Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Ειδικευόμενος Β’ Ουρολογικής Κλινικής Α.Π.Θ.
Διηθητικός ουροθηλιακός καρκίνος ουροδόχου κύστης Βιβλιογραφικές επιλογές Πέτρος Γεωργόπουλος Ειδικευόμενος Β’ Ουρολογικής Κλινικής Α.Π.Θ. Γ.Ν. Παπαγεωργίου

2
Βιβλιογραφικές επιλογές 2012-2013
Επιδημιολογία MIBC Διάγνωση και Σταδιοποίηση Νεοεπικουρική θεραπεία (Neoadjuvant chemotherapy) Λεμφαδενικός καθαρισμός Παρακολούθηση ασθενών μετά από ριζική κυστεκτομή
 Λεμφαδενικός καθαρισμός. Παρακολούθηση ασθενών μετά από ριζική κυστεκτομή.")
3
Επιδημιολογία Παράγοντες κινδύνου ανάπτυξης καρκίνου ουροδόχου κύστης
Παράγοντες κινδύνου ανάπτυξης καρκίνου ουροδόχου κύστης Κάπνισμα Έκθεση σε επαγγελματικούς παράγοντες Ακτινοθεραπεία Διαιτητικές συνήθειες Σχιστοσωμίαση ουροδόχου κύστης Χρόνια φλεγμονή Φύλο Εθνικοί και κοινωνικοοικονομικοί παράγοντες

4
Επιδημιολογία Ακτινοθεραπεία
Ανάπτυξη κακοήθων όγκων της ουροδόχου κύστης μετά από εξωτερική ακτινοθεραπεία για Γυναικολογικούς καρκίνους Καρκίνο προστάτη Συντελεστής επίπτωσης καρκίνου ουροδόχου κύστης μετά από ακτινοθεραπεία Εξωτερική ακτινοθεραπεία – 1,42 Βραχυθεραπεία – 1,10 Συνδυασμός Increased rates of secondary bladder malignancies have been reported after external-beam radiotherapy (EBRT) for gynaecological malignancies, with relative risks of 2-4 (15). A recent population cohort study identified 243,082 men treated for prostate cancer between 1988 and 2003 in the Surveillance, Epidemiology and End Results database (SEER) in the USA. The standardised incidence ratios for bladder cancer developing after radical prostatectomy (RP), EBRT, brachytherapy (BT), and EBRT-BT were 0.99, 1.42, 1.10, and 1.39, respectively, in comparison with the general U.S. population. The increased risk of bladder cancer in patients undergoing ERBT, BT, or ERBT-BT should be taken into account during follow-up, although the likelihood of mortality was described as very low in a recent study (16). It has recently been proposed that patients who have received radiotherapy for prostate cancer with modern modalities such as intensity-modulated radiotherapy (IMRT) may have lower rates of in-field bladder and rectal secondary malignancies (17). Nevertheless, since longer follow-up data are not yet available, and as bladder cancer requires a long period to develop, patients treated with radiation and with a long life-expectancy are at highest risk and should be followed up closely (17).
 for gynaecological malignancies, with relative risks of 2-4 (15). A recent population cohort study. identified 243,082 men treated for prostate cancer between 1988 and 2003 in the Surveillance, Epidemiology. and End Results database (SEER) in the USA. The standardised incidence ratios for bladder cancer developing. after radical prostatectomy (RP), EBRT, brachytherapy (BT), and EBRT-BT were 0.99, 1.42, 1.10, and 1.39, respectively, in comparison with the general U.S. population. The increased risk of bladder cancer in patients. undergoing ERBT, BT, or ERBT-BT should be taken into account during follow-up, although the likelihood. of mortality was described as very low in a recent study (16). It has recently been proposed that patients. who have received radiotherapy for prostate cancer with modern modalities such as intensity-modulated. radiotherapy (IMRT) may have lower rates of in-field bladder and rectal secondary malignancies (17). Nevertheless, since longer follow-up data are not yet available, and as bladder cancer requires a long period. to develop, patients treated with radiation and with a long life-expectancy are at highest risk and should be. followed up closely (17).")
5
Επιδημιολογία Zelefsky MJ, Housman DM, Pei X, et al. Incidence of secondary cancer development after high-dose intensity-modulated radiotherapy and image-guided brachytherapy for the treatment of localized prostate cancer. Int J Radiat Oncol Biol Phys Jul 1;83(3):953-9. Σκοπός: Η εκτίμηση της επίπτωση ανάπτυξης δευτεροπαθών όγκων μετά από μεταβαλλόμενης έντασης ακτινοβόληση για τον καρκίνο του προστάτη Η μεταβαλλόμενης έντασης ακτινοβόληση(IMRT) Προηγμένη μέθοδο ακτινοθεραπείας Υψηλής ακρίβειας Υψηλότερες δόσεις ακτινοβολίας επικεντρωμένες σε περιοχές εντός του όγκου Ελαχιστοποίηση της δόσης στους γύρω ιστούς -In contrast to other studies, we report low rates of IF bladder and rectal SM risks after prostate cancer RT using modern sophisticated treatment techniques. For EBRT patients, compared with the general population, we noted an increased excess risk of OOF skin cancers but not for the brachytherapy patients. When SMs developed, they were generally of an early stage, likely owing to early detection, and the incidence of SM-related mortality was low among these patients. This information would be important to guide patients who are weighing the pros and cons of various treatments to manage prostate cancer. Nevertheless, these data are applicable at 10 years after therapy, and longer follow-up is necessary to clarify the risks at 15 and 20 years after therapy. -EBRT patients were treated with IMRT using a five-field coplanar beam arrangement delivered to the prostate and seminal vesicles using 15 MV photons in daily 1.8-Gy fractions. The treatment planning and delivery were as previously described (12). The median EBRT prescribed dose was 81 Gy -
: Σκοπός: Η εκτίμηση της επίπτωση ανάπτυξης δευτεροπαθών όγκων μετά από μεταβαλλόμενης έντασης ακτινοβόληση για τον καρκίνο του προστάτη. Η μεταβαλλόμενης έντασης ακτινοβόληση(IMRT) Προηγμένη μέθοδο ακτινοθεραπείας. Υψηλής ακρίβειας. Υψηλότερες δόσεις ακτινοβολίας επικεντρωμένες σε περιοχές εντός του όγκου. Ελαχιστοποίηση της δόσης στους γύρω ιστούς. -In contrast to other studies, we report low rates of IF bladder and rectal SM risks after prostate cancer RT using modern sophisticated treatment techniques. For EBRT patients, compared with the general population, we noted an increased excess risk of OOF skin cancers but not for the brachytherapy patients. When SMs developed, they were generally of an early stage, likely owing to early detection, and the incidence of SM-related mortality was low among these patients. This information would be important to guide patients who are weighing the pros and cons of various treatments to manage prostate cancer. Nevertheless, these data are applicable at 10 years after therapy, and longer follow-up is necessary to clarify the risks at 15 and 20 years after therapy. -EBRT patients were treated with IMRT using a five-field coplanar beam arrangement delivered to the prostate and seminal vesicles using 15 MV photons in daily 1.8-Gy fractions. The treatment planning and delivery were as previously described (12). The median EBRT prescribed dose was 81 Gy. -")
6
Επιδημιολογία Zelefsky MJ, Housman DM, Pei X, et al. Incidence of secondary cancer development after high-dose intensity-modulated radiotherapy and image-guided brachytherapy for the treatment of localized prostate cancer. Int J Radiat Oncol Biol Phys Jul 1;83(3):953-9. Μείωση της πιθανότητας ανάπτυξης καρκίνου ουροδόχου κύστης και ορθού μετά από IMRT σχέση με την εξωτερική ακτινοβολία για το καρκίνο του προστάτη Πρώιμη η διάγνωση των όγκων μετά από ακτινοθεραπεία Χαμηλή θνησιμότητα αυτών των ασθενών The 10-year likelihood of SM development was 25% after EBRT and 15% after brachytherapy (p = .02). The corresponding 10-year likelihood for in-field SM development in these groups was 4.9% and 1.6% (p = .24).
: Μείωση της πιθανότητας ανάπτυξης καρκίνου ουροδόχου κύστης και ορθού μετά από IMRT σχέση με την εξωτερική ακτινοβολία για το καρκίνο του προστάτη. Πρώιμη η διάγνωση των όγκων μετά από ακτινοθεραπεία. Χαμηλή θνησιμότητα αυτών των ασθενών. The 10-year likelihood of SM development was 25% after EBRT and 15% after brachytherapy (p = .02). The corresponding 10-year likelihood for in-field SM development in these groups was 4.9% and 1.6% (p = .24).")
7
Σταδιοποίηση Σκοπός της μελέτης
Mitra AP, Skinner EC, Miranda G, et al. A precystectomy decision model to predict pathological upstaging and oncological outcomes in clinical stage T2 bladder cancer. BJU Int 2013 Feb;111(2): Σκοπός της μελέτης Κατηγοριοποίηση των ασθενών σταδίου Τ2 σε ομάδες ανάλογα τον κίνδυνο αύξησης του σταδίου του όγκου μετά την κυστεκτομή Να προβλέψει την πιθανότητα κακής έκβασης μετά την κυστεκτομή με αποτέλεσμα τον καθορισμό των κατάλληλων υποψηφίων για νεοεπικουρική χημειοθεραπεία To categorize patients with clinical stage T2 bladder cancer into risk groups based on their potential for pathological upstaging and eventual oncological outcomes at cystectomy. To pre-emptively identify such patients who will be upstaged and have poor outcomes after cystectomy, aiming to better determine the ideal candidates for neoadjuvant chemotherapy. -a patient was considered pathologically upstaged at cystectomy if the tumour was staged ≥pT3 and/or nodal metastasis was detected. When these factors were included in a decision tree model, 70.6% of patients with hydronephrosis experienced upstaging and had the worst outcome (P < 0.001). In patients without hydronephrosis, tumour growth pattern was a second-tier discriminator (P < 0.001); in patients with non-papillary tumours, 71.7% of cases with evidence of deep muscularis propria involvement experienced upstaging compared to 53.8% of cases with no deep muscle involvement (P = 0.012), whereas, among patients with combined papillary and non-papillary features, 33% of cases aged ≤65 years were upstaged compared to 47% of cases aged >65 years (P = 0.036). The cross-validated decision tree resulted in three risk groups with significantly varying probabilities of recurrence-free and overall survival (both with overall P < 0.001).
: Σκοπός της μελέτης. Κατηγοριοποίηση των ασθενών σταδίου Τ2 σε ομάδες ανάλογα τον κίνδυνο αύξησης του σταδίου του όγκου μετά την κυστεκτομή. Να προβλέψει την πιθανότητα κακής έκβασης μετά την κυστεκτομή με αποτέλεσμα τον καθορισμό των κατάλληλων υποψηφίων για νεοεπικουρική χημειοθεραπεία. To categorize patients with clinical stage T2 bladder cancer into risk groups based on their potential for pathological upstaging and eventual oncological outcomes at cystectomy. To pre-emptively identify such patients who will be upstaged and have poor outcomes after cystectomy, aiming to better determine the ideal candidates for neoadjuvant chemotherapy. -a patient was considered pathologically upstaged at cystectomy if the tumour was staged ≥pT3 and/or nodal metastasis was detected. When these factors were included in a decision tree model, 70.6% of patients with hydronephrosis experienced upstaging and had the worst outcome (P < 0.001). In patients without hydronephrosis, tumour growth pattern was a second-tier discriminator (P < 0.001); in patients with non-papillary tumours, 71.7% of cases with evidence of deep muscularis propria involvement experienced upstaging compared to 53.8% of cases with no deep muscle involvement (P = 0.012), whereas, among patients with combined papillary and non-papillary features, 33% of cases aged ≤65 years were upstaged compared to 47% of cases aged >65 years (P = 0.036). The cross-validated decision tree resulted in three risk groups with significantly varying probabilities of recurrence-free and overall survival (both with overall P < 0.001).")
8
Σταδιοποίηση Μεθοδολογία
Mitra AP, Skinner EC, Miranda G, et al. A precystectomy decision model to predict pathological upstaging and oncological outcomes in clinical stage T2 bladder cancer. BJU Int 2013 Feb;111(2): 240-8 Μεθοδολογία Αναδρομική μελέτη 948 ασθενείς σταδίου pT2N0M0 χωρίς νεοεπικουρική θεραπεία Ως αύξηση του σταδίου θεωρήθηκε η εύρεση λεμφαδενικών μεταστάσεων ή/και ευρήματα ≥pT3 στο παρασκεύασμα της κυστεκτομής a patient was considered pathologically upstaged at cystectomy if the tumour was staged ≥pT3 and/or nodal metastasis was detected.
: Μεθοδολογία. Αναδρομική μελέτη. 948 ασθενείς σταδίου pT2N0M0 χωρίς νεοεπικουρική θεραπεία. Ως αύξηση του σταδίου θεωρήθηκε η εύρεση λεμφαδενικών μεταστάσεων ή/και ευρήματα ≥pT3 στο παρασκεύασμα της κυστεκτομής. a patient was considered pathologically upstaged at cystectomy if the tumour was staged ≥pT3 and/or nodal metastasis was detected.")
9
Σταδιοποίηση Αποτελέσματα :
Mitra AP, Skinner EC, Miranda G, et al. A precystectomy decision model to predict pathological upstaging and oncological outcomes in clinical stage T2 bladder cancer. BJU Int 2013 Feb;111(2): 240-8 Αποτελέσματα : 54% των ασθενών αύξηση του σταδίου μετά την κυστεκτομή Η αύξηση του σταδίου μετά την κυστεκτομή συνδυάζεται με μείωση της συνολικής επιβίωσης Σημαντικοί προγνωστικοί παράγοντες αύξησης του σταδίου είναι: Η παρουσία υδρονέφρωσης (70,6%) ο τύπος του όγκου (θηλωματώδης ή μη) το βάθος διήθησης του μυϊκού χιτώνα η ηλικία (όριο 65 έτη) A total of 948 patients met the inclusion criteria, of whom 512 (54%) patients were upstaged at cystectomy; upstaging was associated with a worse recurrence-free and overall survival (both P < 0.001). Age, presence of hydronephrosis, evidence of deep muscularis propria invasion and lymphovascular invasion on transurethral resection specimen, as well as tumour growth pattern and count, were significantly associated with upstaging. When these factors were included in a decision tree model, 70.6% of patients with hydronephrosis experienced upstaging and had the worst outcome (P < 0.001). In patients without hydronephrosis, tumour growth pattern was a second-tier discriminator (P < 0.001); in patients with non-papillary tumours, 71.7% of cases with evidence of deep muscularis propria involvement experienced upstaging compared to 53.8% of cases with no deep muscle involvement (P = 0.012), whereas, among patients with combined papillary and non-papillary features, 33% of cases aged ≤65 years were upstaged compared to 47% of cases aged >65 years (P = 0.036). The cross-validated decision tree resulted in three risk groups with significantly varying probabilities of recurrence-free and overall survival (both with overall P < 0.001).
: Αποτελέσματα : 54% των ασθενών αύξηση του σταδίου μετά την κυστεκτομή. Η αύξηση του σταδίου μετά την κυστεκτομή συνδυάζεται με μείωση της συνολικής επιβίωσης. Σημαντικοί προγνωστικοί παράγοντες αύξησης του σταδίου είναι: Η παρουσία υδρονέφρωσης (70,6%) ο τύπος του όγκου (θηλωματώδης ή μη) το βάθος διήθησης του μυϊκού χιτώνα. η ηλικία (όριο 65 έτη) A total of 948 patients met the inclusion criteria, of whom 512 (54%) patients were upstaged at cystectomy; upstaging was associated with a worse recurrence-free and overall survival (both P < 0.001). Age, presence of hydronephrosis, evidence of deep muscularis propria invasion and lymphovascular invasion on transurethral resection specimen, as well as tumour growth pattern and count, were significantly associated with upstaging. When these factors were included in a decision tree model, 70.6% of patients with hydronephrosis experienced upstaging and had the worst outcome (P < 0.001). In patients without hydronephrosis, tumour growth pattern was a second-tier discriminator (P < 0.001); in patients with non-papillary tumours, 71.7% of cases with evidence of deep muscularis propria involvement experienced upstaging compared to 53.8% of cases with no deep muscle involvement (P = 0.012), whereas, among patients with combined papillary and non-papillary features, 33% of cases aged ≤65 years were upstaged compared to 47% of cases aged >65 years (P = 0.036). The cross-validated decision tree resulted in three risk groups with significantly varying probabilities of recurrence-free and overall survival (both with overall P < 0.001).")
10
Nodes 1–3 comprised the low–moderate risk group, where 47
Nodes 1–3 comprised the low–moderate risk group, where 47.5% of patients were upstaged with 5-year RFS and OS probabilities of 66% and 48%, respectively (Table 3). Nodes 4 and 5 comprised the moderate–high risk group, where 54.8% of patients experienced upstaging with 5-year RFS and OS probabilities of 61% and 34%, respectively. Patients in node 6 comprised the high-risk group, where 5-year RFS and OS probabilities of 46% and 27%, respectively, were the lowest, and 70.6% of patients were upstaged. Patients in these risk groups therefore had significantly different RFS and OS (both with overall P < 0.001; Fig. 3 and Table 3). The mean (se) accuracy of the final model in predicting pathological upstaging was 65.7%
. Nodes 4 and 5 comprised the moderate–high risk group, where 54.8% of patients experienced upstaging with 5-year RFS and OS probabilities of 61% and 34%, respectively. Patients in node 6 comprised the high-risk group, where 5-year RFS and OS probabilities of 46% and 27%, respectively, were the lowest, and 70.6% of patients were upstaged. Patients in these risk groups therefore had significantly different RFS and OS (both with overall P < 0.001; Fig. 3 and Table 3). The mean (se) accuracy of the final model in predicting pathological upstaging was 65.7%")
11
Σταδιοποίηση Nodes 1–3 comprised the low–moderate risk group, where 47.5% of patients were upstaged with 5-year RFS and OS probabilities of 66% and 48%, respectively (Table 3). Nodes 4 and 5 comprised the moderate–high risk group, where 54.8% of patients experienced upstaging with 5-year RFS and OS probabilities of 61% and 34%, respectively. Patients in node 6 comprised the high-risk group, where 5-year RFS and OS probabilities of 46% and 27%, respectively, were the lowest, and 70.6% of patients were upstaged. Patients in these risk groups therefore had significantly different RFS and OS (both with overall P < 0.001; Fig. 3 and Table 3). The mean (se) accuracy of the final model in predicting pathological upstaging was 65.7%
. Nodes 4 and 5 comprised the moderate–high risk group, where 54.8% of patients experienced upstaging with 5-year RFS and OS probabilities of 61% and 34%, respectively. Patients in node 6 comprised the high-risk group, where 5-year RFS and OS probabilities of 46% and 27%, respectively, were the lowest, and 70.6% of patients were upstaged. Patients in these risk groups therefore had significantly different RFS and OS (both with overall P < 0.001; Fig. 3 and Table 3). The mean (se) accuracy of the final model in predicting pathological upstaging was 65.7%")
12
Διάγνωση και σταδιοποίηση
Διάγνωση και σταδιοποίηση Lu YY, Chen JH, Liang JA, et al. Clinical value of FDG PET or PET/CT in urinary bladder cancer: a systemic review and meta-analysis. Eur J Radiol 2012 Sep;81(9): Μέτα – ανάλυση για την διαγνωστική ακρίβεια του FDG PET ή PET/CT στον καρκίνο της ουροδόχου κύστης H Fruorodeoxyglucose (FDG): ραδιοφάρμακο που δεσμεύεται από κύτταρα με αυξημένο μεταβολισμό της γλυκόζης Η FDG PET αποτελεί σημαντικό μη επεμβατικό τρόπο απεικόνισης κακοηθειών εξαιτίας της μοναδικής ικανότητας αναγνώρισης των ενεργά μεταβολικών βλαβών Δυσκολία στην απεικόνιση των πρωτοπαθών όγκων της κύστης και των περιοχικών λεμφαδένων εξαιτίας απέκκρισης του φαρμάκου στα ούρα -a meta-analysis of pooled sensitivity and specificity in detecting primary and metastatic lesions of bladder cancer Fludeoxyglucose: heart, lungs, brain – tumors The pooled sensitivity and specificity of PET/CT for primary lesion detection of bladder cancer were 0.90 (95% CI: 0.70–0.99) and 1.00 (95% CI: 0.74–1.00), respectively. The pooled sensitivity and specificity of FDG PET or PET/CT for staging or restaging (metastatic lesions) of bladder cancer were 0.82 (95% CI: 0.72–0.89) and 0.89 (95% CI: 0.81–0.95), respectively. The diagnostic accuracy of FDG PET or PET/CT is good in metastatic lesions of urinary bladder cancer. Due to the small number of patients and limited number of studies analyzed, the diagnostic capability of FDG PET or PET/CT in detection of primary bladder wall lesions could not be assessed
: Μέτα – ανάλυση για την διαγνωστική ακρίβεια του FDG PET ή PET/CT στον καρκίνο της ουροδόχου κύστης. H Fruorodeoxyglucose (FDG): ραδιοφάρμακο που δεσμεύεται από κύτταρα με αυξημένο μεταβολισμό της γλυκόζης. Η FDG PET αποτελεί σημαντικό μη επεμβατικό τρόπο απεικόνισης κακοηθειών εξαιτίας της μοναδικής ικανότητας αναγνώρισης των ενεργά μεταβολικών βλαβών. Δυσκολία στην απεικόνιση των πρωτοπαθών όγκων της κύστης και των περιοχικών λεμφαδένων εξαιτίας απέκκρισης του φαρμάκου στα ούρα. -a meta-analysis of pooled sensitivity and specificity in detecting primary and metastatic lesions of bladder cancer. Fludeoxyglucose: heart, lungs, brain – tumors. The pooled sensitivity and specificity of PET/CT for primary lesion detection of bladder cancer were 0.90 (95% CI: 0.70–0.99) and 1.00 (95% CI: 0.74–1.00), respectively. The pooled sensitivity and specificity of FDG PET or PET/CT for staging or restaging (metastatic lesions) of bladder cancer were 0.82 (95% CI: 0.72–0.89) and 0.89 (95% CI: 0.81–0.95), respectively. The diagnostic accuracy of FDG PET or PET/CT is good in metastatic lesions of urinary bladder cancer. Due to the small number of patients and limited number of studies analyzed, the diagnostic capability of FDG PET or PET/CT in detection of primary bladder wall lesions could not be assessed.")
13
Διάγνωση και σταδιοποίηση
Διάγνωση και σταδιοποίηση Lu YY, Chen JH, Liang JA, et al. Clinical value of FDG PET or PET/CT in urinary bladder cancer: a systemic review and meta-analysis. Eur J Radiol 2012 Sep;81(9): Αποτελέσματα Διάγνωση πρωτοπαθών όγκων ουροδόχου κύστης Ευαισθησία 0.90 Ειδικότητα 1.00 Περιορισμοί: μικρός αριθμός μελετών (2) και απέκκριση στα ούρα Σταδιοποίηση (λεμφαδενική διασπορά και απομακρυσμένες μεταστάσεις) Ευαισθησία 0.82 Ειδικότητα 0.89 Εφαρμογές Πρώιμη διάγνωση μεταστάσεων καρκίνου ουροδόχου κύστης - σταδιοποίηση Επιλογή ασθενών για νεοεπικουρική χημειοθεραπεία ? Ανταπόκριση στην επικουρική χημειοθεραπεία ? Διάγνωση πρωτοπαθών όγκων ουροδόχου κύστης Ευαισθησία (95% CI: 0.70–0.99) Ειδικότητα 1.00 (95% CI: 0.74–1.00) Περιορισμοί: μικρός αριθμός μελετών (2) και απέκκριση στα ούρα Σταδιοποίηση (λεμφαδενική διασπορά και απομακρυσμένες μεταστάσεις) Ευαισθησία 0.82 (95% CI: 0.72–0.89) Ειδικότητα 0.89 (95% CI: 0.81–0.95) για την
: Αποτελέσματα. Διάγνωση πρωτοπαθών όγκων ουροδόχου κύστης. Ευαισθησία Ειδικότητα Περιορισμοί: μικρός αριθμός μελετών (2) και απέκκριση στα ούρα. Σταδιοποίηση (λεμφαδενική διασπορά και απομακρυσμένες μεταστάσεις) Ευαισθησία Ειδικότητα Εφαρμογές. Πρώιμη διάγνωση μεταστάσεων καρκίνου ουροδόχου κύστης - σταδιοποίηση. Επιλογή ασθενών για νεοεπικουρική χημειοθεραπεία Ανταπόκριση στην επικουρική χημειοθεραπεία Διάγνωση πρωτοπαθών όγκων ουροδόχου κύστης. Ευαισθησία 0.90 (95% CI: 0.70–0.99) Ειδικότητα 1.00 (95% CI: 0.74–1.00) Περιορισμοί: μικρός αριθμός μελετών (2) και απέκκριση στα ούρα. Σταδιοποίηση (λεμφαδενική διασπορά και απομακρυσμένες μεταστάσεις) Ευαισθησία 0.82 (95% CI: 0.72–0.89) Ειδικότητα 0.89 (95% CI: 0.81–0.95) για την.")
14
Διάγνωση και σταδιοποίηση
Διάγνωση και σταδιοποίηση Vargas HA, Akin O, Schöder H, et al. Prospective evaluation of MRI, ¹¹C- acetate PET/CT and contrast enhanced CT for staging of bladder cancer. Eur J Radiol 2012 Dec;81(12): Σκοπός Αξιολόγηση των MRI, CT και ¹¹C-acetate PET/CT στην σταδιοποίηση του καρκίνου της ουροδόχου κύστης Κριτήρια ένταξης Ασθενείς με διαπιστωμένο ιστολογικά καρκίνο ουροδόχου κύστης Θα υποβληθούν σε ριζική κυστεκτομή και λεμφαδενικό καθαρισμό The exact uptake mechanism of 11C-acetate is not known, but studies suggest that it is incorporated into the lipid pool in cancer tissue with low oxidative metabolism and high lipid synthesis. In staging bladder cancer, MRI, 11C-acetate PET/CT and CT displayed similar levels of accuracy. For all modalities, a history of intravesical and/or systemic chemotherapy affected staging accuracy Unfortunately, we found that for all three imaging modalities studied, staging accuracy was negatively affected by prior BCG administration. 11C-acetate PET/CT appeared to be most affected, having the lowest specificity of all 3 modalities for detection of nodal metastases in patients with prior intravesical BCG administration ( .
: Σκοπός. Αξιολόγηση των MRI, CT και ¹¹C-acetate PET/CT στην σταδιοποίηση του καρκίνου της ουροδόχου κύστης. Κριτήρια ένταξης. Ασθενείς με διαπιστωμένο ιστολογικά καρκίνο ουροδόχου κύστης. Θα υποβληθούν σε ριζική κυστεκτομή και λεμφαδενικό καθαρισμό. The exact uptake mechanism of 11C-acetate is not known, but studies suggest that it is incorporated into the lipid pool in cancer tissue with low oxidative metabolism and high lipid synthesis. In staging bladder cancer, MRI, 11C-acetate PET/CT and CT displayed similar levels of accuracy. For all modalities, a history of intravesical and/or systemic chemotherapy affected staging accuracy. Unfortunately, we found that for all three imaging modalities studied, staging accuracy was negatively affected by prior BCG administration. 11C-acetate PET/CT appeared to be most affected, having the lowest specificity of all 3 modalities for detection of nodal metastases in patients with prior intravesical BCG administration ( .")
16
Διάγνωση και σταδιοποίηση
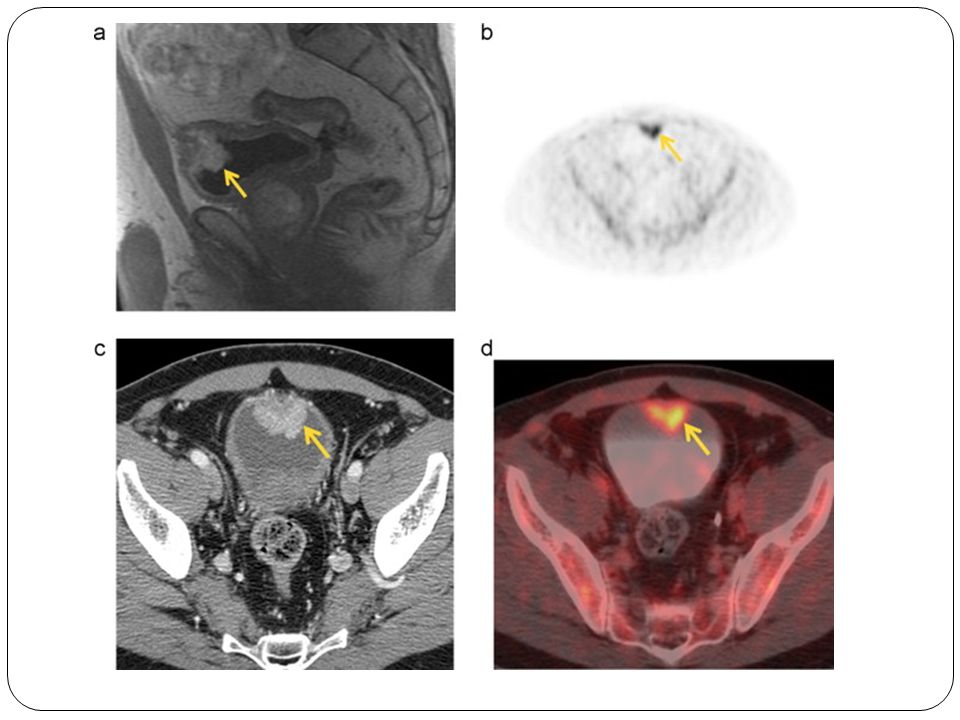
Διάγνωση και σταδιοποίηση Vargas HA, Akin O, Schöder H, et al. Prospective evaluation of MRI, ¹¹C- acetate PET/CT and contrast enhanced CT for staging of bladder cancer. Eur J Radiol 2012 Dec;81(12): Αποτελέσματα MRI: 56% σταδιοποιήθηκαν ορθώς 38% υπερεκτιμήθηκαν 6% υποεκτιμήθηκαν CT: 63% σταδιοποιήθηκαν ορθώς 31% υπερεκτιμήθηκαν ¹¹C-acetate PET/CT (9 ασθενείς) Αληθώς θετικά 7 Ψευδώς θετικά 2 MRI correctly staged 56% (9/16) of patients, overstaged 38% (6/16) and understaged 6% (1/16). CT correctly staged 63% (10/16) of patients, overstaged 31% (5/16) and understaged 6% (1/16). T stages determined at pathology, MRI and CT are summarized in Table 2. On 11C-acetate PET/CT, there was uptake within the bladder wall in 9 patients; the uptake was true positive in 7 and false positive in 2 patients. In the 7 patients without 11C-acetate uptake in the bladder wall, the results were true negative in 5 and false negative in 2. An example of a patient who was correctly staged with MRI and CT and had true-positive uptake on PET is shown in Fig. 2.
: Αποτελέσματα. MRI: 56% σταδιοποιήθηκαν ορθώς. 38% υπερεκτιμήθηκαν. 6% υποεκτιμήθηκαν. CT: 63% σταδιοποιήθηκαν ορθώς. 31% υπερεκτιμήθηκαν. ¹¹C-acetate PET/CT (9 ασθενείς) Αληθώς θετικά 7. Ψευδώς θετικά 2. MRI correctly staged 56% (9/16) of patients, overstaged 38% (6/16) and understaged 6% (1/16). CT correctly staged 63% (10/16) of patients, overstaged 31% (5/16) and understaged 6% (1/16). T stages determined at pathology, MRI and CT are summarized in Table 2. On 11C-acetate PET/CT, there was uptake within the bladder wall in 9 patients; the uptake was true positive in 7 and false positive in 2 patients. In the 7 patients without 11C-acetate uptake in the bladder wall, the results were true negative in 5 and false negative in 2. An example of a patient who was correctly staged with MRI and CT and had true-positive uptake on PET is shown in Fig. 2.")
17
Διάγνωση και σταδιοποίηση
Διάγνωση και σταδιοποίηση Vargas HA, Akin O, Schöder H, et al. Prospective evaluation of MRI, ¹¹C- acetate PET/CT and contrast enhanced CT for staging of bladder cancer. Eur J Radiol 2012 Dec;81(12): Μετά από ενδοκυστικές εγχύσεις BCG 43% σταδιοποιήθηκαν ορθώς με CT και MRI Χωρίς ενδοκυστικές εγχύσεις BCG 67% ορθή σταδιοποίηση με MRI 78% ορθή σταδιοποίηση με CT Both MRI and CT correctly staged 43% (3/7) of patients who had received intravesical BCG prior to imaging. Among patients with no history of intravesical BCG therapy, the percentage correctly staged increased to 67% (6/9) for MRI and 78% (7/9) for CT.
: Μετά από ενδοκυστικές εγχύσεις BCG. 43% σταδιοποιήθηκαν ορθώς με CT και MRI. Χωρίς ενδοκυστικές εγχύσεις BCG. 67% ορθή σταδιοποίηση με MRI. 78% ορθή σταδιοποίηση με CT. Both MRI and CT correctly staged 43% (3/7) of patients who had received intravesical BCG prior to imaging. Among patients with no history of intravesical BCG therapy, the percentage correctly staged increased to 67% (6/9) for MRI and 78% (7/9) for CT.")
18
Διάγνωση και σταδιοποίηση
MRI και CT μετά από ενδοκυστική έγχυση BCG

19
Διάγνωση και σταδιοποίηση
Διάγνωση και σταδιοποίηση Vargas HA, Akin O, Schöder H, et al. Prospective evaluation of MRI, ¹¹C- acetate PET/CT and contrast enhanced CT for staging of bladder cancer. Eur J Radiol 2012 Dec;81(12): Ορθή σταδιοποίηση μετά από συστηματική χημειοθεραπεία 44% MRI 67% CT Ορθή σταδιοποίηση χωρίς προηγηθείσα χημειοθεραπεία 71% MRI 57% CT Of the 9 patients who had received systemic chemotherapy prior to imaging, MRI and CT correctly staged 44% (4/9) and 67% (6/9) and overstaged 44% (4/9) and 33% (3/9), respectively. Of the patients who had not received systemic chemotherapy before imaging, MRI and CT correctly staged 71% (5/7) and 57% (4/7) and overstaged 29% (2/7) and 43% (3/7), respectively. The only patient who was understaged on both MRI and CT received systemic chemotherapy before imaging.
: Ορθή σταδιοποίηση μετά από συστηματική χημειοθεραπεία. 44% MRI. 67% CT. Ορθή σταδιοποίηση χωρίς προηγηθείσα χημειοθεραπεία. 71% MRI. 57% CT. Of the 9 patients who had received systemic chemotherapy prior to imaging, MRI and CT correctly staged 44% (4/9) and 67% (6/9) and overstaged 44% (4/9) and 33% (3/9), respectively. Of the patients who had not received systemic chemotherapy before imaging, MRI and CT correctly staged 71% (5/7) and 57% (4/7) and overstaged 29% (2/7) and 43% (3/7), respectively. The only patient who was understaged on both MRI and CT received systemic chemotherapy before imaging.")
20
Διάγνωση και σταδιοποίηση
Διάγνωση και σταδιοποίηση Vargas HA, Akin O, Schöder H, et al. Prospective evaluation of MRI, ¹¹C- acetate PET/CT and contrast enhanced CT for staging of bladder cancer. Eur J Radiol 2012 Dec;81(12): Συμπεράσματα Ίδια διαγνωστική ακρίβεια και των τριών μεθόδων στην σταδιοποίηση του καρκίνου της ουροδόχου κύστης Μείωση της ακρίβειας μετά από ενδοκυστική έγχυση BCG(υπερσταδιοποίηση) ή χημειοθεραπεία
: Συμπεράσματα. Ίδια διαγνωστική ακρίβεια και των τριών μεθόδων στην σταδιοποίηση του καρκίνου της ουροδόχου κύστης. Μείωση της ακρίβειας μετά από ενδοκυστική έγχυση BCG(υπερσταδιοποίηση) ή χημειοθεραπεία.")
21
Διάγνωση και σταδιοποίηση
Yoshida S, Koga F, Kobayashi S, et al. Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle- invasive bladder cancer. IntJRadiat OncolBiol Phys2012May1;83(1):e21-7 Σκοπός Ο ρόλος της μαγνητικής τομογραφίας διάχυσης (DW MRI) στην αναγνώριση των χημειο-ακτινοευαίσθητων όγκων της ουροδόχου κύστης Πιθανότητα διατήρησης της κύστης σε ασθενείς με χημειο- ακτινοευαίσθητους όγκους In chemoradiation (CRT)-based bladder-sparing approaches for muscle invasive bladder cancer (MIBC), patients who respond favorably to induction CRT enjoy the benefits of bladder preservation, whereas nonresponders do not. Thus, accurate prediction of CRT sensitivity would optimize patient selection for bladder-sparing protocols. Diffusion-weighted MRI (DW-MRI) is a functional imaging technique that quantifies the diffusion of water molecules in a noninvasive manner. We investigated whether DW-MRI predicts CRT sensitivity of MIBC.
:e21-7. Σκοπός. Ο ρόλος της μαγνητικής τομογραφίας διάχυσης (DW MRI) στην αναγνώριση των χημειο-ακτινοευαίσθητων όγκων της ουροδόχου κύστης. Πιθανότητα διατήρησης της κύστης σε ασθενείς με χημειο- ακτινοευαίσθητους όγκους. In chemoradiation (CRT)-based bladder-sparing approaches for muscle invasive bladder cancer (MIBC), patients who respond favorably to induction CRT enjoy the benefits of bladder preservation, whereas nonresponders do not. Thus, accurate prediction of CRT sensitivity would optimize patient selection for bladder-sparing protocols. Diffusion-weighted MRI (DW-MRI) is a functional imaging technique that quantifies the diffusion of water molecules in a noninvasive manner. We investigated whether DW-MRI predicts CRT sensitivity of MIBC.")
22
Διάγνωση και σταδιοποίηση
Yoshida S, Koga F, Kobayashi S, et al. Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle-invasive bladder cancer. IntJRadiat OncolBiol Phys2012May1;83(1):e21-7 H μαγνητική τομογραφία διάχυσης προσμετράει τον τρόπο της τοπικής κινητικότητας των μορίων του νερού Η διάχυση των μορίων του νερού σε διάφορους ιστούς προσμετρείται με τον φαινομενικό συντελεστή διάχυσης (ADC) και είναι διαφορετικός για κάθε ιστό Οι κακοήθεις όγκοι λόγω της κυτταροβρίθειας τους εμφανίζουν χαμηλό συντελεστή διάχυσης 23 MIBC patients (cT2/T3 = 7/16) who underwent induction CRT consisting of radiotherapy to the small pelvis (40 Gy) with two cycles of cisplatin (20 mg/day for 5 days), followed by partial or radical cystectomy. All patients underwent DW-MRI before the initiation of treatment. Associations of apparent diffusion coefficient (ADC) values with CRT sensitivity were analyzed. The proliferative potential of MIBC was also assessed by analyzing the Ki-67 labeling index (LI) in pretherapeutic biopsy specimens. The current study, for the first time to our knowledge, demonstrates the role of DW-MRI in predicting CRT sensitivity of MIBC. Patients with MIBC who have lower ADC values are likely to have a favorable response to induction CRT and thus enjoy its potential benefit, including improved quality of life with bladder preservation and improved survival (14). DW-MRI potentially contributes to optimized patient selection for CRT-based bladder-sparing approaches in a simple and noninvasive manner
:e21-7. H μαγνητική τομογραφία διάχυσης προσμετράει τον τρόπο της τοπικής κινητικότητας των μορίων του νερού. Η διάχυση των μορίων του νερού σε διάφορους ιστούς προσμετρείται με τον φαινομενικό συντελεστή διάχυσης (ADC) και είναι διαφορετικός για κάθε ιστό. Οι κακοήθεις όγκοι λόγω της κυτταροβρίθειας τους εμφανίζουν χαμηλό συντελεστή διάχυσης. 23 MIBC patients (cT2/T3 = 7/16) who underwent induction CRT consisting of radiotherapy to the small pelvis (40 Gy) with two cycles of cisplatin (20 mg/day for 5 days), followed by partial or radical cystectomy. All patients underwent DW-MRI before the initiation of treatment. Associations of apparent diffusion coefficient (ADC) values with CRT sensitivity were analyzed. The proliferative potential of MIBC was also assessed by analyzing the Ki-67 labeling index (LI) in pretherapeutic biopsy specimens. The current study, for the first time to our knowledge, demonstrates the role of DW-MRI in predicting CRT sensitivity of MIBC. Patients with MIBC who have lower ADC values are likely to have a favorable response to induction CRT and thus enjoy its potential benefit, including improved quality of life with bladder preservation and improved survival (14). DW-MRI potentially contributes to optimized patient selection for CRT-based bladder-sparing approaches in a simple and noninvasive manner.")
23
Διάγνωση

24
Διάγνωση και σταδιοποίηση
Yoshida S, Koga F, Kobayashi S, et al. Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle-invasive bladder cancer. IntJRadiat OncolBiol Phys2012May1;83(1):e21-7 Μεθοδολογία 23 ασθενείς σταδίου cT2-3 υπεβλήθησαν σε DW-MRI Έλαβαν ακτινοθεραπεία και δυό κύκλους χημειοθεραπεία με σισπλατίνη Υπεβλήθησαν σε ριζική κυστεκτομή The study cohort consisted of 23 MIBC patients (cT2/T3 = 7/16) who underwent induction CRT consisting of radiotherapy to the small pelvis (40 Gy) with two cycles of cisplatin (20 mg/day for 5 days), followed by partial or radical cystectomy. All patients underwent DW-MRI before the initiation of treatment. Associations of apparent diffusion coefficient (ADC) values with CRT sensitivity were analyzed. The proliferative potential of MIBC was also assessed by analyzing the Ki-67 labeling index (LI) in pretherapeutic biopsy specimens.
:e21-7. Μεθοδολογία. 23 ασθενείς σταδίου cT2-3 υπεβλήθησαν σε DW-MRI. Έλαβαν ακτινοθεραπεία και δυό κύκλους χημειοθεραπεία με σισπλατίνη. Υπεβλήθησαν σε ριζική κυστεκτομή. The study cohort consisted of 23 MIBC patients (cT2/T3 = 7/16) who underwent induction CRT consisting of radiotherapy to the small pelvis (40 Gy) with two cycles of cisplatin (20 mg/day for 5 days), followed by partial or radical cystectomy. All patients underwent DW-MRI before the initiation of treatment. Associations of apparent diffusion coefficient (ADC) values with CRT sensitivity were analyzed. The proliferative potential of MIBC was also assessed by analyzing the Ki-67 labeling index (LI) in pretherapeutic biopsy specimens.")
25
Διάγνωση και σταδιοποίηση
Yoshida S, Koga F, Kobayashi S, et al. Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle-invasive bladder cancer. IntJRadiat OncolBiol Phys2012May1;83(1):e21-7 Αποτελέσματα Χημειο-ακτινοευαίσθητοι όγκοι χαμηλότερες τιμές συντελεστή διάχυσης Η τιμή του ADC σημαντικός και ανεξάρτητος προγνωστικός παράγοντας χημειο-ακτινοευαισθησίας των όγκων (p<o,ooo1). Τιμές ADC<0.74 × 10−3 mm2/s ενδεικτικές για χημειο- ακτινοευαισθησία του όγκου (92% ευαισθησία/90% ειδικότητα) . These CRT-sensitive MIBCs showed significantly lower ADC values (median, 0.63 × 10−3 mm2/s; range, 0.43–0.77) than CRT-resistant (no pCR) MIBCs (median, 0.84 × 10−3 mm2/s; range, 0.69–1.09; p = ). Multivariate analysis identified ADC value as the only significant and independent predictor of CRT sensitivity (p < ; odds ratio per ×10−3 mm2/s increase, 1.03; 95% confidence interval, 1.01–1.08). With a cutoff ADC value at 0.74 × 10−3 mm2/s, sensitivity/specificity/accuracy in predicting CRT sensitivity was 92/90/91%.
:e21-7. Αποτελέσματα. Χημειο-ακτινοευαίσθητοι όγκοι χαμηλότερες τιμές συντελεστή διάχυσης. Η τιμή του ADC σημαντικός και ανεξάρτητος προγνωστικός παράγοντας χημειο-ακτινοευαισθησίας των όγκων (p<o,ooo1). Τιμές ADC<0.74 × 10−3 mm2/s ενδεικτικές για χημειο- ακτινοευαισθησία του όγκου (92% ευαισθησία/90% ειδικότητα) . These CRT-sensitive MIBCs showed significantly lower ADC values (median, 0.63 × 10−3 mm2/s; range, 0.43–0.77) than CRT-resistant (no pCR) MIBCs (median, 0.84 × 10−3 mm2/s; range, 0.69–1.09; p = ). Multivariate analysis identified ADC value as the only significant and independent predictor of CRT sensitivity (p < ; odds ratio per ×10−3 mm2/s increase, 1.03; 95% confidence interval, 1.01–1.08). With a cutoff ADC value at 0.74 × 10−3 mm2/s, sensitivity/specificity/accuracy in predicting CRT sensitivity was 92/90/91%.")
26
Διάγνωση και σταδιοποίηση
Yoshida S, Koga F, Kobayashi S, et al. Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle-invasive bladder cancer. IntJRadiat OncolBiol Phys2012May1;83(1):e21-7 Συμπεράσματα DW MRI προγνωστικός δείκτης χημειοακτινοευαισθησίας των όγκων της ουροδόχου κύστης Προσδιορισμός των κατάλληλων ασθενών για διατήρηση της ουροδόχου κύστεως DW-MRI is a potential biomarker for predicting CRT sensitivity in MIBC. DW-MRI may be useful to optimize patient selection for CRT-based bladder-sparing approaches.
:e21-7. Συμπεράσματα. DW MRI. προγνωστικός δείκτης χημειοακτινοευαισθησίας των όγκων της ουροδόχου κύστης. Προσδιορισμός των κατάλληλων ασθενών για διατήρηση της ουροδόχου κύστεως. DW-MRI is a potential biomarker for predicting CRT sensitivity in MIBC. DW-MRI may be useful to optimize patient selection for CRT-based bladder-sparing approaches.")
27
Νεοεπικουρική χημειοθεραπεία
Meeks JJ, Bellmunt J, Bochner BH, et al. A systematic review of neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol Sep;62(3):523-33 Συστηματική ανασκόπηση Σκοπός: Ανασκόπηση των δεδομένων που υποστηρίζουν την περιεγχειρητική χημειοθεραπεία και τα συνιστώμενα σχήματα Προηγούμενα δεδομένα Υποτροπή με απομακρυσμένες μεταστάσεις πιο συχνή από την τοπική υποτροπή (20–50% vs 5–15%) Η βελτίωση των διαγνωστικών και χειρουργικών μεθόδων δεν αύξησε την συνολική επιβίωση
: Συστηματική ανασκόπηση. Σκοπός: Ανασκόπηση των δεδομένων που υποστηρίζουν την περιεγχειρητική χημειοθεραπεία και τα συνιστώμενα σχήματα. Προηγούμενα δεδομένα. Υποτροπή με απομακρυσμένες μεταστάσεις πιο συχνή από την τοπική υποτροπή (20–50% vs 5–15%) Η βελτίωση των διαγνωστικών και χειρουργικών μεθόδων δεν αύξησε την συνολική επιβίωση.")
28
Νεοεπικουρική χημειοθεραπεία
Meeks JJ, Bellmunt J, Bochner BH, et al. A systematic review of neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol Sep;62(3):523-33 Προσδιορισμός των κατάλληλων ασθενών: 66% σταδίου pΤ2 έχουν λανθασμένη σταδιοποίηση και 42% εμφανίζει όγκο μεγαλύτερου σταδίου κατά την κυστεκτομή 40% ασθενών με NMIBC εμφανίζει καρκίνο σταδίου ≥Τ2 κατά την κυστεκτομή Αν η χημειοθεραπεία χορηγηθεί σε ασθενείς υψηλού ρίσκου (≥pT3 ή pT2 με LVI) μειώνεται η πιθανότητα των ασθενών με μη μυοδιηθητικό καρκίνο ουροδόχου κύστης Χρήση FDG-PET για την πρώιμη αναγνώριση των μεταστάσεων και την ανάδειξη των κατάλληλων ασθενών για νεοεπικουρική χημειοθεραπεία As many as 66% of patients with pT2 disease may be incorrectly staged, with 42% upstaged after RC [8]. Importantly, ≥T2 disease is found at RC in 40% of patients clinically staged as non–muscle-invasive disease prior to RC. A nomogram designed to predict T3–T4 pathologic stage at RC based on 726 patients showed only a 4% improvement in accuracy compared with routine clinical staging [9]. Postoperative nomograms including stage and clinical and pathologic features (eg, grade, lymphovascular invasion [LVI]) modestly improved the accuracy of predicting outcomes compared with staging alone, although histologic subtype was not validated[10] and [11]. If chemotherapy could be applied specifically to patients with high-risk disease (eg, ≥pT3 or pT2 with LVI), the risks of overtreatment for those without invasive cancer or with superficial invasive disease (pT2a) could be reduced. A recent prospective study of the use of nuclear medicine imaging (fludeoxyglucose–positron emission tomography) in 42 patients showed this modality's potential to detect occult metastatic disease
: Προσδιορισμός των κατάλληλων ασθενών: 66% σταδίου pΤ2 έχουν λανθασμένη σταδιοποίηση και 42% εμφανίζει όγκο μεγαλύτερου σταδίου κατά την κυστεκτομή. 40% ασθενών με NMIBC εμφανίζει καρκίνο σταδίου ≥Τ2 κατά την κυστεκτομή. Αν η χημειοθεραπεία χορηγηθεί σε ασθενείς υψηλού ρίσκου (≥pT3 ή pT2 με LVI) μειώνεται η πιθανότητα των ασθενών με μη μυοδιηθητικό καρκίνο ουροδόχου κύστης. Χρήση FDG-PET για την πρώιμη αναγνώριση των μεταστάσεων και την ανάδειξη των κατάλληλων ασθενών για νεοεπικουρική χημειοθεραπεία. As many as 66% of patients with pT2 disease may be incorrectly staged, with 42% upstaged after RC [8]. Importantly, ≥T2 disease is found at RC in 40% of patients clinically staged as non–muscle-invasive disease prior to RC. A nomogram designed to predict T3–T4 pathologic stage at RC based on 726 patients showed only a 4% improvement in accuracy compared with routine clinical staging [9]. Postoperative nomograms including stage and clinical and pathologic features (eg, grade, lymphovascular invasion [LVI]) modestly improved the accuracy of predicting outcomes compared with staging alone, although histologic subtype was not validated[10] and [11]. If chemotherapy could be applied specifically to patients with high-risk disease (eg, ≥pT3 or pT2 with LVI), the risks of overtreatment for those without invasive cancer or with superficial invasive disease (pT2a) could be reduced. A recent prospective study of the use of nuclear medicine imaging (fludeoxyglucose–positron emission tomography) in 42 patients showed this modality s potential to detect occult metastatic disease.")
29
Νεοεπικουρική χημειοθεραπεία
Meeks JJ, Bellmunt J, Bochner BH, et al. A systematic review of neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol Sep;62(3):523-33 Αποτελεσματικότητα νεοεπικουρικής χημειοθεραπείας : Χαμηλότερα ποσοστά εξωκυστικής νόσου (p=0.001) Μικρότερος αριθμός παθολογικών λεμφαδένων (p=0.04) Τα ψηλότερα ποσοστά 5ετούς επιβίωσης παρουσίασαν οι ασθενείς που έλαβαν νεοεπικουρική θεραπεία, υπεβλήθησαν σε ριζική κυστεκτομή και λεμφαδενικό καθαρισμό (≥10 λεμφαδένες) 5% βελτίωση της συνολικής επιβίωσης Θεραπευτικά σχήματα: Μόνο τα θεραπευτικά σχήματα με τον παράγοντα σισπλατίνη (GC, MVAC, DD-MVAC)αποδεδειγμένα βελτιώνουν την επιβίωση
: Αποτελεσματικότητα νεοεπικουρικής χημειοθεραπείας : Χαμηλότερα ποσοστά εξωκυστικής νόσου (p=0.001) Μικρότερος αριθμός παθολογικών λεμφαδένων (p=0.04) Τα ψηλότερα ποσοστά 5ετούς επιβίωσης παρουσίασαν οι ασθενείς που έλαβαν νεοεπικουρική θεραπεία, υπεβλήθησαν σε ριζική κυστεκτομή και λεμφαδενικό καθαρισμό (≥10 λεμφαδένες) 5% βελτίωση της συνολικής επιβίωσης. Θεραπευτικά σχήματα: Μόνο τα θεραπευτικά σχήματα με τον παράγοντα σισπλατίνη (GC, MVAC, DD-MVAC)αποδεδειγμένα βελτιώνουν την επιβίωση.")
30
Νεοεπικουρική χημειοθεραπεία
Meeks JJ, Bellmunt J, Bochner BH, et al. A systematic review of neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer. Eur Urol Sep;62(3):523-33 Περιορισμένη η χρήση της νεοεπικουρικής θεραπείας λόγω Μη επιλογής από τους θεράποντες ή τους ασθενείς Μεγάλης ηλικίας ασθενών Νεφρική ανεπάρκεια Καρδιακή ανεπάρκεια Χαμηλό PS
: Περιορισμένη η χρήση της νεοεπικουρικής θεραπείας λόγω. Μη επιλογής από τους θεράποντες ή τους ασθενείς. Μεγάλης ηλικίας ασθενών. Νεφρική ανεπάρκεια. Καρδιακή ανεπάρκεια. Χαμηλό PS.")
31
Λεμφαδενικός καθαρισμός
Shariat SF, Ehdaie B, Rink M, Cha EK, Svatek RS, Chromecki TF, Fajkovic H, Novara G, David SG, Daneshmand S et al: Clinical nodal staging scores for bladder cancer: a proposal for preoperative risk assessment. Eur Urol 2012, 61(2): Σκοπός μελέτης Η ανάπτυξη μοντέλου για τον καθορισμό του αριθμού λεμφαδένων που απαιτούνται για τον λεμφαδενικό καθαρισμό κατά την ριζική κυστεκτομή Ανάλυση ασθενών που υπεβλήθησαν σε λεμφαδενικό καθαρισμό και ριζική κυστεκτομή , από 3 ακαδημαϊκά κέντρα (USA, Καναδάς, Ευρώπη) To develop a model that allows preoperative determination of the minimum number of lymph nodes (LNs) needed to be removed at RC to ensure true nodal status. We analyzed data from 4335 patients treated with RC and pelvic LND without neoadjuvant chemotherapy at 12 academic centers located in the United States, Canada, and Europe.
: Σκοπός μελέτης. Η ανάπτυξη μοντέλου για τον καθορισμό του αριθμού λεμφαδένων που απαιτούνται για τον λεμφαδενικό καθαρισμό κατά την ριζική κυστεκτομή. Ανάλυση 4335 ασθενών που υπεβλήθησαν σε λεμφαδενικό καθαρισμό και ριζική κυστεκτομή , από 3 ακαδημαϊκά κέντρα (USA, Καναδάς, Ευρώπη) To develop a model that allows preoperative determination of the minimum number of lymph nodes (LNs) needed to be removed at RC to ensure true nodal status. We analyzed data from 4335 patients treated with RC and pelvic LND without neoadjuvant chemotherapy at 12 academic centers located in the United States, Canada, and Europe.")
32
Λεμφαδενικός καθαρισμός
Shariat SF, Ehdaie B, Rink M, Cha EK, Svatek RS, Chromecki TF, Fajkovic H, Novara G, David SG, Daneshmand S et al: Clinical nodal staging scores for bladder cancer: a proposal for preoperative risk assessment. Eur Urol 2012, 61(2): Η κίνδυνος λεμφαδενικών μεταστάσεων και ο βαθμός του λεμφαδενικού καθαρισμού εξαρτάται από το στάδιο του όγκου Ο εκτεταμένος λεμφαδενικός καθαρισμός αυξάνει την νοσηρότητα Περιορισμένος λεμφαδενικός καθαρισμός συστήνεται για όγκους σταδίου cTa – Tis Εκτεταμένος λεμφαδενικός καθαρισμός για όγκους cT1 και άνω Σε όγκους σταδίου cT3-4 και εκτεταμένο λεμφαδενικό καθαρισμό το ποσοστό των παθολογικών λεμφαδένων που διαφεύγουν είναι 20% We found that the risk of LN metastases and the number of LNs needed to be removed to ensure true node-negative status increases with advancing clinical stage. There is no one-size-fits-all for LND in patients treated with RC for bladder cancer. While all patients need an LND, a limited LND seems sufficient in patients with cTa-Tis, while an extended LND should be recommended for those with cT1 and higher stage. In patients with cT3-4, even an extended LND still misses about 20% of LN metastasis.Wedeveloped a simple cNSS to aid preoperative clinical decision making about the extent of LND in patients for whom RC for bladder cancer is planned. After validation, such a tool could help physicians decide treatment strategies prior to RC and tailor the extent of LND at RC.
: Η κίνδυνος λεμφαδενικών μεταστάσεων και ο βαθμός του λεμφαδενικού καθαρισμού εξαρτάται από το στάδιο του όγκου. Ο εκτεταμένος λεμφαδενικός καθαρισμός αυξάνει την νοσηρότητα. Περιορισμένος λεμφαδενικός καθαρισμός συστήνεται για όγκους σταδίου cTa – Tis. Εκτεταμένος λεμφαδενικός καθαρισμός για όγκους cT1 και άνω. Σε όγκους σταδίου cT3-4 και εκτεταμένο λεμφαδενικό καθαρισμό το ποσοστό των παθολογικών λεμφαδένων που διαφεύγουν είναι 20% We found that the risk of LN metastases and the number of. LNs needed to be removed to ensure true node-negative. status increases with advancing clinical stage. There is no. one-size-fits-all for LND in patients treated with RC for. bladder cancer. While all patients need an LND, a limited. LND seems sufficient in patients with cTa-Tis, while an. extended LND should be recommended for those with cT1. and higher stage. In patients with cT3-4, even an extended. LND still misses about 20% of LN metastasis.Wedeveloped a. simple cNSS to aid preoperative clinical decision making. about the extent of LND in patients for whom RC for bladder. cancer is planned. After validation, such a tool could help. physicians decide treatment strategies prior to RC and tailor. the extent of LND at RC.")
33
Λεμφαδενικός καθαρισμός
Η πιθανότητα διαφυγής παθολογικού λεμφαδένα μειώνεται με την αύξηση των αφαιρούμενων λεμφαδένων 52% με την εξαίρεση 3 λεμφαδένων 40% με την εξαίρεση 5 λεμφαδένων 26% με την εξαίρεση 10 λεμφαδένων Meticulous ePLND up to the middle upper third of the common iliac vessels appeared to provide survival and recurrence outcomes similar to those of a superextended template up to the inferior mesenteric artery. a 90% correct node staging can be obtained by removing 6, 9, and 25 LNs in stage Ta/TIS, T1, and T2 bladder cancer, respectively. The probability of missing a positive LN decreased with an increasing number of nodes examined (52% if 3 nodes were examined, 40% if 5 were examined, and 26% if 10 were examined) A cNSS of 90% was achieved by examining 6 nodes for clinical Ta-Tis tumors, 9 nodes for cT1 tumors, and 25 nodes for cT2 tumors. In contrast, examination of 25 nodes provided only 77% cNSS for cT3-T4 tumors. The minimum number of examined LNs for adequate staging depends preoperatively on the clinical T stage. Predictive tools can give a preoperative estimation of the likelihood of nodal metastasis and thereby allow tailored decision-making regarding the extent of LND at RC. In patients with clinical Ta-Tis disease, at least six LNs need to be removed to achieve 90% confidence that the patient is node negative. cT1, at least 10 LNs need to be removed to ensure 90% probability of ascertaining true nodal status. In cT2 bladder cancer patients, removal of 25 LNs results in a >90% probability of ascertaining true nodal status. In cT3-4 bladder cancer, the 90% probability is not reached, with an asymptotic approach to a maximum 80% probability of detecting a positive LN. One possible reason for this is the higher likelihood of skip lesions outside of the regular template in patients with locally advanced tumor stage
 A cNSS of 90% was achieved by examining 6 nodes for clinical Ta-Tis tumors, 9 nodes for cT1 tumors, and 25 nodes for cT2 tumors. In contrast, examination of 25 nodes provided only 77% cNSS for cT3-T4 tumors. The minimum number of examined LNs for adequate staging depends preoperatively on the clinical T stage. Predictive tools can give a preoperative estimation of the likelihood of nodal metastasis and thereby allow tailored decision-making regarding the extent of LND at RC. In patients with clinical Ta-Tis disease, at least six LNs need to be removed to achieve 90% confidence that the patient is node negative. cT1, at least 10 LNs need to be removed to ensure 90% probability of ascertaining true nodal status. In cT2 bladder cancer patients, removal of 25 LNs results in a >90% probability of ascertaining true nodal status. In cT3-4 bladder cancer, the 90% probability is not reached, with an asymptotic approach to a maximum 80% probability of detecting a positive LN. One possible reason for this is the higher likelihood of skip lesions outside of the regular template in patients with locally advanced tumor stage.")
34
Λεμφαδενικός καθαρισμός
90% σταδιοποίηση επιτυγχάνεται Ta-Tis: 6 λεμφαδένες cT1: 10 λεμφαδένες cT2: 25 λεμφαδένες cT3-4 έως 80% Ο επιμελής εκτεταμένος λεμφαδενικός καθαρισμός έως το άνω τριτημόριο της κοινής λαγόνιας έχει παροιμία ποσοστά επιβίωσης με τον καθαρισμό έως την κάτω μεσεντέρια αρτηρία

35
Follow up Soukup V, Babjuk M, Bellmunt J et at. Follow-up after surgical treatment of bladder cancer: A critical analysis of the literature. Eur Urol 2012 Aug 62(2): Συστηματική ανασκόπηση Σκοπός μελέτης: Πρόγραμμα παρακολούθησης των ασθενών που έχουν υποβληθεί σε χειρουργική θεραπεία για καρκίνο της ουροδόχου κύστης Σκοπός του follow up Έγκαιρη αναγνώριση των υποτροπών Έγκαιρη αναγνώριση των επιπλοκών της κυστεκτομής και της εκτροπής των ούρων
: Συστηματική ανασκόπηση. Σκοπός μελέτης: Πρόγραμμα παρακολούθησης των ασθενών που έχουν υποβληθεί σε χειρουργική θεραπεία για καρκίνο της ουροδόχου κύστης. Σκοπός του follow up. Έγκαιρη αναγνώριση των υποτροπών. Έγκαιρη αναγνώριση των επιπλοκών της κυστεκτομής και της εκτροπής των ούρων.")
36
Follow up Εκτίμηση του κινδύνου υποτροπής Περιορισμοί
Karakiewicz's nomogram Ταξινόμηση TNM Ηλικία Φύλο Στάδιο όγκου κατά την κυστεκτομή Παρουσία λεμφαγγειακών διηθήσεων Παρουσία CIS Νεοεπικουρική χημειοθεραπεία Eπικουρική χημειοθεραπεία Aκτινοθεραπεία International Bladder Cancer Nomogram (πιθανότητα υποτροπής στα 5 χρόνια) Χρονικό διάστημα διάγνωση – κυστεκτομή Στάδιο όγκου και βαθμός κακοήθειας Ιστολογικός τύπος (TCC, SCC κτλ) Λεμφαδενική διασπορά Standard predictors, pT and pN, were complemented by age, gender, tumor grade at cystectomy, presence of lymphovascular invasion, presence of carcinoma in situ in the cystectomy specimen, neoadjuvant chemotherapy, adjuvant chemotherapy and adjuvant radiotherapy The final nomogram included information on patient age, sex, time from diagnosis to surgery, pathologic tumor stage and grade, tumor histologic subtype, and regional lymph node status. Περιορισμοί Βασίζονται σε αναδρομικές μελέτες Δεν έχει αξιολογηθεί πλήρως η εγκυρότητά τους GR C
 Χρονικό διάστημα διάγνωση – κυστεκτομή. Στάδιο όγκου και βαθμός κακοήθειας. Ιστολογικός τύπος (TCC, SCC κτλ) Λεμφαδενική διασπορά. Standard predictors, pT and pN, were complemented by age, gender, tumor grade at cystectomy, presence of lymphovascular invasion, presence of carcinoma in situ in the cystectomy specimen, neoadjuvant chemotherapy, adjuvant chemotherapy and adjuvant radiotherapy. The final nomogram included information on patient age, sex, time from diagnosis to surgery, pathologic tumor stage and grade, tumor histologic subtype, and regional lymph node status. Περιορισμοί. Βασίζονται σε αναδρομικές μελέτες. Δεν έχει αξιολογηθεί πλήρως η εγκυρότητά τους. GR C.")
37
Follow up Διάγνωση τοπικής υποτροπής και απομακρυσμένων μεταστάσεων
Διάγνωση τοπικής υποτροπής και απομακρυσμένων μεταστάσεων 5%-16,5% στα 5 έτη μετά την κυστεκτομή - οι περισσότερες τον πρώτο χρόνο 70% των ασθενών με τοπική υποτροπή έχει και απομακρυσμένες μεταστάσεις Μέση επιβίωση 4-8 μήνες Η αναγνώριση των υποτροπών πριν την εμφάνιση συμπτωμάτων βελτιώνει την επιβίωση Κύρια απεικονιστική μέθοδος : Αξονική τομογραφία The rate of local recurrence after RC has been reported to range between 5% and 16.5% within 5 yr after surgery. Most of these recurrences are diagnosed during the first 24 mo [5]. Up to 70% of patients with local recurrence will also have distant metastases. The reported median survival after the diagnosis of a local recurrence is only 4–8 mo despite systemic and local treatment. Approximately 80% of patients die of disease within 1 yr, and only 3.5% experience 5-yr survival

38
Follow up Υποτροπή στην ουρήθρα
1,5-6% στους άνδρες & 0,83-4,3 στις γυναίκες Μέση επιβίωση μήνες Παρακολούθηση με κυτταρολογική εκπλύματος ουρήθρας και ουρηθροσκόπηση Αύξηση επιβίωσης με έγκαιρη ανίχνευσης των υποτροπών Χρησιμοποιούμενες θεραπείες BCG ενδοουρηθρικά – σε CIS Ουρηθρεκτομή 1.5–6% after RC, with a mean recurrence-free interval of 13.5–39 mo median overall survival in these patients ranges from 28 to 38 mo, and >50% died because of systemic diseas Reported independent predictors of urethral recurrence were cystectomy for NMIBC, prostate involvement, and a history of previously recurrent NMIBC The surveillance strategies range from observation alone to monitoring with cytology by urethral washings and urethroscopy. In several studies, there was no reported significant survival difference in patients followed with or without urethral washings [78]. However, a recent large retrospective series reported a highly significant survival advantage in male patients with urethral recurrence diagnosed asymptomatic by follow-up compared with male patients diagnosed by symptoms (LE 3) [83]. Thus, follow-up of the male urethra should be recommended, and any pertaining symptoms must be investigated. Recurrent CIS in the urethra with orthotopic bladder substitution can be treated successfully with intraurethral BCG in approximately 80% of patients, while papillary and invasive urethral recurrence should lead to urethrectomy [78]. Fewer data are available on the treatment of urethral recurrences in females. All reported cases were treated with urethrectomy [80], [81] and [82].
 [83]. Thus, follow-up of the male urethra should be recommended, and any pertaining symptoms must be investigated. Recurrent CIS in the urethra with orthotopic bladder substitution can be treated successfully with intraurethral BCG in approximately 80% of patients, while papillary and invasive urethral recurrence should lead to urethrectomy [78]. Fewer data are available on the treatment of urethral recurrences in females. All reported cases were treated with urethrectomy [80], [81] and [82].")
39
Follow up Υποτροπή στο ανώτερο ουροποιητικό σύστημα 1,8-6% πιθανότητα
1,8-6% πιθανότητα Το συχνότερο σημείο όψιμων υποτροπών (28-49 μήνες) Μέση επιβίωση μήνες Κυτταρολογική ούρων διαγνωστική <30% και % σε συμπτωματικούς ασθενείς Συμπτώματα: οσφυϊκό άλγος και μικροσκοπική αιματουρία ή ασυμπτωματική υδρονέφρωση Παρακολούθηση με κυτταρολογική ούρων - Εναλλακτικά: CT urography ή MRI urography UUTTs occur in 1.8–6% of cases in contemporary series (Table 7) and generally are seen later than urethral recurrence (median time to recurrence: 28–49 mo). In fact, the upper urinary tract is the most common site of late recurrence (≥3 yr of disease-free survival following RC) [62], [84] and [85]. The median overall survival is 10–55 mo, and 60–67% of patients die of metastatic disease Urinary cytology can detect <30% of UUTTs when used for routine postcystectomy surveillance; however, in patients with symptoms, findings are positive in 80–100% a positive cytology is highly predictive of upper urinary tract recurrence (LE 3) [89], and cytology is recommended for upper urinary tract follow-up. CT urography with MRI urography as an alternative is standard examination of the upper urinary tract after RC (Table 8).
 Μέση επιβίωση μήνες. Κυτταρολογική ούρων διαγνωστική <30% και % σε συμπτωματικούς ασθενείς. Συμπτώματα: οσφυϊκό άλγος και μικροσκοπική αιματουρία ή ασυμπτωματική υδρονέφρωση. Παρακολούθηση με κυτταρολογική ούρων - Εναλλακτικά: CT urography ή MRI urography. UUTTs occur in 1.8–6% of cases in contemporary series (Table 7) and generally are seen later than urethral recurrence (median time to recurrence: 28–49 mo). In fact, the upper urinary tract is the most common site of late recurrence (≥3 yr of disease-free survival following RC) [62], [84] and [85]. The median overall survival is 10–55 mo, and 60–67% of patients die of metastatic disease Urinary cytology can detect <30% of UUTTs when used for routine postcystectomy surveillance; however, in patients with symptoms, findings are positive in 80–100% a positive cytology is highly predictive of upper urinary tract recurrence (LE 3) [89], and cytology is recommended for upper urinary tract follow-up. CT urography with MRI urography as an alternative is standard examination of the upper urinary tract after RC (Table 8).")
40
Follow up Follow up επιπλοκών
Μέτρηση βιταμίνης Β12 για εκτομή τελικού ειλεού >20cm Παρακολούθηση βιτΒ12 και θεραπεία για 3-5 έτη μετά την κυστεκτομή (GR C) Μεταβολική οξέωση ≤15% ασθενών με ileal conduit Παρακολούθηση της μεταβολικής οξέωσης τον 1ο χρόνο και κατόπιν κάθε 6-12 μήνες (GR C) For patients with terminal ileal resections >20 cm, B12 serum levels should be measured. Vitamin B12 deficiency may lead to megaloblastic anaemia reversible by substitution treatment and irreversible neuropathy As the average body deposits of vitamin B12 are large, vitamin B12measurements and/or substitution should be realised from 3–5 yr after RC onwards (GR C). Metabolic acidosis can be expected in ≤15% of patients with an ileal conduit The risk of metabolic acidosis is the highest during the early postoperative period, in neobladder patients with postvoid residual urine, with urinary tract infection, and in patients with reduced renal function. Serum evaluation for metabolic acidosis should be done regularly during the first 12 mo after RC and then probably every 6–12 mo (GR C). The most frequent complications are symptomatic urinary tract infections; urolithiasis; stenosis of the ureterointestinal anastomosis with potential loss of renal function; complications related to the stoma in conduits; and in neobladder patients, urinary retention and day and/or nighttime incontinence. In a series with ileal conduit, complications developed in 45% of patients within the first 5 yr. This percentage increased to 50%, 54%, and 94% in patients surviving 10, 15, and >15 yr, respectively (LE 3)
 Μεταβολική οξέωση ≤15% ασθενών με ileal conduit. Παρακολούθηση της μεταβολικής οξέωσης τον 1ο χρόνο και κατόπιν κάθε 6-12 μήνες (GR C) For patients with terminal ileal resections >20 cm, B12 serum levels should be measured. Vitamin B12 deficiency may lead to megaloblastic anaemia reversible by substitution treatment and irreversible neuropathy. As the average body deposits of vitamin B12 are large, vitamin B12measurements and/or substitution should be realised from 3–5 yr after RC onwards (GR C). Metabolic acidosis can be expected in ≤15% of patients with an ileal conduit. The risk of metabolic acidosis is the highest during the early postoperative period, in neobladder patients with postvoid residual urine, with urinary tract infection, and in patients with reduced renal function. Serum evaluation for metabolic acidosis should be done regularly during the first 12 mo after RC and then probably every 6–12 mo (GR C). The most frequent complications are symptomatic urinary tract infections; urolithiasis; stenosis of the ureterointestinal anastomosis with potential loss of renal function; complications related to the stoma in conduits; and in neobladder patients, urinary retention and day and/or nighttime incontinence. In a series with ileal conduit, complications developed in 45% of patients within the first 5 yr. This percentage increased to 50%, 54%, and 94% in patients surviving 10, 15, and >15 yr, respectively (LE 3)")
41
Follow up Follow up των επιπλοκών σχετικών με την εκτροπή των ούρων
Συχνότερες επιπλοκές Ουρολοιμώξεις Ουρολιθίαση Στένωση ουρητηροεντερικής αναστόμωσης και νεφρική ανεπάρκεια Επίσχεση ούρων Ακράτεια ούρων Στο 45% των ασθενών με ileal conduit τα πρώτα 5 χρόνια Αύξηση του ποσοστού σε 50% στα 10 χρόνια και 94% >15 χρόνια The most frequent complications are symptomatic urinary tract infections; urolithiasis; stenosis of the ureterointestinal anastomosis with potential loss of renal function; complications related to the stoma in conduits; and in neobladder patients, urinary retention and day and/or nighttime incontinence. In a series with ileal conduit, complications developed in 45% of patients within the first 5 yr. This percentage increased to 50%, 54%, and 94% in patients surviving 10, 15, and >15 yr, respectively (LE 3)
")
42
Follow up Συμπεράσματα Εντατική παρακολούθηση τα 5 πρώτα χρόνια
Η εξωκυστική νόσος και η λεμφαδενική διασπορά αυξάνουν τα ποσοστά υποτροπής Η έγκαιρη αναγνώριση των υποτροπών της ουρήθρας με κυτταρολογική εκπλυματος και ουρηθροσκόπηση βελτιώνει την επιβίωση The early detection of tumour recurrence after RC allows for early treatment. As most relapses occur within 5 yr and the median time to local and distant recurrence is 12–18 mo after RC, follow-up should be intensive for the first 5 yr, particularly for the first 2 yr. Patients with extravesical and lymph nod–positive disease at RC have the highest risk of recurrence. Regular follow-up of the male urethra by urethral washings and urethroscopy has survival benefit, if urethral recurrence is diagnosed early before symptoms occur. Most upper urinary tract recurrences occur >3 yr after RC, at a time when the risk of local and systemic recurrence is decreasing. Lifelong yearly upper urinary tract imaging is advisable in all patients. This study also allows for early detection of urinary diversion complications. Metabolic evaluation should continue throughout life, and vitamin B12 substitution should commence from 3–5 yr after surgery (Table 8 and Table 9). In general, the studies about follow-up after RC are low LE and based on retrospective data. Nonetheless, reasonable recommendations can be made until further prospective randomised studies that test different follow-up schedules have been performed.
. In general, the studies about follow-up after RC are low LE and based on retrospective data. Nonetheless, reasonable recommendations can be made until further prospective randomised studies that test different follow-up schedules have been performed.")
Παρόμοιες παρουσιάσεις













 Γιωργάκης Ε., (1) Οικονομάκης Ι., (1) Πετρωνιάτης Τ., (1)>")




 Κώτης Α., (3) Παπαντωνίου Ν., (4) Πολίτου Μ., (1) Κινούς Β..>")
