Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Μυκωτικά Ανευρύσματα – Μόλυνση Ενδοπρόθεσης Κωνσταντίνος Γ. Μουλακάκης
Κωνσταντίνος Γ. Μουλακάκης Επιμελητής Β Αγγειοχειρουργός, Αγγειοχειρουργική Κλινική, “ Aττικόν” Νοσοκομείο 2014

2
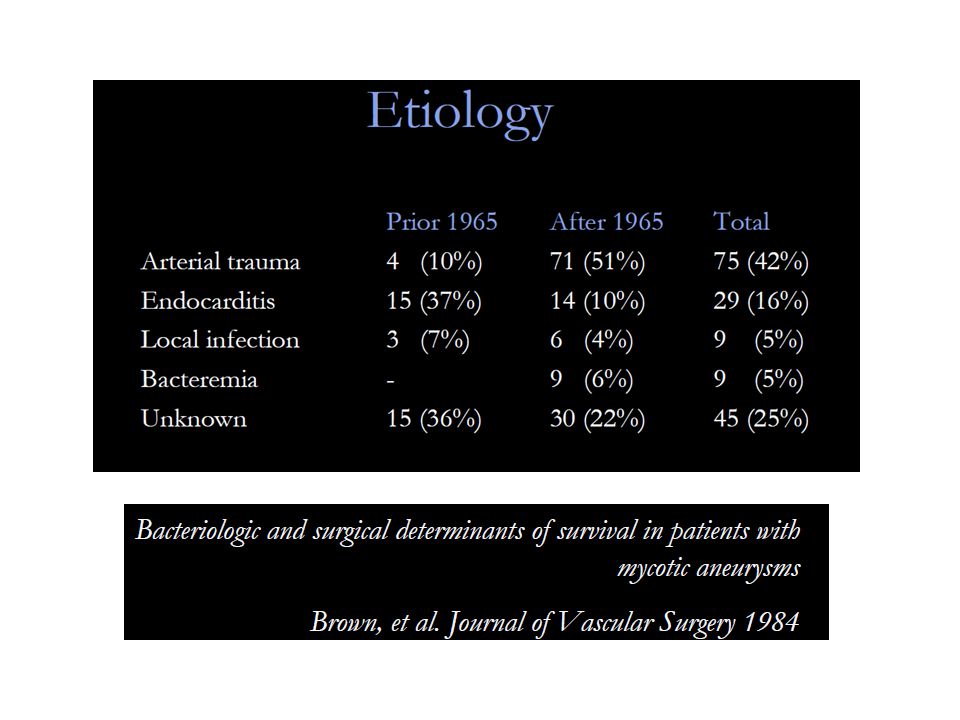
"infected aneurysm" has gradually replaced the original designation "mycotic aneurysm“

3
Μυκωτικά Ανευρύσματα – Αιτιολογία και Παράγοντες Κινδύνου
Μυκωτικά Ανευρύσματα – Αιτιολογία και Παράγοντες Κινδύνου Βακτηριακή Ενδοκαρδίτιδα (σηπτικά έμβολα) Αρτηριακό Τραύμα, ή τραύμα του ενδοθηλίου (Τοξικομανείς, Στεφανιογραφίες, ΧΝΑ) Φλεγμονή, Μικροβιαιμία (Ουρολοίμωξη, Πνευμονία, Εκκολπωματίτιδα) Διασπορά από Φλεγμονή περιξ της αορτής (σπονδυλίτιδα, γαστρεντεριτιδα με προσβολή παραορτικών λεμφαδένων) Διαταραχές ανοσοποιητικού συστήματος (70%) Αθηροσκλήρωση (αποικισμός πλακών από μικρόβια)
 Αρτηριακό Τραύμα, ή τραύμα του ενδοθηλίου (Τοξικομανείς, Στεφανιογραφίες, ΧΝΑ) Φλεγμονή, Μικροβιαιμία (Ουρολοίμωξη, Πνευμονία, Εκκολπωματίτιδα) Διασπορά από Φλεγμονή περιξ της αορτής (σπονδυλίτιδα, γαστρεντεριτιδα με προσβολή παραορτικών λεμφαδένων) Διαταραχές ανοσοποιητικού συστήματος (70%) Αθηροσκλήρωση (αποικισμός πλακών από μικρόβια)")
5
Ο ρόλος της ενδαγγειακής αποκατάστασης στη θεραπεία των Μυκωτικών ανευρυσμάτων

7
21 patients, 17 abdominal and four thoracic infected aortic aneurysms were treated with an endovascular stent graft. Five patients presented with fistula complications, 1 aortoesophageal, 1 aortobronchial, 1 aortocaval, and 2 aortoenteric fistulas. J Vasc Surg 2011

8
The overall in-hospital mortality was 19% (4/21): 60% (3/5) in the fistula group and only 6% (1/16) in the nonfistula group. During the follow-up period, one of the two survivors in the fistula group died at 18 months from unrelated causes. there were no deaths in the 15 patients of the nonfistula group with an average patient follow-up of 22 months (range, 1-54

9
11 patients – endovascular repair of 13 MAAs
Aortic arch (n=1) , descending TAA (n=4), suprarenal AAA (n=3), infrarenal AAA (n=5) Mean follow-up 27 months Sorelius JVS 2009
 , descending TAA (n=4), suprarenal AAA (n=3), infrarenal AAA (n=5) Mean follow-up 27 months. Sorelius JVS")
11
53% Survival 48m Sorelius JVS 2009

12
Retrospective case series 673 AAA – 19 (2.8%) infected
16 TAAs , 7 AAAs 6 RAA (32%) 15 (79%) positive blood cultures Staphylococcus aureus (+) Clough EJVES 2009
 15 (79%) positive blood cultures. Staphylococcus aureus (+) Clough EJVES")
13
Clough EJVES 2009

14
Overall Mortality in follow-up 42%
Stroke (n=1) , CSF drainage/ paraplegia (n=1) 30-day mortality = 11% Survival 20 months = 73% All 8 deaths aneurysm related! Overall Mortality in follow-up 42%
 , CSF drainage/ paraplegia (n=1) 30-day mortality = 11% Survival 20 months = 73% All 8 deaths aneurysm related! Overall Mortality in follow-up 42%")
15
Retrospective case series
27 patients – TEVAR for infected aneurysm 26 high-risk for surgery Patel JVS 2010

16
27 patients 3-year survival 58.4% Patel JVS 2010

17
Endograft infection Graft infection after endovascular aneurysm repair (EVAR or TEVAR) is an underrecognized and underreported event. The incidence of aorto-iliac stent-graft infection ranges from 0.4% to 0.7% (1). Although rare, it may have devastating consequences. Mortality rates range from 25% to 100% (0.6% to 3% for open aortic graft infection 2,3) Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg. 2010 T.W. Swain, et al. Management of infected aortic prosthetic grafts. Vasc Endovascular Surg. 2004 S. O’Connor, et al. A systematic review and meta-analysis of treatments for aortic graft infection. JVS.2006
. Although rare, it may have devastating consequences. Mortality rates range from 25% to 100% (0.6% to 3% for open aortic graft infection 2,3) Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg T.W. Swain, et al. Management of infected aortic prosthetic grafts. Vasc Endovascular Surg S. O’Connor, et al. A systematic review and meta-analysis of treatments for aortic graft infection. JVS")
18
Pathogenesis Stent Graft Related
Bacterial inoculation during endovascular procedure Pre-existing -mycotic aneurysm or inflammatory aneurysm-, could result in intestinal necrosis and fistula formation Remote source of sepsis (eg, endocarditis, pneumonia, urinary tract infection) Cancer or immunodeficiency Repeated secondary procedures Stent migration Erosion of the aorta and the duodenum by embolization coils Fabric rupture ?? Erosion of the aorta by the hooks and barbs Endoleak and endotension may lead to aorto-enteric fistula formation ?? Stent Graft Related Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg. 2010
 Cancer or immunodeficiency. Repeated secondary procedures. Stent migration. Erosion of the aorta and the duodenum by embolization coils. Fabric rupture Erosion of the aorta by the hooks and barbs. Endoleak and endotension may lead to aorto-enteric fistula formation Stent Graft Related. Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg")
19
Clinical Presentation
Aortic Endograft Infection Thoracic Endograft Infection Low grade infection Systemic Sepsis Aortoenteric Fistula (41%) Abdominal or back Pain Abscess (psoas) Pseudonaurysm Urinary tract infection Low grade infection Systemic Sepsis Fistula (aortoesophageal or broncial) (38%) Chest Pain Abscess (periaortic) Pseudonaurysm Pneumonia, mediastinitis 52%% 50%% Numan F. et al. Management of endograft infections. J Cardiovasc Surg. 2011
 Abdominal or back Pain. Abscess (psoas) Pseudonaurysm. Urinary tract infection. Low grade infection. Systemic Sepsis. Fistula (aortoesophageal or broncial) (38%) Chest Pain. Abscess (periaortic) Pseudonaurysm. Pneumonia, mediastinitis. 52%% 50%% Numan F. et al. Management of endograft infections. J Cardiovasc Surg")
20
Εμπλεκόμενοι Μικροοργανισμοί
20-83% αναγνωρίζεται και ταυτοποιείται ο υπεύθυνος μικροβιακός παράγοντας St.Aureus 22% Streptococcus sp. 11% Multiple pathogens 21% Candida Ablicans , Mycetes 6% E.Coli Enterococci Pseudomonas, Serratia, Klebsiella, Ent.Cloacae ↑f Numan F. et al. Management of endograft infections. J Cardiovasc Surg Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg. 2010

21
Διάγνωση μολυσμένου Μοσχεύματος
βαθμός υποψίας Καλλιέργειες Ενδοσκοπικός Ελεγχος (AEF) CT / MR PET CT Πυρηνικός Ελεγχος ,Σπινθηρογράγημα
 CT / MR. PET CT. Πυρηνικός Ελεγχος ,Σπινθηρογράγημα.")
22
Απεικονιστική διάγνωση της λοίμωξης της ενδοπρόθεσης
18 FDG PET/CT

23
Management of Infected Endograft
Depends on : Patient’s clinical status Co-morbidities Presence of preoperative sepsis Microorganisms involved

24
1. ΑΝΟΙΚΤΗ ΧΕΙΡΟΥΡΓΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ
1. ΑΝΟΙΚΤΗ ΧΕΙΡΟΥΡΓΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ

25
Management of Infected Endograft
Graft Excision is the GOLD STANDARD Graft Excision & Extra-anatomic bypass Neo-aortoiliac System Procedure In Situ Aortic Graft Replacement (Homograft, Silver Graft) High mortality and morbidity rates, especially when undertaken in unstable, septic patients with severe comorbidities Variable results on patency and reinfection rates Fiorani P, et al. Endovascular graft infection: preliminary results of an international enquiry. JEVT 2003
 High mortality and morbidity rates, especially when undertaken in unstable, septic patients with severe comorbidities. Variable results on patency and reinfection rates. Fiorani P, et al. Endovascular graft infection: preliminary results of an international enquiry. JEVT")
32
Technique of Aortic stent-graft explantation
JEVT 2010 Technique of Aortic stent-graft explantation Factors that may influence the feasibility of aortic stent-graft explantation The fixation system (hooks or barbs) the associated periaortic inflammatory reaction and endograft incorporation the presence of any additional grafts, cuffs, or coils placed as secondary interventions
 the associated periaortic inflammatory reaction and endograft incorporation. the presence of any additional grafts, cuffs, or coils placed as secondary interventions.")
33
2. ΠΑΡΟΧΕΤΕΥΣΗ, ΧΕΙΡΟΥΡΓΙΚΟΣ ΚΑΘΑΡΙΣΜΟΣ, ΔΙΑΤΗΡΗΣΗ ΤΟΥ ΜΟΣΧΕΥΜΑΤΟΣ
2. ΠΑΡΟΧΕΤΕΥΣΗ, ΧΕΙΡΟΥΡΓΙΚΟΣ ΚΑΘΑΡΙΣΜΟΣ, ΔΙΑΤΗΡΗΣΗ ΤΟΥ ΜΟΣΧΕΥΜΑΤΟΣ

34
Management of Infected Endograft in High Risk patients for open repair
Surgical or CT-guided percutaneous placement of drains into the aneurismal sac abscess contiguous to the graft, in conjunction with irrigation of the perigraft area followed by appropriate antibiotic therapy Promising results in patients without signs of severe sepsis Pryluck DS et al. Percutaneous drainage of aortic aneurysm sac abscesses following endovascular aneurysm repair.Vasc Endovascular Surg.2010 Deshmukh H. et al. Percutaneous management of complications (aortoenteric fistula and sac abscess) following bypass surgery for abdominal aortic aneurysm.Cardiovasc Intervent Radiol. 2007 S.J. Hulin* and G.E. Morris .Eur J Vasc Endovasc Surg .2007
 following bypass surgery for abdominal aortic aneurysm.Cardiovasc Intervent Radiol S.J. Hulin* and G.E. Morris .Eur J Vasc Endovasc Surg")
35
Management of Infected Endograft in High Risk patients for open repair
CT-guided percutaneous drainage followed by appropriate antibiotic therapy Pryluck DS et al. Percutaneous drainage of aortic aneurysm sac abscesses following endovascular aneurysm repair.Vasc Endovascular Surg.2010 Deshmukh H. et al. Percutaneous management of complications (aortoenteric fistula and sac abscess) following bypass surgery for abdominal aortic aneurysm.Cardiovasc Intervent Radiol. 2007 S.J. Hulin* and G.E. Morris .Eur J Vasc Endovasc Surg .2007
 following bypass surgery for abdominal aortic aneurysm.Cardiovasc Intervent Radiol S.J. Hulin* and G.E. Morris .Eur J Vasc Endovasc Surg")
36
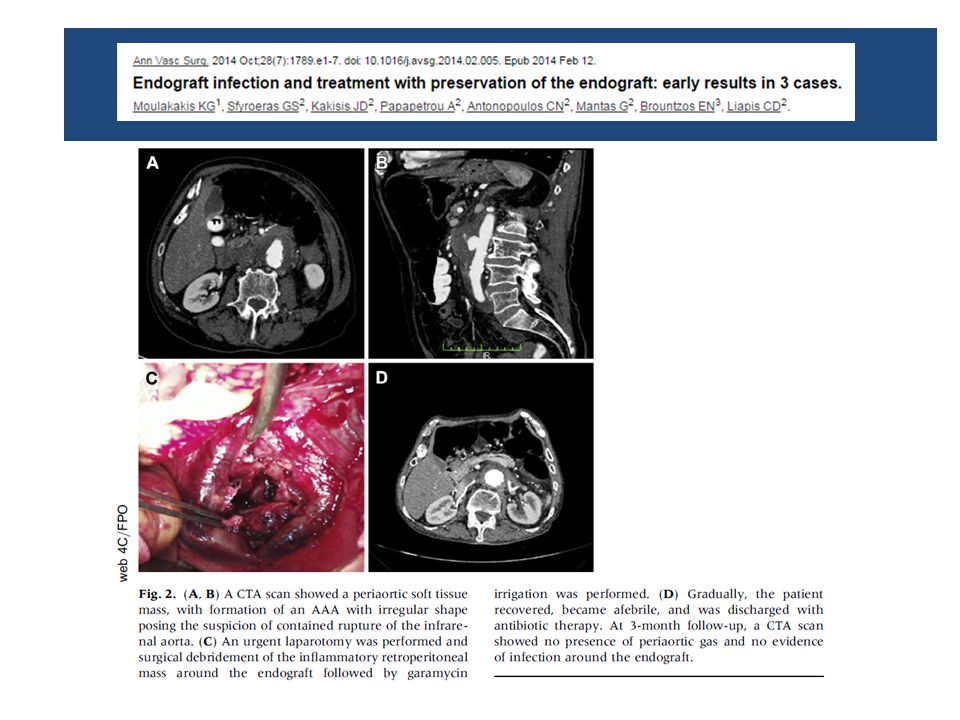
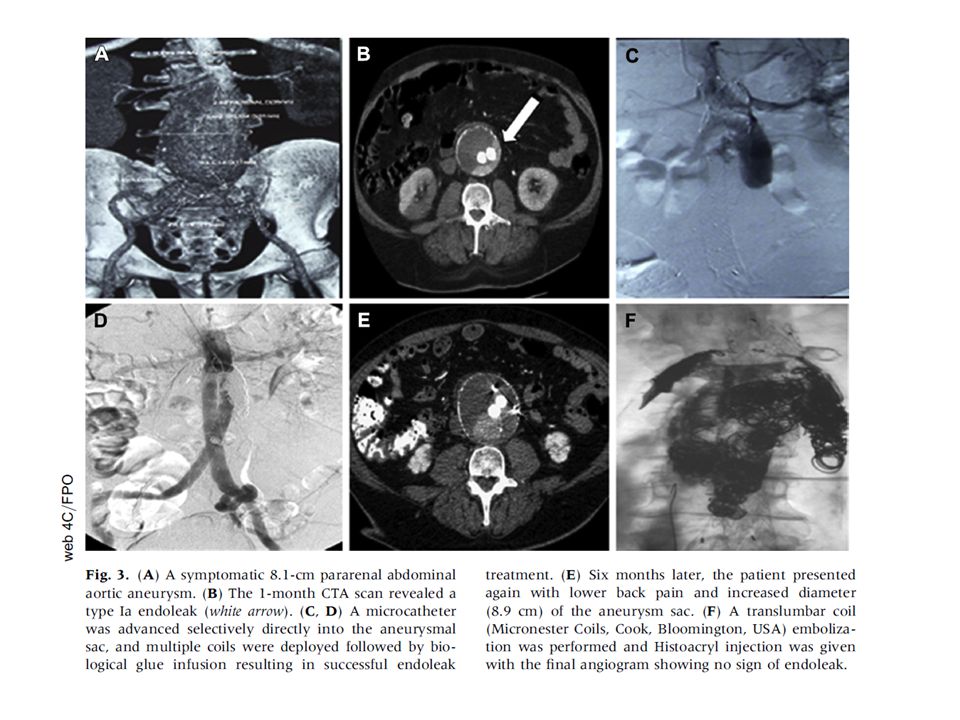
Symptomatic 8.1 cm pararenal abdominal aortic aneurysm
CASE 1 A 63-year old man, smoker Hostile abdomen Previous MI AF under oral anticoagulants COPD Severe obesity (BMI: 36.6) EVAR 1 month CT type-Ia endoleak multiple coils were deployed followed by biological glue infusion resulting in successful type Ia endoleak treatment….BUT
 EVAR. 1 month CT type-Ia endoleak. multiple coils were deployed followed by biological glue infusion resulting in successful type Ia endoleak treatment….BUT.")
37
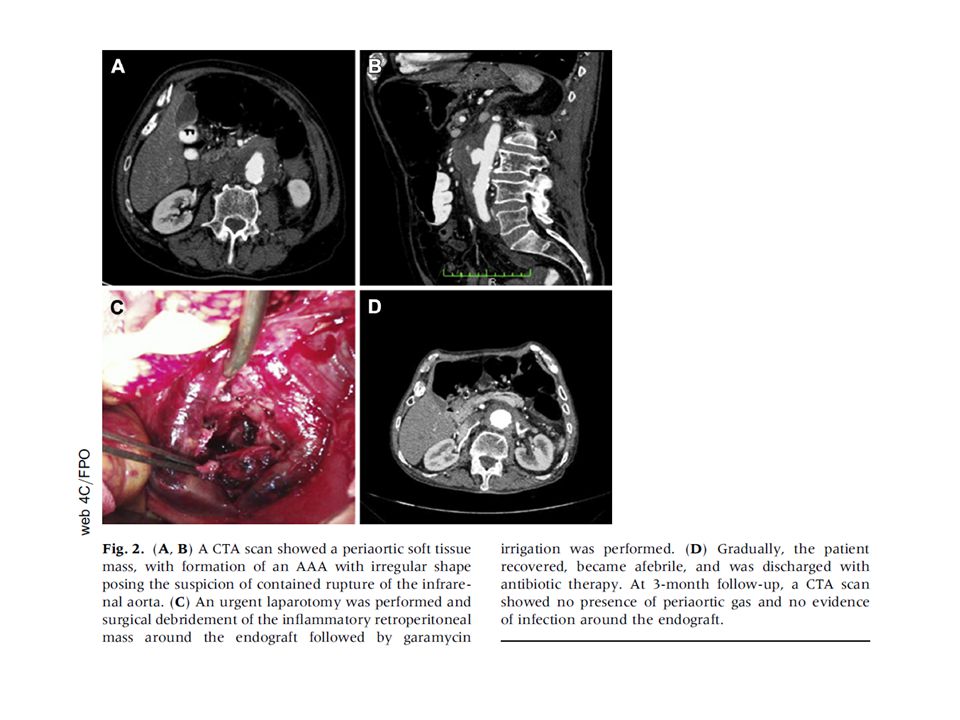
Eight months later…. Endograft Infection Fever up to 39,4 C
Lower back Pain Leucocytosis Increased CRP CTA Presence of air in the aneurysm sac cavity Blood Cultures: E.Coli and Ent. Faecalis Endograft Infection

38
Mini-Laparotomy : Sigmoid detached from the inflammatory mass, omentoplasty.
Percutaneous continuous drainage of aortic aneurysm sac abscess for 15 days CT- guided percutaneous continuous drainage followed by Vancomycin intrasac administration for 15 days Oral administration of moxifloxacin ( 400 mg daily dose x 30d)
")
39
Follow-up at 18 months CTA : No presence of air in the sac cavity
Decrease of aneurysm sac diameter Patient remains asymptomatic, afebrile. WBC : 5.300, CRP:9

40
Management of Infected Endograft in High Risk patients for open repair
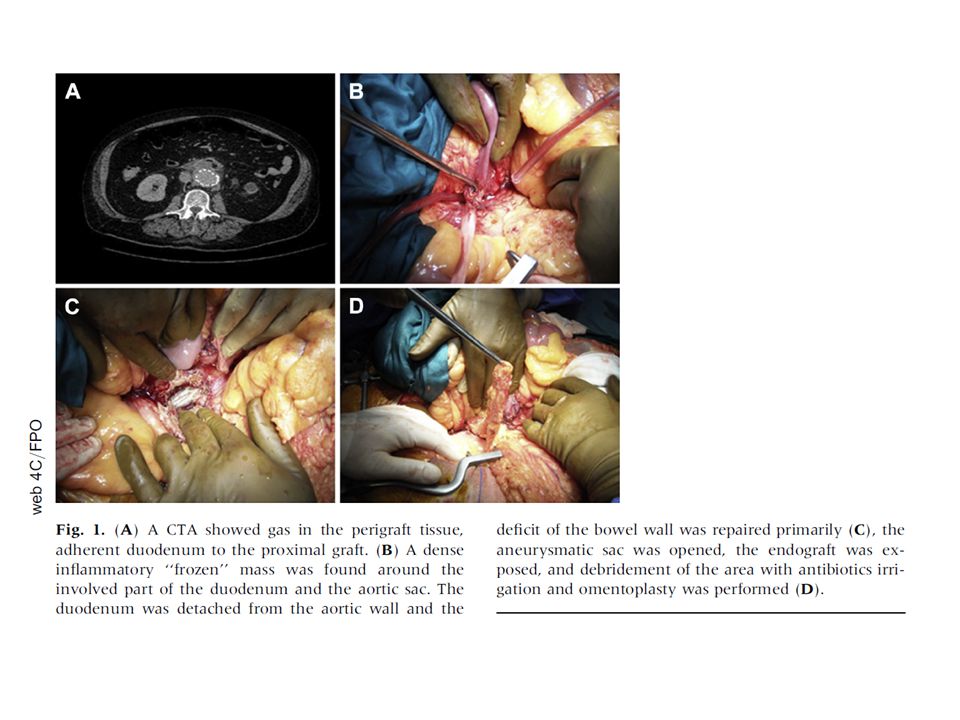
63-year old man Infection 3 years after EVAR. Patient presented unstable, with sepsis and massive bleeding due to AEF CASE 2 Excision of the eroded part of the duodenum or the bowel and interposition of the omentum, without further aortic reconstruction, followed by antibiotic therapy.

41
interposition of the omentum, without further aortic reconstruction
Patient died on 3rd postoperative day due to MOF

42
Πρόγνωση Θνητότητας λόγω Μόλυνσης του Ενδομοσχεύματος
Fungal or gram negative species Presentation with severe sepsis AEF Bleeding requiring massive transfusion Advanced ASA physical status Age > 65 Renal insufficiency Stableford J. Endograft Infection after EVAR. October 2009

43
Ανασκόπηση της Βιβλιογραφίας
129 reported cases (36 post TEVAR, 93 post EVAR) Range of endograft infection 0.2-3% Mean Time to presentation 15.4 m (1-96 m) 33% Early < 4months % > 4 months Numan F. et al. Management of endograft infections. J Cardiovasc Surg Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg. 2010 Cernohorsky P.,JVS 2011
 Range of endograft infection 0.2-3% Mean Time to presentation 15.4 m (1-96 m) 33% Early < 4months - 67% > 4 months. Numan F. et al. Management of endograft infections. J Cardiovasc Surg Setacci C. et al. Management of abdominal endograft infection. J Cardiovasc Surg Cernohorsky P.,JVS")
44
Ανασκόπηση της Βιβλιογραφίας (Σειρές ≥ 3pts)
Author Pts Type of Endograft Procedure Schlensak C., JVS 2001 5 Stentor 2, Vanguard 3 EVAR Eggebrecht H., JEVT 2004 3 N.D. TEVAR Sharif MA, JVS 2007 6 Zenith 4, Talent 2 Brown KE.,JVS 2008 TAG 5, Cuff 1 Girdauskas E,J.Thor.Card.Surg. 2008 4 Sarantzis N., JEVT 2008 Ebdofit 3, Anaconda 1, Powerlink 1 Heyer KS, JVIR 2009 10 TAG 4, Excluder 3, Zenith 2, Ancure 1 5 EVAR 5 TEVAR Kelso RL, JVS 2009 Excluder 2, AneuRx 1, Ancure 1 Chiesa R.,J.Card.Surg.2010 7 Zenith 3, Endofit 1, TAG 1, Relay 1, N.D. 1 Cernohorsky P.,JVS 2011 12 Zenith 3, Talent 9 2 TEVAR/ 10 EVAR

45
3/4 pts treated conservatively
Author Pts Management Mortality Schlensak C. 5 Stent Removal and Extra-an. BP (5) Not Described Eggebrecht H. 3 Conservative (3) 100% Sharif MA 6 Stent Removal and Extra-an. BP (3) Conservative (2) None (Early Death) (1) 50% Brown KE. Stent Removal and Extra-an. BP (1) Conservative (1) Unknown (4) 66.6% Girdauskas E 4 Stent Removal and reconstruction (4) 25% Sarantzis N. None (Early Death) (2) 60% Heyer KS 10 Conservative (4) Stent Removal and reconstruction (3) 30% 3/4 pts treated conservatively Kelso RL Stent Removal and Extra-an. BP (2) Stent Removal and aortobifemoral (1) Inraoperative Death (1) 1 Death 3 Lost in FU Chiesa R. 7 Stent Removal and reconstruction (2) Conservative (1) None (periop. Death) (3) 71% Cernohorsky P. 12 Surgical Repair (6) Conservative (6)
 Not Described. Eggebrecht H. 3. Conservative (3) 100% Sharif MA. 6. Stent Removal and Extra-an. BP (3) Conservative (2) None (Early Death) (1) 50% Brown KE. Stent Removal and Extra-an. BP (1) Conservative (1) Unknown (4) 66.6% Girdauskas E. 4. Stent Removal and reconstruction (4) 25% Sarantzis N. None (Early Death) (2) 60% Heyer KS. 10. Conservative (4) Stent Removal and reconstruction (3) 30% 3/4 pts treated conservatively. Kelso RL. Stent Removal and Extra-an. BP (2) Stent Removal and aortobifemoral (1) Inraoperative Death (1) 1 Death. 3 Lost in FU. Chiesa R. 7. Stent Removal and reconstruction (2) Conservative (1) None (periop. Death) (3) 71% Cernohorsky P. 12. Surgical Repair (6) Conservative (6)")
46
Review of the literature Clinical Outcomes in 102 pts
Overall Mortality 40.1% TEVAR 64.7%, EVAR 30.1% TEVAR EVAR Surgical Treat. Conservative Mortality (8/17) 47.1% (7/10) 70% 17/ % (4/6) 66.6% Numan F. et al. Management of endograft infections. J Cardiovasc Surg
 47.1% (7/10) 70% 17/ % (4/6) 66.6% Numan F. et al. Management of endograft infections. J Cardiovasc Surg")
47
Review of the literature Clinical Outcomes in 102 pts
EVAR- Surgical Repair Overall Mortality (17/60) 28.3% aorta ligation and extra anatomic BP (42) - Mortality (13/42) : 30.9% In situ reconstruction (18) - Mortality ( 4 /18) : 22.2% TEVAR - Surgical Repair Thor. aorta ligation and extra-anatom. BP (5) In situ reconstruction (9) Esophageal or bronchial repair (3) Overall Mortality (8/17) 47.1%
 28.3% aorta ligation and extra anatomic BP (42) - Mortality (13/42) : 30.9% In situ reconstruction (18) - Mortality ( 4 /18) : 22.2% TEVAR - Surgical Repair. Thor. aorta ligation and extra-anatom. BP (5) In situ reconstruction (9) Esophageal or bronchial repair (3) Overall Mortality (8/17) 47.1%")
52
Μόλυνση Ενδομοσχεύματπος μετά από EVAR

53
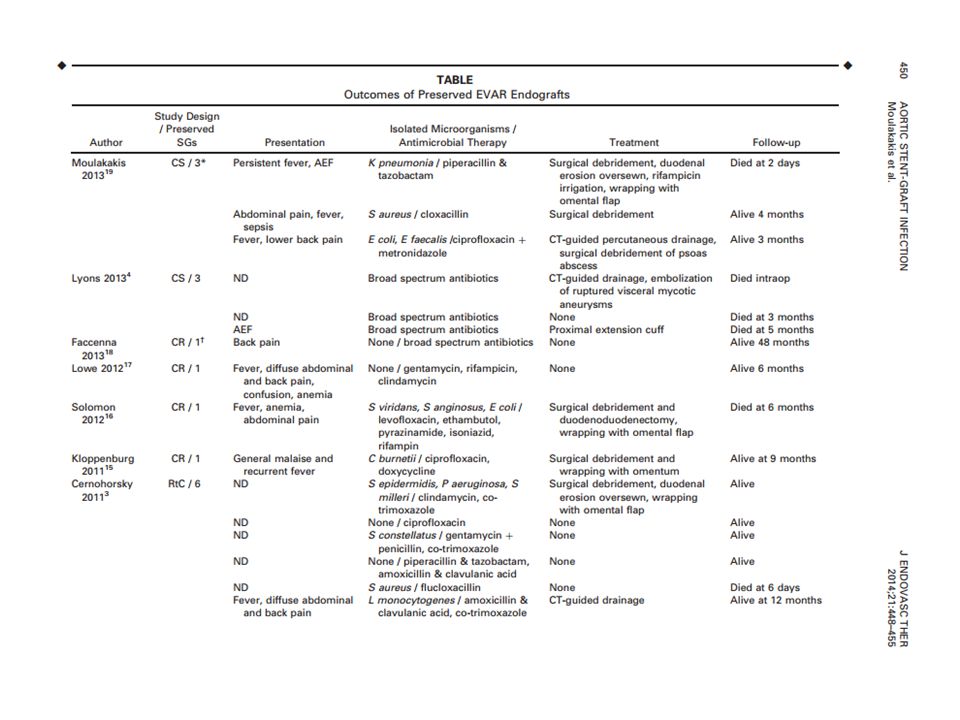
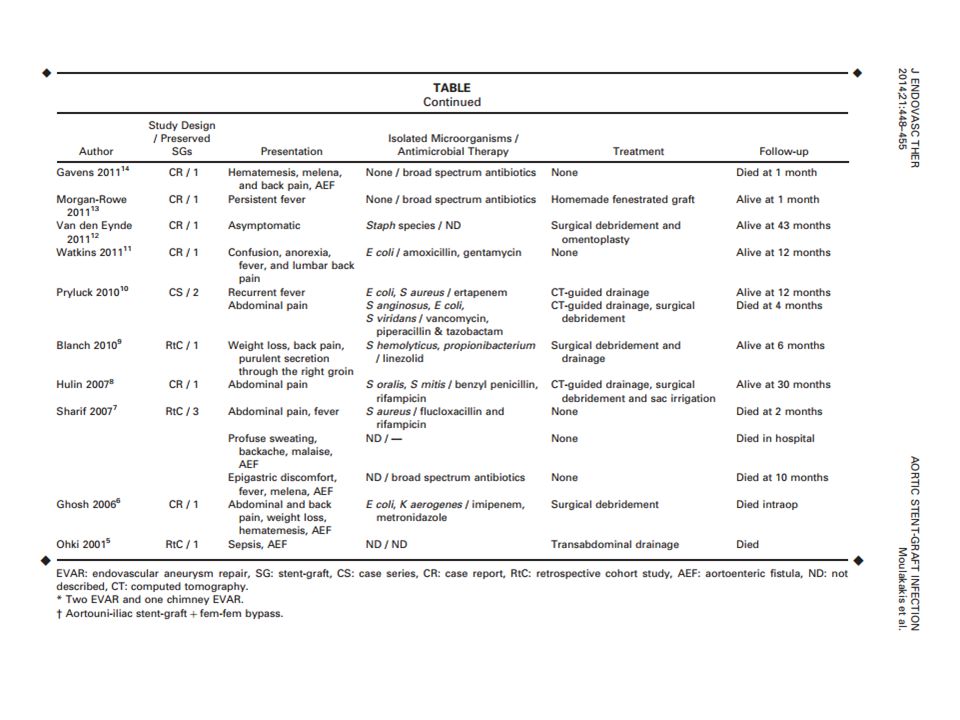
N of patients treated with endograft preservation
Author Study design Type of procedure N of patients treated with endograft preservation Moulakakis et al, case series 2EVAR, 1ch-EVAR 3 Lyons et al, 20134 EVAR Faccenna et al, case report AUI + fem-fem 1 Lowe et al, Solomon et al, Kloppenburg et al,201116 Cernohorsky et al, 20113 Retr. cohort study 6 Gavens et al, EVAR/TEVAR Morgan-Rowe et al, FEVAR Van den Eynde et al, Watkins et al, Pryluck et al, 2 Blanch et al, Saleem et al, 20089 Hulin et al,20078 Sharif et al, 20077 Ghosh et al, 20066 Ohki et al, 20015 Total 30

54
Μόλυνση Ενδομοσχεύματπος μετά από EVAR
Number of patients 30 Gender (%male) 94 Age (years, mean ± SE) 72.8 ±8.4 Setting of the EVAR procedure ● Elective (%) ● Emergent (%) 82 18 Reintervention (%) 13 Time to infection (mean, days) 360±81
 94. Age (years, mean ± SE) 72.8 ±8.4. Setting of the EVAR procedure. ● Elective (%) ● Emergent (%) Reintervention (%) 13. Time to infection (mean, days) 360±81.")
58
Infected Endograft as “bridging “ procedure after Aortoenteric Fistula

60
Μόλυνση Ενδομοσχεύματπος μετά από TEVAR
Author Study design Type of procedure N of patients Lyons et al, 20132 Retr. cohort study TEVAR 9 Muradi et al, 20133 case report 1 Akkoyunlu et al, 20124 Cernohorsky et al, 20115 2 Motloch et al, 20116 elephant trunk Numan et al, 20117 Ishikawa et al, Gavens et al, 20119 Chiesa et al, 16 d'Ettorre et al, Eggebrecht et al, 5 Isasti et al, Heyer et al, 4 Martens et al, Bockler et al, Czerny et al, Total 47

61
Preservation of Endograft Number of patients 47 Gender (%male) 75 Age (mean, years) 69.3 (95% CI 66.5 to 72.1) Setting of the procedure Elective (%) Emergent (%) 76 24 Indication for TEVAR Atherosclerotic aneurysm 55.3% Aortic dissection 17.0% Pseudoaneurysm following open aortic repair 14.9% Mycotic aneurysm 6.4% Secondary AEF following open repair 4.2% Cutaneous left subclavian aneurysm fistula following radiotherapy 2.1% Time to infection (mean, days) 292.5 (95%CI to 406.2)
 Emergent (%) Indication for TEVAR. Atherosclerotic aneurysm. 55.3% Aortic dissection. 17.0% Pseudoaneurysm following open aortic repair. 14.9% Mycotic aneurysm. 6.4% Secondary AEF following open repair. 4.2% Cutaneous left subclavian aneurysm fistula following radiotherapy. 2.1% Time to infection (mean, days) (95%CI to 406.2)")
62
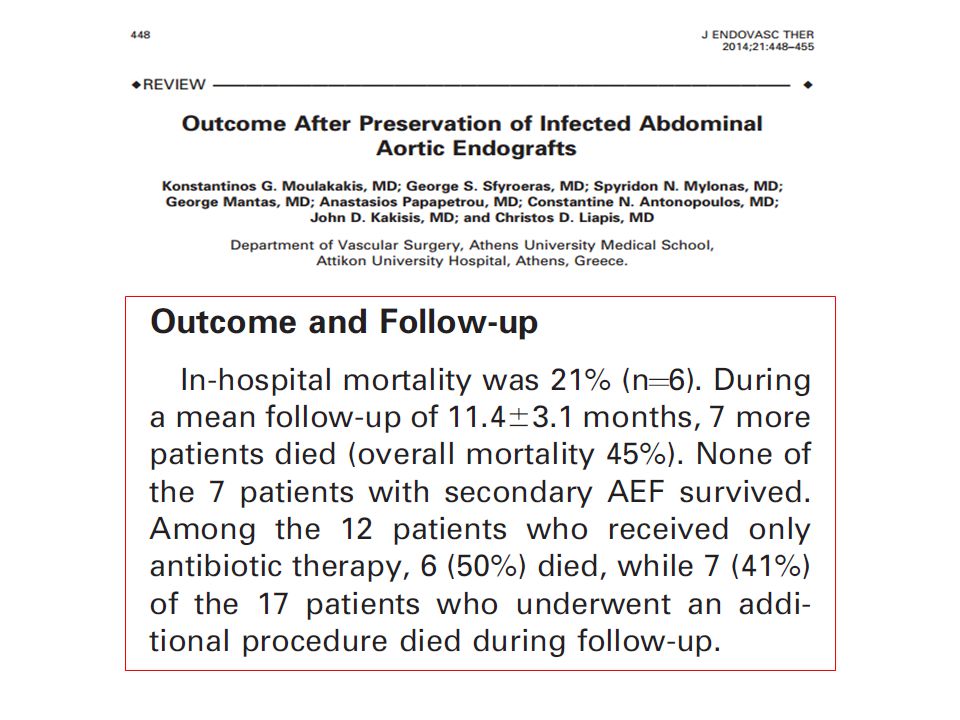
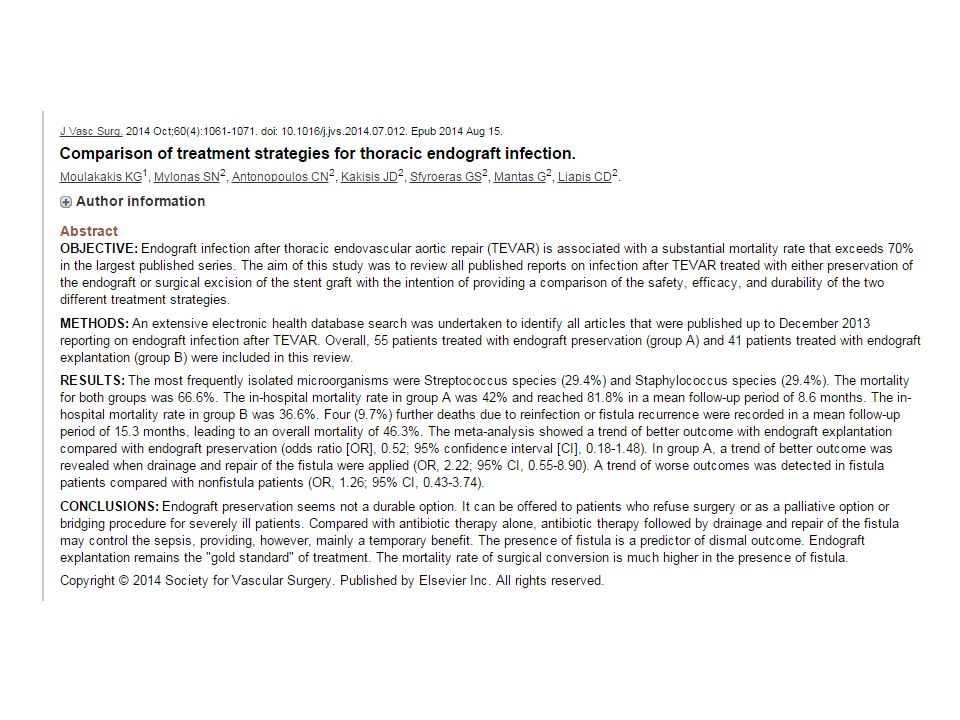
The in-hospital mortality rate in group A was 42% and reached 81
The in-hospital mortality rate in group A was 42% and reached 81.8% in a mean follow-up period of 8.6 months. The in-hospital mortality rate in group B was 36.6%. Four (9.7%) further deaths due to reinfection or fistula recurrence were recorded in a mean follow-up period of 15.3 months, leading to an overall mortality of 46.3%. Endograft preservation seems not a durable option. It can be offered to patients who refuse surgery or as a palliative option or bridging procedure for severely ill patients.
 further deaths due to reinfection or fistula recurrence were recorded in a mean follow-up period of 15.3 months, leading to an overall mortality of 46.3%. Endograft preservation seems not a durable option. It can be offered to patients who refuse surgery or as a palliative option or bridging procedure for severely ill patients.")
63
Μόλυνση Ενδομοσχεύματος - Συμπεράσματα
Η ανοικτή αποκατάσταση αποτελεί gold standard σε ασθενείς με προσδόκιμο επιβίωσης, που συνοδεύεται με υψηλή θνητότητα 15-40% . (Υπάρχει πάντα κίνδυνος για υποτροπή της σήψης) Η συντηρητική αντιμετώπιση με παροχέτευση και διατήρηση του μοσχεύματος θα πρέπει να γίνεται σε υψηλού χειρουργικού κινδύνου ασθενείς που δεν μπορούν να υποβληθούν σε ανοικτή επέμβαση Η παροχέτευση και ο συνοδός χειρουργικός καθαρισμός έχουν καλύτερα αποτελέσματα σε σχέση με την αντιβιωτική αγωγή από μόνη της. Η παρουσία επικοινωνίας, εκτεταμένης φλεγμονής-σήψης, είναι αρνητικός προγνωστικός παράγοντας για συντηρητική αντιμετώπιση με διατήρηση του μοχεύματος. Σε συντηρητική αντιμετώπιση συνιστάται αντιβιωτική αγωγή εφ’ όρου ζωής
 Η συντηρητική αντιμετώπιση με παροχέτευση και διατήρηση του μοσχεύματος θα πρέπει να γίνεται σε υψηλού χειρουργικού κινδύνου ασθενείς που δεν μπορούν να υποβληθούν σε ανοικτή επέμβαση. Η παροχέτευση και ο συνοδός χειρουργικός καθαρισμός έχουν καλύτερα αποτελέσματα σε σχέση με την αντιβιωτική αγωγή από μόνη της. Η παρουσία επικοινωνίας, εκτεταμένης φλεγμονής-σήψης, είναι αρνητικός προγνωστικός παράγοντας για συντηρητική αντιμετώπιση με διατήρηση του μοχεύματος. Σε συντηρητική αντιμετώπιση συνιστάται αντιβιωτική αγωγή εφ’ όρου ζωής.")
64
Μόλυνση Ενδομοσχεύματος - Συμπεράσματα
5. Στην μόλυνση μετα από TEVAR, η διατήρηση του μοσχεύματος έχει εξαιρετικά απογοητευτικά αποτελέσματα 6. Όταν συνυπάρχει επικοινωνία η ενδαγγειακή αποκατάσταση συνίσταται για τον έλεγχο της αομορραγίας, την βελτίωση της γενικής κατάστασης του ασθενή και σαν γέφυρα για μελλοντική εξαίρεση του μοσχεύματος.

Παρόμοιες παρουσιάσεις





 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")


















