Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Διαβητικός ασθενής με νεφρολογικά προβλήματα
Κωνσταντίνος Μακρυλάκης Αναπληρωτής Καθηγητής ΕΚΠΑ Α’ Προπαιδευτική Παθολογική Κλινική & Διαβητολογικό Κέντρο ΓΝΑ Λαϊκό Φάνης Αποστόλου Δ/ντής ΕΣΥ Νεφρολογικό Τμήμα ΓΝΑ «Ο Ευαγγελισμός»

2
Περίπτωση 1η ACR: 45 mg/g κρεατινίνης
Άνδρας 62 ετών, με ΣΔ2 από 8ετίας Προσέρχεται για «2η γνώμη» ΣΒ: 91 kg, ΔΜΣ: 30,1 kg/m2, ΑΠ: 122/78 mmHg Θεραπεία με μετφορμίνη (1000 mgx2) + DPP-4 αναστολέα HbA1c: 8,3% Αρχόμενη αμφιβλ/θεια υποστρώματος Λευκωματίνη/κρεατινίνη ούρων σε τυχαίο δείγμα: ACR: 45 mg/g κρεατινίνης Υπερχοληστερολαιμία (παίρνει στατίνη –> LDL-C:98 mg/dl) Γενική αίματος, τρανσαμινάσες, γενική ούρων: κφ Ουρία: 32 mg/dl, κρεατινίνη: 1,3 mg/dl
 + DPP-4 αναστολέα. HbA1c: 8,3% Αρχόμενη αμφιβλ/θεια υποστρώματος. Λευκωματίνη/κρεατινίνη ούρων σε τυχαίο δείγμα: ACR: 45 mg/g κρεατινίνης. Υπερχοληστερολαιμία (παίρνει στατίνη –> LDL-C:98 mg/dl) Γενική αίματος, τρανσαμινάσες, γενική ούρων: κφ. Ουρία: 32 mg/dl, κρεατινίνη: 1,3 mg/dl.")
3
Περίπτωση 1η Ο οικογενειακός του ιατρός του είπε ότι έχει μικρολευκωματινουρία (άρα νεφροπάθεια) Επομένως του συνέστησε να διακόψει τη μετφορμίνη και να αρχίσει ινσουλίνη ACR: 45 mg/g κρεατινίνης

4
Ερώτηση Έχει μικρολευκωματινουρία; Έχει νεφροπάθεια;
Ναι Όχι Έχει νεφροπάθεια; Πρέπει να διακόψει τη μετφορμίνη;

5
Ερώτηση Έχει μικρολευκωματινουρία; Έχει νεφροπάθεια;
Ναι Όχι Έχει νεφροπάθεια; Πρέπει να διακόψει τη μετφορμίνη;

6
ΑΛΒΟΥΜΙΝΟΥΡΙΑ

7
ΠΟΣΟΤΙΚΟΣ ΠΡΟΣΔΙΟΡΙΣΜΟΣ ΛΕΥΚΩΜΑΤΙΝΗΣ ΟΥΡΩΝ
Κατηγορία 24ωρη συλλογή (mg/24h) 8ωρη συλλογή (μg/min) Τυχαία συλλογή (mg/g κρ.) Φυσιολογικές τιμές <30 <20 Μικρολευκωματινουρία 30-300 Κλινική λευκωματινουρία >300 >200
 8ωρη συλλογή. (μg/min) Τυχαία συλλογή. (mg/g κρ.) Φυσιολογικές τιμές. <30. <20. Μικρολευκωματινουρία Κλινική λευκωματινουρία. >300. >200.")
8
ΛΟΓΟΣ ΛΕΥΚΩΜΑΤΙΝΗΣ/ΚΡΕΑΤΙΝΙΝΗ ΣΕ ΤΥΧΑΙΟ ΔΕΙΓΜΑ ΟΥΡΩΝ (ACR):
ΛΕΥΚΩΜΑΤΙΝΟΥΡΙΑ ΛΟΓΟΣ ΛΕΥΚΩΜΑΤΙΝΗΣ/ΚΡΕΑΤΙΝΙΝΗ ΣΕ ΤΥΧΑΙΟ ΔΕΙΓΜΑ ΟΥΡΩΝ (ACR): < 30 mg/g: Φυσιολογικό mg/g: Μικρολευκωματινουρία (Μικροαλβουμινουρία) >300 mg/g: Έκδηλη λευκωματουρία
: < 30 mg/g: Φυσιολογικό mg/g: Μικρολευκωματινουρία. (Μικροαλβουμινουρία) >300 mg/g: Έκδηλη λευκωματουρία.")
9
ΛΟΓΟΣ ΑΛΒΟΥΜΙΝΗΣ/ΚΡΕΑΤΙΝΙΝΗ ΣΕ ΤΥΧΑΙΟ ΔΕΙΓΜΑ ΟΥΡΩΝ
Φυσιολογική απέκκριση αλβουμίνης σε 24 hrs: <30 mg Φυσιολογική απέκκριση κρεατινίνης σε 24 hrs: ~1 g (15-20 mg/kg Γ, mg/kg A) Ανώτερος Φυσιολογικός λόγος Αλβουμίνης/Κρεατινίνη: 30 mg/1 g=30 mg/g Έκδηλη πρωτεϊνουρία: 300/1=300 mg/g
 Ανώτερος Φυσιολογικός λόγος Αλβουμίνης/Κρεατινίνη: 30 mg/1 g=30 mg/g. Έκδηλη πρωτεϊνουρία: 300/1=300 mg/g.")
10
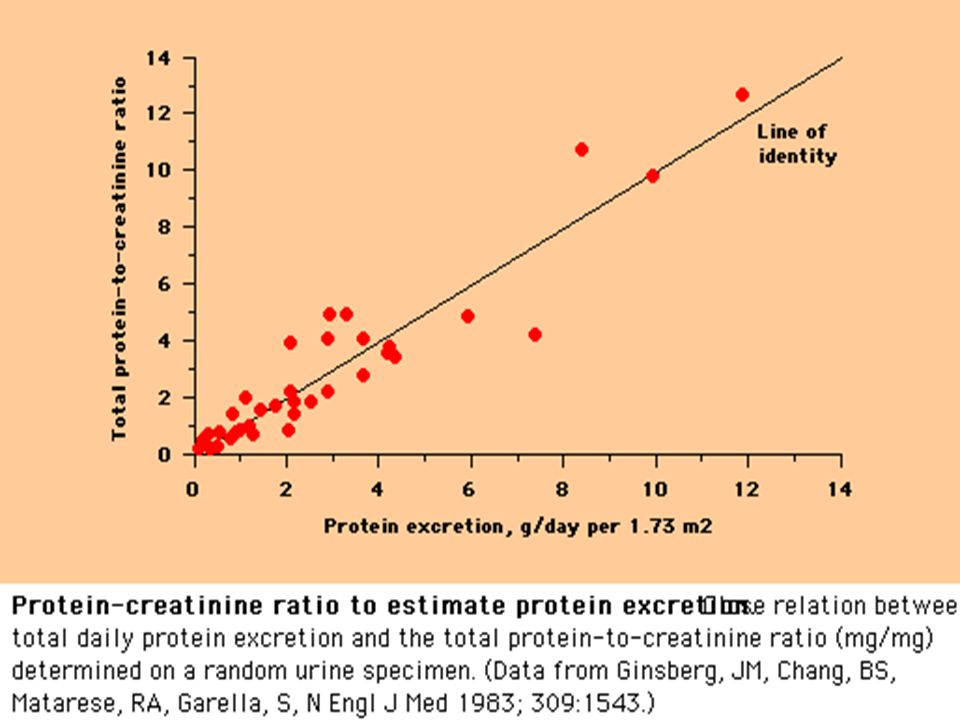
ΛΟΓΟΣ ΠΡΩΤΕΪΝΗΣ/ΚΡΕΑΤΙΝΙΝΗ ΣΕ ΤΥΧΑΙΟ ΔΕΙΓΜΑ ΟΥΡΩΝ:
ΠΡΩΤΕΪΝΟΥΡΙΑ ΛΟΓΟΣ ΠΡΩΤΕΪΝΗΣ/ΚΡΕΑΤΙΝΙΝΗ ΣΕ ΤΥΧΑΙΟ ΔΕΙΓΜΑ ΟΥΡΩΝ: < 0.3: Φυσιολογικό : Πρωτεϊνουρία >3.0: Νεφρωσικό σύνδρομο

12
There is also an association of cardiovascular morbidity and mortality with microalbuminuria in patients with type 2 DM. This slide shows the odds ratios of cardiovascular morbidity and mortality in patients with type 2 DM with albuminuria versus those who had normal albumin excretion. In the top portion of this slide are data from five old studies that show this increase in cardiovascular mortality odds ratio in 4 of the 5 studies, then a subtotal and then a 6th study by Macleod et al., in 1995, that also shows a substantial increase. So that overall there is about a two-fold increase in cardiovascular morbidity and mortality in patients who have elevated levels of urinary albumin.

13
ΣΤΑΔΙΑ ΧΡΟΝΙΑΣ ΝΕΦΡΙΚΗΣ ΝΟΣΟΥ (ΧΝΝ) < 15 ή εξωνεφρική κάθαρση
Στάδιο Περιγραφή ΣΔ (ml/min/1,73m2) 1 Νεφρική βλάβη με φυσιολογική ή ΣΔ 90 2 Νεφρική βλάβη με ήπια ΣΔ 60-89 3α 3β Μέτρια ΣΔ 59-45 44-30 4 Σοβαρή ΣΔ 15-29 5 Νεφρική ανεπάρκεια < 15 ή εξωνεφρική κάθαρση
 1. Νεφρική βλάβη με φυσιολογική ή ΣΔ. Νεφρική βλάβη με ήπια ΣΔ α. 3β. Μέτρια ΣΔ Σοβαρή ΣΔ Νεφρική ανεπάρκεια. < 15 ή εξωνεφρική κάθαρση.")
14
Πρόγνωση ΧΝΝ με εκτίμηση ΣΔ και κατηγορία λευκωματινουρίας

15
Οι τρέχουσες θεραπείες στο ΣΔτ2 έχουν όρια όταν η νεφρική λειτουργία μειώνεται
3α 3β 4 5 Ινσουλίνη Ενέσιμα Λιραγλουτίδη Eξενατίδη Λιναγλιπτίνη Σιταγλιπτίνη Βιλνταγλιπτίνη Σαξαγλιπτίνη Μετφορμίνη Δισκία Ακαρβόζη Ρεπαγλινίδη Γλιμεπιρίδη Γλικλαζίδη Πιογλιταζόνη 45 90 60 30 15 ΧΝΑΤΣ GFR Schernthaner G, et al. Nephrol Dial Transplant. 2011;26(2):454–7 and respective EMEA SmPCs , . Deacon CF. Diabetes, Obes Metab. 2011;13(1):7–18
:454–7 and respective EMEA SmPCs , . Deacon CF. Diabetes, Obes Metab. 2011;13(1):7–18.")
16
Υπολογισμός σπειραματικής διήθησης (ml/min)
(140 - ηλικία) x ΒΣ (Kg) ( ή ) x κρεατ. (mg/dl)
 x ΒΣ (Kg) (72 ή 85) x κρεατ. (mg/dl)")
17
Υπολογισμός σπειραματικής διήθησης (ml/min)
( ) x 91 (Kg) ( x 1,3 (mg/dl) eGFR = 76 ml/min
 x 91 (Kg) (72 x 1,3 (mg/dl) eGFR = 76 ml/min.")
18
GFR Prediction Equations
Cockcroft-Gault formula Ccr (ml/min) = 1.23 x (140-age) x weight/Pcr (x 0.85 if female) MDRD Study equation GFR (ml/min/1.73 m2) = 186 x [(Pcr)/88.4] x (age) x (0.742 if female) x (1.210 if African American) Cockcroft & Gault. Nephron 1976; 16: 31-41 Levey AS, et al. Ann Intern Med 1999;130:
 = 1.23 x (140-age) x weight/Pcr. (x 0.85 if female) MDRD Study equation. GFR (ml/min/1.73 m2) = 186 x [(Pcr)/88.4] x (age) x (0.742 if female) x (1.210 if African American) Cockcroft & Gault. Nephron 1976; 16: Levey AS, et al. Ann Intern Med 1999;130:")
19
CKD EPI & MDRD GFR equation
4 variable MDRD CKD EPI Equation (with SI Units) using standardized serum creatinine, age, race, gender by Stephen Z. Fadem, M.D., FACP, FASN and Brian Rosenthal
 using standardized serum creatinine, age, race, gender. by Stephen Z. Fadem, M.D., FACP, FASN and Brian Rosenthal.")
20
Οι τρέχουσες θεραπείες στο ΣΔτ2 έχουν όρια όταν η νεφρική λειτουργία μειώνεται
3α 3β 4 5 Ινσουλίνη Ενέσιμα Λιραγλουτίδη Eξενατίδη Λιναγλιπτίνη Σιταγλιπτίνη Βιλνταγλιπτίνη Σαξαγλιπτίνη Μετφορμίνη Δισκία Ακαρβόζη Ρεπαγλινίδη Γλιμεπιρίδη Γλικλαζίδη Πιογλιταζόνη 45 90 60 30 15 ΧΝΑΤΣ GFR Schernthaner G, et al. Nephrol Dial Transplant. 2011;26(2):454–7 and respective EMEA SmPCs , . Deacon CF. Diabetes, Obes Metab. 2011;13(1):7–18
:454–7 and respective EMEA SmPCs , . Deacon CF. Diabetes, Obes Metab. 2011;13(1):7–18.")
21
Ερώτηση Έχει μικρολευκωματινουρία; Έχει νεφροπάθεια;
Ναι (ACR: 45 mg αλβουμίνης /g κρεατινίνης) Όχι Έχει νεφροπάθεια; Ναι (eGFR: 76 ml/min -> στάδιο 2 ΧΝΝ) Πρέπει να διακόψει τη μετφορμίνη; Ναι Όχι (έχει ένδειξη έως GFR>30 ml/min)
 Όχι. Έχει νεφροπάθεια; Ναι (eGFR: 76 ml/min -> στάδιο 2 ΧΝΝ) Πρέπει να διακόψει τη μετφορμίνη; Ναι. Όχι (έχει ένδειξη έως GFR>30 ml/min)")
22
Ερώτηση Τι θεραπεία θα δώσουμε για τη μικρολευκωματινουρία;
Τι θεραπεία θα δώσουμε για τη μικρολευκωματινουρία; Ο ασθενής μας δεν είναι υπερτασικός!!

23
Ερώτηση Τι θεραπεία θα δώσουμε για τη μικρολευκωματινουρία; αΜΕΑ ΑRB
Τι θεραπεία θα δώσουμε για τη μικρολευκωματινουρία; αΜΕΑ ΑRB b-blocker Διουρητικά CCBs

24
Περίπτωση 2η Γυναίκα 39 χρόνων με ΣΔ 1 από 15ετίας, e-GFR 54
Προσέρχεται για κόπωση, αδυναμία, οίδημα, εξάνθημα κ.α. Λευκωματουρία νεφρωσικού εύρους (>3.5 γ/ημ) Αναιμία (Ht 24% Hb 8,2) Πυρετός, εξάνθημα, μείωση νεφρικής λειτουργίας (eGFR 35) ΑΠ 160/100 mm Hg Ήπιες ατροφικές αλλοιώσεις κ.α. Ιστορικό Laser εφαρμογής στα μάτια U/S νεφρών ήπια αύξηση ηχογένειας, οριακό μέγεθος
 Αναιμία (Ht 24% Hb 8,2) Πυρετός, εξάνθημα, μείωση νεφρικής λειτουργίας (eGFR 35) ΑΠ 160/100 mm Hg. Ήπιες ατροφικές αλλοιώσεις κ.α. Ιστορικό Laser εφαρμογής στα μάτια. U/S νεφρών ήπια αύξηση ηχογένειας, οριακό μέγεθος.")
25
Διαβητική νεφροπάθεια. Ιστορικό
Μακρά πορεία διαβήτου Αφρώδη ούρα-Λευκωματουρία Διαβητική αμφιβλ/θεια Κόπωση και οιδήματα Περιφερική αγγειακή νόσο, υπέρταση Νευροπάθεια

26
Ερώτηση 1. Τι σκεπτόμαστε;
Πρόοδος διαβητικής νεφροπάθεας Οξεία σωληναριακή νέκρωση Άλλη νεφροπάθεια

27
Διαφοροδιαγνωστικά στοιχεία ενδεικτικά νεφροπάθειας μη διαβητικής αιτιολογίας
Παθολογικό ίζημα ούρων (αιματουρία, πυουρία, δύσμορφα ερυθρά, ερυθροκυτταρικοί κύλινδροι) Απουσία διαβητικής αμφιβληστροειδοπάθειας Ταχεία επιδείνωση πρωτεϊνουρίας Ταχεία άνοδος της κρεατινίνης του ορού Άτυπες υπερηχογραφικές αλλοιώσεις των νεφρών Διάρκεια του ΣΔ τύπου 1 λιγότερο από 5 χρόνια
 Απουσία διαβητικής αμφιβληστροειδοπάθειας. Ταχεία επιδείνωση πρωτεϊνουρίας. Ταχεία άνοδος της κρεατινίνης του ορού. Άτυπες υπερηχογραφικές αλλοιώσεις των νεφρών. Διάρκεια του ΣΔ τύπου 1 λιγότερο από 5 χρόνια.")
28
Διαφορική διάγνωση σε ασθενή με λευκωματουρία και διαβήτη άγνωστης έναρξης
Νόσος ελαφρών αλύσεων Πολλαπλούν μυέλωμα Διάμεση νεφρίτις Νεφροσκλήρυνση Στένωση νεφρικής αρτηρίας Νεφραγγειακή υπέρταση Θρόμβωση νεφρικής φλέβας Άλλη νεφροπάθεια Εργαστηριακά εστάλησαν, αποκλείστηκε η θρόμβωση, αιμάτωση νεφρών φυσιολογική, αύξηση ηχογένειας νεφρών Έγινε Βιοψία νεφρού αφού διορθώθηκε η ΑΠ)
")
29
Διαβητική Νεφροπάθεια
Διαβητική Νεφροπάθεια. Διάχυτη και οζώδης υπερπλασία του μεσαγγείου, πάχυνση των τριχοειδικών τοιχωμάτων, εναποθέσεις υαλοειδούς ουσίας στους τριχοειδικούς αυλούς και υπερπλασία τοιχώματος αρτηριδίων. (χρώσεις Masson και PASM)
")
30
Αλλοιώσεις Εξωτριχοειδικής ΣΝ.
Τμηματικές ρήξεις τριχοειδικών τοιχωμάτων, εναποθέσεις ινικής και ανάπτυξη κυτταροβριθών μηνοειδών σχηματισμών (crescents). (χρώσεις PASM, Masson και PAS)
. (χρώσεις PASM, Masson και PAS)")
31
Figure 1. Representative examples of the morphologic lesions in DN
Glomerulus showing only mild ischemic changes, with splitting of Bowman's capsule. No clear mesangial alteration Class I, GBM thickening glomeruli with mild and moderate mesangial expansion, respectively Class II, mesangial expansion C : mesangial expansion < mean area of a capillary lumen (IIa), D: mesangial expansion > mean area of a capillary lumen (IIb). glomeruli with mild and moderate mesangial expansion, respectively Class III, nodular sclerosis E: a convincing Kimmelstiel–Wilson lesion, F: Kimmelstiel–Wilson lesion Figure 1. Representative examples of the morphologic lesions in DN. Glomerulus showing only mild ischemic changes, with splitting of Bowman's capsule. No clear mesangial alteration. (B) EM of this glomerulus: the mean width of the GBM was 671 nm (mean taken over 55 random measurements). EM provides the evidence for classifying the biopsy with only mild light microscopic changes into class I. (C, D) Class II glomeruli with mild and moderate mesangial expansion, respectively. In panel C, the mesangial expansion does not exceed the mean area of a capillary lumen (IIa), whereas in panel D it does (IIb). (E, F) In panel F is a class III Kimmelstiel–Wilson lesion. The lesion in panel E is not a convincing Kimmelstiel–Wilson lesion, therefore (on the basis of the findings in this glomerulus) the finding is consistent with class IIb. For the purpose of the classification, at least one convincing Kimmelstiel–Wilson (as in panel F) needs to be present. In panel H, signs of class IV DN consist of hyalinosis of the glomerular vascular pole and a remnant of a Kimmelstiel–Wilson lesion on the opposite site of the pole. Panel G is an example of glomerulosclerosis that does not reveal its cause (glomerulus from the same biopsy as panel H). For the purpose of the classification, signs of DN should be histopathologically or clinically present to classify a biopsy with global glomerulosclerosis in >50% of glomeruli as class IV. Class IV, advanced glomerulosclerosis G: glomerulosclerosis that does not reveal its cause H: hyalinosis of the glomerular vascular pole and a remnant of a Kimmelstiel–Wilson lesion on the opposite site of the pole, Tervaert, T. W. C. et al. J Am Soc Nephrol 2010;21: Copyright ©2010 American Society of Nephrology
, D: mesangial expansion > mean area of a capillary lumen (IIb). glomeruli with mild and moderate mesangial expansion, respectively. Class III, nodular sclerosis. E: a convincing Kimmelstiel–Wilson lesion, F: Kimmelstiel–Wilson lesion. Figure 1. Representative examples of the morphologic lesions in DN. Glomerulus showing only mild ischemic changes, with splitting of Bowman s capsule. No clear mesangial alteration. (B) EM of this glomerulus: the mean width of the GBM was 671 nm (mean taken over 55 random measurements). EM provides the evidence for classifying the biopsy with only mild light microscopic changes into class I. (C, D) Class II glomeruli with mild and moderate mesangial expansion, respectively. In panel C, the mesangial expansion does not exceed the mean area of a capillary lumen (IIa), whereas in panel D it does (IIb). (E, F) In panel F is a class III Kimmelstiel–Wilson lesion. The lesion in panel E is not a convincing Kimmelstiel–Wilson lesion, therefore (on the basis of the findings in this glomerulus) the finding is consistent with class IIb. For the purpose of the classification, at least one convincing Kimmelstiel–Wilson (as in panel F) needs to be present. In panel H, signs of class IV DN consist of hyalinosis of the glomerular vascular pole and a remnant of a Kimmelstiel–Wilson lesion on the opposite site of the pole. Panel G is an example of glomerulosclerosis that does not reveal its cause (glomerulus from the same biopsy as panel H). For the purpose of the classification, signs of DN should be histopathologically or clinically present to classify a biopsy with global glomerulosclerosis in >50% of glomeruli as class IV. Class IV, advanced glomerulosclerosis. G: glomerulosclerosis that does not reveal its cause. H: hyalinosis of the glomerular vascular pole and a remnant of a Kimmelstiel–Wilson lesion on the opposite site of the pole, Tervaert, T. W. C. et al. J Am Soc Nephrol 2010;21: Copyright ©2010 American Society of Nephrology.")
32
Normal glomerulus Light micrograph of a normal glomerulus.
There are only 1 or 2 cells per capillary tuft, the capillary lumens are open, the thickness of the glomerular capillary wall (long arrow) is similar to that of the tubular basement membranes (short arrow), and the mesangial cells and mesangial matrix are located in the central or stalk regions of the tuft (arrows). Courtesy of Helmut G Rennke.
 is similar to that of the tubular basement membranes (short arrow), and. the mesangial cells and mesangial matrix are located in the central or stalk regions of the tuft (arrows). Courtesy of Helmut G Rennke.")
33
Accumulation of extracellular DN
Simple microscope: Mesangium Expansion Diffusive Type Kimmelstiel-Wilson nodules (acellular accumulation) Thickening GBM, TBM Glomerulosclerosis diffuse mesangial hypercellularity and expansion with only small nodule formation. Periodic acid-Schiff stain, original magnification X200. Οσον αφορά στις ιστολογικές βλάβες της ΔΝ The key change in diabetic glomerulopathy is augmentation of extracellular material, that is, quantitative deviations from normal values. Thickening of the peripheral BM is the first demonstrable deviation from normal. In advanced stages, the mesangial matrix accumulation dominates the picture,45, 46 and the BM thickening from early to advanced stages is less marked. Therefore, the mesangial changes correlate more closely with the functional deterioration,46, 47 which has raised the question of whether the early BM thickening is of any clinical relevance. In comparing the different structural parameters, the precision in the individual estimates should be taken into account, and in this respect, the BM thickness has the greater advantage. In patients in the early phase of nephropathy, significant correlations have been found between BM thickness and matrix parameters,45, 48 indicating that the augmentation of extracellular material takes place in parallel at the two locations. The mesangial expansion and glomerulosclerosis do not always develop in parallel, suggesting that they may have somewhat different underlying pathogenesis [22]. GBM = glomerular basement membrane TBM = tubular basement membrane 17. Fioretto, P, Steffes, MW, Brown, DM, Mauer, SM. An overview of renal pathology in insulin-dependent diabetes mellitus in relationship to altered glomerular hemodynamics. Am J Kidney Dis 1992; 20:549. 18. Adler, S. Diabetic nephropathy: Linking histology, cell biology, and genetics. Kidney Int 2004; 66:2095. 33
 Thickening GBM, TBM. Glomerulosclerosis. diffuse mesangial hypercellularity and expansion with only small nodule formation. Periodic acid-Schiff stain, original magnification X200. Οσον αφορά στις ιστολογικές βλάβες της ΔΝ The key change in diabetic glomerulopathy is augmentation of extracellular material, that is, quantitative deviations from normal values. Thickening of the peripheral BM is the first demonstrable deviation from normal. In advanced stages, the mesangial matrix accumulation dominates the picture,45, 46 and the BM thickening from early to advanced stages is less marked. Therefore, the mesangial changes correlate more closely with the functional deterioration,46, 47 which has raised the question of whether the early BM thickening is of any clinical relevance. In comparing the different structural parameters, the precision in the individual estimates should be taken into account, and in this respect, the BM thickness has the greater advantage. In patients in the early phase of nephropathy, significant correlations have been found between BM thickness and matrix parameters,45, 48 indicating that the augmentation of extracellular material takes place in parallel at the two locations. The mesangial expansion and glomerulosclerosis do not always develop in parallel, suggesting that they may have somewhat different underlying pathogenesis [22]. GBM = glomerular basement membrane. TBM = tubular basement membrane. 17. Fioretto, P, Steffes, MW, Brown, DM, Mauer, SM. An overview of renal pathology in insulin-dependent diabetes mellitus in relationship to altered glomerular hemodynamics. Am J Kidney Dis 1992; 20: Adler, S. Diabetic nephropathy: Linking histology, cell biology, and genetics. Kidney Int 2004; 66:")
34
Histological Lesions DN
electronic microscope Στο ηλεκτρονικό μικροσκόπιο ... [1].Steffes MW, et al: Diabetes 41: , 1992. [2].Mauer SM, et al: J Clin Invest 74: , 1984. 34

35
Οζώδης σκλήρυνση

36
Διάχυτη σπειραματοσκλήρυνση

37
Υπερηχογράφημα Μέγεθος νεφρών Νεφρική βιοψία;
Συνήθως φυσιολογικό-αυξημένο σε πρόσφατη νεφρική νόσο. Νεφρική βιοψία;

38
Διαβητική νεφροπάθεια Μικρολευκωματινουρία
Υπερδιήθηση Μικρολευκωματινουρία Λευκωματουρία Χρόνια νεφρική νόσος 12 ml/min/year GFR 38

39
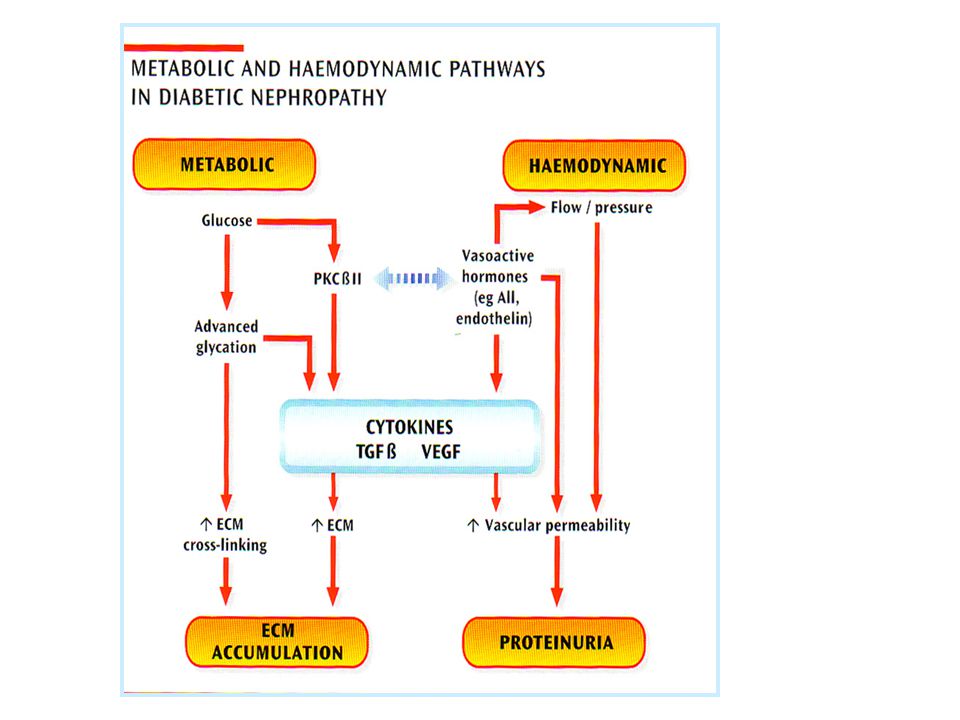
Παθογένεια διαβητικής νεφροπάθειας
Διαταραχή μεταξύ παραγωγής -αποδόμησης της θεμέλιας μεσαγγειακής ουσίας

41
Ιστολογικά ευρήματα Τρία χαρακτηριστικά ευρήματα Μεσαγγειακή αύξηση
Πάχυνση βασικής σπειραματικής μεμβράνης Σκλήρυνση σπειραμάτων Οζώδης σπειραματοσκλήρυνση (βλάβη των Kimmestiel – Wilson) Διάχυτη σπειραματοσκλήρυνση Καψικές σταγόνες (capsular drops) Κάλυμμα ινικής (fibrin cap)
 Διάχυτη σπειραματοσκλήρυνση. Καψικές σταγόνες (capsular drops) Κάλυμμα ινικής (fibrin cap)")
42
Ερώτηση 2η Διαβητική νεφροπάθεια
Όλοι οι ασθενείς θα αναπτύξουν διαβητική νεφροπάθεια; Υπάρχει αναστροφή στην εξέλιξη της; Πότε ένταξη σε εξωνεφρική κάθαρση;

43
Εμφάνιση ΔΝ σε ασθενείς με ΣΔ
type 1 type 2 Diabetic Nephropathy 80% 20% 1/3 30-40% των ασθ με ΣΔ type 1 or 2 θα αναπτύξουν ΔΝ 30-40% A fraction of these progress to ESRD smaller in type 2 diabetes, However, because of the much greater prevalence of type 2 diabetes, such patients constitute over half of those diabetic patients currently starting on dialysis. Diabetic Nephropathy, American Diabetes Association Diabetes Care :S94-S98, 2003 43 43

44
Diabetic nephropathy in types 1 and 2
In this figure, the curve for loss of glomerular filtration rate is plotted together with the curve for transition from microalbuminuria to gross proteinuria, affording a perspective of the course of diabetic nephropathy in both types of diabetes. While not all microalbuminuric individuals progress to proteinuria and azotemia, the majority are at risk for end-stage renal disease due to diabetic nephropathy. GFR-glomerular filtration rate. months-years hyperfiltration and microalbuminuria clinical diabetic nephropathy (macroalbuminuria, dipstick(+)) 44
) 44.")
45
Φυσική εξέλιξη της διαβητικής νεφροπάθειας
Η διαβητική νεφροπάθεια είναι μη αναστρέψιμη στον άνθρωπο. Καμία περίπτωση υποστροφής ή θεραπείας της νόσου δεν αναφέρεται στη βιβλιογραφία. Από τη στιγμή που τα κλινικά σημεία και ευρήματα της νεφροπάθειας έχουν εκδηλωθεί, η φυσική εξέλιξη είναι αμετάβλητη και οδηγεί στο θάνατο Kussman et al, 1976

46
Μη αναστρέψιμοι παράγοντες κινδύνου εμφάνισης και εξέλιξης της ΔΝ
Μη αναστρέψιμοι παράγοντες κινδύνου εμφάνισης και εξέλιξης της ΔΝ Γενετική προδιάθεση Διάρκεια του διαβήτη

47
Δυνητικά αναστρέψιμοι παράγοντες κινδύνου εμφάνισης και εξέλιξης της ΔΝ
Υπεργλυκαιμία Υπερλιποπρωτεϊναιμία Υπέρταση Υψηλή περιεκτικότητα της τροφής σε λεύκωμα Κάπνισμα Λευκωματουρία per se

48
Διαβητική Νεφροπάθεια τύπου 1
Lewis et al, N Engl J Med, 1993

49
Επίδραση των ACEΙ σε πρωτεϊνουρικούς ασθενείς με διαβήτη τύπου 2
FU Decline GFR Investigator year n Treatment (yrs) Proteinuria (ml/min/y) Walker et al [‘92] 86 ACEI vs conv 3 Lebovitz et al [‘94] 46 ACEI vs conv 3 Bakris et al [‘96] 52 ACEI vs CA vs BB 5 Nielsen et al [‘97] 36 ACEI vs BB 3 Estacio et al [‘00] 83 ACEI vs CA 5 Fogari et al [‘99] 51 ACEI vs CA 2 Η μέση ετήσια μείωση του GFR χωρίς θεραπεία είναι 12 ml/min Parving H-H et al, Curr Opin Nephrol Hypertens, 2001
 Proteinuria (ml/min/y) Walker et al [‘92] 86 ACEI vs conv 3 Lebovitz et al [‘94] 46 ACEI vs conv 3 Bakris et al [‘96] 52 ACEI vs CA vs BB 5 Nielsen et al [‘97] 36 ACEI vs BB 3 Estacio et al [‘00] 83 ACEI vs CA 5 Fogari et al [‘99] 51 ACEI vs CA 2 Η μέση ετήσια μείωση του GFR χωρίς θεραπεία είναι 12 ml/min. Parving H-H et al, Curr Opin Nephrol Hypertens,")
50
H Επίδραση των ACEI στην πρωτεϊνουρία και την εξέλιξη της ΧΝΑ σε ασθενείς με διαβήτη τύπου 2
N Rx Proteinuria Renal Function* ESRD Ravid, Vs placebo ND Lebovitz, Vs CT † ND Bakris, Vs CCB ND Vs BB ND Ahmad, Vs placebo ND Nielsen, Vs BB ND UKPDS, Vs BB ND Fogari, Vs CCB ND ABCD, Vs CCB ND REIN, Vs CT ND Micro-HOPE 3577 Vs placebo ND *Serum creatinine or GFR. † in patients with baseline urine albumin 300 mg/d, in patients with urine albumin >300 mg/d. CT = conventional therapy; ND = not determined.

51
In patients with type 1 DM without uremia which have not received a kidney transplant, pancreas transplantation does not ameliorate established lesions of diabetic nephropathy within 5 years after Tx, but the effects of longer periods of normoglycemia are unknown. We studied kidney function and performed renal biopsies before pancreas Tx and 5 and 10 years thereafter in 8 patients with type 1 diabetes but without uremia who had mild to advanced lesions of diabetic nephropathy at the time of Tx. The biopsy samples were analyzed morphometrically. 51 51

52
at base line and 5 and 10 years after pancreas transplantation
thickness of the TBM thickness of the GBM mesangial-matrix fractional volume mesangial fractional volume at base line and 5 and 10 years after pancreas transplantation 52 52

53
Θεραπευτική παρέμβαση σε ασθενείς με ΣΔ
Reversal Prevention Primary Secondary Tertiary Normoalbuminuria Microalbuminuria Proteinuria GFR ESRD Strict glycemic control Strict control of hypertension, Administration ACEi-ARB, Protein intake, statins, .. Για τον λόγο αυτό η θεραπευτική περέμβαση στηρίζεται κυρίως στον αυστηρό γλυκαιμικό έλεγχο και τον έλεγχο της υπέρτασης, με βάση τους οποίους επιδιώκεται η πρωτογενής, η δευτερογενής ή τριτογενής πρόληψη ή και η αναστροφή της πορείας της ΔΝ. Γλυκαιμικός έλεγχος It can partially reverse the glomerular hypertrophy and hyperfiltration* At least in type 1 diabetes, it can delay the development of microalbuminuria It can stabilize or decrease protein excretion in patients with microalbuminuria** Mesangial volume and mesangial matrix volume were significantly decreased as compared to the same measurements at zero and five years In some patients, the width of the glomerular and tubular basement membranes and the mesangial volumes had returned to normal, and nodular glomerular lesions had disappeared. *both in the basal state and after a protein load) that are thought to be important risk factors for glomerular injury. **although this effect may not be apparent until relative normoglycemia has been maintained for two years. 53
 that are thought to be important risk factors for glomerular injury. **although this effect may not be apparent until relative normoglycemia has been maintained for two years. 53.")
54
Μεγάλος Μέτριος Ελάχιστος
Ερώτηση 3η Ποιός ο καρδιαγγειακός κίνδυνος στους ασθενείς με ΧΝΝ και ΣΔ Μεγάλος Μέτριος Ελάχιστος

55
Distribution of markers of CKD in NHANES participants with diabetes & hypertension, 2005–2010 Figure 1.11 (Volume 1) NHANES 1988–1994 & 2005–2010 participants age 20 & older; single sample estimates of eGFR & ACR. eGFR calculated using the CKD-EPI equation. USRDS 2013

56
Ασθενείς με ΧΝΝ πεθαίνουν πριν το ΤΣΧΝΝ
25% 30% 40% 15% 9% Collins, Adv Studies in Med, (3C) 2003, Medicare Cohort
 2003, Medicare Cohort")
57
Steno-2: Goal Attainment
Intensive therapy Conventional therapy 100 P<0.001 P=0.21 80 P=0.005 60 P=0.001 Intervention 40 P=0.06 20 Patients (%) 100 P=0.35 P=0.005 P=0.14 During treatment, compared with participants receiving conventional therapy, individuals in the Steno-2 intensive treatment group were more likely to reach goals for risk factors such as HbA1c, cholesterol levels, and systolic blood pressure. As this slide shows, after an average of 7.8 years of treatment and 5.5 years of follow-up, the observed differences between the intensive and conventional treatment groups had narrowed. This was a result of patients originally assigned to conventional treatment receiving more intensive therapy, as more intensive treatment became the norm in clinical practice. Even though both Steno-2 groups showed similar risk factor reductions at follow-up, patients in the original intensive treatment group showed decreased long-term risk for all assessed complications (ie, cardiovascular death, cardiovascular events, and end-stage renal disease, data not shown). This provides another example of the need for early and intensive intervention. Gaede P, Lund-Anderson H, Parving HH, Pederson O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358: 80 60 Follow-up 40 P=0.27 P=0.31 20 HbA1c <6.5% Cholesterol <175 mg/dL Triglycerides <150 mg/dL Systolic BP <130 mm Hg Diastolic BP <80 mm Hg BP=blood pressure. Gaede P, et al. N Engl J Med. 2008;358: 57
 100. P=0.35. P= P=0.14. During treatment, compared with participants receiving conventional therapy, individuals in the Steno-2 intensive treatment group were more likely to reach goals for risk factors such as HbA1c, cholesterol levels, and systolic blood pressure. As this slide shows, after an average of 7.8 years of treatment and 5.5 years of follow-up, the observed differences between the intensive and conventional treatment groups had narrowed. This was a result of patients originally assigned to conventional treatment receiving more intensive therapy, as more intensive treatment became the norm in clinical practice. Even though both Steno-2 groups showed similar risk factor reductions at follow-up, patients in the original intensive treatment group showed decreased long-term risk for all assessed complications (ie, cardiovascular death, cardiovascular events, and end-stage renal disease, data not shown). This provides another example of the need for early and intensive intervention. Gaede P, Lund-Anderson H, Parving HH, Pederson O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358: Follow-up. 40. P=0.27. P= HbA1c <6.5% Cholesterol <175 mg/dL. Triglycerides <150 mg/dL. Systolic BP <130 mm Hg. Diastolic BP <80 mm Hg. BP=blood pressure. Gaede P, et al. N Engl J Med. 2008;358:")
58
Lasting Benefits of Early, Intensive Intervention: UKPDS “Legacy” Effect
Any Diabetes Endpoint Microvascular Disease Myocardial Infarction All-cause Mortality P=0.44 Intervention P=0.029 P=0.052 The UKPDS randomized >3800 adults newly diagnosed with type 2 diabetes to conventional or intensive treatment over 10 years to compare treatment outcomes for micro- and macrovascular complications.1 At the trial’s end, the intensive treatment group showed a significant 12% decrease in any diabetes-related endpoint; this was driven by a 25% reduction in microvascular disease risk.1 A recently published 10-year follow-up study (UKPDS 80) showed a sustained benefit of early intervention. Specifically, even though the randomized UKPDS interventions were not maintained, at 10-year follow-up, patients who had received early, intensive treatment showed significant decreases in any diabetes-related endpoint and in microvascular disease of 9% and 24%, respectively.2 Patients not only experienced a continued benefit in terms of microvascular risk, but over the course of the follow-up, reductions in macrovascular risk—17% for diabetes-related death (not shown), 15% for MI, and 13% for all-cause mortality—all reached statistical significance.2 It is of interest that these benefits were apparent without a sustained difference in HbA1c levels maintained between the 2 groups, an outcome sometimes called the “legacy” effect.2 These findings demonstrate the importance of early, intensive treatment of type 2 diabetes. UKPDS Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352: Holman RR, Paul SK, Bethel MA, Matthews DR, Neil AW. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359: P=0.0099 Relative Risk Reduction (%) P=0.040 Post-trial Monitoring P=0.007 P=0.014 P=0.001 Holman RR, et al. N Engl J Med. 2008;359: ; UKPDS Study Group. Lancet. 1998;352:
 showed a sustained benefit of early intervention. Specifically, even though the randomized UKPDS interventions were not maintained, at 10-year follow-up, patients who had received early, intensive treatment showed significant decreases in any diabetes-related endpoint and in microvascular disease of 9% and 24%, respectively.2. Patients not only experienced a continued benefit in terms of microvascular risk, but over the course of the follow-up, reductions in macrovascular risk—17% for diabetes-related death (not shown), 15% for MI, and 13% for all-cause mortality—all reached statistical significance.2. It is of interest that these benefits were apparent without a sustained difference in HbA1c levels maintained between the 2 groups, an outcome sometimes called the legacy effect.2 These findings demonstrate the importance of early, intensive treatment of type 2 diabetes. UKPDS Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352: Holman RR, Paul SK, Bethel MA, Matthews DR, Neil AW. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359: P= Relative Risk Reduction (%) P= Post-trial Monitoring. P= P= P= Holman RR, et al. N Engl J Med. 2008;359: ; UKPDS Study Group. Lancet. 1998;352:")
59
Εξωνεφρική κάθαρση Η ένταξη γίνεται συνήθως πρώιμα
eGFR of mL/min Μείωση ουραιμικών επιπλοκών Ρύθμιση αρτηριακής πίεσης Πρόληψη αγγειακών επιπλοκών. Όλες οι μέθοδοι ΑΜΚ, ΠΚ, Τχ, Διπλή Τχ (πάγκρεας/νεφρός)
")
Παρόμοιες παρουσιάσεις