratio (95% CI)a Key Point Maternal smoking more than doubles the likelihood of infants being small for their gestational age. Cnattingius et al analyzed data from 1,057,711 births occurring in Sweden from 1983 to The mothers’ smoking habits were determined at the first prenatal visit and were categorized by extent of smoking; 25% of the mothers were smokers, 10% heavy smokers (10 or more cigarettes/day), and 15% were moderate smokers (<10/day). Multiple logistic regression analysis controlling for parity and family situation was performed to determine the effect of smoking on birth weight. Infants were considered small for gestational age (SGA) if their weight was <2 standard deviations below the Swedish recorded mean birth weight for their gestational age. The infants of smokers were more than twice as likely to be SGA than those of nonsmokers. The OR for moderate smokers was 2.1 (95% CI, ), and the odds ratio for heavy smokers was 2.7 (95% CI, ). ΜΗ ΚΑΠΝΙΣΤΕΣ 10 ΤΣΙΓΑΡΑ / ΗΜΕΡΑ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Cnattingius. Am J Epidemiol. 1997;145(4): Reference Cnattingius S. Maternal age modifies the effect of maternal smoking on intrauterine growth retardation but not on late fetal death and placental abruption. Am J Epidemiol. 1997;145(4):
a. Key Point. Maternal smoking more than doubles the likelihood of infants being small for their gestational age. Cnattingius et al analyzed data from 1,057,711 births occurring in Sweden from 1983 to The mothers’ smoking habits were determined at the first prenatal visit and were categorized by extent of smoking; 25% of the mothers were smokers, 10% heavy smokers (10 or more cigarettes/day), and 15% were moderate smokers (<10/day). Multiple logistic regression analysis controlling for parity and family situation was performed to determine the effect of smoking on birth weight. Infants were considered small for gestational age (SGA) if their weight was <2 standard deviations below the Swedish recorded mean birth weight for their gestational age. The infants of smokers were more than twice as likely to be SGA than those of nonsmokers. The OR for moderate smokers was 2.1 (95% CI, ), and the odds ratio for heavy smokers was 2.7 (95% CI, ). ΜΗ ΚΑΠΝΙΣΤΕΣ. 10 ΤΣΙΓΑΡΑ / ΗΜΕΡΑ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Cnattingius. Am J Epidemiol. 1997;145(4): Reference. Cnattingius S. Maternal age modifies the effect of maternal smoking on intrauterine growth retardation but not on late fetal death and placental abruption. Am J Epidemiol. 1997;145(4):")
35
ΚΙΝΔΥΝΟΣ ΕΚΤΟΠΗΣ ΚΥΗΣΗ ΚΑΙ ΚΑΠΝΙΣΜΑ
Το κάπνισμα αυξάνει σημαντικά το κίνδυνο έκτοπης κύησης δοσοεξαρτώμενα 3.9 3.1 Odds Ratio (95% CI)a 1.7 1.5 Key Point Smoking increases the likelihood of occurrence of ectopic pregnancy in a dose-dependent manner. Bouyer et al conducted a study to determine the effect of smoking and other variables on ectopic pregnancy. They gathered data from the ectopic pregnancy register of Auvergne, France. Information on each of the women was collected by interview and through medical records. The data analyzed spanned from September 1993 to December 2000, and included 803 cases. The 1683 controls were women who delivered at the center and those who delivered shortly after each case was treated. None of the women analyzed was using contraception at the time of conception and all were living as a couple. Multivariate logistic regression analysis was used to analyze the data and statistics were expressed as adjusted ORs. In addition, attributable risk from each variable was calculated. Smoking risk was adjusted for age, prior spontaneous abortions, prior induced abortions, appendectomy, prior sexually transmitted diseases, prior tubal surgery, previous use of contraceptives, previous use of intrauterine device, and history of infertility. Smoking increased the risk of ectopic pregnancy in a dose-dependent manner. Ex-smokers had an increased risk of ectopic pregnancy (OR, 1.5; 95% CI, ), whereas the risk for current smokers was higher and increased with consumption of greater numbers of cigarettes: 1-9 cigarettes/day: OR, 1.7; 95% CI, ; cigarettes/day: OR, 3.1; 95% CI, ; ≥20 cigarettes/day: OR, 3.9; 95% CI, 1.0 ΜΗ ΚΑΠΝΙΣΤΕΣ ΠΡΩΗΝ ΚΑΠΝΙΣΤΕΣ 1-9 10-19 20 ΝΥΝ ΚΑΠΝΙΣΤΕΣ (ΤΣΙΓΑΡΑ / ΗΜΕΡΑ) Adjusted for age (the category years was taken as the reference because this corresponds to the mean age for delivery in France at the time of the study). bP for trend =.001. Bouyer. Am J Epidemiol. 2003;157(3): Reference Bouyer J, Coste J, Shojaei T, et al. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population-based study in France. Am J Epidemiol. 2003;157(3):
a Key Point. Smoking increases the likelihood of occurrence of ectopic pregnancy in a dose-dependent manner. Bouyer et al conducted a study to determine the effect of smoking and other variables on ectopic pregnancy. They gathered data from the ectopic pregnancy register of Auvergne, France. Information on each of the women was collected by interview and through medical records. The data analyzed spanned from September 1993 to December 2000, and included 803 cases. The 1683 controls were women who delivered at the center and those who delivered shortly after each case was treated. None of the women analyzed was using contraception at the time of conception and all were living as a couple. Multivariate logistic regression analysis was used to analyze the data and statistics were expressed as adjusted ORs. In addition, attributable risk from each variable was calculated. Smoking risk was adjusted for age, prior spontaneous abortions, prior induced abortions, appendectomy, prior sexually transmitted diseases, prior tubal surgery, previous use of contraceptives, previous use of intrauterine device, and history of infertility. Smoking increased the risk of ectopic pregnancy in a dose-dependent manner. Ex-smokers had an increased risk of ectopic pregnancy (OR, 1.5; 95% CI, ), whereas the risk for current smokers was higher and increased with consumption of greater numbers of cigarettes: 1-9 cigarettes/day: OR, 1.7; 95% CI, ; cigarettes/day: OR, 3.1; 95% CI, ; ≥20 cigarettes/day: OR, 3.9; 95% CI, ΜΗ ΚΑΠΝΙΣΤΕΣ. ΠΡΩΗΝ. ΚΑΠΝΙΣΤΕΣ 20. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. (ΤΣΙΓΑΡΑ / ΗΜΕΡΑ) Adjusted for age (the category years was taken as the reference because this corresponds to the mean age for delivery in France at the time of the study). bP for trend =.001. Bouyer. Am J Epidemiol. 2003;157(3): Reference. Bouyer J, Coste J, Shojaei T, et al. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population-based study in France. Am J Epidemiol. 2003;157(3):")
36
ΠΑΡΑΓΟΝΤΕΣ ΚΙΝΔΥΝΟΥ ΓΙΑ ΕΚΤΟΠΗ ΚΥΗΣΗ
ΑΠΟΔΙΔΟΜΕΝΟΣ ΚΙΝΔΥΝΟΣ Η επίδραση του καπνίσματος στη έκτοπη κύηση υποτιμάται ενώ είναι ανάλογη των λοιμώξεων. Λοιμώξεις, Χειρουργείο 33% Κάπνισμα 35% Key Point A large percentage of ectopic pregnancies can be attributed to smoking. Bouyer et al conducted a study to determine the effect of smoking and other variables on ectopic pregnancy. They gathered data from the ectopic pregnancy register of Auvergne, France. Information on each of the women was collected by interview and through medical records. The data analyzed spanned from September 1993 to December 2000, and included 803 cases. The 1683 controls were women who delivered at the center and those who delivered shortly after each case was treated. None of the women analyzed was using contraception at the time of conception and all were living as a couple. Multivariate logistic regression analysis was used to analyze the data, and statistics were expressed as adjusted ORs. In addition, attributable risk from each variable was calculated. Smoking risk was adjusted for age, prior spontaneous abortions, prior induced abortions, appendectomy, prior sexually transmitted diseases, prior tubal surgery, previous use of contraceptives, previous use of intrauterine device, and history of infertility. The study calculated the percentage of ectopic pregnancies attributable to smoking in this population, which emerged as 35%, which was similar to the percent attributable to infectious causes and tubal surgeries considered together (33%). Άλλα 32% Bouyer. Am J Epidemiol. 2003;157(3): Reference Bouyer J, Coste J, Shojaei T, et al. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population-based study in France. Am J Epidemiol. 2003;157(3):
. Άλλα. 32% Bouyer. Am J Epidemiol. 2003;157(3): Reference. Bouyer J, Coste J, Shojaei T, et al. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population-based study in France. Am J Epidemiol. 2003;157(3):")
37
ΚΑΠΝΙΣΜΑ ΚΑΙ ΚΙΝΔΥΝΟΣ ΕΜΒΡΥΙΚΟΥ ΘΑΝΑΤΟΥ
Το κάπνισμα σχετίζεται με αυξημένο κίνδυνο εμβρυïκού θανάτου Relative Risk (95% CI) Key Point Smoking is associated with increased risk of fetal death. Yuan et al analyzed United States data for live births and fetal deaths in All singleton live births and all fetal deaths at 20 weeks or later in gestation were included in the analysis. Data from all states (and the District of Columbia) where information on maternal smoking was available were included. (Excluded were California, Hawaii, Indiana, Louisiana, Maryland, Massachusetts, New York, Oklahoma, South Dakota, Texas, and Illinois.) In total, there were 1,806,406 live births and 2620 fetal deaths analyzed. Relative risk and 95% CI were determined. Fetal death occurred more often when the mother was a smoker. The RR for fetal death with maternal smoking was 1.73 (95% CI, ) compared with 1.00 in nonsmokers. ΜΗ ΚΑΠΝΙΣΤΡΙΕΣ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Yuan et al. Am J Obstet Gynecol. 2005;193: Reference Yuan H, Platt RW, Morin L, Joseph KS, Kramer MS. Fetal deaths in the United States, 1997 vs Am J Obstet Gynecol. 2005;193:
 Key Point. Smoking is associated with increased risk of fetal death. Yuan et al analyzed United States data for live births and fetal deaths in All singleton live births and all fetal deaths at 20 weeks or later in gestation were included in the analysis. Data from all states (and the District of Columbia) where information on maternal smoking was available were included. (Excluded were California, Hawaii, Indiana, Louisiana, Maryland, Massachusetts, New York, Oklahoma, South Dakota, Texas, and Illinois.) In total, there were 1,806,406 live births and 2620 fetal deaths analyzed. Relative risk and 95% CI were determined. Fetal death occurred more often when the mother was a smoker. The RR for fetal death with maternal smoking was 1.73 (95% CI, ) compared with 1.00 in nonsmokers. ΜΗ ΚΑΠΝΙΣΤΡΙΕΣ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Yuan et al. Am J Obstet Gynecol. 2005;193: Reference. Yuan H, Platt RW, Morin L, Joseph KS, Kramer MS. Fetal deaths in the United States, 1997 vs Am J Obstet Gynecol. 2005;193:")
38
ΠΡΩÏΜΗ ΡΗΞΗ ΥΜΕΝΩΝ (PPROM) ΚΑΙ ΚΑΠΝΙΣΜΑ
Rate of PPROM (per 1000) Key Point Smoking increases the rate of PPROM in a dose-dependent manner. Data from 311,977 live births in Sweden from 1991 to 1993 were compiled, and the effect of smoking on PPROM was determined. The rate of PPROM in nonsmoking mothers was 6.5 per 1000 live single births, whereas mothers who smoked 1 to 9 cigarettes per day had a rate of 9.3/1000, and the rate for mothers who smoked at least 10 cigarettes per day was 11.5/1000. ΜΗ ΚΑΠΝΙΣΤΕΣ 1-9 10 ΤΣΙΓΑΡΑ / ΗΜΕΡΑ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Kyrklund-Blomberg et al. Am J Obstet Gynecol. 1998;179: Reference Kyrklund-Blomberg NB, Cnattingius S. Preterm birth and maternal smoking: risks related to gestational age and onset of delivery. Am J Obstet Gynecol. 1998;179:
 Key Point. Smoking increases the rate of PPROM in a dose-dependent manner. Data from 311,977 live births in Sweden from 1991 to 1993 were compiled, and the effect of smoking on PPROM was determined. The rate of PPROM in nonsmoking mothers was 6.5 per 1000 live single births, whereas mothers who smoked 1 to 9 cigarettes per day had a rate of 9.3/1000, and the rate for mothers who smoked at least 10 cigarettes per day was 11.5/1000. ΜΗ ΚΑΠΝΙΣΤΕΣ 10. ΤΣΙΓΑΡΑ / ΗΜΕΡΑ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Kyrklund-Blomberg et al. Am J Obstet Gynecol. 1998;179: Reference. Kyrklund-Blomberg NB, Cnattingius S. Preterm birth and maternal smoking: risks related to gestational age and onset of delivery. Am J Obstet Gynecol. 1998;179:")
39
ΠΡΩÏΜΗ ΡΗΞΗ ΥΜΕΝΩΝ (PROM)
5% -15% όλων των κυήσεων Πρώιμη (<37 w.) ρήξη υμένων (PPROM) προκύπτει σε 0.7%-2.0% όλων των κυήσεων PPROM αποδίδεται το 30% όλων των πρώιμων κυήσεων Premature rupture of membranes (PROM) occurs in 5% to 15% of all pregnancies. Preterm (<37 weeks) PROM (PPROM) occurs in 0.7% to 2.0% of all pregnancies, and accounts for approximately 30% of all preterm births. Andres et al. Semin Neonatol. 2000;5: ; Accessed October 12, 2007. Reference Andres RL, Day M-C. Perinatal complications associated with maternal tobacco use. Semin Neonatol. 2000;5:
 ρήξη υμένων (PPROM) προκύπτει σε 0.7%-2.0% όλων των κυήσεων. PPROM αποδίδεται το 30% όλων των πρώιμων κυήσεων. Premature rupture of membranes (PROM) occurs in 5% to 15% of all pregnancies. Preterm (<37 weeks) PROM (PPROM) occurs in 0.7% to 2.0% of all pregnancies, and accounts for approximately 30% of all preterm births. Andres et al. Semin Neonatol. 2000;5: ; Accessed October 12, Reference. Andres RL, Day M-C. Perinatal complications associated with maternal tobacco use. Semin Neonatol. 2000;5:")
40
ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΡΩïΜΟΣ ΤΟΚΕΤΟΣ (<32 ΕΒΔΟΜΑΔΑ)
ΚΑΠΝΙΣΜΑ ΚΑΙ ΠΡΩïΜΟΣ ΤΟΚΕΤΟΣ (<32 ΕΒΔΟΜΑΔΑ) Odds Ratio (95% CI)a Key Point Smoking is associated with risk of preterm birth. Burguet et al studied the relationship between smoking and risk of preterm birth using data from the EPIPAGE study conducted in France in The study included all the births occurring in that year between 22 and 32 weeks of gestation in 9 areas of France (n=861) and a control group of full-term infants from the same areas (n=560). Data were adjusted for maternal age, marital status, educational level, employment, prepregnancy body mass index, previous induced or spontaneous abortion, and parity. Multivariate logistic regression analysis was used to estimate the ORs of preterm birth associated with smoking. Any extent of regular maternal smoking, from 1 to more than 10 cigarettes per day, was associated with higher incidences of preterm birth. (All smokers: OR, 1.7; 95% CI, ; 1-10/day: 1.6; 95% CI, ; ≥10/day: 1.9; 95% CI, ) Preterm infants are vulnerable to many complications, including respiratory, gastrointestinal, immune system, central nervous system, hearing, and vision problems. Infants born prior to 32 weeks have the greatest risk for death and poor health outcomes. ΜΗ ΚΑΠΝΙΣΤΕΣ 1-9 10 ΤΣΙΓΑΡΑ / ΗΜΕΡΑ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Adjusted for maternal age, marital status, educational level, employment, prepregnancy body mass index, previous induced or spontaneous abortion, and parity. Burguet et al. Br J Obstet Gynaecol. 2004;111: References Behrman RE, Stith Butler A, eds. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: National Academies Press; 2007. Burguet A, Kaminski M, Abraham-Lerat L, et al; the EPIPAGE Study Group. The complex relationship between smoking in pregnancy and very preterm delivery: results of the EPIPAGE study. Br J Obstet Gynaecol. 2004;111:
 Odds Ratio (95% CI)a. Key Point. Smoking is associated with risk of preterm birth. Burguet et al studied the relationship between smoking and risk of preterm birth using data from the EPIPAGE study conducted in France in The study included all the births occurring in that year between 22 and 32 weeks of gestation in 9 areas of France (n=861) and a control group of full-term infants from the same areas (n=560). Data were adjusted for maternal age, marital status, educational level, employment, prepregnancy body mass index, previous induced or spontaneous abortion, and parity. Multivariate logistic regression analysis was used to estimate the ORs of preterm birth associated with smoking. Any extent of regular maternal smoking, from 1 to more than 10 cigarettes per day, was associated with higher incidences of preterm birth. (All smokers: OR, 1.7; 95% CI, ; 1-10/day: 1.6; 95% CI, ; ≥10/day: 1.9; 95% CI, ) Preterm infants are vulnerable to many complications, including respiratory, gastrointestinal, immune system, central nervous system, hearing, and vision problems. Infants born prior to 32 weeks have the greatest risk for death and poor health outcomes. ΜΗ ΚΑΠΝΙΣΤΕΣ 10. ΤΣΙΓΑΡΑ / ΗΜΕΡΑ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Adjusted for maternal age, marital status, educational level, employment, prepregnancy body mass index, previous induced or spontaneous abortion, and parity. Burguet et al. Br J Obstet Gynaecol. 2004;111: References. Behrman RE, Stith Butler A, eds. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: National Academies Press; Burguet A, Kaminski M, Abraham-Lerat L, et al; the EPIPAGE Study Group. The complex relationship between smoking in pregnancy and very preterm delivery: results of the EPIPAGE study. Br J Obstet Gynaecol. 2004;111:")
41
ΠΡΟΔΡΟΜΟΣ ΠΛΑΚΟΥΝΤΑΣ 0.3% -0.5% των κυήσεων Προδιαθεσικοί παράγοντες:
Προηγούμενη καισαρική Έκτρωση Χειρουργείο κοιλιάς Κάπνισμα ⇑ ηλικία Πολύτοκες Χρήση κοκαίνης Πολύδυμη κύηση Complete Partial Key Point Placenta previa complicates 0.3% to 0.5% of pregnancies and is associated with numerous risk factors and complications. Placenta previa is a condition in which the placenta overlies or is adjacent to the internal os of the cervix. It is traditionally divided into 4 categories, each depending on how low the placenta is lying and how much of the internal os is covered. A low-lying placenta does not reach the internal os; marginal reaches, but does not cover it; partial covers part of the os; and complete placenta previa covers the entire os. Women with placenta previa may experience painless bleeding in the second half of pregnancy. Placenta previa is present in 0.3% to 0.5% of pregnancies. There are a number of factors that have been determined to increase the risk of placenta previa, including prior cesarean delivery, termination of pregnancy, uterine surgery, smoking, increasing age, multiparity, cocaine use, and a multiple pregnancy. Placenta previa is associated with multiple potential complications including antepartum bleeding, need for hysterectomy, morbid adherence of the placenta, intrapartum hemorrhage, postpartum hemorrhage, septicemia, and thrombophlebitis. Marginal Low lying Oyelese et al. Obstet Gynecol. 2006;107(4): Reference Oyelese Y, Smulian JC. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol. 2006;107(4):
: Reference. Oyelese Y, Smulian JC. Placenta previa, placenta accreta, and vasa previa. Obstet Gynecol. 2006;107(4):")
42
ΠΡΟΔΡΟΜΟΣ ΠΛΑΚΟΥΝΤΑΣ ΚΑΙ ΚΑΠΝΙΣΜΑ ΔΟΣΟΕΞΑΡΤΩΜΕΝΗ ΣΥΣΧΕΤΙΣΗ
P<.00001 Incidence per 1000 Births Key Point Smoking increases the risk of placenta previa in a dose-dependent manner. Meyer et al analyzed data from the Ontario Perinatal Mortality Study, which was conducted from 1960 to 1961 and included 51,490 births. The mothers’ maximum smoking habits at any time during pregnancy were used for this analysis and were divided into none, <1 pack/day, and 1 pack per day. Data were analyzed for significance using the Cochran’s 2 test. There was a significant (P<.00001) increase in placenta previa with increasing amounts of maternal smoking. Heavy smokers had an incidence of 13.1 for every 1000 births, compared with an incidence of 8.2 per 1000 for moderate smokers and 6.4 per 1000 for nonsmokers. ΓΥΝΑΙΚΕΣ ΚΑΠΝΙΣΤΡΙΕΣ <1 πακέτο/ημέρα ΓΥΝΑΙΚΕΣ ΚΑΠΝΙΣΤΡΙΕΣ 1 πακέτο/ημέρα ΜΗ ΚΑΠΝΙΣΤΕΣ ΤΣΙΓΑΡΑ / ΗΜΕΡΑ ΝΥΝ ΚΑΠΝΙΣΤΕΣ Meyer et al. Am J Obstet Gynecol. 1977;128(5): Reference Meyer MB, Tonascia JA. Maternal smoking, pregnancy complications, and perinatal mortality. Am J Obstet Gynecol. 1977;128:
 increase in placenta previa with increasing amounts of maternal smoking. Heavy smokers had an incidence of 13.1 for every 1000 births, compared with an incidence of 8.2 per 1000 for moderate smokers and 6.4 per 1000 for nonsmokers. ΓΥΝΑΙΚΕΣ ΚΑΠΝΙΣΤΡΙΕΣ <1 πακέτο/ημέρα. ΓΥΝΑΙΚΕΣ. ΚΑΠΝΙΣΤΡΙΕΣ 1 πακέτο/ημέρα. ΜΗ ΚΑΠΝΙΣΤΕΣ. ΤΣΙΓΑΡΑ / ΗΜΕΡΑ. ΝΥΝ ΚΑΠΝΙΣΤΕΣ. Meyer et al. Am J Obstet Gynecol. 1977;128(5): Reference. Meyer MB, Tonascia JA. Maternal smoking, pregnancy complications, and perinatal mortality. Am J Obstet Gynecol. 1977;128:")
43
ΕΠΙΔΡΑΣΗ ΤΟΥ ΚΑΠΝΙΣΜΑΤΟΣ ΣΤΟΝ ΑΙΜΑΤΟΚΡΙΤΗ ΤΟΥ ΕΜΒΡΥΟΥ
⇑ht εμβύου πιθανά να οφείλεται στη χρόνια υποξαιμία P≤.05a Ht (%) Key Point The fetuses of smokers experience chronic hypoxemia, as evidenced by elevated hematocrit level. Bush et al measured hematocrit levels in cord blood samples after delivery of infants in Aberdeen, United Kingdom. Mothers’ smoking habits were determined both by interview and by measuring maternal plasma cotinine levels at 34 weeks’ gestation. Comparisons between nonsmokers (n=10-12) and current smokers (n=22-27) were expressed as means and SEM, and significance was determined by using the t test. The mean hematocrit of the fetuses of nonsmokers was 52.3% (SEM: 2.41); of current smokers determined by reported cigarette intake, 55.6% (SEM: 1.08); and of current smokers determined by cotinine levels, 55.4% (SEM: 1.09) (P≤05). ΜΗ ΚΑΠΝΙΣΤΡΙΕΣ ΝΥΝ ΚΑΠΝΙΣΤΡΙΕΣ (packyears) ΝΥΝ ΚΑΠΝΙΣΤΡΙΕΣ (ΕΠΙΠΕΔΑ ΚΟΤΙΝΙΝΗΣ) Bush et al. Placenta. 2000;21: Reference Bush PG, Mayhew TM, Abramovich DR, Aggett PJ, Burke MD, Page KR. Maternal cigarette smoking and oxygen diffusion across the placenta. Placenta. 2000;21:
 Key Point. The fetuses of smokers experience chronic hypoxemia, as evidenced by elevated hematocrit level. Bush et al measured hematocrit levels in cord blood samples after delivery of infants in Aberdeen, United Kingdom. Mothers’ smoking habits were determined both by interview and by measuring maternal plasma cotinine levels at 34 weeks’ gestation. Comparisons between nonsmokers (n=10-12) and current smokers (n=22-27) were expressed as means and SEM, and significance was determined by using the t test. The mean hematocrit of the fetuses of nonsmokers was 52.3% (SEM: 2.41); of current smokers determined by reported cigarette intake, 55.6% (SEM: 1.08); and of current smokers determined by cotinine levels, 55.4% (SEM: 1.09) (P≤05). ΜΗ ΚΑΠΝΙΣΤΡΙΕΣ. ΝΥΝ ΚΑΠΝΙΣΤΡΙΕΣ. (packyears) ΝΥΝ ΚΑΠΝΙΣΤΡΙΕΣ. (ΕΠΙΠΕΔΑ ΚΟΤΙΝΙΝΗΣ) Bush et al. Placenta. 2000;21: Reference. Bush PG, Mayhew TM, Abramovich DR, Aggett PJ, Burke MD, Page KR. Maternal cigarette smoking and oxygen diffusion across the placenta. Placenta. 2000;21:")
44
ΔΙΑΚΟΠΗ ΚΑΠΝΙΣΜΑΤΟΣ ΣΕ ΓΟΝΕΙΣ
Η έκθεση στον καπνό του τσιγάρου μετά τη γέννηση ενέχει ΣΟΒΑΡΟΥΣ, ΑΠΟΛΥΤΑ ΤΕΚΜΗΡΙΩΜΕΝΟΥΣ κινδύνους για το νεογνό, βρέφος και παιδί, αντίστοιχους με αυτούς της έκθεσης του εμβρύου καπνίστριας μητέρας στη διάρκεια της κύησης. Το κάπνισμα των γονέων αποτελεί πρότυπο για έναρξη καπνίσματος στα παιδιά, συγκεκριμένα διπλασιάζει τον κίνδυνο της καπνιστικής συνήθειας στα παιδιά. Το 1/3 περίπου των παιδιών που καπνίζουν μπορεί να ααποδοθεί στην καπνιστική συνήθεια των γονέων.

45
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΚΑΡΚΙΝΟΓΟΝΟΣ ΔΡΑΣΗ
Ca πνεύμονος (αύξηση κινδύνου κατά 20-3-%) το 1/3 των καρκίνων σε μη καπνιστές αποδίδεται σε παθητικό κάπνισμα. Ca παραρρινίων κόλπων Ca τραχήλου μήτρας (?) Λευχαιμία (?) Ca μαστού (?) Ca εγκεφάλου στα παιδιά (?)
 το 1/3 των καρκίνων σε μη καπνιστές αποδίδεται σε παθητικό κάπνισμα. Ca παραρρινίων κόλπων. Ca τραχήλου μήτρας ( ) Λευχαιμία ( ) Ca μαστού ( ) Ca εγκεφάλου στα παιδιά ( )")
46
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΕΝΗΛΙΚΕΣ
ΒΡΟΓΧΙΚΟ ΑΣΘΜΑ Επιδείνωση βρογχικού άσθματος Πρόκληση παροξύνσεων. Παράγοντας κινδύνου για φτωχή πρόγνωση και κακό έλεγχο των συμπτωμάτων. Το παθητικό κάπνισμα επιδεινώνει το άσθμα των ενηλίκων κατά 20%

47
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ ΚΑΙ ΕΝΗΛΙΚΕΣ
Ερεθισμό στα μάτια 20% Βήχα 21% ναυτία 8% Κεφαλαλγία 6%

49
ASTHMA AND ENVIRONMENTAL TOBACCO SMOKE (ETS)
ETS aggravates asthma in childhood Asthmatic children whose mothers smoke have more severe cases of asthma compared with those whose mothers don’t smoke Prenatal smoking is causally associated with increased prevalence of asthma in children Key Point Environmental tobacco smoke (ETS) aggravates asthma in childhood. Chan-Yeung et al quote the World Health Organization (WHO) as estimating that more than a billion adults are smokers worldwide, and that at least 700 million, almost half of the world’s children, breath air polluted by tobacco smoke at home. Asthmatic children whose mothers smoke have more severe cases of asthma than those who have mothers who don’t smoke. The authors note that increased airways responsiveness at 4.5 weeks of age has been demonstrated in normal infants of smoking parents compared with infants who have nonsmoking parents. The authors also comment that reduced forced expiratory volume in 1 second (FEV1) shortly after birth has been shown in healthy infants born to mothers who smoke. Chan-Yeung et al. Respirology. 2003;8: ; Courtesy of Getty Images. Accessed October 12, 2007. Reference Chan-Yeung M, Dimich-Ward H. Respiratory health effects of exposure to environmental tobacco smoke. Respirology. 2003;8(2): Erratum in: Respirology. 2005;10(4):553.
 aggravates asthma in childhood. Chan-Yeung et al quote the World Health Organization (WHO) as estimating that more than a billion adults are smokers worldwide, and that at least 700 million, almost half of the world’s children, breath air polluted by tobacco smoke at home. Asthmatic children whose mothers smoke have more severe cases of asthma than those who have mothers who don’t smoke. The authors note that increased airways responsiveness at 4.5 weeks of age has been demonstrated in normal infants of smoking parents compared with infants who have nonsmoking parents. The authors also comment that reduced forced expiratory volume in 1 second (FEV1) shortly after birth has been shown in healthy infants born to mothers who smoke. Chan-Yeung et al. Respirology. 2003;8: ; Courtesy of Getty Images. v=1&c=CFW&k=2&d=2EA4B0C59585DB42C1FF2DD0E5B2E618EC7C5022FB410D56. Accessed October 12, Reference. Chan-Yeung M, Dimich-Ward H. Respiratory health effects of exposure to environmental tobacco smoke. Respirology. 2003;8(2): Erratum in: Respirology. 2005;10(4):553.")
50
PRENATAL SMOKING AND ASTHMA IN CHILDREN
Analysis of 60 studies revealed that the risk of asthma in school- aged children is increased if either parent smokes; Odds Ratio (OR)a=1.21 (95% CI, ) Maternal smoking did have a greater effect than paternal smoking, yet the effect of the father only was clearly significant Results suggest postnatal effect is also important Key Point The risk of asthma in school-aged children is increased if either parent smokes. Cook and Strachan performed a meta-analysis on 60 studies to assess the effects of parental smoking on the prevalence of asthma and respiratory symptoms in school-age children. The authors determined that the pooled OR for either parent smoking was 1.21 (95% CI, ) for asthma, 1.24 (95% CI, ) for wheezing, and 1.4 (95% CI, ) for chronic cough. Cook et al also found that although maternal smoking had a greater effect than paternal smoking, the effect of paternal smoking alone was also important, suggesting that the postnatal effect is significant as well. aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Cook et al. Thorax. 1997;52(12): ; Accessed October 12, 2007. Reference Cook DG, Strachan DP. Health effects of passive smoking, 3: parental smoking and prevalence of respiratory symptoms and asthma in school age children. Thorax. 1997;52(12):
a=1.21 (95% CI, ) Maternal smoking did have a greater effect than paternal smoking, yet the effect of the father only was clearly significant. Results suggest postnatal effect is also important. Key Point. The risk of asthma in school-aged children is increased if either parent smokes. Cook and Strachan performed a meta-analysis on 60 studies to assess the effects of parental smoking on the prevalence of asthma and respiratory symptoms in school-age children. The authors determined that the pooled OR for either parent smoking was 1.21 (95% CI, ) for asthma, 1.24 (95% CI, ) for wheezing, and 1.4 (95% CI, ) for chronic cough. Cook et al also found that although maternal smoking had a greater effect than paternal smoking, the effect of paternal smoking alone was also important, suggesting that the postnatal effect is significant as well. aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Cook et al. Thorax. 1997;52(12): ; Accessed October 12, Reference. Cook DG, Strachan DP. Health effects of passive smoking, 3: parental smoking and prevalence of respiratory symptoms and asthma in school age children. Thorax. 1997;52(12):")
51
ASTHMA: EFFECTS OF ENVIRONMENTAL TOBACCO SMOKE IN UTERO OR EARLY CHILDHOOD
Exposure to pre- and postnatal smoking carries a substantial risk for developing adult asthma No exposure to maternal smoking Exposure to maternal smoking Odds Ratio (95% CI)a Key Point Exposure to pre- and postnatal smoking carries a substantial risk for developing adult asthma. Skorge et al evaluated the effects of pre- or postnatal passive smoking on the adult incidence of asthma and respiratory symptoms. An 11-year community cohort study was conducted between 1985 and 1996/1997 in western Norway. The final cohort included 2819 subjects (those who responded to both surveys) aged 15 to 70 years who responded to a mailed questionnaire that consisted of 40 questions about respiratory health, allergies, smoking habits, and occupational exposure. The follow-up survey was conducted between September 1996 and May The questionnaire was expanded to 58 questions and included questions on education and exposure to passive smoking. At follow-up the subjects also were asked the following 3 questions about their parents’ smoking habits: Did your mother smoke when she was pregnant with you? Did your mother smoke when you were a child? Did others in the household smoke when you were a child? Participants reporting smoking exposure in utero had a significantly higher risk for the adult incidence of asthma, even after extensive adjustment for confounders. A similar but weaker trend was seen with exposure to maternal smoking in childhood. With the combined variable, it is apparent that the association between maternal smoking and adult incidence of asthma and respiratory symptoms is strongest with prenatal exposure. Prenatal Postnatal Pre- and Postnatal aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for sex, age, educational level, active smoking in terms of both smoking habits and pack/years, occupational exposure, and hay fever. In addition, when estimating the ORs for the 3 maternal smoking variables, adjustment was made for exposure to smoking from other household members. Skorge et al. Am J Resp Crit Care Med. 2005;172(1):61-66. Reference Skorge TD, Eagan TML, Eide GE, Gulsvik A, Bakke PS. The adult incidence of asthma and respiratory symptoms by passive smoking in utero or in childhood. Am J Respir Crit Care Med. 2005;172(1):61-66.
a. Key Point. Exposure to pre- and postnatal smoking carries a substantial risk for developing adult asthma. Skorge et al evaluated the effects of pre- or postnatal passive smoking on the adult incidence of asthma and respiratory symptoms. An 11-year community cohort study was conducted between 1985 and 1996/1997 in western Norway. The final cohort included 2819 subjects (those who responded to both surveys) aged 15 to 70 years who responded to a mailed questionnaire that consisted of 40 questions about respiratory health, allergies, smoking habits, and occupational exposure. The follow-up survey was conducted between September 1996 and May The questionnaire was expanded to 58 questions and included questions on education and exposure to passive smoking. At follow-up the subjects also were asked the following 3 questions about their parents’ smoking habits: Did your mother smoke when she was pregnant with you Did your mother smoke when you were a child Did others in the household smoke when you were a child Participants reporting smoking exposure in utero had a significantly higher risk for the adult incidence of asthma, even after extensive adjustment for confounders. A similar but weaker trend was seen with exposure to maternal smoking in childhood. With the combined variable, it is apparent that the association between maternal smoking and adult incidence of asthma and respiratory symptoms is strongest with prenatal exposure. Prenatal. Postnatal. Pre- and Postnatal. aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for sex, age, educational level, active smoking in terms of both smoking habits and pack/years, occupational exposure, and hay fever. In addition, when estimating the ORs for the 3 maternal smoking variables, adjustment was made for exposure to smoking from other household members. Skorge et al. Am J Resp Crit Care Med. 2005;172(1): Reference. Skorge TD, Eagan TML, Eide GE, Gulsvik A, Bakke PS. The adult incidence of asthma and respiratory symptoms by passive smoking in utero or in childhood. Am J Respir Crit Care Med. 2005;172(1):")
52
EΠΙΔΡΑΣΕΙΣ ETS ΣΤΟ ΚΑΡΔΙΑΓΓΕΙΑΚΟ
Effects of environmental tobacco smoke risk of heart disease platelet and endothelial function arterial stiffness atherosclerosis oxidative stress inflammation ↓ heart rate variability energy metabolism infarct size Environmental tobacco smoke has multiple deleterious effects on the cardiovascular system, including increased risk of heart disease, diminished platelet and endothelial function and energy metabolism, increased arterial stiffness, oxidative stress and inflammation, and reduced heart rate variability. Environmental tobacco smoke contributes to the progression of atherosclerosis and is associated with increased infarct size in smokers who experience a myocardial infarction. American Heart Association. Scientific Position, Risk Factors and Coronary Heart Disease, Accessed February 2007; Barnoya et al. Circulation. 2005; 111: ; Accessed October 11, 2007. References American Heart Association. Scientific position, risk factors and coronary heart disease, Accessed February 2007. Barnoya J, Glantz SA. Cardiovascular effects of environmental tobacco smoke nearly as large as smoking. Circulation. 2005;111:

53
Environmental Tobacco Smoke Exposure (Hours per Week)
Exposure to environmental tobacco smoke increased the risk of non-fatal acute MI in a graded manner 4 Nonsmokers 2 Odds Ratio (95% CI)a Key Point Exposure to environmental tobacco smoke increased the risk of nonfatal acute (MI) in a graded manner. Teo et al evaluated 12,133 cases of first acute MI and 14,435 age-matched and sex-matched controls in the international, multicenter INTERHEART study. Trained staff administered a questionnaire to both cases and controls in which participants were asked detailed questions about their smoking status. After adjusting for age, sex, region, physical activity, and consumption of fruits, vegetables, and alcohol, nonsmokers who had no previous environmental tobacco smoke exposure showed increasing risk of nonfatal acute MI with increasing levels of exposure to environmental tobacco smoke. Although the etiology is unclear, this increase in risk was slightly attenuated in subjects with 22 hours per week of environmental tobacco smoke exposure. 1 Never 1-7 8-14 15-21 22 0.75 Environmental Tobacco Smoke Exposure (Hours per Week) aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for age, sex, region, physical activity, and consumption of fruits, vegetables, and alcohol. Adapted from Teo et al. Lancet. 2006;368: Reference Teo KK, Ounpuu S, Hawken S, et al, on behalf of the INTERHEART Study Investigators. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. Lancet. 2006;368:
a. Key Point. Exposure to environmental tobacco smoke increased the risk of nonfatal acute (MI) in a graded manner. Teo et al evaluated 12,133 cases of first acute MI and 14,435 age-matched and sex-matched controls in the international, multicenter INTERHEART study. Trained staff administered a questionnaire to both cases and controls in which participants were asked detailed questions about their smoking status. After adjusting for age, sex, region, physical activity, and consumption of fruits, vegetables, and alcohol, nonsmokers who had no previous environmental tobacco smoke exposure showed increasing risk of nonfatal acute MI with increasing levels of exposure to environmental tobacco smoke. Although the etiology is unclear, this increase in risk was slightly attenuated in subjects with 22 hours per week of environmental tobacco smoke exposure. 1. Never Environmental Tobacco Smoke Exposure (Hours per Week) aThe ratio of the odds of development of disease in exposed persons to the odds of development of disease in nonexposed persons. Adjusted for age, sex, region, physical activity, and consumption of fruits, vegetables, and alcohol. Adapted from Teo et al. Lancet. 2006;368: Reference. Teo KK, Ounpuu S, Hawken S, et al, on behalf of the INTERHEART Study Investigators. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. Lancet. 2006;368:")
54
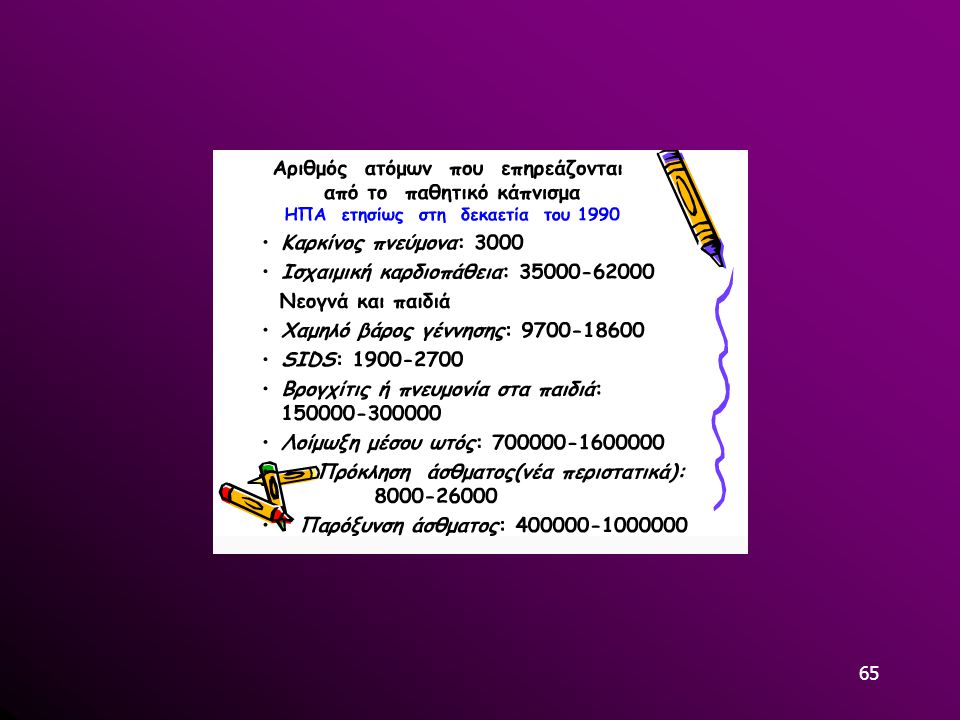
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ-ΝΟΥΜΕΡΑ
Κάθε χρόνο πάνω από (!) μη καπνιστές πεθαίνουν λόγω παθητικού καπνίσματος.
 μη καπνιστές πεθαίνουν λόγω παθητικού καπνίσματος.")
55
600.000 (!) ΘΑΝΑΤΟΙ ΕΤΗΣΙΩΣ ΑΠΌ ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ
Οι θάνατοι από παθητικό κάπνισμα είναι περισσότεροι στις γυναίκες απ’ότι στους άντρες. Περίπου μισοί από αυτούς τους θανάτους (47% ή ) αφορούν γυναίκες. θάνατοι (28%) αφορούν παιδιά μικρότερα από 5 ετών.
 αφορούν γυναίκες θάνατοι (28%) αφορούν παιδιά μικρότερα από 5 ετών.")
56
600.000 (!) ΘΑΝΑΤΟΙ ΕΤΗΣΙΩΣ ΑΠΌ ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ
θάνατοι από ΣΝ. θάνατοι από λοιμώξεις κατώτερου αναπνευστικού. θάνατοι από άσθμα. θάνατοι από καρκίνο πνεύμονος.

57
DALYs (disability-adjusted life years) KAI ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ
σε καπνό. DALYs αφορούν απώλειες λόγω ασθένειας, αναπηρίας ή θάνατο. 61% των DALYS αφορούν παιδιά λόγω λοιμώξεων του κατώτερου αναπνευστικού ( ) και άσθματος ( ).
 και άσθματος ( ).")
58
ΠΑΘΗΤΙΚΟ ΚΑΠΝΙΣΜΑ DALYs

59
ΤΡΙΤΟΓΕΝΕΣ ΚΑΠΝΙΣΜΑ

60
ΣΥΜΠΕΡΑΣΜΑΤΑ Δεν υπάρχει ασφαλές όριο έκθεσης στο παθητικό κάπνισμα.
Το παθητικό κάπνισμα σκοτώνει πάνω από ανθρώπους ετησίως. Παγκοσμίως τα παιδιά εκτείθονται περισσότερο στο παθητικό κάπνισμα από οποιαδήποτε άλλη ηλικιακή ομάδα. Οι θάνατοι και η νοσηρότητα λόγω παθητικού καπνίσματος είναι περισσότεροι στις γυναίκες και τα παιδιά. Οι κυβερνήσεις θα πρέπει να προστατεύσουν τους πολίτες από τους κινδύνους του παθητικού καπνίσματος με τη θέσπιση νόμων απαγόρευσης του καπνίσματος στους χώρους εργασίας και στους δημόσιους χώρους.

61
ΣΥΜΠΕΡΑΣΜΑΤΑ Το παθητικό κάπνισμα βλάπτει σοβαρά την υγεία.
Καθένας πρέπει να εκτίθεται σε παθητικό κάπνισμα μόνο με δική του βούληση.

62
ΝΟΜΟΘΕΣΙΑ

64
Σας ευχαριστώ για την προσοχή σας

66
ETS is risk factor for: lung cancer asthma attacks worsening symptoms of bronchitis recurrent respiratory illnesses ETS can also cause: shortness of breath airway irritation coughing

Παρόμοιες παρουσιάσεις
 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")


















