Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Ανατομία dsfsf dsfsf Γόνατο dsfsf Ελευθερία Θωμαΐδου, Pt

2
Μαθησιακά Αποτελέσματα
Στο τέλος του μαθήματος και έπειτα από την ατομική σας μελέτη πρέπει να είστε σε θέση να : Αναγνωρίζετε τα οστικά σημεία στην περιοχή της άρθρωσης Κατανοήσετε τις κινήσεις του γόνατος Εντοπίζεται τους συνδέσμους Αναγνωρίζετε τις προσφύσεις των μυών που δρούν στο γόνατο

3
Άρθρωση του Γόνατος Η άρθρωση του γόνατος είναι η μεγαλύτερη διάρθρωση του σώματος. Αποτελείται από : Την άρθρωση μεταξύ μηριαίου- κνήμης Την άρθρωση μεταξύ επιγονατίδας - μηριαίου

4
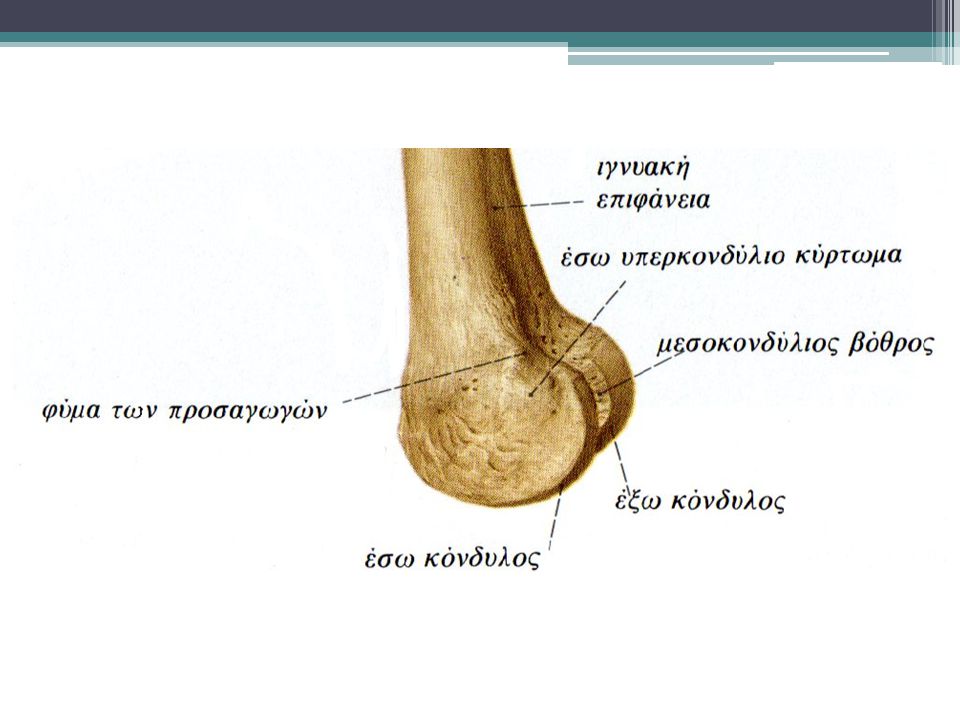
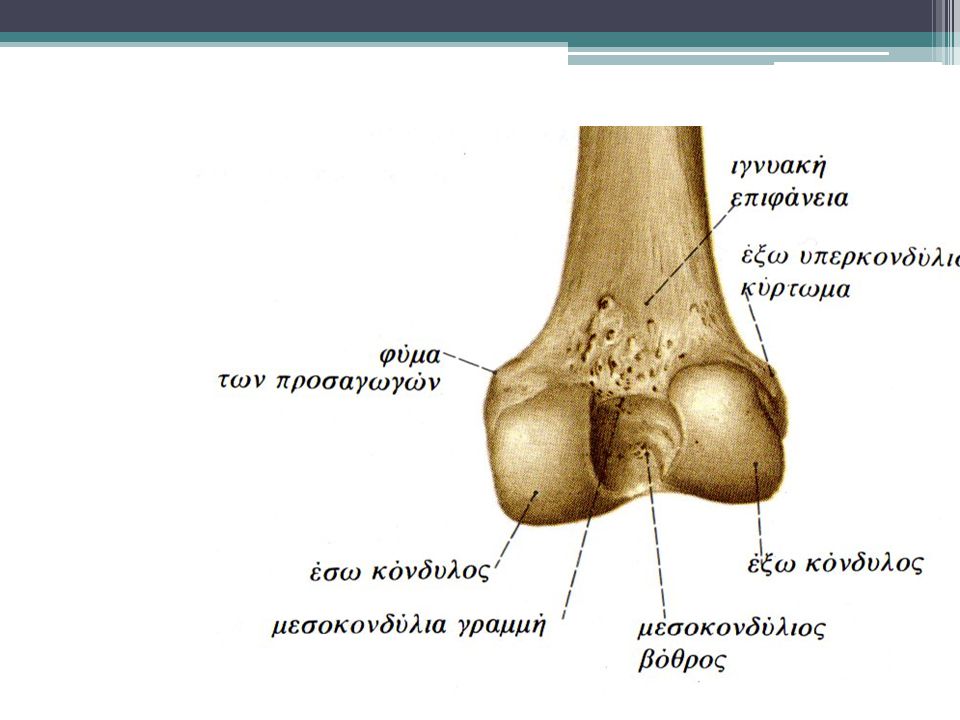
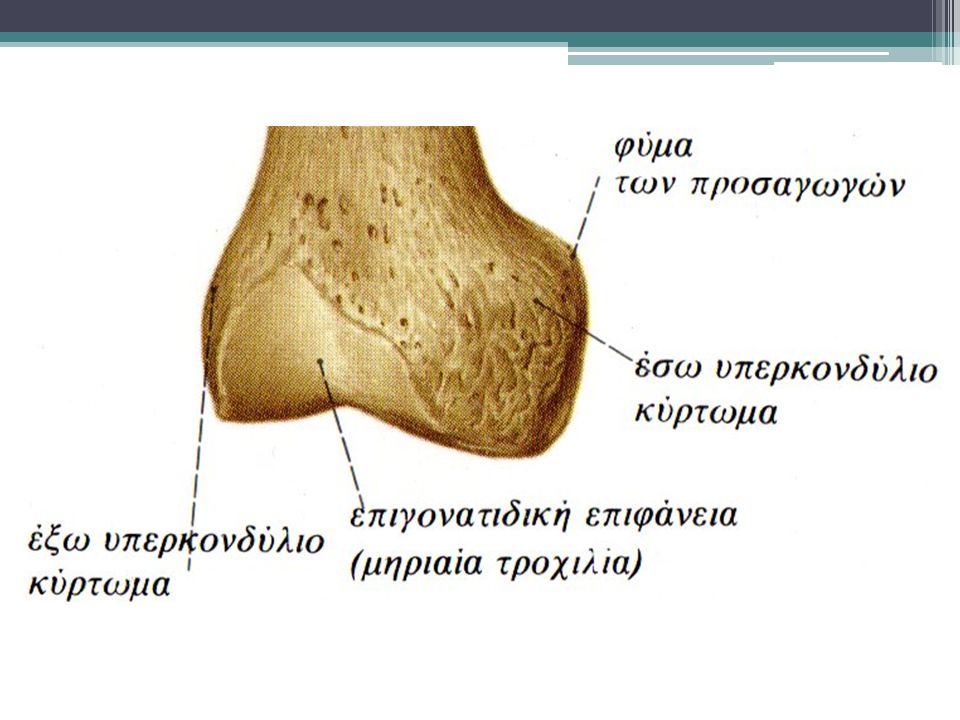
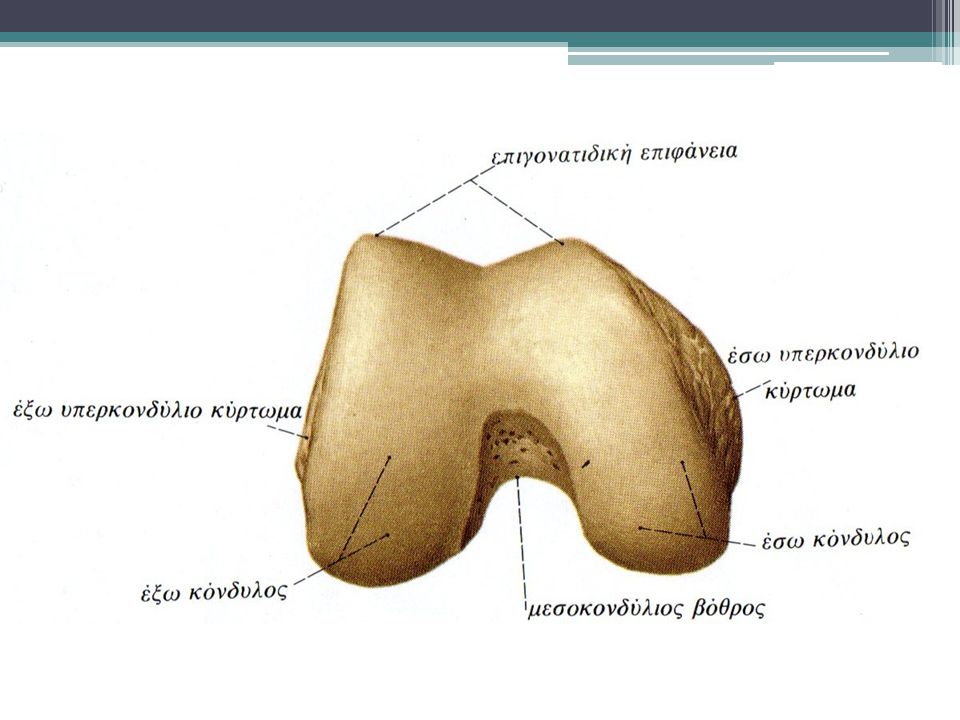
Μηριαίο οστό Οι δύο μηριαίοι κόνδυλοι ( έσω και έξω) ενώνονται προς τα μπρός σε μία κοινή επιφάνεια τη μηριαία τροχιλία. Στην πίσω επιφάνεια αποκλίνουν και σχηματίζεται η μεσοκονδύλια εντομή ή βόθρος Πλάγια των κονδύλων υπάρχουν τα δύο υπερκονδύλια κυρτώματα( ή αλλιώς έσω και έξω επικόνδυλοι) Πάνω από τον έσω επικόνδυλο υπάρχει το φύμα των προσαγωγών
 ενώνονται προς τα μπρός σε μία κοινή επιφάνεια τη μηριαία τροχιλία. Στην πίσω επιφάνεια αποκλίνουν και σχηματίζεται η μεσοκονδύλια εντομή ή βόθρος Πλάγια των κονδύλων υπάρχουν τα δύο υπερκονδύλια κυρτώματα( ή αλλιώς έσω και έξω επικόνδυλοι) Πάνω από τον έσω επικόνδυλο υπάρχει το φύμα των προσαγωγών")
9
Επιγονατίδα Η επιγονατίδα έχει τριγωνικό σχήμα
Η επιγονατίδα παρεμβάλλεται στον τένοντα του 4φάλου Η κορυφή το οστού είναι προς τα κάτω(πρόσφυση επιγονατιδικού συνδέσμου) Η βάση είναι προς τα πάνω(κατάφυση 4φάλου μυός) Η έσω επιφάνεια χωρίζεται σε δύο πλάγια τμήματα με μια μέση κάθετο ακρολοφία ( αρθρώνεται με το μηριαίο) Στα πλάγια χείλη της προσφύονται σύνδεσμοι και μοίρες του 4φαλου μυός.
 Η βάση είναι προς τα πάνω(κατάφυση 4φάλου μυός) Η έσω επιφάνεια χωρίζεται σε δύο πλάγια τμήματα με μια μέση κάθετο ακρολοφία ( αρθρώνεται με το μηριαίο) Στα πλάγια χείλη της προσφύονται σύνδεσμοι και μοίρες του 4φαλου μυός.")
10
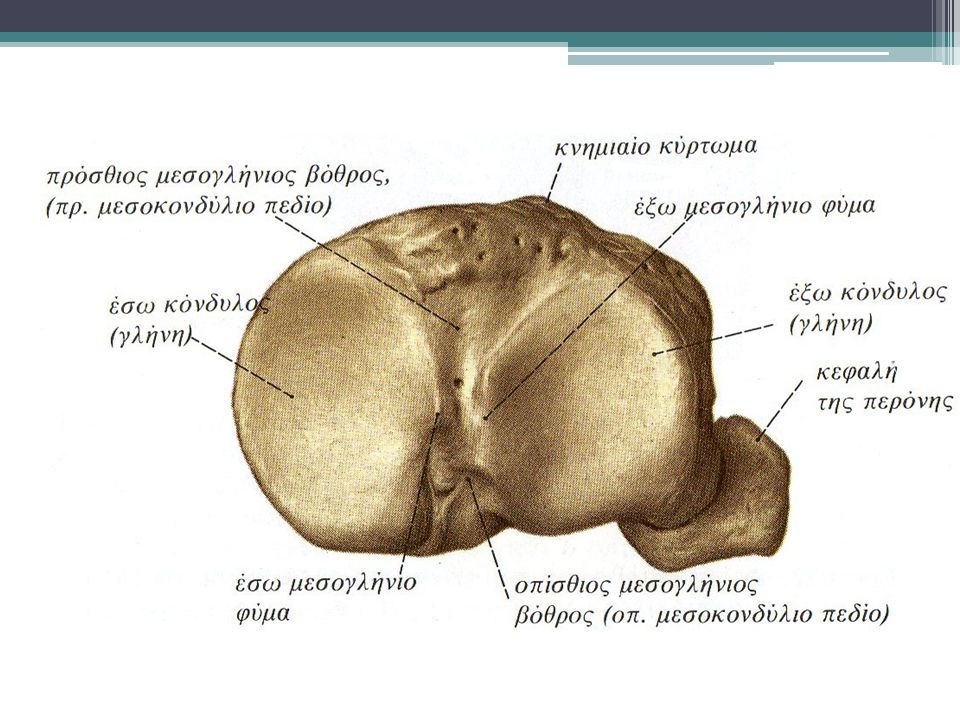
Κνήμη Το άνω άκρο της κνήμης αποτελείται από τον έσω και έξω κόνδυλο που σχηματίζουν αρθρικές επιφάνειες την έσω και έξω κνημιαία γλήνη αντίστοιχα. Χωρίζονται από το μεσογλήνιο έπαρμα οπου βρίσκονται σύνδεσμοι( χιαστοί) και μεσάθριοι χόνδροι(μηνίσκοι) Χαμηλότερα από τους κονδύλους υπάρχει το κνημιαίο όγκωμα ή κύρτωμα
 και μεσάθριοι χόνδροι(μηνίσκοι) Χαμηλότερα από τους κονδύλους υπάρχει το κνημιαίο όγκωμα ή κύρτωμα.")
12
Πλάγια όψη( έξω) Μηριαίο (Femur):έξω μηριαίος κόνδυλος( lateral epicondyle & condyle) Επιγονατίδα (Patella) Κνήμη (Tibia): έξω κόνδυλος lateral condyle, Κνημιαίο όγκωμα (tibial tuberosity) Περόνη (Fibula): head of the fibula Lateral View LE P LFC LTC HoF TT
: έξω κόνδυλος lateral condyle, Κνημιαίο όγκωμα (tibial tuberosity) Περόνη (Fibula): head of the fibula. Lateral View. LE. P. LFC. LTC. HoF. TT.")
13
Πλάγια όψη ( έσω) Μηριαίο (Femur): έσω μηριαίος κόνδυλος medial epicondyle & condyle Επιγονατίδα( Patella) Κνήμη (Tibia|): medial condyle Medial View P ME P MFC MTC
: medial condyle. Medial. View. P. ME. P. MFC. MTC.")
14
Οπίσθια όψη Έσω και έξω υπερκονδύλιες γραμμές M/L supracondylar lines
Ιγνυακή επιφάνεια Popliteal surface M/L femoral condyles M/L tibial condyles Head of the fibula M L Post PS MFC LFC MTC LTC HoF

15
Tibial Plateau

17
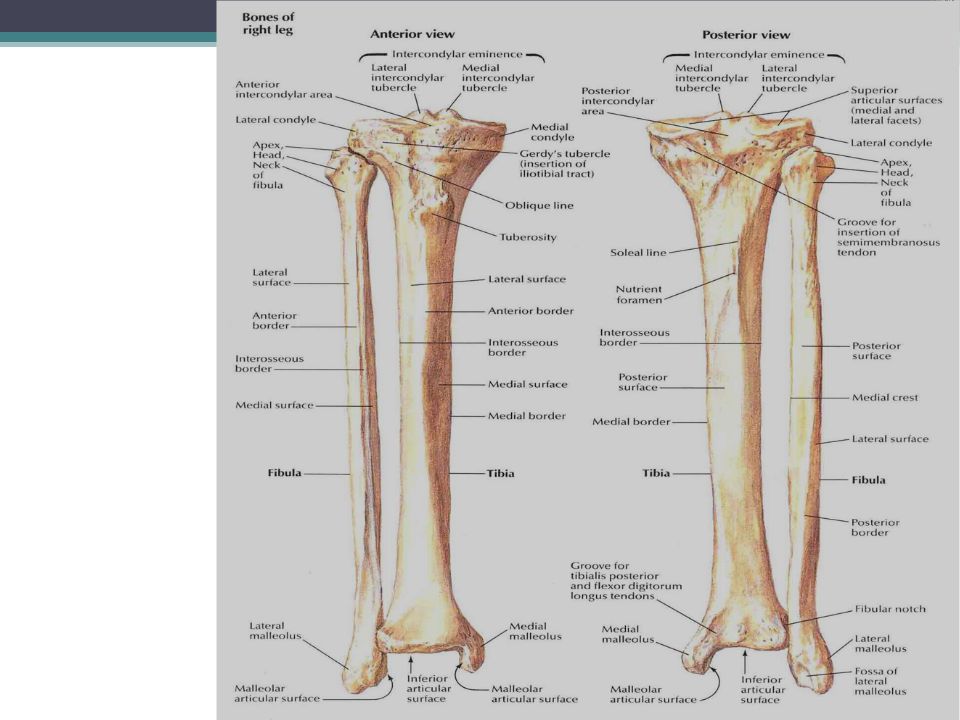
Κνήμη Το σώμα της κνήμης είναι τρίγωνο και παρουσιάζει 3 επιφάνειες(έσω, έξω και οπίσθια) και 3 χείλη( πρόσθιο, έσω και έξω) Το πρόσθιο χείλος είναι ψηλαφητό -> κνημιαία ακρολοφία Το κάτω άκρο της κνήμης σχηματίζει το έσω σφυρό για την σύνταξη με το ταρσό και το σχηματισμό της ΠΔΚ και την περονιαία εντομή για την υποδοχή της περόνης Μεσόστεος υμένας

18
Περόνη Το άνω άκρο της ( κεφαλή) συντάσσεται με την κνήμη
Το άνω άκρο της ( κεφαλή) συντάσσεται με την κνήμη Το κάτω άκρο της κατεβαίνει χαμηλότερα της επίφυσης της κνήμης και καταλήγει στο έξω σφυρό ( ΠΔΚ)
 συντάσσεται με την κνήμη. Το κάτω άκρο της κατεβαίνει χαμηλότερα της επίφυσης της κνήμης και καταλήγει στο έξω σφυρό ( ΠΔΚ)")
19
Πάνω από το γόνατο, στην οπίσθια επιφάνεια, το ισχιακό νεύρο διαιρείται στους τελικούς του κλάδους:
Κνημιαίο ν- κοινό περονιαίο ν

20
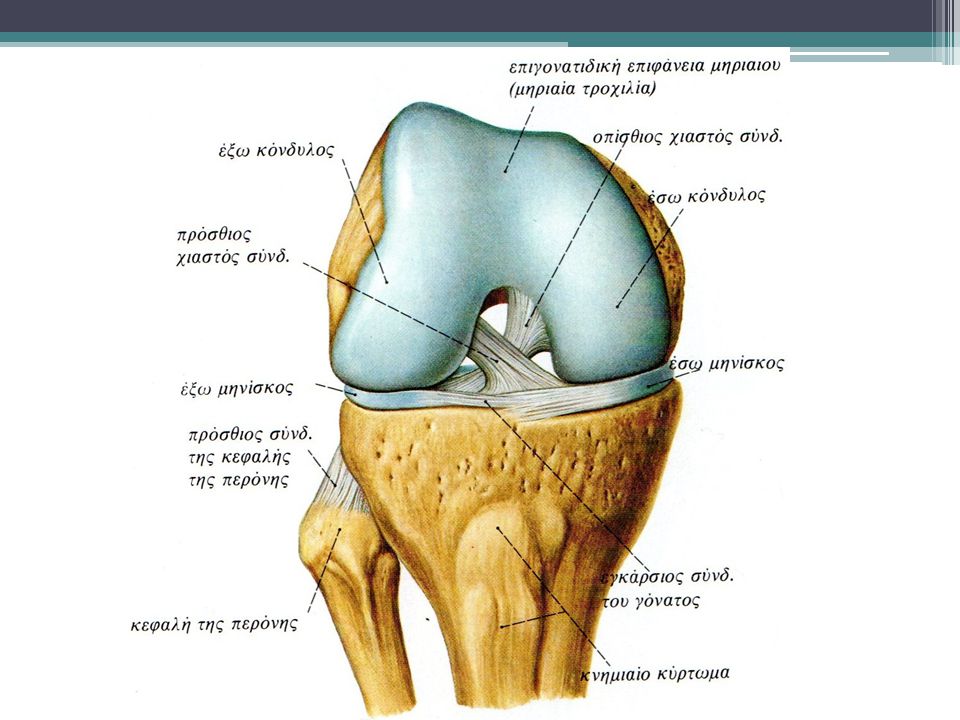
Σύνδεσμοι Οι κύριοι σύνδεσμοι που σχετίζονται με το γόνατο είναι :
Οι κύριοι σύνδεσμοι που σχετίζονται με το γόνατο είναι : Επιγονατιδικός σύνδεσμος Καθεκτικοί της επιγονατίδας Κνημιαίος( έσω πλάγιος) σύνδεσμος Περονιαίος( έξω πλάγιος) σύνδεσμος Πρόσθιος χιαστός Οπίσθιος χιαστός Λοξός ιγνυακός σύνδεσμος
 σύνδεσμος. Περονιαίος( έξω πλάγιος) σύνδεσμος. Πρόσθιος χιαστός. Οπίσθιος χιαστός. Λοξός ιγνυακός σύνδεσμος.")
23
Έσω πλάγιος: πλατειά ταινία
Έξω πλάγιος σύνδεσμος: στενή ταινία Αποτρέπουν τις πλάγιες παρεκκλίσεις του γόνατος Και οι δύο είναι τεταμένοι με το γόνατο σε έκταση και χαλαρώνουν σε θέση κάμψης

24
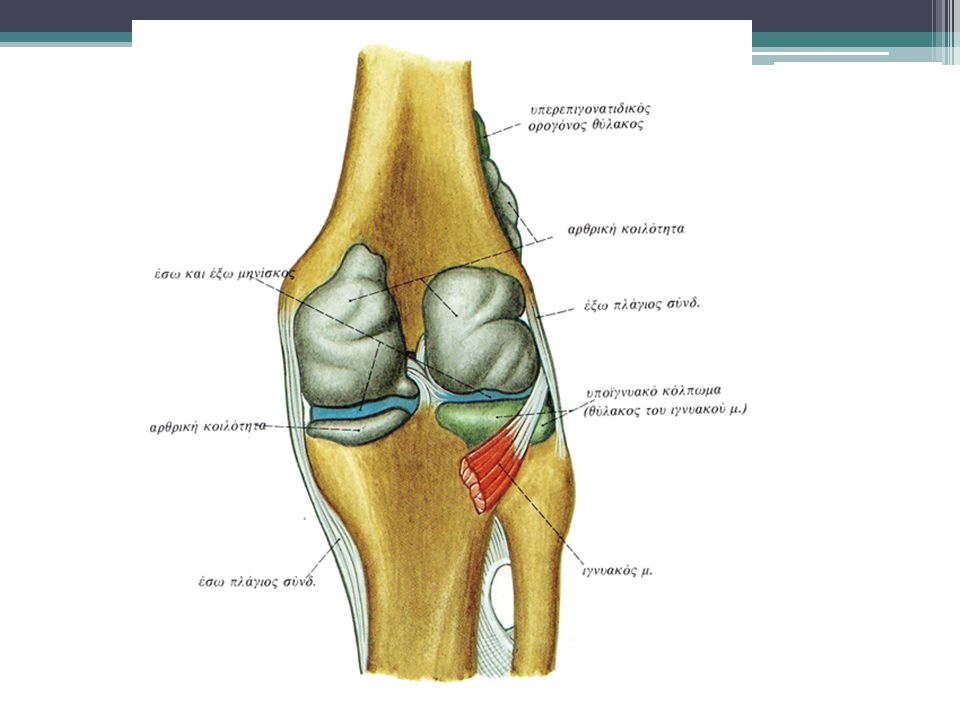
Αρθρικός υμένας και αρθρικοί θύλακες
The suprapatellar bursa lies between the femur and the quads tendon The prepatellar bursa lies outside the synovial cavity but within the capsule The synovial capsule is the largest joint space in the body and lines the fibrous capsule

26
Υποεπιγονατιδικό λιπώδες σώμα

27
Knee Flexion and Extension

28
Knee Medial and Lateral Rotation This is an accessory movement only
Medial Rotation Lateral Rotation

29
Joint Lines Patellofemoral joint Tibia Fibula

30
Πρόσθιος Χιαστός Anterior Cruciate Ligament
Ο ΠΧΣ εκφύεται από ένα βοθρίο του πρόσθιου τμήματος της μεσοκονδύλιας περιοχής της κνήμης, φέρεται προς τα επάνω και πίσω και καταφύεται σε ένα βοθρίο στο πίσω μέρος του έξω τοιχώματος του μεσοκονδυλίου βόθρου του μηριαίου οστού. Εμποδίζει την πρόσθια μετατόπιση της κνήμης 38mm long, 10mm wide

31
Anterior Cruciate Ligament
Anatomy Arises from the anterior aspect of the intercondylar area of the tibia, posterior to the attachment of the medial meniscus Extends posterolaterally and superiorly to attach to the posterior part of the medial side of the lateral femoral condyle Slack in flexion > taut in extension > becomes taut again at 90º flexion Function ACL is the primary restraint to: anterior displacement of the tibia on the femur i.e. posterior displacement of the femur on the tibia Also helps restrain excessive varus and valgus and IR of the tibia (component of pronation) Usually injured during valgus force and or rotational twist with the foot planted or hyperextension of the knee.
 Usually injured during valgus force and or rotational twist with the foot planted or hyperextension of the knee.")
32
The cruciate ligaments (image) are two in number
The cruciate ligaments (image) are two in number. They are named anterior and posterior with regard to the positions of their attachments on the tibial plateau; the anterior cruciate ligament being attached to the anterior intercondylar area of the tibial plateau, and the posterior cruciate being attached to the posterior intercondylar area of the tibial plateau. They are named cruciate ligaments because they cross each other (like the limbs of the letter X). Both cruciate ligaments are situated within the capsule of the knee joint. However they are not within the synovial cavity of the knee joint. The cruciate ligaments receive a sensory innervation from the genicular branches of the tibial, common peroneal and obturator nerves. Sensations subserved by these sensory nerves include both pain and proprioception, and correspondingly both pain receptors and mechano-receptors have been identified within the cruciate ligaments. The cruciate ligaments are vascularized structures; the blood supply of the cruciate ligaments being derived from the genicular branches (principally the middle genicular branch) of the popliteal artery. Thus hemarthrosis is an important clinical feature of cruciate rupture. The function of the anterior cruciate ligament (movie) is to resist posterior displacement of the femur on the tibia. The function of the posterior cruciate ligament (movie) is to resist anterior displacement of the femur on the tibia. The anterior cruciate ligament lies entirely within the capsule of the knee joint but extrasynovially. Its inferior attachment ( Slide 1 (image) , Slide 2 (image) ) (i.e., tibial attachment (movie) ) is to a facet on the medial part of the anterior intercondylar area of the tibial plateau. Its superior attachment (image) is to a facet on the posterior part of the medial surface of the lateral femoral condyle. Thus the anterior cruciate ligament runs obliquely upwards, posteriorly and laterally from its tibial attachment to its femoral attachment. However, the fibers arising most anteriorly on the tibial plateau are attached most posteriorly on the lateral femoral condyle, and the fibers arising most posteriorly on the tibial plateau are attached most anteriorly on the femur. As a result of this arrangement the anterior cruciate ligament is slightly twisted about its long axis. Because of this helical structure, in a functional sense the anterior cruciate ligament appears to consist of two bands (movie) although morphologically it is a single structure. These are referred to as the anteromedial and posterolateral bands. Of the two, the posterolateral component makes up the greater part of the ligament. Knee flexion is associated with a greater degree of tautness in the anteromedial component, while extension results in a greater degree of tautness in the posterolateral component. Another consequence of the spiral nature of the anterior cruciate ligament is that tension in the ligament is increased during internal rotation of the joint, while external rotation of the joint results in a decrease in ligament tension. In the adult, the anterior cruciate ligament is 38mm long and 10mm wide on average. Clinical Text Jump to Anatomy Text The anterior cruciate ligament tibial attachment fans out to form a ' footprint (movie) ' region anteriorly, which resembles a webbed duck's foot ('fanning out'). This allows the anterior cruciate ligament to fit under the roof of the intercondylar notch in full knee extension. A difficulty is presented when attempting to reconstruct the anterior cruciate ligament anatomically, because anterior cruciate ligament grafts are straight and so anteriorly do not possess such a 'footprint'. If the graft is placed anteriorly, it may therefore impinge (movie) on the roof of the intercondylar notch, resulting in possible graft failure. A graft that is placed too posteriorly may not function adequately in resisting the anterior displacement of the tibia. The anterior cruciate ligament (image) is usually ruptured in a rotary strain to the knee. This is frequently in contact games, such as soccer and rugby/football. Skiing is another common sport in which this severe rotary strain is applied to the knee, rupturing the anterior cruciate ligament and occasionally causing associated meniscal or osteochondral damage. X-rays are taken to exclude other bony lesions and MRI scans taken to accurately confirm the rupture. There is frequently a bone bruise (image) associated and there may be meniscal damage - particularly posterior segment and peripheral.
 are two in number. They are named anterior and posterior with regard to the positions of their attachments on the tibial plateau; the anterior cruciate ligament being attached to the anterior intercondylar area of the tibial plateau, and the posterior cruciate being attached to the posterior intercondylar area of the tibial plateau. They are named cruciate ligaments because they cross each other (like the limbs of the letter X). Both cruciate ligaments are situated within the capsule of the knee joint. However they are not within the synovial cavity of the knee joint. The cruciate ligaments receive a sensory innervation from the genicular branches of the tibial, common peroneal and obturator nerves. Sensations subserved by these sensory nerves include both pain and proprioception, and correspondingly both pain receptors and mechano-receptors have been identified within the cruciate ligaments. The cruciate ligaments are vascularized structures; the blood supply of the cruciate ligaments being derived from the genicular branches (principally the middle genicular branch) of the popliteal artery. Thus hemarthrosis is an important clinical feature of cruciate rupture. The function of the anterior cruciate ligament (movie) is to resist posterior displacement of the femur on the tibia. The function of the posterior cruciate ligament (movie) is to resist anterior displacement of the femur on the tibia. The anterior cruciate ligament lies entirely within the capsule of the knee joint but extrasynovially. Its inferior attachment ( Slide 1 (image) , Slide 2 (image) ) (i.e., tibial attachment (movie) ) is to a facet on the medial part of the anterior intercondylar area of the tibial plateau. Its superior attachment (image) is to a facet on the posterior part of the medial surface of the lateral femoral condyle. Thus the anterior cruciate ligament runs obliquely upwards, posteriorly and laterally from its tibial attachment to its femoral attachment. However, the fibers arising most anteriorly on the tibial plateau are attached most posteriorly on the lateral femoral condyle, and the fibers arising most posteriorly on the tibial plateau are attached most anteriorly on the femur. As a result of this arrangement the anterior cruciate ligament is slightly twisted about its long axis. Because of this helical structure, in a functional sense the anterior cruciate ligament appears to consist of two bands (movie) although morphologically it is a single structure. These are referred to as the anteromedial and posterolateral bands. Of the two, the posterolateral component makes up the greater part of the ligament. Knee flexion is associated with a greater degree of tautness in the anteromedial component, while extension results in a greater degree of tautness in the posterolateral component. Another consequence of the spiral nature of the anterior cruciate ligament is that tension in the ligament is increased during internal rotation of the joint, while external rotation of the joint results in a decrease in ligament tension. In the adult, the anterior cruciate ligament is 38mm long and 10mm wide on average. Clinical Text Jump to Anatomy Text The anterior cruciate ligament tibial attachment fans out to form a footprint (movie) region anteriorly, which resembles a webbed duck s foot ( fanning out ). This allows the anterior cruciate ligament to fit under the roof of the intercondylar notch in full knee extension. A difficulty is presented when attempting to reconstruct the anterior cruciate ligament anatomically, because anterior cruciate ligament grafts are straight and so anteriorly do not possess such a footprint . If the graft is placed anteriorly, it may therefore impinge (movie) on the roof of the intercondylar notch, resulting in possible graft failure. A graft that is placed too posteriorly may not function adequately in resisting the anterior displacement of the tibia. The anterior cruciate ligament (image) is usually ruptured in a rotary strain to the knee. This is frequently in contact games, such as soccer and rugby/football. Skiing is another common sport in which this severe rotary strain is applied to the knee, rupturing the anterior cruciate ligament and occasionally causing associated meniscal or osteochondral damage. X-rays are taken to exclude other bony lesions and MRI scans taken to accurately confirm the rupture. There is frequently a bone bruise (image) associated and there may be meniscal damage - particularly posterior segment and peripheral.")
33
Οπίσθιος χιαστός σύνδεσμος Posterior Cruciate Ligament
Posterior View Ο ΟΧΣ εκφύεται από το οπίσθιο τμήμα της μεσοκονδύλιας περιοχής της κνήμης, φέρεται προς τα επάνω και εμπρός και καταφύεται στο έσω τοίχωμα του μεσοκονδύλιου βόθρου του μηριαίου. Εμποδίζει την οπίσθια παρεκτόπιση της κνήμης 38mm long, 13 wide Thicker & less oblique

34
The Posterior Cruciate Ligament
Anatomy Task: Describe the anatomical path of the PCL PCL is stronger than the ACL Slack when knee is in extension; tightens during knee flexion Function Prevents posterior displacement of the tibia on the femur (or anterior displacement of the femur on the tibia) Helps to stabilise the weight- bearing flexed knee, e.g. when walking downhill, or up stairs Can be injured when the upper tibia is struck when the knee is in flexion, e.g. a driver in a RTA Clinically, this is seen as a positive posterior drawer sign
 Helps to stabilise the weight- bearing flexed knee, e.g. when walking downhill, or up stairs. Can be injured when the upper tibia is struck when the knee is in flexion, e.g. a driver in a RTA. Clinically, this is seen as a positive posterior drawer sign.")
35
Έσω πλάγιος Σύνδεσμος Medial Collateral Ligament
Εκφύεται από τον έσω επικόνδυλο Καταφύεται στο έσω χείλος και την έσω επιφάνεια της κνήμης πάνω από το χήνειο πόδα Ενώνεται με τον έσω μηνίσκο Πλατειά και επίπεδη ταινία Προσφύεται στον αρθρικό θύλακο 2x

36
The Medial Collateral Ligament
MCL extends from the medial epicondyle of the femur to the medial border of the tibia and also on the anteromedial surface of the tibia. The inferior attachment of the tibial collateral ligament is almost a hand's breadth below the knee joint line. Part of the MCL inserts into the medial tibial condyle. Attached firmly to the capsule and blends with the capsule, which is in turn firmly attached to the medial meniscus The attachment of the MCL to the medial meniscus results in associated injuries to the meniscus and ACL

37
Medial Collateral Ligament (Syn
Medial Collateral Ligament (Syn. Tibial Collateral Ligament) Anatomy Text The tibial collateral ligament (image) is a strong, flat band on the medial aspect of the knee joint. From its superior attachment to the medial femoral epicondyle, the tibial collateral ligament widens gradually towards its inferior attachment to the medial border of the tibia and somewhat anteriorly on the adjacent medial surface of the tibia. The inferior attachment of the tibial collateral ligament is almost a hand's breadth below the knee joint line. The lower end of the ligament is crossed superficially by the pes anserinus; often a bursa (the bursa anserinus) lies between the two. The tibial collateral ligament is described as consisting of two parts (movie) - an anterior band and a posterior band. The two parts are of course not physically separate. Sometimes a bursa or two lie deep to the anterior band, separating the ligament from the underlying joint capsule and medial meniscus, while still more distally the medial inferior genicular neurovascular structures lie between the medial collateral ligament and the tibia. The posterior part of the tibial collateral ligament turns postero-medially and blends with the capsule of the knee joint and, in part, fuses with the medial edge of the medial meniscus. Part of the posterior part of the medial collateral ligament also attaches to the medial tibial condyle.
 Anatomy Text The tibial collateral ligament (image) is a strong, flat band on the medial aspect of the knee joint. From its superior attachment to the medial femoral epicondyle, the tibial collateral ligament widens gradually towards its inferior attachment to the medial border of the tibia and somewhat anteriorly on the adjacent medial surface of the tibia. The inferior attachment of the tibial collateral ligament is almost a hand s breadth below the knee joint line. The lower end of the ligament is crossed superficially by the pes anserinus; often a bursa (the bursa anserinus) lies between the two. The tibial collateral ligament is described as consisting of two parts (movie) - an anterior band and a posterior band. The two parts are of course not physically separate. Sometimes a bursa or two lie deep to the anterior band, separating the ligament from the underlying joint capsule and medial meniscus, while still more distally the medial inferior genicular neurovascular structures lie between the medial collateral ligament and the tibia. The posterior part of the tibial collateral ligament turns postero-medially and blends with the capsule of the knee joint and, in part, fuses with the medial edge of the medial meniscus. Part of the posterior part of the medial collateral ligament also attaches to the medial tibial condyle.")
38
Έξω πλάγιος Σύνδεσμος Lateral Collateral Ligament
Έξω επικόνδυλος Κεφαλή περόνης Δεν προσφύεται στον αρθρικό θύλακο ή το μηνίσκο Σχοινιοειδής κατασκευή Lateral View

39
The Lateral Collateral Ligament
LCL is a strong cord extending from the lateral epicondyle of the femur to the lateral surface of the fibular head LCL and capsule are separated from the lateral meniscus by the tendon of popliteus Fuses with the fibrous capsule of the knee joint superiorly Not commonly torn, although there may be partial tears of the distal end of the ligament A complete LCL tear is associated with injury to the common peroneal nerve

40
Lateral Collateral Ligament (Syn
Lateral Collateral Ligament (Syn. Fibular Collateral Ligament) Anatomy Text Jump to Clinical Text The fibular collateral ligament is a cord-like structure, ( Slide 1 (image) , Movie 1 (movie) ). It is attached superiorly to the lateral femoral epicondyle on the lateral surface of the lateral femoral condyle. Its inferior attachment is to the fibular head where it blends, in part, with the tendon of insertion of biceps femoris. Unlike the tibial (medial) collateral ligament which blends with the capsule of the knee joint and is partly attached to the medial edge of the medial meniscus, the fibular collateral ligament remains free both of the knee joint capsule and the lateral meniscus. The fibular collateral ligament arches over the tendon of popliteus and the lateral inferior genicular nerve and vessels. Bursa between fibular collateral ligament and popliteus tendon This may communicate with the joint cavity. Bursa between fibular collateral ligament and biceps femoris tendon Occasionally a bursa may be found in relation to the fibular end of the biceps femoris tendon insertion. A bursa may, at times, be present at a higher level in the lateral part of the popliteal fossa. Clinical Text Jump to Anatomy Text The biceps femoris bursa, may be confused with a ganglion arising from the superior tibiofibular joint. However, both abnormalities usually require excision.
 Anatomy Text Jump to Clinical Text The fibular collateral ligament is a cord-like structure, ( Slide 1 (image) , Movie 1 (movie) ). It is attached superiorly to the lateral femoral epicondyle on the lateral surface of the lateral femoral condyle. Its inferior attachment is to the fibular head where it blends, in part, with the tendon of insertion of biceps femoris. Unlike the tibial (medial) collateral ligament which blends with the capsule of the knee joint and is partly attached to the medial edge of the medial meniscus, the fibular collateral ligament remains free both of the knee joint capsule and the lateral meniscus. The fibular collateral ligament arches over the tendon of popliteus and the lateral inferior genicular nerve and vessels. Bursa between fibular collateral ligament and popliteus tendon This may communicate with the joint cavity. Bursa between fibular collateral ligament and biceps femoris tendon Occasionally a bursa may be found in relation to the fibular end of the biceps femoris tendon insertion. A bursa may, at times, be present at a higher level in the lateral part of the popliteal fossa. Clinical Text Jump to Anatomy Text The biceps femoris bursa, may be confused with a ganglion arising from the superior tibiofibular joint. However, both abnormalities usually require excision.")
41
Πλάγιοι Σύνδεσμοι Collateral ligaments
Ο Έσω πλάγιος σύνδεσμος περιορίζει: Ο έξω πλάγιος σύνδεσμος περιορίζει : Βλαισές δυνάμεις Έκταση του γόνατος Στροφή του γόνατος Συνήθως τραυματίζεται με βλαισά φορτία όταν το πόδι είναι σταθερό. Ραιβές δυνάμεις Έκταση του γόνατος Στροφή του γόνατος Συνήθως τραυματίζεται με ραιβά φορτία όταν το πόδι είναι σταθερό.

42
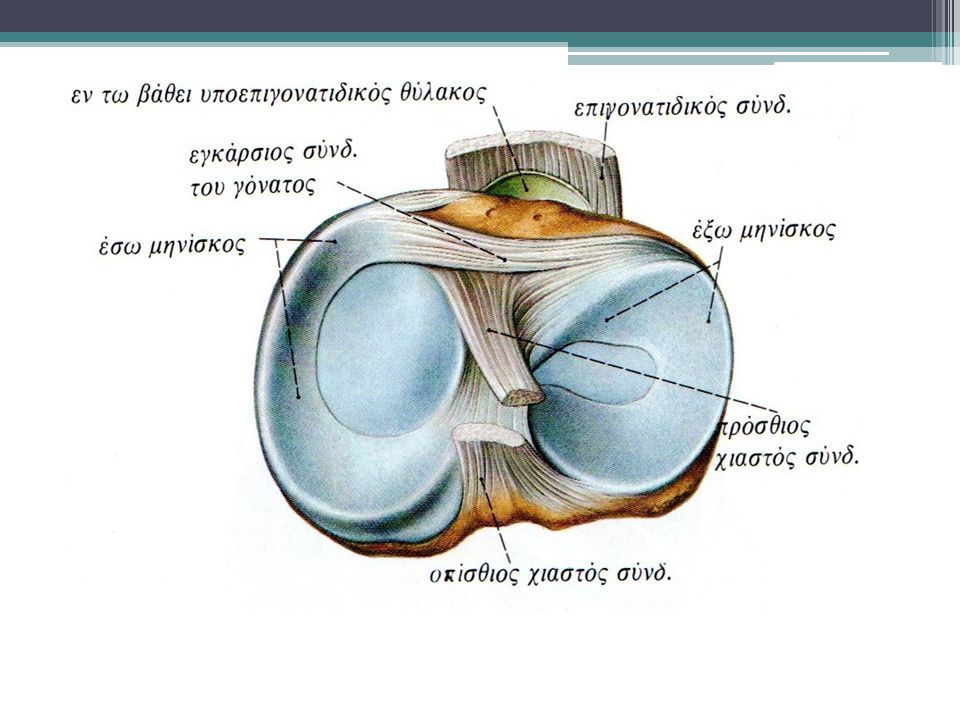
Μηνίσκοι 2 μηνίσκοι( έσω- έξω) Ινοχόνδρινοι ημιδακτύλιοι σχήματος C
Χωρίζουν την αρθρική κοιλότητα στα δύο Απορρόφηση κραδασμών Σφηνοειδείς Βελτιώνουν την προσαρμογή μηριαίων και κνημιαίων κονδύλων Σταθεροποιούν το γόνατο

43
The Menisci Οι μηνίσκοι προσφύονται με τα δύο άκρα τους ( κέρατα) σε βοθρία της μεσοκονδύλιας περιοχής της άνω επιφάνειας της κνήμης. Οι μηνίσκοι ενώνονται προς τα μπρος μεταξύ του με τον εγκάρσιο σύνδεσμο. Συντελούν στην κατανομή των φορτίων στην άρθρωση, την βαθαίνουν κα απορροφούν τους κραδασμούς (Blue denotes attachment sites for horns of menisci; pink denotes cruciate ligament attachments)
")
44
Ο έσω μηνίσκος είναι μεγαλύτερος από τον έξω
Μόνο η περιφέρεια αιματώνεται καθώς επίσης το έξω 1/3 του μηνίσκου είναι εννευρωμένο. Lateral meniscus Medial meniscus The menisci ( Slide 1 (image) , Slide 2 (image) ) (also known as semilunar cartilages) are two in number. Termed medial and lateral, they are crescentic fibrocartilaginous structures situated within the capsule of the knee joint. They are interposed between the tibial plateau and the femoral condylar articular area. The medial and lateral menisci are attached by their peripheries to the rims of the corresponding articular facets on the tibial plateau. The peripheral attached border of each meniscus is thick while the inner free border is thin. Thus each meniscus is wedge-shaped (i.e., triangular) in cross section. This arrangement serves to deepen the articular area afforded by the tibia. The upper surface of each meniscus is concave and articulates with the peripheral part of the overlying femoral condyle. The lower surface of the meniscus is flat and rests on the articular facet of the tibial plateau. The peripheral edge of each meniscus blends with the inner surface of the fibrous capsule of the knee joint. Being crescentic, each meniscus possesses an anterior horn (image) and a posterior horn (image) . The horns of the menisci are attached to the non-articular intercondylar area of the tibial plateau, and are fairly well-vascularized like the peripheral part of the meniscus. Histological studies have confirmed that the horns of the menisci are well innervated and have a variety of sensory receptors believed to mediate proprioception. Lateral meniscus The lateral meniscus is nearly circular in outline, and unlike the medial meniscus its width is more or less uniform along its length. The lateral meniscus covers more of the tibial articular surface than does the medial meniscus. The anterior horn of the lateral meniscus is attached to the anterior intercondylar area of the tibia immediately in front of the intercondylar eminence. The posterior horn of the lateral meniscus is attached to the posterior intercondylar area of the tibia immediately posterior to the intercondylar eminence. The tendon of popliteus on its way to the lateral surface of the lateral femoral condyle grooves the posterior convexity of the lateral meniscus and is partially attached to it. Attached to the posterior part of the lateral meniscus just behind its posterior horn are the anterior and posterior meniscofemoral ligaments. These ligaments extend from the medial femoral condyle to the lateral meniscus and run respectively in front of and behind the posterior cruciate ligament to reach the lateral meniscus. A meniscofibular ligament extending from the posterolateral aspect of the lateral meniscus to the fibular head has been described. In at least one anatomical study, the meniscofibular ligament was found to be present in the majority of knees examined. 2D image (image) of the lateral meniscus. 3D rendered images of the lateral meniscus ( Slide 1 (image) , Slide 2 (image) ). Medial meniscus The medial meniscus is approximately semicircular. It is 3.5cms in antero-posterior dimension on average, and is considerably wider posteriorly than anteriorly. Its anterior horn attaches to the anterior intercondylar area of the tibia in front of the tibial attachment of the anterior cruciate ligament. The posterior horn is attached to the posterior tibial intercondylar area in front of the attachment of the posterior cruciate ligament. Its peripheral edge blends with the capsule of the knee joint and with the deep surface of the tibial collateral ligament. Vascular anatomy of menisci The peripheral edge of each meniscus is penetrated by the capsular blood vessels derived from the genicular anastomosis. On the basis of anatomic studies it has been estimated that the depth of vascular penetration from the periphery inwards is approximately 20 percent of the thickness of the medial meniscus, and 15 percent of the thickness of the lateral meniscus. The inner zone of the meniscus is avascular, and like articular hyaline cartilage, is believed to derive its nutrition chiefly by diffusion. As distinct from repair, menisci are capable of a degree of regeneration after total meniscectomy, particularly in children. Regeneration takes place from the peripheral vascularized tissue. Menisci have only a limited capacity for repair and that mainly in the peripheral vascularized zone. Thus tears in the inner part of the meniscus seldom heal spontaneously. Meniscal biochemistry Histologically, the menisci are composed of fibroblasts and chondrocytes set in a complex extracellular matrix. This extracellular matrix is elaborated by the meniscal cells, and is made up of an interlacing network of collagen fibers (making up approximately 70% of the dry weight of the meniscus) of different biochemical types, with type 1 collagen predominating. In addition to collagen, the extracellular matrix consists of a variety of proteoglycans and other proteins such as adhesion protein molecules and elastin. Ultrastructural studies have revealed that the collagen fibers in the peripheral third of the width of each meniscus are arranged circumferentially, while in the inner two-thirds of the meniscus the fibers have a predominantly radial orientation. It has been suggested that the radial fibers provide structural support by functioning as ties, and thereby resisting longitudinal splitting of the meniscus. Clinical Text Jump to Anatomy Text Approximately 50% of the compressive load of the knee joint is transmitted through the meniscus in extension, and 85% of the load is transmitted in 90 degrees of flexion. After meniscectomy the contact area in the knee is reduced approximately 50%. As a result, the load per unit area increases, subjecting the articular cartilage to increased risk of damage. Seedholm and Hargreaves have shown that removal of 15-34% of the meniscus increases contact pressures by more than 350%. With the passage of time, joint space narrowing, osteophyte formation, and flattening of the femoral condyle occur. Meniscal tears are amongst the most common traumatic lesions of the knee joint. Meniscal tears may be traumatic or degenerative with a mild injury producing the problem. The usual mechanism of injury is a twisting force on a weight bearing flexed knee. Sometimes the twist is fairly trivial and in some degenerative menisci the tear may be substantial. The incidence of certain meniscal tear types varies with the age of the individual. Medial meniscal tears are more commonly associated with stable knee joints. Lateral meniscal tears are of a more common occurrence with anterior cruciate ligament injuries. Treatment options depend on a number of factors including tear type, location, and severity. Some minor tears require no treatment especially when they are associated with anterior cruciate ligament rupture. A tear within 3 mm from the periphery is vascular and therefore heals well. Many tears are unrepairable and partial menisectomy is the treatment of choice. Meniscal repairs can be undertaken using sutures, biodegradable materials such as arrows, T-fixes, screws and absorbable hooks. Collagen meniscal implants may be inserted into meniscal defects and meniscal allografts are still undergoing evaluation and should be undertaken in specific units where research continues. Surgical approaches to a meniscal repair include open, combined arthroscopic-open or arthroscopic procedures. Open repair usually deals with peripheral tears only at the meniscosynovial junction. Arthroscopic techniques include inside out, outside in, and all inside techniques. In these techniques, freshing of the tear with a rasp, vertically orientated sutures and in chronic tears the possible use of a fibrin clot is recommended. Non absorbable sutures that retain their strength for several months are required. Articular cartilage
 , Slide 2 (image) ) (also known as semilunar cartilages) are two in number. Termed medial and lateral, they are crescentic fibrocartilaginous structures situated within the capsule of the knee joint. They are interposed between the tibial plateau and the femoral condylar articular area. The medial and lateral menisci are attached by their peripheries to the rims of the corresponding articular facets on the tibial plateau. The peripheral attached border of each meniscus is thick while the inner free border is thin. Thus each meniscus is wedge-shaped (i.e., triangular) in cross section. This arrangement serves to deepen the articular area afforded by the tibia. The upper surface of each meniscus is concave and articulates with the peripheral part of the overlying femoral condyle. The lower surface of the meniscus is flat and rests on the articular facet of the tibial plateau. The peripheral edge of each meniscus blends with the inner surface of the fibrous capsule of the knee joint. Being crescentic, each meniscus possesses an anterior horn (image) and a posterior horn (image) . The horns of the menisci are attached to the non-articular intercondylar area of the tibial plateau, and are fairly well-vascularized like the peripheral part of the meniscus. Histological studies have confirmed that the horns of the menisci are well innervated and have a variety of sensory receptors believed to mediate proprioception. Lateral meniscus The lateral meniscus is nearly circular in outline, and unlike the medial meniscus its width is more or less uniform along its length. The lateral meniscus covers more of the tibial articular surface than does the medial meniscus. The anterior horn of the lateral meniscus is attached to the anterior intercondylar area of the tibia immediately in front of the intercondylar eminence. The posterior horn of the lateral meniscus is attached to the posterior intercondylar area of the tibia immediately posterior to the intercondylar eminence. The tendon of popliteus on its way to the lateral surface of the lateral femoral condyle grooves the posterior convexity of the lateral meniscus and is partially attached to it. Attached to the posterior part of the lateral meniscus just behind its posterior horn are the anterior and posterior meniscofemoral ligaments. These ligaments extend from the medial femoral condyle to the lateral meniscus and run respectively in front of and behind the posterior cruciate ligament to reach the lateral meniscus. A meniscofibular ligament extending from the posterolateral aspect of the lateral meniscus to the fibular head has been described. In at least one anatomical study, the meniscofibular ligament was found to be present in the majority of knees examined. 2D image (image) of the lateral meniscus. 3D rendered images of the lateral meniscus ( Slide 1 (image) , Slide 2 (image) ). Medial meniscus The medial meniscus is approximately semicircular. It is 3.5cms in antero-posterior dimension on average, and is considerably wider posteriorly than anteriorly. Its anterior horn attaches to the anterior intercondylar area of the tibia in front of the tibial attachment of the anterior cruciate ligament. The posterior horn is attached to the posterior tibial intercondylar area in front of the attachment of the posterior cruciate ligament. Its peripheral edge blends with the capsule of the knee joint and with the deep surface of the tibial collateral ligament. Vascular anatomy of menisci The peripheral edge of each meniscus is penetrated by the capsular blood vessels derived from the genicular anastomosis. On the basis of anatomic studies it has been estimated that the depth of vascular penetration from the periphery inwards is approximately 20 percent of the thickness of the medial meniscus, and 15 percent of the thickness of the lateral meniscus. The inner zone of the meniscus is avascular, and like articular hyaline cartilage, is believed to derive its nutrition chiefly by diffusion. As distinct from repair, menisci are capable of a degree of regeneration after total meniscectomy, particularly in children. Regeneration takes place from the peripheral vascularized tissue. Menisci have only a limited capacity for repair and that mainly in the peripheral vascularized zone. Thus tears in the inner part of the meniscus seldom heal spontaneously. Meniscal biochemistry Histologically, the menisci are composed of fibroblasts and chondrocytes set in a complex extracellular matrix. This extracellular matrix is elaborated by the meniscal cells, and is made up of an interlacing network of collagen fibers (making up approximately 70% of the dry weight of the meniscus) of different biochemical types, with type 1 collagen predominating. In addition to collagen, the extracellular matrix consists of a variety of proteoglycans and other proteins such as adhesion protein molecules and elastin. Ultrastructural studies have revealed that the collagen fibers in the peripheral third of the width of each meniscus are arranged circumferentially, while in the inner two-thirds of the meniscus the fibers have a predominantly radial orientation. It has been suggested that the radial fibers provide structural support by functioning as ties, and thereby resisting longitudinal splitting of the meniscus. Clinical Text Jump to Anatomy Text Approximately 50% of the compressive load of the knee joint is transmitted through the meniscus in extension, and 85% of the load is transmitted in 90 degrees of flexion. After meniscectomy the contact area in the knee is reduced approximately 50%. As a result, the load per unit area increases, subjecting the articular cartilage to increased risk of damage. Seedholm and Hargreaves have shown that removal of 15-34% of the meniscus increases contact pressures by more than 350%. With the passage of time, joint space narrowing, osteophyte formation, and flattening of the femoral condyle occur. Meniscal tears are amongst the most common traumatic lesions of the knee joint. Meniscal tears may be traumatic or degenerative with a mild injury producing the problem. The usual mechanism of injury is a twisting force on a weight bearing flexed knee. Sometimes the twist is fairly trivial and in some degenerative menisci the tear may be substantial. The incidence of certain meniscal tear types varies with the age of the individual. Medial meniscal tears are more commonly associated with stable knee joints. Lateral meniscal tears are of a more common occurrence with anterior cruciate ligament injuries. Treatment options depend on a number of factors including tear type, location, and severity. Some minor tears require no treatment especially when they are associated with anterior cruciate ligament rupture. A tear within 3 mm from the periphery is vascular and therefore heals well. Many tears are unrepairable and partial menisectomy is the treatment of choice. Meniscal repairs can be undertaken using sutures, biodegradable materials such as arrows, T-fixes, screws and absorbable hooks. Collagen meniscal implants may be inserted into meniscal defects and meniscal allografts are still undergoing evaluation and should be undertaken in specific units where research continues. Surgical approaches to a meniscal repair include open, combined arthroscopic-open or arthroscopic procedures. Open repair usually deals with peripheral tears only at the meniscosynovial junction. Arthroscopic techniques include inside out, outside in, and all inside techniques. In these techniques, freshing of the tear with a rasp, vertically orientated sutures and in chronic tears the possible use of a fibrin clot is recommended. Non absorbable sutures that retain their strength for several months are required. Articular cartilage.")
45
The Medial Meniscus Ο έσω μηνίσκος προσφύεται περιφερικά στον αρθρικό θύλακο και στον έσω πλάγιο σύνδεσμο Ο έσω μηνίσκος τραυματίζεται 20 φορές πιο συχνά από τον έξω Ο τραυματισμός συνήθως γίνεται με τη στροφή του γόνατος όταν βρίσκεται σε κάμψη Το κλείδωμα ( block) στο γόνατο συμβαίνει όταν τμήμα από το θραύσμα του μηνίσκου εγκλωβιστεί μεταξύ μηριαίων και κνημιαίων κονδύλων. Medial meniscus broader posteriorly than anteriorly Firmly adherent (via the capsule) to the deep surface of the MCL
 στο γόνατο συμβαίνει όταν τμήμα από το θραύσμα του μηνίσκου εγκλωβιστεί μεταξύ μηριαίων και κνημιαίων κονδύλων. Medial meniscus broader posteriorly than anteriorly. Firmly adherent (via the capsule) to the deep surface of the MCL.")
46
The Lateral Meniscus Ο έξω μηνίσκος είναι μικρότερος πιο ευκίνητος από τον έσω και πιο κυκλικός στην όψη. Ο έξω μηνίσκος δεν προσφύεται στον αρθρικό θύλακο και έξω πλάγιο σύνδεσμο καθώς παρεμβάλλεται ο τένοντας του ιγνυακού μυος

47
Μηρίαιο Νεύρο Νευρώνει το :
Ορθό μηριαίο μυ Rectus femoris: Τετρακέφαλος μυς Έξω πλατύ μυVastus lateralis: Έσω πλατύ Vastus medialis: Μέσο πλατύ Vastus intermedius: Ραπτικό μυ Sartorius:

48
Τετρακέφαλος Quadriceps Muscle Group
Vastus Lateralis Vastus Medialis Vastus Intermedius Rectus Femoris

49
Rectus Femoris Έκφυση: Ορθή κεφαλή -ΠΚΛΑ
Λοξή κεφαλή – όφρυς της κοτύλης Κατάφυση: Βάση και πρόσθια επιφάνεια επιγονατίδας και κνημιαίο κύρτωμα Νεύρωση: Μηριαίο νεύρο( Ο2,Ο3,Ο4 ) Λειτουργία :κάμπτει το μηρό,εκτείνει την κνήμη
 Λειτουργία :κάμπτει το μηρό,εκτείνει την κνήμη.")
50
Vastus Intermedius Έκφυση: Άνω 2/3 της πρόσθιας και έξω επιφάνειας του μηριαίου Κατάφυση: Τένοντας του τετρακεφάλου μηριαίου και έξω χείλος επιγονατίδας Εν τω βάθει μυς Νευρωση : Μηριαίο νεύρο(Ο3,Ο4) Λειτουργία: εκτείνει την κνήμη
 Λειτουργία: εκτείνει την κνήμη")
51
Vastus Medialis Έκφυση: Μεσοτροχαντήρια γραμμή, κτενιαία γραμμή, έσω χείλος τραχείας Κατάφυση: Τένοντας τετρακεφάλου και έσω χείλος Επιγονατίδας Νεύρωση: μηριαίο νεύρο ( Ο3, Ο4) Λειτουργία: εκτείνει την κνήμη
 Λειτουργία: εκτείνει την κνήμη")
52
Vastus Lateralis Έκφυση: Μεσοτροχαντήρια γραμμή, χείλος του μ.τροχαντήρα, γλουτιαιο όγκωμα, έξω χείλος τραχείας γραμμής Κατάφυση: Τένοντας του τετρακεφάλου , έξω χείλος επιγονατίδας Νεύρωση: (μηριαίο νεύρο Ο3,Ο4) Λειτουργία: εκτείνει την κνήμη
 Λειτουργία: εκτείνει την κνήμη")
53
Ραπτικός Sartorius Ε: ΠΑΛΑ
Κ: κνημιαίο κύρτωμα και έσω κόνδυλος της κνήμης( χήνειος πόδας) Ν: Μηριαίο νεύρο( Ο1-Ο3) Λ: Κάμπτει την κνήμη και το μηρό προς την κοιλιά. Στρέφει το μηρό προς τα έξω
 Ν: Μηριαίο νεύρο( Ο1-Ο3) Λ: Κάμπτει την κνήμη και το μηρό προς την κοιλιά. Στρέφει το μηρό προς τα έξω.")
54
Κνημιαίο νεύρο Νευρώνει: Δικέφαλο μηριαίο ΜΚ Biceps femoris LH:
Ημιτενοντώδης Semitendinosus: Ημιυμενώδης Semimembranosus: Ιγνυακός Popliteus: Γαστροκνήμιος Gastrocnemius:

55
Hamstring Muscle Group
Biceps Femoris Semimembranosus Semitendinosus

56
Biceps Femoris Έκφυση : Μακρά κεφαλή:ισχιακό κύρτωμα Βραχεία κεφαλή :έξω χείλος ταχείας γραμμής,έξω υπερκονδύλιας γραμμή Κατάφυση: Κεφαλή τη περόνης Νεύρωση: Ισχιακό νεύρο Ο5-Ι2) Λειτουργία: Κάμπτει την κνήμη προς το μηρό, εκτείνει το μηρό, με λυγισμένο το Γόνατο έξω στροφή κνήμης
 Λειτουργία: Κάμπτει την κνήμη προς το μηρό, εκτείνει το μηρό, με λυγισμένο το Γόνατο έξω στροφή κνήμης")
57
Semimembranosus Έκφυση: Ισχιακό κύρτωμα Κατάφυση: Αύλακα της οπίσθιας επιφάνειας του έσω μηριαίου κονδύλου Νεύρωση: Ισχιακό νεύρο (Ο5,Ι1,Ι2) Λειτουργία : κάμπτει την κνήμη, εκτείνει το μηρό
 Λειτουργία : κάμπτει την κνήμη, εκτείνει το μηρό")
58
Semitendinosus Έκφυση: Ισχιακό κύρτωμα Κατάφυση: Εσω άνω επιφάνεια κνήμης Χήνειος πόδας Νεύρωση: ισχιακό νεύρο ( Ο5-Ι2) Λειτουργία: κάμπτει την κνήμη ,εκτείνει το μηρό
 Λειτουργία: κάμπτει την κνήμη ,εκτείνει το μηρό")
59
Popliteus Έκφυση : Έξω μηριαίος κόνδυλος Λοξός ιγνυακός σύνδεσμος Κατάφυση: Ιγνυακή επιφάνεια της κνήμης Νεύρωση: Κνημιαίο νεύρο(Ο4-Ι1) Λειτουργία: Κάμπτει την κνήμη, έσω στροφή κνήμης
 Λειτουργία: Κάμπτει την κνήμη, έσω στροφή κνήμης")
60
Gastrocnemius Έκφυση: ΜΚ: ιγνυακή επιφάνεια του μηριαίου επάνω από τον έσω μηριαίο κόνδυλο ΒΚ: οπισθιοπλάγια επιφάνεια έξω μηριαίου κονδύλου Κατάφυση: μέσω του αχιλλείου τένοντα στην οπίσθια επιφάνεια της πτέρνας Νεύρωση: Κνημιαίο νεύρο Ο1-Ο2 Λειτουργία: Κάμψη του γόνατος και πελματιαία κάμψη του άκρου ποδός

61
Θυροειδές νεύρο Νευρώνει: Ισχνό Προσαγωγό μυ Gracilis:

62
Gracilis Εκφυση: ηβική σύμφυση. Κάτω χείλος ηβοισχιακού κλάδου Κατάφυση: έσω επιφάνεια κνήμης ( χήνειο πόδι) Νεύρωση: θυροειδές νεύρο (Ο2-Ο4) Λειτουργία: προσάγει το μηρό ,κάμπτει την κνήμη και τη στρέφει προς τα έσω
 Νεύρωση: θυροειδές νεύρο (Ο2-Ο4) Λειτουργία: προσάγει το μηρό ,κάμπτει την κνήμη και τη στρέφει προς τα έσω")
63
Χήνειος Πόδας Sartorius Semitendinosus Gracilis
Pes Anserine: Latin for Goose’s Foot, due to shape of tendons at insertion on tibia

Παρόμοιες παρουσιάσεις














 1/2>")





