Κατέβασμα παρουσίασης
1
Η ΣΤΕΦΑΝΙΑΙΑ ΑΘΗΡΟΘΡΟΜΒΩΣΗ: Ο ΣΥΝΕΧΙΖΟΜΕΝΟΣ ΚΑΡΔΙΑΓΓΕΙΑΚΟΣ ΚΙΝΔΥΝΟΣ ΚΑΙ Η ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΟΥ ΜΩΥΣΗΣ ΕΛΙΣΑΦ ΚΑΘΗΓΗΤΗΣ ΠΑΘΟΛΟΓΙΑΣ ΙΑΤΡΙΚΗΣ ΣΧΟΛΗΣ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΙΩΑΝΝΙΝΩΝ

2
Continuous cardiovascular risk in patients who have experienced a prior MI

3
Patients with prior MI have a higher risk of CV mortality compared with controls CV, cardiovascular; MI, myocardial infarction. 1. Norgaard ML et al. Diabetologia 2010;53:1612–1619. Epidemiology study of mortality in patients aged ≥30 years with a first MI over a 10-year period in Denmark (n=3,092,580) [Norgaard 2010] CV mortality (%) Females with incident MI Males with incident MI Reference females Reference males 100 80 60 40 20 0 102345 Time from event (years)
 [Norgaard 2010] CV mortality (%) Females with incident MI Males with incident MI Reference females Reference males Time from event (years).")
4
Despite improvements in survival rates, ~1 in 8 patients will die within 3 years of a STEMI STEMI, ST-segment elevation myocardial infarction. Adapted from: Nauta ST et al. PLoS One 2011;6:e26917. Prospective study of 3-year outcomes in a consecutive series of STEMI patients (n=6820) [Nauta 2011] 0123 Overall log-rank p<0.001 Time from event (years) Cumulative mortality in STEMI patients (%) 1985–19901990–20002000–2008 13% 25% 27% 0 10 20 30 40
 [Nauta 2011] 0123 Overall log-rank p<0.001 Time from event (years) Cumulative mortality in STEMI patients (%) 1985– – – % 25% 27%")
5
NSTEMI, non-ST-segment elevation myocardial infarction. Adapted from: Nauta ST et al. PLoS One 2011;6:e26917. Survival rates post-NSTEMI have not markedly improved – ~1 in 8 patients will die within 3 years of a NSTEMI Prospective study of 3-year outcomes in a consecutive series of NSTEMI patients (n=7614) [Nauta 2011] 0123 Overall log-rank p<0.001 40 0 10 20 30 Cumulative mortality in NSTEMI patients (%) 12% 14% 15% Time from event (years) 1985–19901990–20002000–2008
 [Nauta 2011] 0123 Overall log-rank p< Cumulative mortality in NSTEMI patients (%) 12% 14% 15% Time from event (years) 1985– – –2008.")
6
MI, myocardial infarction; OACIS, Osaka Acute Coronary Insufficiency Study. Nakatani D et al. Circ J 2013;77:439–446. The highest risk of recurrent MI occurs in the initial year post-discharge, but the risk is continuous and linear up to year 5 OACIS registry: Observational study of recurrent MI in Japanese patients with acute MI with up to 5 years of follow-up (n=7870) [Nakatani 2013] 10 0 0 4 400 Time from discharge (days) Cumulative rate of recurrent MI (%) 8 6 2 80012001600 A patient is at the same risk at 1, 2, 3, 4 and 5 years post-discharge
 [Nakatani 2013] Time from discharge (days) Cumulative rate of recurrent MI (%) A patient is at the same risk at 1, 2, 3, 4 and 5 years post-discharge.")
7
~1 in 5 patients, event-free for 1 year post-MI suffered an MI, stroke or CV death within 3 years CV, cardiovascular; MI, myocardial infarction. Jernberg, T. et al. Eur Heart J 2015: doi:10.1093/eurheartj/ehu505 APOLLO HELICON Sweden analysis 1-year event-free MI survivors (n=76,687) [Jernberg 2014] Cumulative 3 year incidence of CV death, MI or stroke (%)
 [Jernberg 2014] Cumulative 3 year incidence of CV death, MI or stroke (%).")
8
Revisiting the pathophysiology of coronary atherothrombosis

9
Stages in the development of atherogenesis Libby P et al. Nature 2011;473(7347):317–325. Platelet Foam cell T cell Dendritic cell Monocyte Thrombus formation Fibrous cap rupture Lipid core Dividing SMC Apoptotic bodies Apoptotic macrophage Migrating SMC Vasa vasorum Cholesterol crystal Foam cell Collagen Mast cell Fibroblast Adventitia Media Intima SMCs Endothelial cell
:317–325. Platelet Foam cell T cell Dendritic cell Monocyte Thrombus formation Fibrous cap rupture Lipid core Dividing SMC Apoptotic bodies Apoptotic macrophage Migrating SMC Vasa vasorum Cholesterol crystal Foam cell Collagen Mast cell Fibroblast Adventitia Media Intima SMCs Endothelial cell.")
10
The role of the platelet in coronary atherothrombosis

11
Platelets may be involved in all stages of atherothrombosis Fuentes QE et al. Platelets 2013;24(4):255–262; Gawaz M. Eur Heart J Suppl 2008:10(Suppl 1);14–17. Initiation and progression Plaque ruptureAcute thrombus formation Platelet adhesion & activation Release of inflammatory mediators, cell recruitment Platelet activation Release of inflammatory mediators, plaque instability Platelet aggregation
:255–262; Gawaz M. Eur Heart J Suppl 2008:10(Suppl 1);14–17. Initiation and progression Plaque ruptureAcute thrombus formation Platelet adhesion & activation Release of inflammatory mediators, cell recruitment Platelet activation Release of inflammatory mediators, plaque instability Platelet aggregation.")
12
The role of the platelet in thrombosis Platelet-activated thrombosis involves three principal steps: [Franchi 2014] -Platelet adhesion -Activation and recruitment of additional platelets -Platelet aggregation 1. Franchi F, Angiolillo DJ. Nat Rev Cardiol 2014; Epub ahead of print Oct 7.
![The role of the platelet in thrombosis Platelet-activated thrombosis involves three principal steps: [Franchi 2014] -Platelet adhesion -Activation and recruitment of additional platelets -Platelet aggregation 1.](http://images.slideplayer.gr/28/9322267/slides/slide_12.jpg "Franchi F, Angiolillo DJ. Nat Rev Cardiol 2014; Epub ahead of print Oct 7..")
13
Potential role of the platelet in inflammation CCR1, chemokine (CC motif) receptor 1; CD40L, soluble CD40L; IL-1 , interleukin-1 ; GPIb , glycoprotein Ib ; JAM-3, junctional adhesion molecule 3; Mac-1, macrophage 1 antigen; PSGL-1, P-selectin glycoprotein ligand 1; RANTES, regulated on activation, normal t cell expressed and secreted; SDF-1, stroma cell-derived factor-1; TLR, toll-like receptor; TP, thromboxane A2 receptor; TXA 2, thromboxane A2. Fuentes QE et al. Platelets 2013;24(4):255–262. Laboratory studies show that activated platelets produce inflammatory molecules that can contribute to all stages of atherosclerosis.
:255–262. Laboratory studies show that activated platelets produce inflammatory molecules that can contribute to all stages of atherosclerosis..")
20
Studies supporting long-term secondary prevention therapy with oral antiplatelet agents

21
ΜΕΛΕΤΗ CAPRIE-ΣΥΜΠΕΡΑΣΜΑΤΑ Clopidogrel vs aspirin σε ασθενείς με Ηχ ΟΕΜ, ΑΕΕ, περιφερικής αγγειοπάθειας Clopidogrel > aspirin κυρίως σε ασθενείς με περιφερική αγγειοπάθεια Σε μετεμφραγματικούς ασθενείς: clopidogrel >aspirin Παρόμοια επίπτωση αιμορραγιών-λιγότερες ΓΕΣ αιμορραγίες με κλοπιδογρέλη

22
CHARISMA: Study design Clopidogrel 75 mg QD (n=7802) Placebo 1 tablet QD (n=7801) 1-month visit Final visit (fixed study end date) Patients aged ≥45 years at high risk of atherothrombotic events R Double-blind treatment until a total of 1040 CV death, MI or stroke events recorded Low-dose ASA 75 162 mg/day (n=15,603) Ongoing visits every 6 months 3-month visit ASA, acetylsalicylic acid; CV, cardiovascular; MI, myocardial infarction; QD, once daily; R, randomisation. Bhatt DL, Topol EJ. Am Heart J 2004;148:263–268; Bhatt DL, et al. N Engl J Med 2006;354:1706–1717. 6-month visit

23
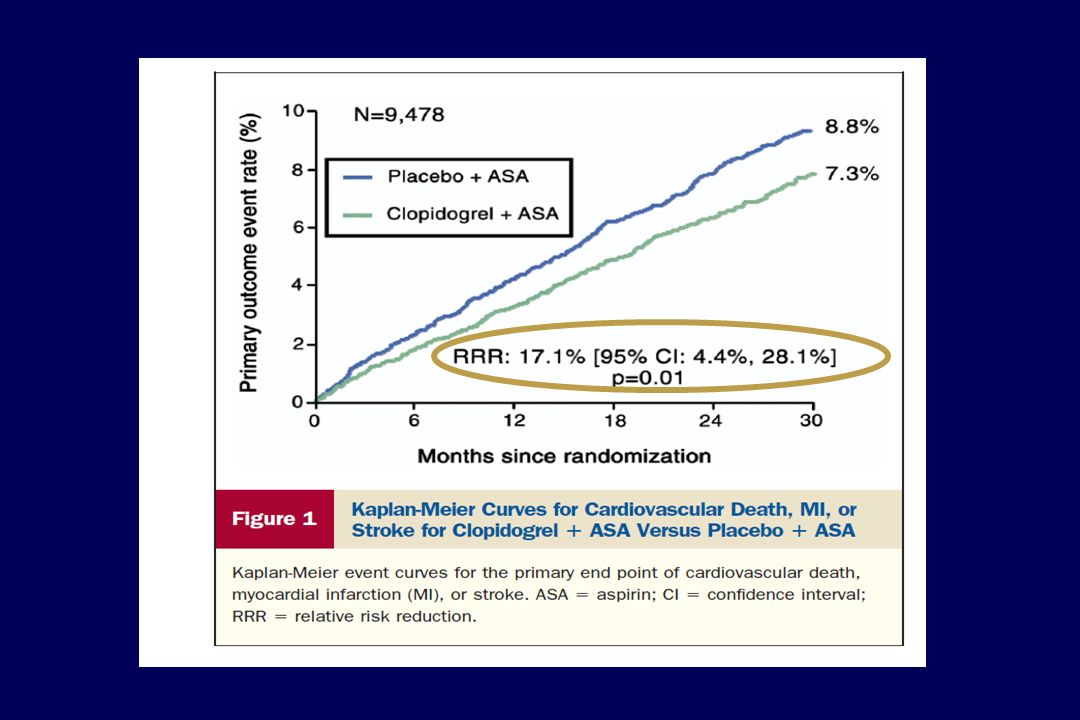
CHARISMA: Cumulative incidence of CV death, MI or stroke (primary endpoint) ASA, acetylsalicylic acid; CI, confidence interval; CV, cardiovascular; MI, myocardial infarction; RR, relative risk. Bhatt DL, et al. N Engl J Med 2006;354:1706–1717. 7.3% 6.8% No. at risk Clopidogrel Placebo 7802 7801 7653 7644 7510 7482 7363 7316 5299 5212 2770 2753 RR=0.93 (95% CI: 0.83–1.05); p=0.22 Placebo + ASA Clopidogrel + ASA
; p=0.22 Placebo + ASA Clopidogrel + ASA.")
26
ΜΕΛΕΤΗ CHARISMA-ΣΥΜΠΕΡΑΣΜΑΤΑ Διπλή αντιαιμοπεταλιακή αγωγή vs μονοθεραπεία: όχι διαφορά σε θανάτους/ΟΕΜ/ΑΕΕ Όμως σε άτομα με εγκατεστημένη αγγειακή νόσο: συμβαμάτων κατά 17%, p=0.001 αιμορραγιών, όχι όμως των σοβαρών αιμορραγικών επιπλοκών

27
Clopidogrel ή Prasugrel

28
Cumulative Incidence of Stent Thrombosis Mauri L, et al. N Engl J Med. Nov 16, 2014. DOI: 10.1056/NEJMe1413297.. 100 80 60 40 20 0 012182124273033 Months Since Enrollment Cumulative Incidence (%) 8 6 4 2 0 012182430212733 15 12–30 mo: Thienopyridine vs. placebo, 0.4% vs. 1.4%; hazard ratio, 0.29; P <0.001 12–33 mo: Thienopyridine vs. placebo, 0.7% vs. 1.4%; hazard ratio, 0.45; P <0.001 4934487048284765468646423110 Thienopyridine 4845477547214651460345563105 Placebo No. at Risk 5020 4941 Thienopyridine Placebo
 –30 mo: Thienopyridine vs. placebo, 0.4% vs. 1.4%; hazard ratio, 0.29; P < –33 mo: Thienopyridine vs. placebo, 0.7% vs. 1.4%; hazard ratio, 0.45; P < Thienopyridine Placebo No. at Risk Thienopyridine Placebo.")
29
Cumulative Incidence of MACCE Mauri L, et al. N Engl J Med. Nov 16, 2014. DOI: 10.1056/NEJMe1413297.. 100 80 60 40 20 0 012182124273033 Months Since Enrollment 50204917484047784702461145543029 Thienopyridine 49414799471546354542447644122997 Placebo No. at Risk Cumulative Incidence (%) 8 6 4 2 0 012182430212733 15 12–30 mo: Thienopyridine vs. placebo, 4.3% vs. 5.9%; hazard ratio, 0.71; P <0.001 12–33 mo: Thienopyridine vs. placebo, 5.6% vs. 6.5%; hazard ratio, 0.82; P <0.02 Thienopyridine Placebo
 –30 mo: Thienopyridine vs. placebo, 4.3% vs. 5.9%; hazard ratio, 0.71; P < –33 mo: Thienopyridine vs. placebo, 5.6% vs. 6.5%; hazard ratio, 0.82; P <0.02 Thienopyridine Placebo.")
30
All-Cause Mortality Mauri L, et al. N Engl J Med. Nov 16, 2014. DOI: 10.1056/NEJMe1413297.. HR 1.36; P = 0.05 HR 1.36; P = 0.04 The rate of death from noncardiovascular causes (1.1% vs. 0.6%; hazard ratio, 1.80; P = 0.01) accounting for the difference in rates between the two analysis period
 accounting for the difference in rates between the two analysis period.")
31
DUAL ANTIPLATELET THERAPY (DAT) vs PLACEBO (>12months) PLACEBOR.R.DAT Stent thrombosis1.4%0.290.4% Μείζονα συμβάματα 5.9%0.714.3% ΟΕΜ4.1%0.472.1% Θάνατοι1.5%1.362% Αιμορραγίες1.6% 1.562.5% N Engl J Med 2014;371: 2155-2166
 vs PLACEBO (>12months) PLACEBOR.R.DAT Stent thrombosis1.4% % Μείζονα συμβάματα 5.9% % ΟΕΜ4.1% % Θάνατοι1.5%1.362% Αιμορραγίες1.6% % N Engl J Med 2014;371:")
33
κινδύνου εμφάνισης αιμορραγιών κατά 61% Ενδοκράνιες αιμορραγίες 0.6% vs 0.4 % -20%

34
Ορισμένα άτομα με στεφανιαία νόσο πολύ υψηλού κινδύνου με Ηχ ρήξης αθηρωματικών πλακών και θρόμβωση πιθανά ωφελούνται από παρατεταμένη διπλή αντιαιμοπεταλιακή αγωγή

35
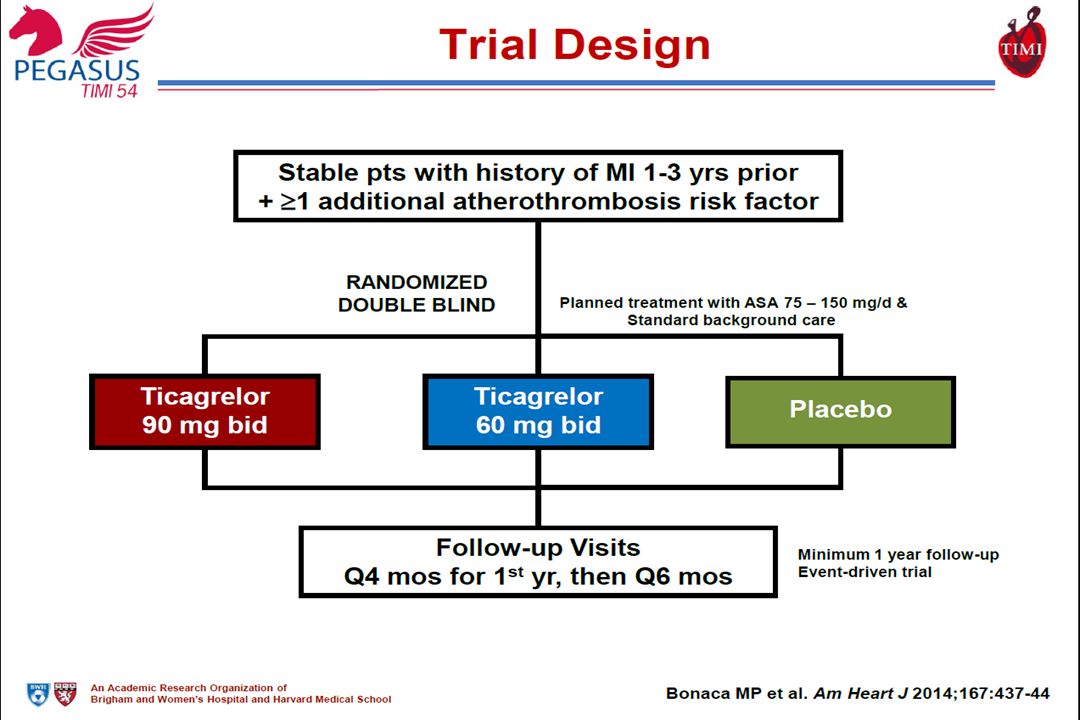
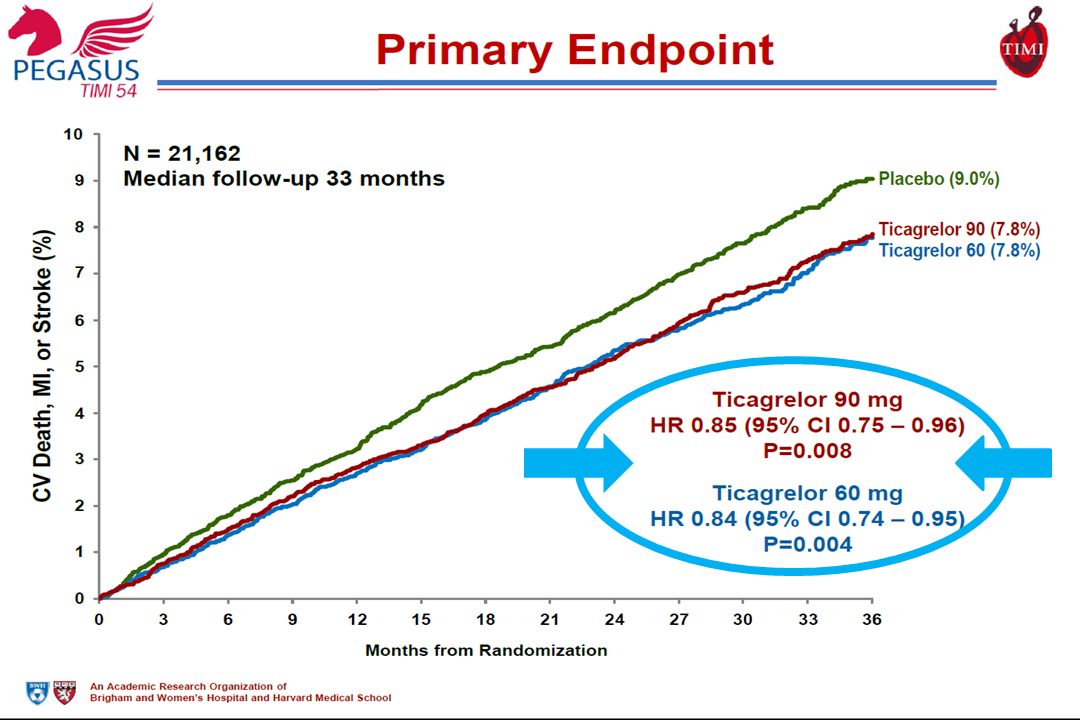
PEGASUS-TIMI 54 A randomised, double-blind, placebo-controlled, parallel-group, multinational trial, to assess the prevention of thrombotic events with ticagrelor compared with placebo on a background of acetylsalicylic acid therapy in patients with a history of myocardial infarction

36
ΧΑΡΑΚΤΗΡΙΣΤΙΚΑ ΤΗΣ TICAGRELOR (1) Αναστολέας του υποδοχέα P2Υ12 Προκαλεί αντιστρεπτή και εκλεκτική αναστολή Διακοπή (offset) της δράσης σε 3-5 ημέρες Δεν είναι προφάρμακο-χορηγείται ανεξάρτητα από την τροφή Έχει γρηγορότερη έναρξη δράσης (vs clopidogrel) – έναρξη δράσης 30’-4h Δοσολογία: φόρτιση 180mg/d / δόση συντήρησης 90mg X 2/d Χρόνος ημίσειας ζωής 8-12h Μεταβολίζεται σε ενεργό μεταβολίτη με τα CYP3A4, CYP3A5 Απεκκρίνεται κυρίως διαμέσου ηπατικού μεταβολισμού
 Αναστολέας του υποδοχέα P2Υ12 Προκαλεί αντιστρεπτή και εκλεκτική αναστολή Διακοπή (offset) της δράσης σε 3-5 ημέρες Δεν είναι προφάρμακο-χορηγείται ανεξάρτητα από την τροφή Έχει γρηγορότερη έναρξη δράσης (vs clopidogrel) – έναρξη δράσης 30’-4h Δοσολογία: φόρτιση 180mg/d / δόση συντήρησης 90mg X 2/d Χρόνος ημίσειας ζωής 8-12h Μεταβολίζεται σε ενεργό μεταβολίτη με τα CYP3A4, CYP3A5 Απεκκρίνεται κυρίως διαμέσου ηπατικού μεταβολισμού")
37
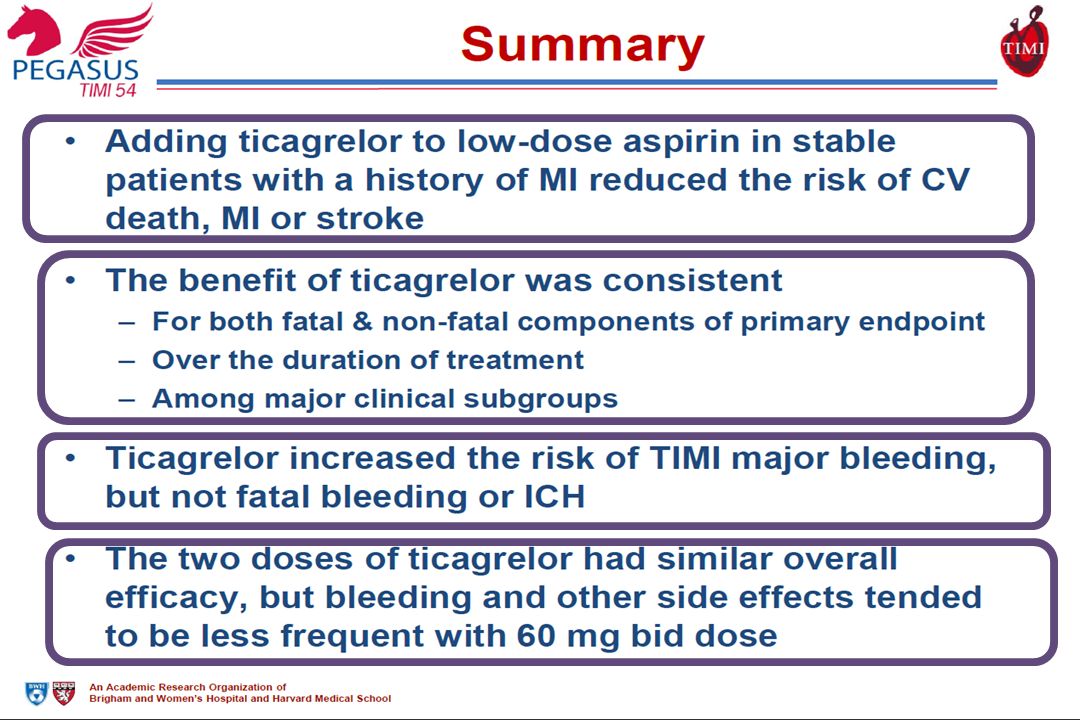
ΧΑΡΑΚΤΗΡΙΣΤΙΚΑ ΤΗΣ TICAGRELOR (2) Μειώνει τα καρδιαγγειακά συμβάματα και την ολική θνητότητα σε σύγκριση με clopidogrel Δεν αυξάνει τις μείζονες αιμορραγίες-αύξηση αιμορραγικών επιπλοκών Έχει και επιπρόσθετες δράσεις ( ΑΔΕΝΟΣΙΝΗΣ) στεφανιαία αγγειοδιαστολή μείωση ισχαιμικών βλαβών και βλαβών επαναγγείωσης αντιφλεγμονώδης δράση αρνητική ινότροπη και χρονότρoπη δράση GFR-διέγερση των πνευμονικών ινών C του πνευμονογαστρικού δύσπνοια
 Μειώνει τα καρδιαγγειακά συμβάματα και την ολική θνητότητα σε σύγκριση με clopidogrel Δεν αυξάνει τις μείζονες αιμορραγίες-αύξηση αιμορραγικών επιπλοκών Έχει και επιπρόσθετες δράσεις ( ΑΔΕΝΟΣΙΝΗΣ) στεφανιαία αγγειοδιαστολή μείωση ισχαιμικών βλαβών και βλαβών επαναγγείωσης αντιφλεγμονώδης δράση αρνητική ινότροπη και χρονότρoπη δράση GFR-διέγερση των πνευμονικών ινών C του πνευμονογαστρικού δύσπνοια")
38
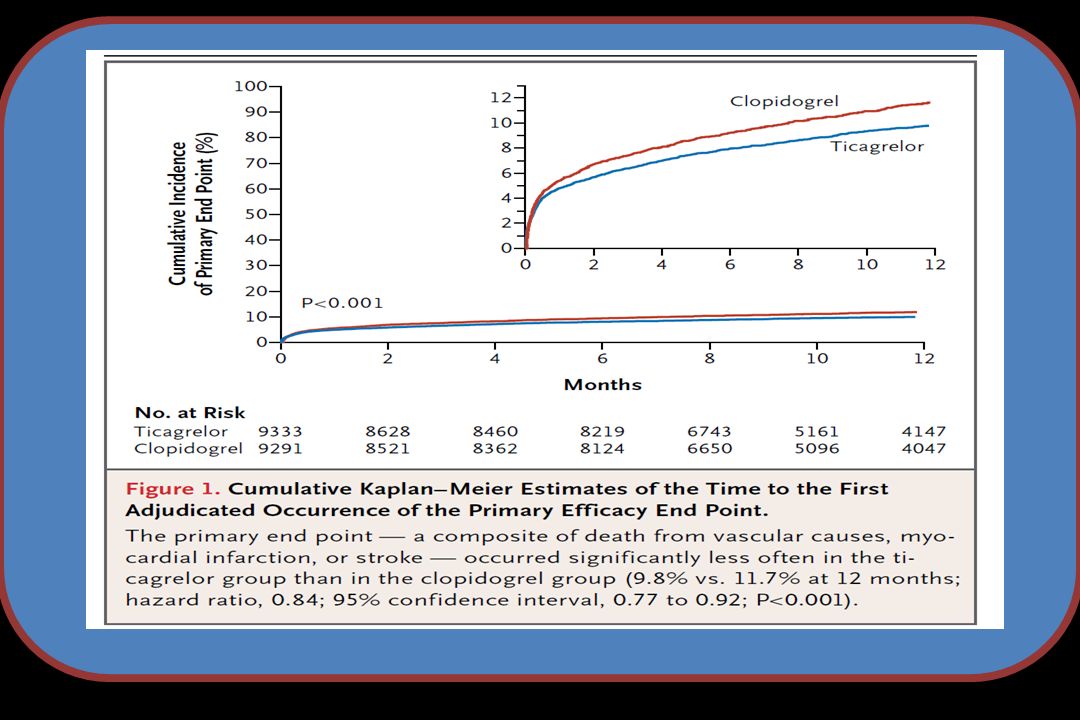
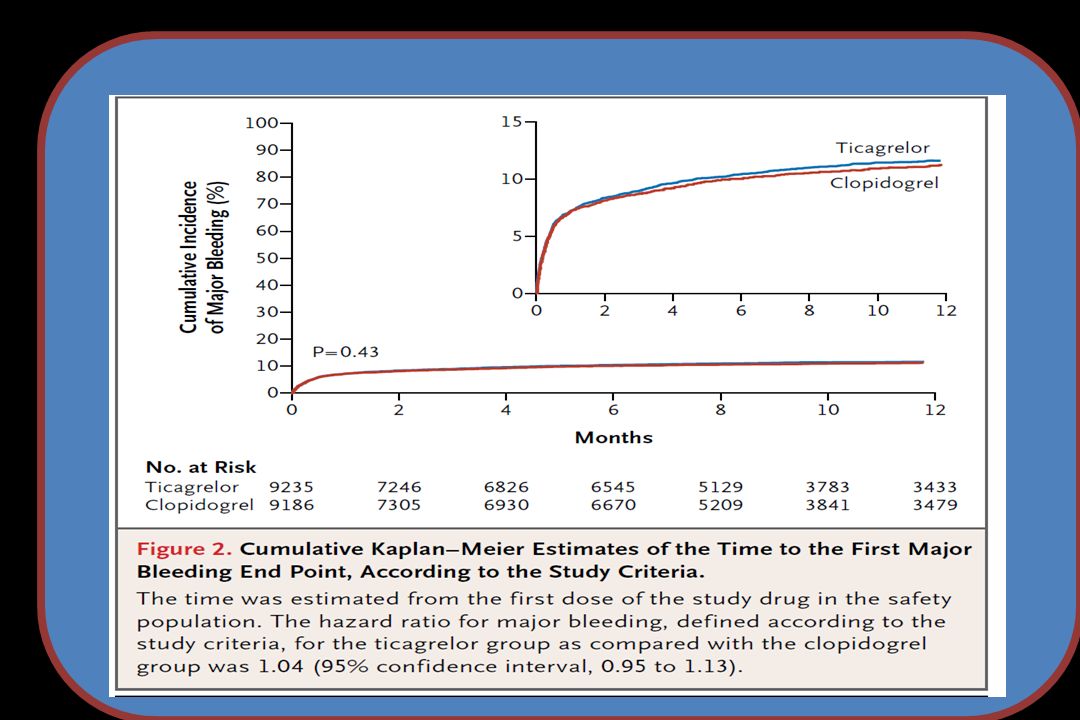
PLATO: TICAGRELOR vs CLOPIDOGREL (acute coronary syndromes) OEM, AEE, θανάτων κατά 16%, p=0.003 καρδιαγγειακής θνητότητας κατά 21%, p=0.001 θρομβώσεων των stent κατά 33% Όχι μειζόνων ή θανατηφόρων αιμορραγιών όλων των αιμορραγικών επιπλοκών κατά 11%, p=0.008-ενδοκράνιες αιμορραγίες 0.3% vs 0.2% Δύσπνοια (διακοπή στο 1%)
 OEM, AEE, θανάτων κατά 16%, p=0.003 καρδιαγγειακής θνητότητας κατά 21%, p=0.001 θρομβώσεων των stent κατά 33% Όχι μειζόνων ή θανατηφόρων αιμορραγιών όλων των αιμορραγικών επιπλοκών κατά 11%, p=0.008-ενδοκράνιες αιμορραγίες 0.3% vs 0.2% Δύσπνοια (διακοπή στο 1%)")
41
60mg/d: θεραπεία 10.000 ασθενών για ένα έτος 42 λιγότερα συμβάματα και 31 περισσότερες αιμορραγίες

44
BALANCING THE RISKS AND BENEFITS OF DUAL PLATELET INHIBITORS συμβαμάτων- αιμορραγικών επιπλοκών Ανάγκη εξατομίκευσης της αγωγής Ερωτήματα: Ποιο φάρμακο? Διάρκεια αγωγής?

50
ΑΛΛΗΛΕΠΙΔΡΑΣΕΙΣ ΤΗΣ TICAGRELOR ΜΕ ΑΛΛΑ ΦΑΡΜΑΚΑ Όχι με ισχυρούς αναστολείς του CYP3A4/CYP3A5 [ketoconazole, clarithromycin, nefazodone, zitonavir, atazanavir]* Επαγωγείς της CYP3A4 (ριφαμπικίνη) δράσης TICAGRELOR Αναστέλλει το P4503A4 SIMVA, LOVA SIMVA<40mg/d Grapefruit* επιπέδων ticagrelor Υπόστρωμα και ασθενής αναστολέας της Pgp προσοχή με δακτυλίτιδα * ΠΡΟΣΟΧΗ ΜΕ ΜΕΤΡΙΟΥΣ ΑΝΑΣΤΟΛΕΙΣ ΤΟΥ P4503A4 [diltiazem, verapamil, fluconazole, erythromycin]
![ΑΛΛΗΛΕΠΙΔΡΑΣΕΙΣ ΤΗΣ TICAGRELOR ΜΕ ΑΛΛΑ ΦΑΡΜΑΚΑ Όχι με ισχυρούς αναστολείς του CYP3A4/CYP3A5 [ketoconazole, clarithromycin, nefazodone, zitonavir, atazanavir]* Επαγωγείς της CYP3A4 (ριφαμπικίνη) δράσης TICAGRELOR Αναστέλλει το P4503A4 SIMVA, LOVA SIMVA<40mg/d Grapefruit* επιπέδων ticagrelor Υπόστρωμα και ασθενής αναστολέας της Pgp προσοχή με δακτυλίτιδα * ΠΡΟΣΟΧΗ ΜΕ ΜΕΤΡΙΟΥΣ ΑΝΑΣΤΟΛΕΙΣ ΤΟΥ P4503A4 [diltiazem, verapamil, fluconazole, erythromycin]](http://images.slideplayer.gr/28/9322267/slides/slide_50.jpg "ΑΛΛΗΛΕΠΙΔΡΑΣΕΙΣ ΤΗΣ TICAGRELOR ΜΕ ΑΛΛΑ ΦΑΡΜΑΚΑ Όχι με ισχυρούς αναστολείς του CYP3A4/CYP3A5 [ketoconazole, clarithromycin, nefazodone, zitonavir, atazanavir]* Επαγωγείς της CYP3A4 (ριφαμπικίνη) δράσης TICAGRELOR Αναστέλλει το P4503A4 SIMVA, LOVA SIMVA<40mg/d Grapefruit* επιπέδων ticagrelor Υπόστρωμα και ασθενής αναστολέας της Pgp προσοχή με δακτυλίτιδα * ΠΡΟΣΟΧΗ ΜΕ ΜΕΤΡΙΟΥΣ ΑΝΑΣΤΟΛΕΙΣ ΤΟΥ P4503A4 [diltiazem, verapamil, fluconazole, erythromycin]")
51
ΑΝΕΠΙΘΥΜΗΤΕΣ ΕΝΕΡΓΕΙΕΣ Δύσπνοια Κοιλιακές --- UA, Pcr (πέραν των αιμορραγικών επιπλοκών)
")
52
TICAGRELOR Limitations of clopidogrel Characteristics of ticagrelor Clinical data Clinical practice

53
CAPRIE: Risk of CV death, MI or ischaemic stroke (primary endpoint) ASA, acetylsalicylic acid; CI, confidence interval; CV, cardiovascular; MI, myocardial infarction; RRR, relative risk reduction. CAPRIE steering committee. Lancet 1996;348:1329–1339. No. at risk ASA Clopidogrel 9586 9599 9190 9247 8087 8131 6139 6160 3979 4053 2143 2170 542 539 RRR=8.7% (95% CI: 0.3–16.5); p=0.043 ASA Clopidogrel
; p=0.043 ASA Clopidogrel.")
54
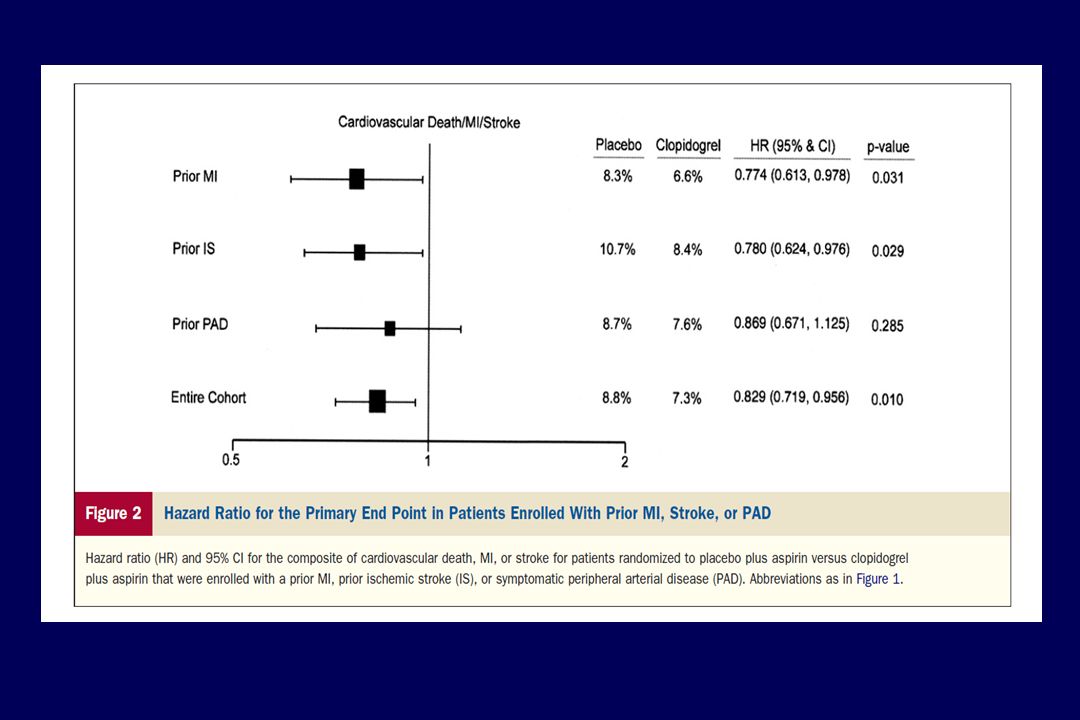
CAPRIE history of MI subgroup analysis: Risk of CV death, MI or ischaemic stroke SubgroupEvent rate, % per yearRRR (95% CI) MI qualifying event (n=6302) Clopidogrel (patient-years=5787) ASA (patient-years=5843) 5.03 4.84 –3.7% (–22.1–12.0) Ischaemic stroke/PAD qualifying event and prior MI (n=2144) Clopidogrel (patient-years=1963) ASA (patient-years=1825) 8.35 10.74 22.7% (4.9–37.2) Any prior MI (n=8446) Clopidogrel (patient-years=7751) ASA (patient-years=7668) 5.87 6.25 7.4% (–5.2–18.6) ASA, acetylsalicylic acid; CI, confidence interval; CV, cardiovascular; MI, myocardial infarction; PAD, peripheral artery disease; RRR, relative risk reduction. CAPRIE steering committee. Lancet 1996;348:1329–1339.

55
CAPRIE subgroup analyses: RRR by qualifying event ASA, acetylsalicylic acid; CI, confidence interval; MI, myocardial infarction; PAD, peripheral artery disease; RRR, relative risk reduction. CAPRIE steering committee. Lancet 1996;348:1329–1339. Stroke PAD MI All patients ASA better Clopidogrel better RRR, % (95% CI) –40–30–20–10010203040
 –40–30–20–")
56
CHARISMA A prospective, multicentre, randomised, double-blind, placebo- controlled study of the efficacy and safety of clopidogrel plus acetylsalicylic acid as compared with acetylsalicylic acid alone in patients at high risk for a cardiovascular event

57
CHARISMA: Cumulative incidence of CV death, MI, stroke or hospitalisation (secondary endpoint) ASA, acetylsalicylic acid; CI, confidence interval; CV, cardiovascular; MI, myocardial infarction; RR, relative risk. Bhatt DL, et al. N Engl J Med 2006;354:1706–1717. No. at risk Clopidogrel Placebo 7802 7801 7401 7371 7104 7029 6802 6705 4774 4640 2450 2374 17.9% 16.7% Cumulative incidence (%) Months since randomisation Placebo + ASA Clopidogrel + ASA RR=0.92 (95% CI: 0.86–0.995); p=0.04 20 15 10 5 0 0612182430
 Months since randomisation Placebo + ASA Clopidogrel + ASA RR=0.92 (95% CI: 0.86–0.995); p=")
58
CHARISMA: Primary and secondary safety endpoints ASA, acetylsalicylic acid; ICH, intracranial haemorrhage. Bhatt DL, et al. N Engl J Med 2006;354:1706–1717. p=0.09 p=0.17 p=0.89 p<0.001

62
12 vs. 30 months of DAPT-Thienopyridines in patients with a PCI Not eligible for Randomization If Death, MI, Repeat Revascularization, Stent Thrombosis, CABG, Stroke, GUSTO moderate or severe bleed, Non compliance with thienopyridine (interruptions >14 days), switched thienopyridine type or dose within 6 months before randomization. DAPT Study design Primary analysis powered for DES treated subjects : compare 12 versus 30 months of DAPT with thienopyridines among patients with PCI with DES 2 co-primary endpoints : stent thrombosis and MACCE (death, myocardial infarction or stroke) Secondary analysis : compare MACCE and ST in subjects treated with BMS vs. DES (non-inferiority) Major Bleeding outcome : Non inferiority of 30 vs. 12 months of DAPT with respect to the incidence of GUSTO moderate or severe bleeding (non-inferiority) Eligible for Enrolment PCI with DES (n=22,866) or BMS (n=2816) Eligible for Enrolment PCI with DES (n=22,866) or BMS (n=2816) Randomization Patients who are “event free” N=9961 Randomization Patients who are “event free” N=9961 12 month Observation Period All subjects on aspirin + open label thienopyridine treatment 18 month Treatment Period Study drug discontinued, all subject on ASA alone 65% Clopidogrel / 35% Prasugrel 65% Clopidogrel / 35% Prasugrel Mauri L, et al. N Engl J Med. Nov 16, 2014. DOI: 10.1056/NEJMe1413297.. Clinical follow-up at 33 mo n=4658 (94.3%) Clinical follow-up at 33 mo n=4658 (94.3%) Clinical follow-up at 33 mo n=4732 (94.3%) Clinical follow-up at 33 mo n=4732 (94.3%) Clinical follow-up at 30 mo n=4715 (95.4%) Clinical follow-up at 30 mo n=4715 (95.4%) Clinical follow-up at 30 mo n=4783 (95.3%) Clinical follow-up at 30 mo n=4783 (95.3%) Aspirin + Placebo “12 month DAPT arm” n=4941 Aspirin + Placebo “12 month DAPT arm” n=4941 Aspirin + thienopyridines “30 month DAPT arm” n=5020 Aspirin + thienopyridines “30 month DAPT arm” n=5020
, switched thienopyridine type or dose within 6 months before randomization. DAPT Study design Primary analysis powered for DES treated subjects : compare 12 versus 30 months of DAPT with thienopyridines among patients with PCI with DES 2 co-primary endpoints : stent thrombosis and MACCE (death, myocardial infarction or stroke) Secondary analysis : compare MACCE and ST in subjects treated with BMS vs. DES (non-inferiority) Major Bleeding outcome : Non inferiority of 30 vs. 12 months of DAPT with respect to the incidence of GUSTO moderate or severe bleeding (non-inferiority) Eligible for Enrolment PCI with DES (n=22,866) or BMS (n=2816) Eligible for Enrolment PCI with DES (n=22,866) or BMS (n=2816) Randomization Patients who are event free N=9961 Randomization Patients who are event free N= month Observation Period All subjects on aspirin + open label thienopyridine treatment 18 month Treatment Period Study drug discontinued, all subject on ASA alone 65% Clopidogrel / 35% Prasugrel 65% Clopidogrel / 35% Prasugrel Mauri L, et al. N Engl J Med. Nov 16, DOI: /NEJMe Clinical follow-up at 33 mo n=4658 (94.3%) Clinical follow-up at 33 mo n=4658 (94.3%) Clinical follow-up at 33 mo n=4732 (94.3%) Clinical follow-up at 33 mo n=4732 (94.3%) Clinical follow-up at 30 mo n=4715 (95.4%) Clinical follow-up at 30 mo n=4715 (95.4%) Clinical follow-up at 30 mo n=4783 (95.3%) Clinical follow-up at 30 mo n=4783 (95.3%) Aspirin + Placebo 12 month DAPT arm n=4941 Aspirin + Placebo 12 month DAPT arm n=4941 Aspirin + thienopyridines 30 month DAPT arm n=5020 Aspirin + thienopyridines 30 month DAPT arm n=5020.")
63
Cumulative Incidence of Myocardial Infarction Mauri L, et al. N Engl J Med. Nov 16, 2014. DOI: 10.1056/NEJMe1413297. Appendix. 100 80 60 40 20 0 1215182124273033 Months Since Enrollment 50204920484947894717463445803051 Thienopyridine 49414804472746534565450144403012 Placebo No. at Risk Cumulative Incidence (%) Primary Analysis Period 12-30 Months: Hazard Ratio 0.47 (0.37-0.61) 2.1% vs 4.1% P<0.001 12-33 Months: Hazard Ratio 0.61 (0.49-0.76) 3.0% vs 4.5% P<0.001 10 6 8 4 2 0 1215182430212733 Myocardial Infarction Thienopyridine Placebo
 Primary Analysis Period Months: Hazard Ratio 0.47 ( ) 2.1% vs 4.1% P< Months: Hazard Ratio 0.61 ( ) 3.0% vs 4.5% P< Myocardial Infarction Thienopyridine Placebo.")
64
PEGASUS-TIMI 54: Study design Stable CAD patients with prior MI 1–3 years ago AND at least one additional atherothrombosis risk factor* (n=21,000) Ticagrelor 60 mg BID + ASA 75–150 mg/day Minimum of 12 months follow up: Every 4 months in Year 1, then semi-annually Primary efficacy endpoint: CV death, MI or stroke Primary safety endpoint: TIMI-defined major bleeding Placebo + ASA 75–150 mg/day Ticagrelor 90 mg BID + ASA 75–150 mg/day *Age ≥65 years, diabetes, second prior MI, multivessel CAD or chronic non-end stage renal disease. ASA, acetylsalicylic acid; BID, twice daily; CAD, coronary artery disease; CV, cardiovascular; MI, myocardial infarction; TIMI, Thrombolysis in Myocardial Infarction. Bonaca MP, et al. Am Heart J 2014;167:437–444.






















 : ΑΝΟΙΧΤΩΝ Vs ΚΛΕΙΣΤΩΝ ΚΥΨΕΛΩΝ>")


. ΣΥΓΚΟΠΤΙΚΗ ΚΡΙΣΗ Αιφνίδια και σύντομη απώλεια συνείδησης που προκαλείται από ανεπαρκή εγκεφαλική αιμάτωση λόγω μειωμένης.>")
