Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Δ. Ρίχτερ Πρόεδρος ΕΕΛΙΑ Διευθυντής Καρδιολογικής Κλινικής, «Ευρωκλινική» Αθηνών Χ. Μιχαλακέας Καρδιολόγος Επιστημονικός Συνεργάτης Ασθενής με χρόνια κολπική μαρμαρυγή και ανάγκη διακοπής αντιπηκτικών λόγω επέμβασης

2
Παρουσίαση περιστατικού
Γυναίκα ηλικίας 60 ετών προσέρχεται στον καρδιολόγο λόγω αισθήματος παλμών Ατομικό αναμνηστικό: α) Αρτηριακή υπέρταση υπό αγωγή (Ιρβεσαρτάνη/ΗΤΖ 150/12,5 mg, Βεραπαμίλη 80 mg x 2) β) Δυσλιπιδαιμία υπό αγωγή (Ατορβαστατίνη 20 mg) Κλινική εξέταση: S1-S2, ρυθμικοί, ευκρινείς, ΑΠ=150/90 mmHg HKΓ: Φλεβοκομβικός ρυθμός ~ 80 bpm Holter ρυθμού: δύο επεισόδια κολπικής μαρμαρυγής διάρκειας 40 και 50 sec αντίστοιχα.
 Αρτηριακή υπέρταση υπό αγωγή (Ιρβεσαρτάνη/ΗΤΖ 150/12,5 mg, Βεραπαμίλη 80 mg x 2) β) Δυσλιπιδαιμία υπό αγωγή (Ατορβαστατίνη 20 mg) Κλινική εξέταση: S1-S2, ρυθμικοί, ευκρινείς, ΑΠ=150/90 mmHg. HKΓ: Φλεβοκομβικός ρυθμός ~ 80 bpm. Holter ρυθμού: δύο επεισόδια κολπικής μαρμαρυγής διάρκειας 40 και 50 sec αντίστοιχα.")
3
Διαγνωστική διερεύνηση
Γενική αίματος: κφ Έλεγχος θυρεοειδούς: κφ Έλεγχος νεφρικής λειτουργίας: (Kρεατινίνη = 1,1 mg/dL, Κάθαρση= 52 ml/min) Echo: EF=60%, οριακό πάχος τοιχωμάτων, διαστολική δυσλειτουργία grade I, LA=41 mm Δοκιμασία Κοπώσεως, 6’00’’ εφο.
 Echo: EF=60%, οριακό πάχος τοιχωμάτων, διαστολική δυσλειτουργία grade I, LA=41 mm. Δοκιμασία Κοπώσεως, 6’00’’ εφο.")
4
1) Ποια αντιπηκτική αγωγή πρέπει να λάβει η ασθενής;
1) Ασπιρίνη 2) Κλοπιδογρέλη 3) Ασπιρίνη και Κλοπιδογρέλη 4) Αντιπηκτικά 5) Τίποτα
 Ασπιρίνη. 2) Κλοπιδογρέλη. 3) Ασπιρίνη και Κλοπιδογρέλη. 4) Αντιπηκτικά. 5) Τίποτα.")
5
Risk of stroke according to CHADS2
Risk of stroke, %/year* CHADS2 total score 30 2 3 4 5 6 10 15 20 25 1 CHADS2 criteria Score Congestive heart failure 1 Hypertension Age ≥75 years Diabetes mellitus Stroke/transient ischaemic attack 2 Error bars = 95% confidence intervals; *Theoretical rates without therapy ACC/AHA/ESC guidelines: Fuster V et al. Circulation 2006;114:e257–354 & Eur Heart J 2006;27:1979–2030; Gage BF et al. JAMA 2001;285:2864–70 5 5

6
The CHA2DS2VASc Index Stroke Risk Score for AFib
Weight (points) Congestive heart failure or LVEF < 35% Hypertension Age >75 years Diabetes mellitus Stroke/TIA/systemic embolism Vascular Disease (MI/PAD/Aortic plaque) Age years Sex Category (female) Moderate-High risk > 2 Low risk Lip GYH, Halperin JL. Am J Med 2010; 123: 484.
 Congestive heart failure or LVEF < 35% 1. Hypertension 1. Age >75 years 2. Diabetes mellitus 1. Stroke/TIA/systemic embolism 2. Vascular Disease (MI/PAD/Aortic plaque) 1. Age years 1. Sex Category (female) 1. Moderate-High risk > 2. Low risk 0-1. Lip GYH, Halperin JL. Am J Med 2010; 123: 484.")
7
The CHADS2 Index Stroke Risk Score for Atrial Fibrillation Score
(points) Risk of Stroke (%/year) Approximate Risk threshold for Anticoagulation 3%/year Van Walraven C, et al. Arch Int Med 2003 Go A, et al. JAMA 2003 Gage BF, et al. Circulation 2004
 Risk of Stroke. (%/year) Approximate. Risk threshold for. Anticoagulation. 3%/year. Van Walraven C, et al. Arch Int Med Go A, et al. JAMA Gage BF, et al. Circulation")
8
Risk of stroke according to CHA2DS2-VASc
CHA2DS2-VASc criteria Score Congestive heart failure/ left ventricular dysfunction 1 Hypertension Age 75 years 2 Diabetes mellitus Stroke/transient ischaemic attack/TE Vascular disease (prior myocardial infarction, peripheral artery disease, or aortic plaque) Age 65–74 years Sex category (i.e. female gender) Total score N Adjusted stroke rate (%/year)* 1 0.0 422 1.3 2 1230 2.2 3 1730 3.2 4 1718 4.0 5 1159 6.7 6 679 9.8 7 294 9.6 8 82 9 14 15.2 *Adjusted for warfarin use. Theoretical rates without therapy; assuming that warfarin provides a 64% reduction in stroke risk, based on Hart RG et al TE = thromboembolism Lip G et al. Chest 2010;137:263–72; Lip G et al. Stroke 2010;41:2731–8; ESC guidelines: Camm J et al. Eur Heart J 2010;31:2369–429; Hart RG et al. Ann Intern Med 2007;146:857–67 8 8 8
 Age 65–74 years. Sex category (i.e. female gender) Total score. N. Adjusted stroke rate (%/year)* *Adjusted for warfarin use. Theoretical rates without therapy; assuming that warfarin provides a 64% reduction in stroke risk, based on Hart RG et al TE = thromboembolism. Lip G et al. Chest 2010;137:263–72; Lip G et al. Stroke 2010;41:2731–8; ESC guidelines: Camm J et al. Eur Heart J 2010;31:2369–429; Hart RG et al. Ann Intern Med 2007;146:857–")
9
Κουμαρινικά αντιπηκτικά έναντι ασπιρίνης
Ελάττωση κινδύνου ισχαιμικών ΑΕΕ Βαρφαρίνη αποτελεσματικότερη ασπιρίνης - 36% ελάττωση κινδύνου Hart RG et al. Ann Intern Med 1999;131(7)192
192.")
10
2) Πόσες πιθανότητες έχει αυτή η γυναίκα να πάρει αντιπηκτικά απ τον ιατρό της;
1) 30% 2) 65% 3) 80%
 30% 2) 65% 3) 80%")
11
Αντιμετώπιση της KΜ στην κλινική πράξη: Συνταγογράφηση των ανταγωνιστών της βιταμίνης Κ σε κατάλληλους ασθενείς 64% Λαμβανόμενη θεραπεία: n = Medicare cohort, USA1 Όχι αντιπηκτικά Ανταγωνιστές βιταμίνης Κ 67% n = 5333 EuroHeart survey2 55% n = ATRIA cohort (managed care system, California, USA)3 ATRIA = Anticoagulation and Risk Factors in Atrial Fibrillation 1. Birman-Deych E et al. Stroke 2006;37:1070–4; 2. Nieuwlaat R et al. Eur Heart J 2005;26:2422–34; 3. Go AS et al. JAMA 2003;290:2685–92 11
3. ATRIA = Anticoagulation and Risk Factors in Atrial Fibrillation. 1. Birman-Deych E et al. Stroke 2006;37:1070–4; 2. Nieuwlaat R et al. Eur Heart J 2005;26:2422–34; 3. Go AS et al. JAMA 2003;290:2685–")
12
3) Πόσες πιθανότητες έχει αυτή η γυναίκα να ρυθμίζει διαχρονικά καλά το INR της;
1) 30% 2) 45% 3) 80%
 30% 2) 45% 3) 80%")
13
Ιδανικό INR στην Κολπική Μαρμαρυγή
The European Atrial Fibrillation Trial Study Group, N Engl J Med 1995; 333:5.

14
Κουμαρινικά: Στενό θεραπευτικό εύρος
Ischaemic stroke Intracranial hemorrhage 80 The anticoagulant effect of VKAs is optimized when therapeutic doses are maintained within a very narrow range 60 Target INR (2.0–3.0) Events / 1000 patient years 40 Narrow therapeutic range with VKAs VKAs such as warfarin have a very narrow therapeutic range, within which anticoagulation provides sufficient protection from stroke with a low risk of bleeding complications.1 The anticoagulant activity of VKAs is monitored using the international normalized ratio (INR), which provides a standardized measure of the tendency of a sample of blood to clot. This slide presents rates of ischaemic stroke and intracranial haemorrhage according to INR using data from a retrospective cohort study of 13,559 patients with non-valvular AF enrolled in a health maintenance organization in Northern California, USA.1 As the INR falls below 2.0, the risk of ischaemic stroke increases sharply, indicating that the patient is under-anticoagulated.1 As the INR rises above 3.0, the risk of intracranial haemorrhage which is a dangerous bleeding complication increases, reflecting over-anticoagulation.1 Therefore, the objective with VKAs is generally to achieve and then maintain an INR of 2.03.0.2 However, in practice, achieving and maintaining INR in the target range is often challenging, as VKAs have a slow onset and offset of action and are subject to numerous food and drug interactions. Consequently, continuous and regular anticoagulation monitoring is necessary during treatment with VKAs. References Hylek EM, Go AS, Chang Y, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med 2003;349:10191026. Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation. Circulation 2006;114:e257–354 & Eur Heart J 2006;27:1979–2030. 20 <1.5 1.5–1.9 2.0–2.5 2.6–3.0 3.1–3.5 3.6–4.0 4.1–4.5 >4.5 INR = International normalized ratio; VKA = vitamin K antagonist. Hylek EM, et al. N Eng J Med 2003;349:
 Events / 1000 patient years. 40. Narrow therapeutic range with VKAs. VKAs such as warfarin have a very narrow therapeutic range, within which anticoagulation provides sufficient protection from stroke with a low risk of bleeding complications.1. The anticoagulant activity of VKAs is monitored using the international normalized ratio (INR), which provides a standardized measure of the tendency of a sample of blood to clot. This slide presents rates of ischaemic stroke and intracranial haemorrhage according to INR using data from a retrospective cohort study of 13,559 patients with non-valvular AF enrolled in a health maintenance organization in Northern California, USA.1. As the INR falls below 2.0, the risk of ischaemic stroke increases sharply, indicating that the patient is under-anticoagulated.1. As the INR rises above 3.0, the risk of intracranial haemorrhage which is a dangerous bleeding complication increases, reflecting over-anticoagulation.1. Therefore, the objective with VKAs is generally to achieve and then maintain an INR of 2.0 However, in practice, achieving and maintaining INR in the target range is often challenging, as VKAs have a slow onset and offset of action and are subject to numerous food and drug interactions. Consequently, continuous and regular anticoagulation monitoring is necessary during treatment with VKAs. References. Hylek EM, Go AS, Chang Y, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med 2003;349:10191026. Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation. Circulation 2006;114:e257–354 & Eur Heart J 2006;27:1979– < – – – – – –4.5. >4.5. INR = International normalized ratio; VKA = vitamin K antagonist. Hylek EM, et al. N Eng J Med 2003;349:")
15
Έλεγχος INR: Κλινικές μελέτες έναντι καθημερινής πρακτικής (TTR)
Clinical trial1 Clinical practice2,3 66% Eligible patients receiving Warfarin (%) 44% 38% 25% INR control: Clinical trials vs. clinical practice The challenges of treatment with VKAs mean that many patients are often outside the target INR range and so are at increased risk of either stroke or bleeding complications.13 In a pooled analysis of data from five randomized controlled trials,1 the INR was: in the target range (INR 2.03.0) for 66% of the time below the target range (INR <2.0) for 25% of the time above the target range (INR >3.0) for 9% of the time. In routine clinical practice, INR control might be expected to be worse than that within the controlled setting of a randomized clinical trial where patients are regularly reviewed and rigorously followed-up. Indeed, in a retrospective review of the medical records of 660 patients with AF managed by general internists and family physicians in the US states of New York and North Carolina,2 the INR was: in the target range (INR 2.03.0) for 44% of the time below the target range (INR <2.0) for 38% of the time above the target range (INR >3.0) for 18% of the time. As INR control tends to be worse in routine practice1,2 than in clinical trials,3 the balance of benefit to risk with VKAs may be worse in routine practice than suggested by the results of clinical trials. References Kalra L, Yu G, Perez I, et al. Prospective cohort study to determine if trial efficacy of anticoagulation for stroke prevention in atrial fibrillation translates into clinical effectiveness. BMJ 2000;220:12361239. Samsa GP, Matchar DB, Goldstein LB, et al. Quality of anticoagulation management among patients with atrial fibrillation: results of a review of medical records from 2 communities. Arch Intern Med 2000;160:967973. Matchar DB, Samsa GP, Cohen SJ, et al. Improving the quality of anticoagulation of patients with atrial fibrillation in managed care organizations: results of the managing anticoagulation services trial. Am J Med 2002;113:4251. 18% 9% <2.0 2.0–3.0 >3.0 INR INR = international normalized ratio ; TTR = time-in-therapeutic-range (INR 2.0–3.0). 1. Kalra L, et al. BMJ 2000;320: ; *Pooled data: up to 83–71% in individualized trials. 2. Samsa GP, et al. Arch Intern Med 2000;160: Matchar DB, et al. Am J Med 2002;113:42-51.
 44% 38% 25% INR control: Clinical trials vs. clinical practice. The challenges of treatment with VKAs mean that many patients are often outside the target INR range and so are at increased risk of either stroke or bleeding complications.13. In a pooled analysis of data from five randomized controlled trials,1 the INR was: in the target range (INR 2.03.0) for 66% of the time. below the target range (INR <2.0) for 25% of the time. above the target range (INR >3.0) for 9% of the time. In routine clinical practice, INR control might be expected to be worse than that within the controlled setting of a randomized clinical trial where patients are regularly reviewed and rigorously followed-up. Indeed, in a retrospective review of the medical records of 660 patients with AF managed by general internists and family physicians in the US states of New York and North Carolina,2 the INR was: in the target range (INR 2.03.0) for 44% of the time. below the target range (INR <2.0) for 38% of the time. above the target range (INR >3.0) for 18% of the time. As INR control tends to be worse in routine practice1,2 than in clinical trials,3 the balance of benefit to risk with VKAs may be worse in routine practice than suggested by the results of clinical trials. References. Kalra L, Yu G, Perez I, et al. Prospective cohort study to determine if trial efficacy of anticoagulation for stroke prevention in atrial fibrillation translates into clinical effectiveness. BMJ 2000;220:12361239. Samsa GP, Matchar DB, Goldstein LB, et al. Quality of anticoagulation management among patients with atrial fibrillation: results of a review of medical records from 2 communities. Arch Intern Med 2000;160:967973. Matchar DB, Samsa GP, Cohen SJ, et al. Improving the quality of anticoagulation of patients with atrial fibrillation in managed care organizations: results of the managing anticoagulation services trial. Am J Med 2002;113:4251. 18% 9% < –3.0. >3.0. INR. INR = international normalized ratio ; TTR = time-in-therapeutic-range (INR 2.0–3.0). 1. Kalra L, et al. BMJ 2000;320: ; *Pooled data: up to 83–71% in individualized trials. 2. Samsa GP, et al. Arch Intern Med 2000;160: Matchar DB, et al. Am J Med 2002;113:")
16
4) Ένα χρόνο αργότερα μετά από μεγάλη ταλαιπωρία στη ρύθμιση του INR μαθαίνει πως μπορεί να λαμβάνει νεώτερης γενιάς αντιπηκτικά για την αντιπηκτική της ρύθμιση. Ποιες είναι οι απαραίτητες εργαστηριακές εξετάσεις που θα χρειαστείτε για τη μετάβαση στα νεώτερης γενιάς αντιπηκτικά; 1) Γενική αίματος 2) Κρεατινίνη 3) INR 4) Όλα τα ανωτέρω 5) Το 2 και το 3
 Γενική αίματος. 2) Κρεατινίνη. 3) INR. 4) Όλα τα ανωτέρω. 5) Το 2 και το 3.")
17
5) Ποιό αντιπηκτικό θα της δίνατε;
1. DABIGATRAN 2. RIVAROXABAN 3. APIXABAN

18
The RE-LY Study: Randomized Evaluation of Long-term anticoagulant therapY
Dabigatran Compared to Warfarin in 18,113 Patients with Atrial Fibrillation at Risk of Stroke 18

19
Πρωτεύον σημείο αποτελεσματικότητας
Πρωτεύον σημείο αποτελεσματικότητας 0.50 0.75 1.00 1.25 1.50 Dabigatran 110 vs. Warfarin Dabigatran 150 vs. Warfarin Μη-κατωτερότητα p-value <0.001 Ανωτερότητα 0.30 Margin = 1.46 HR (95% CI)
")
20
Ταξινόμηση ΑΕΕ D 110mg D 150mg warfarin D 110 mg vs. Warfarin
Number rate/yr RR 95% CI p Iσχαιμικό 152 1.29 %/yr 103 0.9 %/yr 133 1.1 %/yr 1.14 0.28 0.76 0.03 Αιμορραγικό 14 0.1 %/yr 12 45 0.4 %/yr 0.31 <0.001 0.26 Iσχαιμικό/ Άγνωστης αιτιολογίας 159 1.3 %/yr 111 142 1.2 %/yr 1.11 0.32

21
Σημεία μειζόνων αιμορραγιών
Dabigatran 110mg Dabigatran 150mg warfarin D 110mg vs. Warfarin D 150mg vs. Warfarin Ετήσιο ποσοστό RR 95% CI p Γαστρεντερικές (ΓΕΣ) 1.1 % 1.5 % 1.0 % 1.10 0.43 1.50 <0.001 Ενδοκράνιες 0.2 % 0.3 % 0.7 % 0.31 0.40 Mείζονες αιμορραγίες (εκτός ΓΕΣ, Μη- ενδοκράνιες ) 1.8 % 0.85 0.11 0.87 0.16
 1.1 % 1.5 % 1.0 % < Ενδοκράνιες. 0.2 % 0.3 % 0.7 % Mείζονες αιμορραγίες (εκτός ΓΕΣ, Μη- ενδοκράνιες ) 1.8 %")
22
G w_script.ppt 4/3/2017 3:16:45 PM Rivaroxaban Once-daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation 22

23
Primary Efficacy Outcome Stroke and non-CNS Embolism
Rivaroxaban Warfarin Event Rate 1.71 2.16 Warfarin Rivaroxaban Cumulative event rate (%) HR (95% CI): 0.79 (0.66, 0.96) P-value Non-Inferiority: <0.001 Days from Randomization No. at risk: Rivaroxaban Warfarin Event Rates are per 100 patient-years Based on Protocol Compliant on Treatment Population
 HR (95% CI): 0.79 (0.66, 0.96) P-value Non-Inferiority: < Days from Randomization. No. at risk: Rivaroxaban Warfarin Event Rates are per 100 patient-years. Based on Protocol Compliant on Treatment Population.")
24
Key Secondary Efficacy Outcomes
Rivaroxaban Warfarin Event Rate HR (95% CI) P-value Vascular Death, Stroke, Embolism 4.51 4.81 0.94 (0.84, 1.05) 0.265 Stroke Type Hemorrhagic Ischemic Unknown Type 0.26 1.62 0.15 0.44 1.64 0.14 0.58 (0.38, 0.89) 0.99 (0.82, 1.20 1.05 (0.55, 2.01) 0.012 0.916 0.871 Non-CNS Embolism 0.16 0.21 0.74 (0.42, 1.32 0.308 Myocardial Infarction 1.02 1.11 0.91 (0.72, 1.16) 0.464 All Cause Mortality Vascular Non-vascular Unknown Cause 4.52 2.91 1.15 0.46 4.91 3.11 1.22 0.57 0.92 (0.82, 1.03) 0.94 (0.81, 1.08) 0.94 (0.75, 1.18) 0.80 (0.57, 1.12) 0.152 0.350 0.611 0.195 Event Rates are per 100 patient-years Based on Intention-to-Treat Population
 P-value. Vascular Death, Stroke, Embolism (0.84, 1.05) Stroke Type Hemorrhagic Ischemic Unknown Type (0.38, 0.89) 0.99 (0.82, (0.55, 2.01) Non-CNS Embolism (0.42, Myocardial Infarction (0.72, 1.16) All Cause Mortality Vascular Non-vascular Unknown Cause (0.82, 1.03) 0.94 (0.81, 1.08) 0.94 (0.75, 1.18) 0.80 (0.57, 1.12) Event Rates are per 100 patient-years. Based on Intention-to-Treat Population.")
25
Presented on behalf of the ARISTOTLE Investigators and Committees
Apixaban versus Warfarin in Patients with Atrial Fibrillation Results of the ARISTOTLE Trial Presented on behalf of the ARISTOTLE Investigators and Committees Sponsored by Bristol-Myers Squibb and Pfizer

26
Primary Outcome Stroke (ischemic or hemorrhagic) or systemic embolism
P (non-inferiority)<0.001 21% RRR Apixaban 212 patients, 1.27% per year Warfarin patients, 1.60% per year HR 0.79 (95% CI, 0.66–0.95); P (superiority)=0.011 No. at Risk Apixaban Warfarin
< % RRR. Apixaban 212 patients, 1.27% per year. Warfarin 265 patients, 1.60% per year. HR 0.79 (95% CI, 0.66–0.95); P (superiority)= No. at Risk. Apixaban Warfarin")
27
Efficacy Outcomes Outcome Apixaban (N=9120) Warfarin (N=9081)
HR (95% CI) P Value Event Rate (%/yr) Stroke or systemic embolism* 1.27 1.60 0.79 (0.66, 0.95) 0.011 Stroke 1.19 1.51 0.79 (0.65, 0.95) 0.012 Ischemic or uncertain 0.97 1.05 0.92 (0.74, 1.13) 0.42 Hemorrhagic 0.24 0.47 0.51 (0.35, 0.75) <0.001 Systemic embolism (SE) 0.09 0.10 0.87 (0.44, 1.75) 0.70 All-cause death* 3.52 3.94 0.89 (0.80, 0.998) 0.047 Stroke, SE, or all-cause death 4.49 5.04 0.89 (0.81, 0.98) 0.019 Myocardial infarction 0.53 0.61 0.88 (0.66, 1.17) 0.37 * Part of sequential testing sequence preserving the overall type I error
 P Value. Event Rate. (%/yr) Stroke or systemic embolism* (0.66, 0.95) Stroke (0.65, 0.95) Ischemic or uncertain (0.74, 1.13) Hemorrhagic (0.35, 0.75) < Systemic embolism (SE) (0.44, 1.75) All-cause death* (0.80, 0.998) Stroke, SE, or all-cause death (0.81, 0.98) Myocardial infarction (0.66, 1.17) * Part of sequential testing sequence preserving the overall type I error.")
28
Adverse Events and Liver Function Tests
Apixaban (N=9088) Warfarin (N=9052) Total patients with an adverse event 7406 (81.5) 7521 (83.1) Total patients with a serious adverse event 3182 (35.0) 3302 (36.5) Serious adverse events reported in ≥ 1% of patients in either treatment group Atrial fibrillation 301 (3.3) 287 (3.2) Pneumonia 202 (2.2) 231 (2.6) Discontinuations due to an adverse event 688 (7.6) 758 (8.4) ALT or AST > 3X ULN and total bilirubin > 2X ULN 30/ 8788 (0.3) 31/ 8756 (0.4) ALT elevation > 3X ULN 100/ 8790 (1.1) 89/ 8759 (1.0) > 5X ULN 45/ 8790 (0.5) 47/ 8759 (0.5) > 10X ULN 16/ 8790 (0.2) 20/ 8759 (0.2) > 20X ULN 8/ 8790 (<0.1) 12/ 8759 (0.1)
 Warfarin. (N=9052) Total patients with an adverse event (81.5) 7521 (83.1) Total patients with a serious adverse event (35.0) 3302 (36.5) Serious adverse events reported in ≥ 1% of patients in either treatment group. Atrial fibrillation. 301 (3.3) 287 (3.2) Pneumonia. 202 (2.2) 231 (2.6) Discontinuations due to an adverse event. 688 (7.6) 758 (8.4) ALT or AST > 3X ULN and total bilirubin > 2X ULN. 30/ 8788 (0.3) 31/ 8756 (0.4) ALT elevation. > 3X ULN. 100/ 8790 (1.1) 89/ 8759 (1.0) > 5X ULN. 45/ 8790 (0.5) 47/ 8759 (0.5) > 10X ULN. 16/ 8790 (0.2) 20/ 8759 (0.2) > 20X ULN. 8/ 8790 (<0.1) 12/ 8759 (0.1)")
29
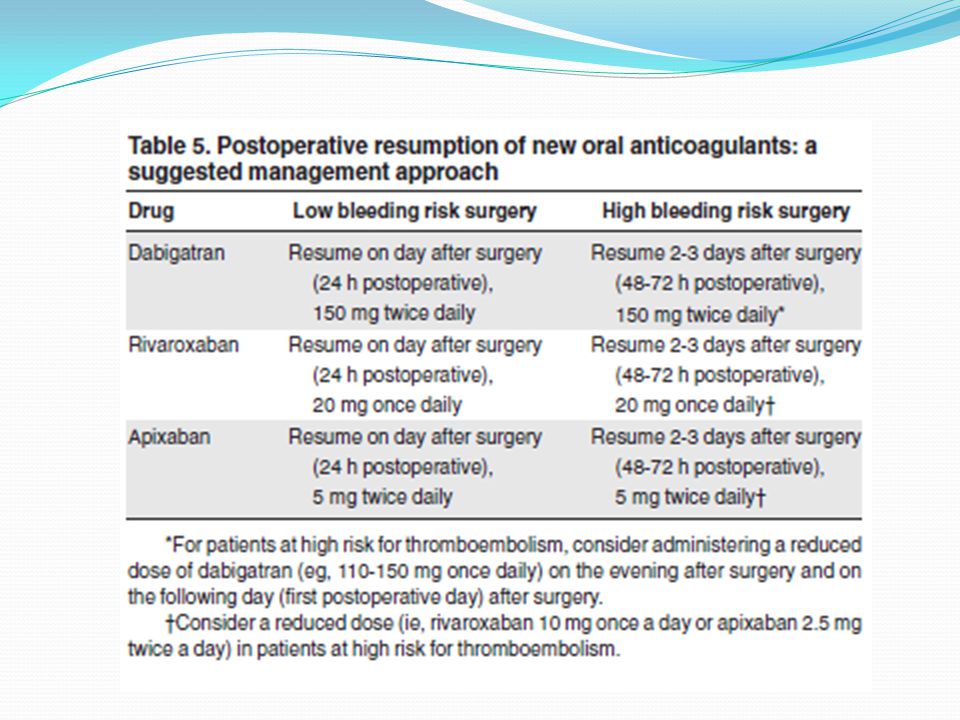
Τροποποίηση αγωγής Ο γιατρός της της βάζει dabigatran 110 mg 1 x 2
Διακοπή βεραπαμίλης Έναρξη νεμπιβολόλης 5 mg 1 x 1 Rythmonorm 150mg 1X3 Omeprazole 20mg 1X1

30
Possible drug-drug interactions – Effect on NOAC plasma levels part 1
Dabigatran Apixaban Edoxaban Rivaroxaban Atorvastatin P-gp/ CYP3A4 +18% no data yet no effect Digoxin P-gp Verapamil P-gp/ wk CYP3A4 +12–180% + 53% (slow release) minor effect Diltiazem +40% No data Quinidine +50% +80% Amiodarone +12–60% Dronedarone P-gp/CYP3A4 +70–100% +85% Ketoconazole; itraconazole; voriconazole; posaconazole; P-gp and BCRP/ CYP3A4 +140–150% +100% up to +160% Red – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations 19
 minor effect. Diltiazem. +40% No data. Quinidine. +50% +80% Amiodarone. +12–60% Dronedarone. P-gp/CYP3A4. +70–100% +85% Ketoconazole; itraconazole; voriconazole; posaconazole; P-gp and BCRP/ CYP3A –150% +100% up to +160% Red – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations")
31
Πορεία Η ασθενής ένα χρόνο μετά και έπειτα από διαλείποντα επεισόδια κοιλιακού άλγους υποβάλλεται σε υπέρηχο κοιλίας και διαγιγνώσκεται με χολολιθίαση Προγραμματίζεται για λαπαροσκοπική χολοκυστεκτομή

32
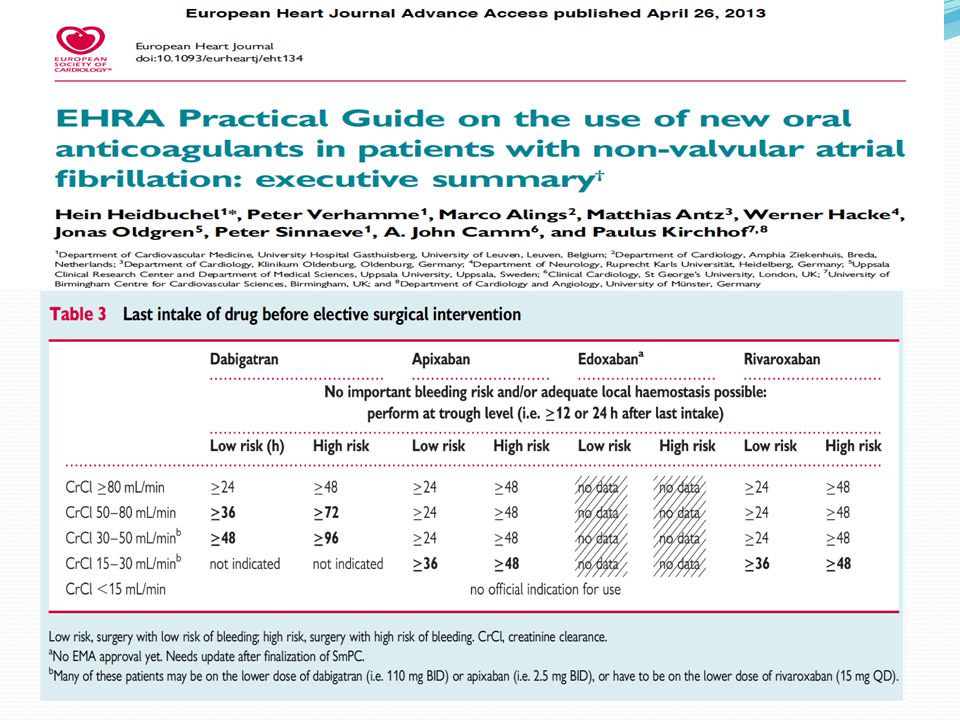
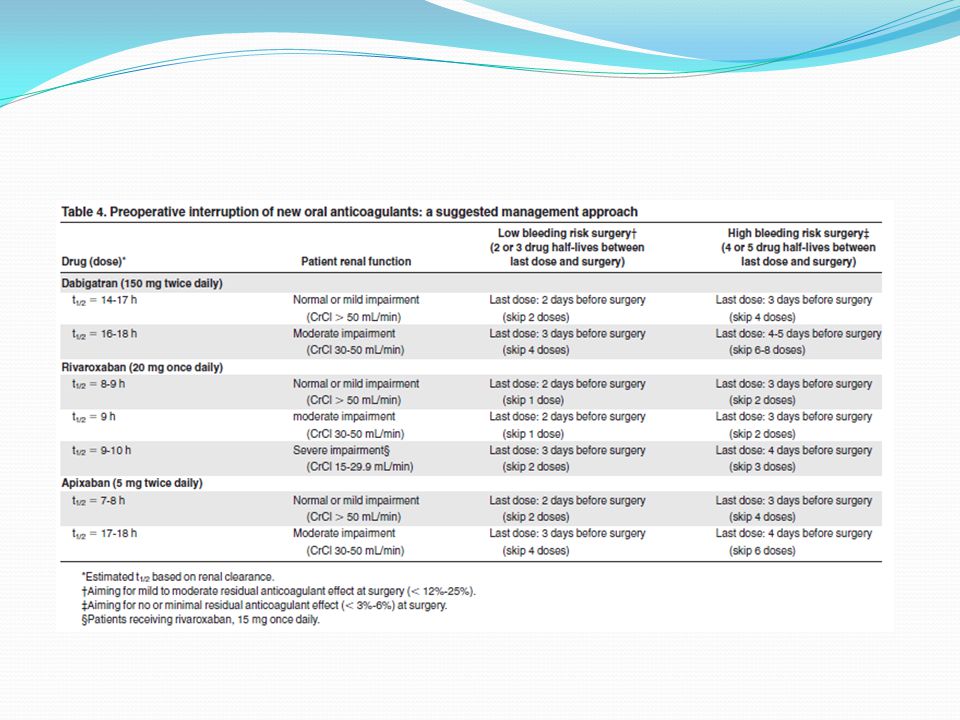
6) Πότε θα διακόψουμε την αντιπηκτική αγωγή πριν από την προγραμματισμένη επέμβαση;
1) 2 ημέρες πριν την επέμβαση για το dabigatran 2) Εξαρτάται από τη νεφρική λειτουργία της ασθενούς 3) 5 ημέρες προ της επέμβασης εφόσον χορηγείται κουμαρινικό αντιπηκτικό 4) 1 και 2 σωστά 5) 2 και 3 σωστά
 2 ημέρες πριν την επέμβαση για το dabigatran. 2) Εξαρτάται από τη νεφρική λειτουργία της ασθενούς. 3) 5 ημέρες προ της επέμβασης εφόσον χορηγείται κουμαρινικό αντιπηκτικό. 4) 1 και 2 σωστά. 5) 2 και 3 σωστά.")
33
Εκτίμηση αιμορραγικού κινδύνου

35
Patients with chronic kidney disease
Estimated t½ and AUC NOAC plasma concentrations compared to healthy controls Dabigatran Apixaban Edoxaban Rivaroxaban CrCl ≥ 60 ml/min CKD Stage I & II ~ 14 h 1 no data ~ 8.6 h 2 ~ 8.5 h 3 (+44%) CrCl 30–60 ml/min CKD Stage III ~ 18 h 1 ~ 9.4 h 2 ~ 9 h 3 (+52%) CrCl 15–30 ml/min CKD Stage IV ~ 28 h 1 ~ 16.9 h 2 ~ 9.5 h 3 (+64%) CrCl ≤ 15 ml/min CKD Stage V 1. Stangier et al, Clinical pharmacokinetics 2010;49: Ridout et al, J Clin Pharmacol 2009:49:1124 3. Kubitza et al, Br J Clin Pharmacol 2010:70:703-2 26
 CrCl 30–60 ml/min. CKD Stage III. ~ 18 h 1. ~ 9.4 h 2. ~ 9 h 3. (+52%) CrCl 15–30 ml/min. CKD Stage IV. ~ 28 h 1. ~ 16.9 h 2. ~ 9.5 h 3. (+64%) CrCl ≤ 15 ml/min. CKD Stage V. 1. Stangier et al, Clinical pharmacokinetics 2010;49: Ridout et al, J Clin Pharmacol 2009:49: Kubitza et al, Br J Clin Pharmacol 2010:70:")
36
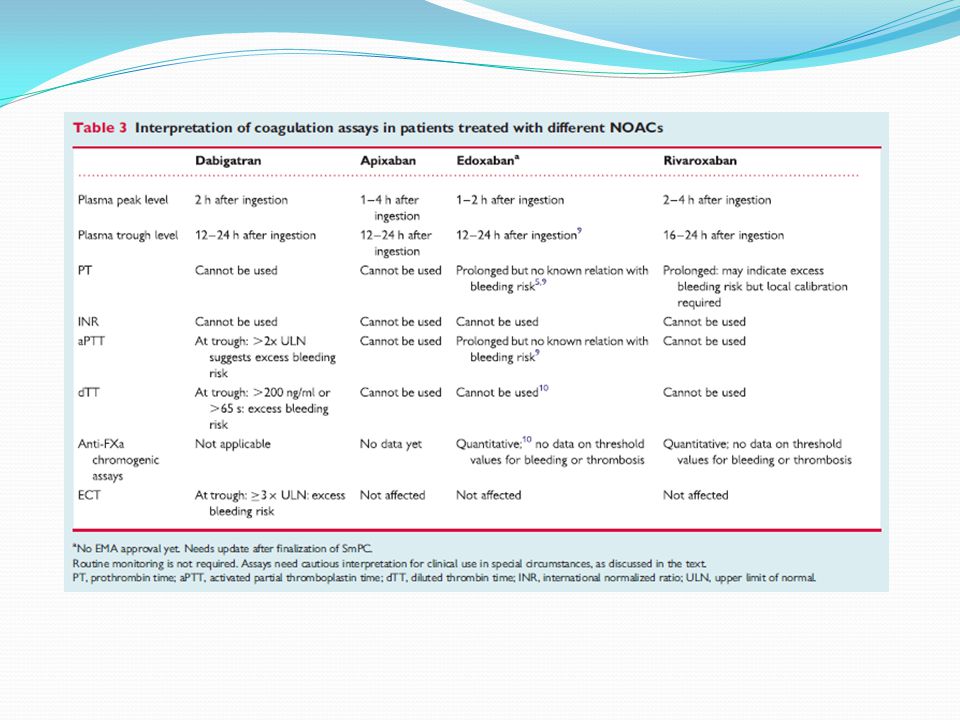
7) Αν η ασθενής έπρεπε να υποβληθεί σε επείγουσα χειρουργική επέμβαση ποιά από τις παρακάτω εξετάσεις θα βοηθούσε να εκτιμήσουμε τον αιμορραγικό κίνδυνο της ασθενούς; 1) aPTT 2) PT 3) INR 4) Anti Xa 5) Καμία από τις ανωτέρω
 aPTT. 2) PT. 3) INR. 4) Anti Xa. 5) Καμία από τις ανωτέρω.")
38
Measuring the anticoagulant effect of NOACs
Important to know exactly when NOAC was administered relative to time of blood sampling. Maximum effect at maximum plasma concentration (~3h after administration). Activated thromboplastin time (aPTT): qualitative assessment of dabigatran, but sensitivity varies. Diluted thrombin time (DTT): Hemoclot® suitable for quantitative assessment of dabigatran but no data on cut off below which surgery is safe. Anti-FXa chromogenic assays: commercially available for quantitative assessment, but no data to associate level with bleeding or thrombo- embolism risk. 11
. Activated thromboplastin time (aPTT): qualitative assessment of dabigatran, but sensitivity varies. Diluted thrombin time (DTT): Hemoclot® suitable for quantitative assessment of dabigatran but no data on cut off below which surgery is safe. Anti-FXa chromogenic assays: commercially available for quantitative assessment, but no data to associate level with bleeding or thrombo- embolism risk")
39
8) Αν η επέμβαση ήταν επείγουσα κ όχι προγραμματισμένη θα ήταν καλύτερα να λάμβανε η ασθενής κουμαρινικά; 1) ΝΑΙ 2) ΟΧΙ
 ΝΑΙ. 2) ΟΧΙ.")
40
Periprocedural outcomes subgroup analysis: rationale
A number of patients receiving anticoagulation will require a surgical procedure, so optimal management of Pradaxa® in the periprocedural period is an important consideration Patients should be managed to reduce the chance of unnecessary bleeding, whilst maintaining adequate levels of anticoagulation to prevent stroke Outcomes in patients from RE-LY® undergoing surgery/invasive procedures during the study were assessed

41
Periprocedural outcomes subgroup analysis: anticoagulation management
Warfarin managed according to local practice Pradaxa® withheld prior to procedure: Dec 2005 – Aug 2008: 24 hours for all patients Aug 2008 – Mar 2009: 2–5 days (based on CrCl) for high-risk procedures Pradaxa® restarted post-procedure after achieving adequate haemostasis Time from last anticoagulant dose to procedure: Pradaxa®: 49 (35–85) hours Warfarin: 114 (87–144) hours Periprocedural bridging with heparin used in 15.3% (110 mg BID), 17.0% (150 mg BID), and 28.5% (warfarin) of patients (P<0.001) Healey JS et al. Circulation 2012;126:343–8
 for high-risk procedures. Pradaxa® restarted post-procedure after achieving adequate haemostasis. Time from last anticoagulant dose to procedure: Pradaxa®: 49 (35–85) hours. Warfarin: 114 (87–144) hours. Periprocedural bridging with heparin used in 15.3% (110 mg BID), 17.0% (150 mg BID), and 28.5% (warfarin) of patients (P<0.001) Healey JS et al. Circulation 2012;126:343–8.")
42
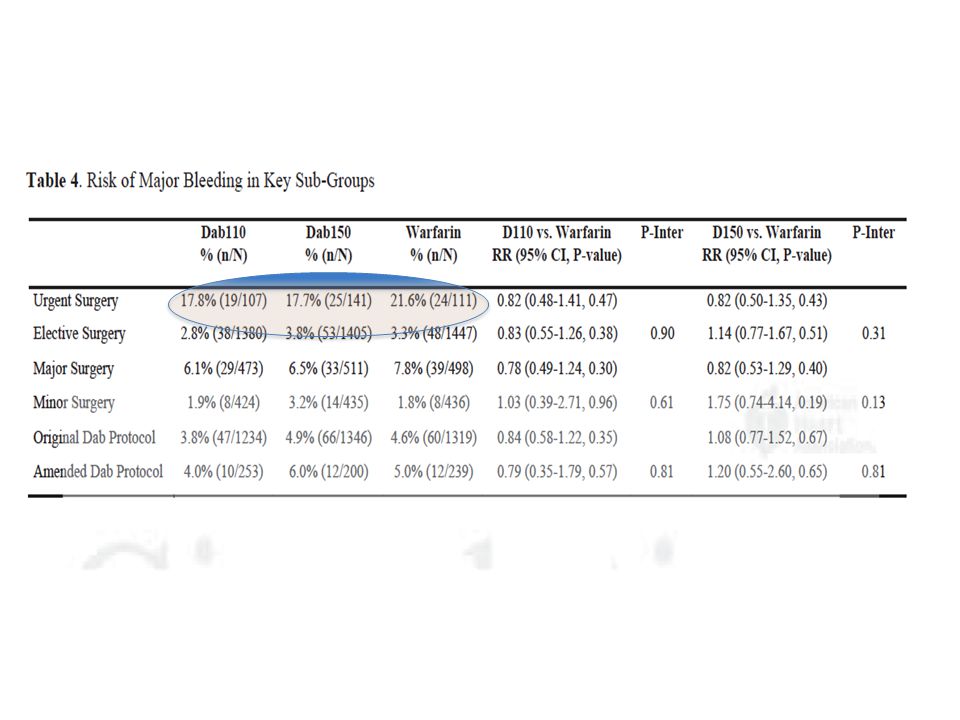
Periprocedural outcomes subgroup analysis: bleeding outcomes
No significant difference in risk of bleeding for either dose vs warfarin % patients P110 vs warfarin P150 vs warfarin P110 n=1487 P150 n=1546 Warfarin n=1558 RR (95% CI) P value P value Major bleeding 3.8 5.1 4.6 0.83 (0.59–1.17) 0.28 1.09 (0.80–1.49) 0.58 Fatal bleeding 0.2 0.1 1.57 (0.26–9.39) 0.62 1.01 (0.14–7.15) 0.99 Re-operation 0.6 1.4 1.0 0.59 (0.26–1.33) 0.20 1.39 (0.73–2.63) 0.32 Red blood cell transfusion 3.3 3.5 4.0 0.81 (0.56–1.18) 0.27 0.86 (0.60–1.23) 0.42 Minor bleeding 8.1 9.0 7.8 1.03 (0.81–1.31) 0.81 1.15 (0.91–1.45) 0.24 Both doses of Pradaxa® showed no significant difference in risk of bleeding, or bleeding-related events vs warfarin during the periprocedural period. P110 = Pradaxa® 110 mg twice daily; P150 = Pradaxa® 150 mg twice daily; Healey JS et al. Circulation 2012;126:343–8
 P value. P value. Major bleeding (0.59–1.17) (0.80–1.49) Fatal bleeding (0.26–9.39) (0.14–7.15) Re-operation (0.26–1.33) (0.73–2.63) Red blood cell transfusion (0.56–1.18) (0.60–1.23) Minor bleeding (0.81–1.31) (0.91–1.45) Both doses of Pradaxa® showed no significant difference in risk of bleeding, or bleeding-related events vs warfarin during the periprocedural period. P110 = Pradaxa® 110 mg twice daily; P150 = Pradaxa® 150 mg twice daily; Healey JS et al. Circulation 2012;126:343–8.")
43
Periprocedural outcomes subgroup analysis: thromboembolic events
Low incidence of thromboembolic events across all treatment groups % patients P110 vs warfarin P150 vs warfarin P110 n=1487 P150 n=1546 Warfarin n=1558 RR (95% CI) P value P value Ischaemic stroke or SE 0.5 1.05 (0.55–2.01) 0.89 1.01 (0.35–2.87) 0.99 Stroke (all cause) 0.6 0.73 (0.28–1.92) 0.53 0.71 (0.27–1.85) 0.48 SE 0.1 1.05 (0.07–16.7) 0.97 1.01 (0.06–16.1) 1.00 CV death 1.35 (0.50–3.61) 0.55 (0.35–2.96) The incidence of stroke and other thromboembolic complications was low, and did not differ significantly between treatment groups. P110 = Pradaxa® 110 mg twice daily; P150 = Pradaxa® 150 mg twice daily Healey JS et al. Circulation 2012;126:343–8
 P value. P value. Ischaemic stroke or SE (0.55–2.01) (0.35–2.87) Stroke (all cause) (0.28–1.92) (0.27–1.85) SE (0.07–16.7) (0.06–16.1) CV death (0.50–3.61) (0.35–2.96) The incidence of stroke and other thromboembolic complications was low, and did not differ significantly between treatment groups. P110 = Pradaxa® 110 mg twice daily; P150 = Pradaxa® 150 mg twice daily. Healey JS et al. Circulation 2012;126:343–8.")
47
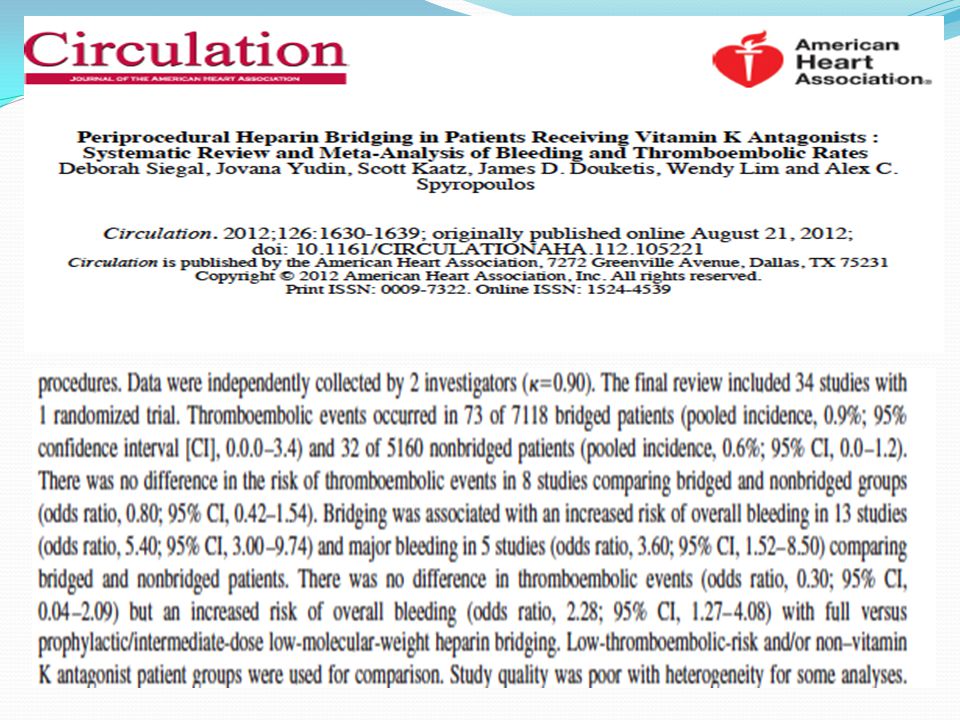
9) Είναι απαραίτητη η περιεπεμβατική γεφύρωση της αντιπηκτικής αγωγής με ΗΧΜΒ (bridging) στην ασθενή μας; 1) Ναι γιατί κάνω bridging σε όλους ως ρουτίνα 2) Όχι, διότι πρόκειται για ασθενή χαμηλού κινδύνου (CHADS2 < 3) 3) Όχι, διότι η ασθενής λαμβάνει NOAC 4) Ναι, αλλά μόνο μετά την επέμβαση 5) 2 κ 3
 Ναι γιατί κάνω bridging σε όλους ως ρουτίνα. 2) Όχι, διότι πρόκειται για ασθενή χαμηλού κινδύνου (CHADS2 < 3) 3) Όχι, διότι η ασθενής λαμβάνει NOAC. 4) Ναι, αλλά μόνο μετά την επέμβαση. 5) 2 κ 3.")
48
Καμία από τις ανωτέρω ● κίτρινες πλάκες του δέρματος των βλεφάρων
● οφείλονται σε εναπόθεση χοληστερόλης ● απαντούν και σε άτομα χωρίς υπερχοληστερολαιμία

53
Ongoing Studies…Stay Tuned
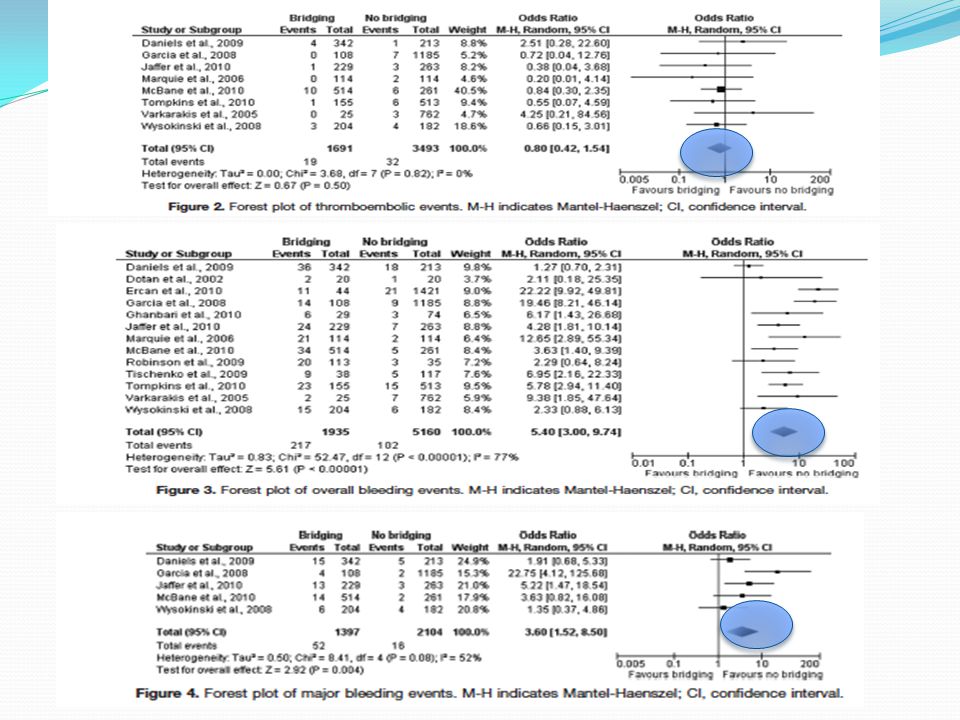
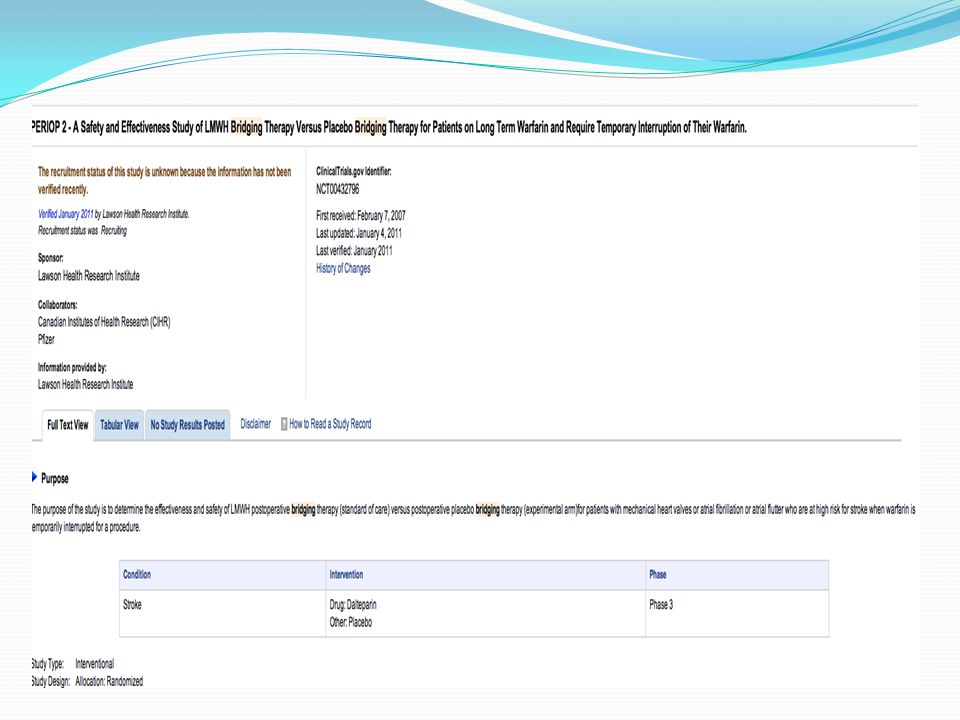
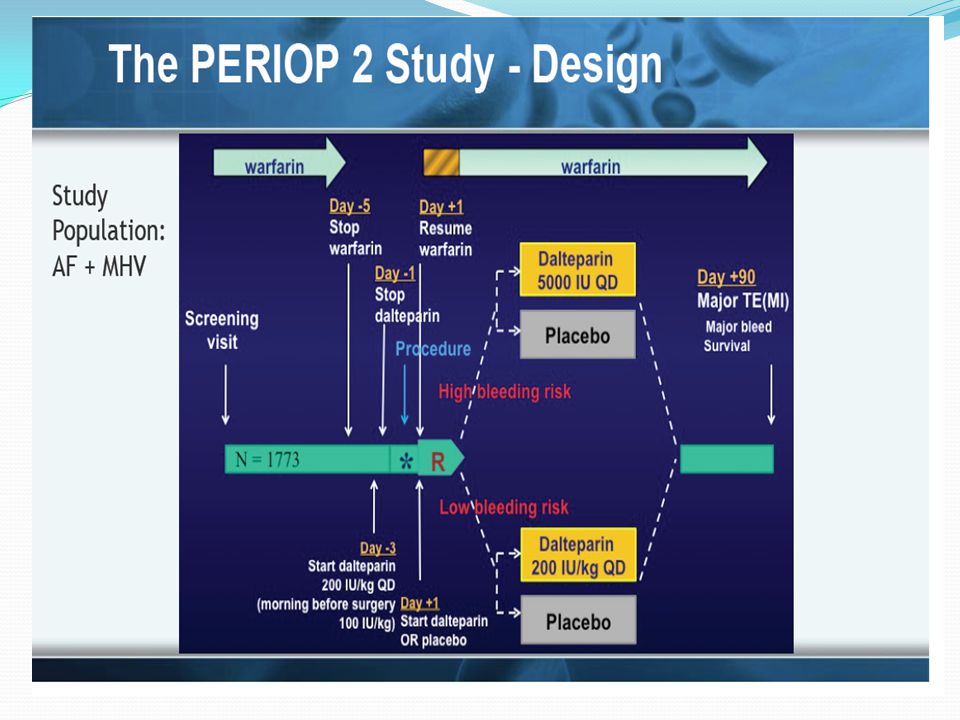
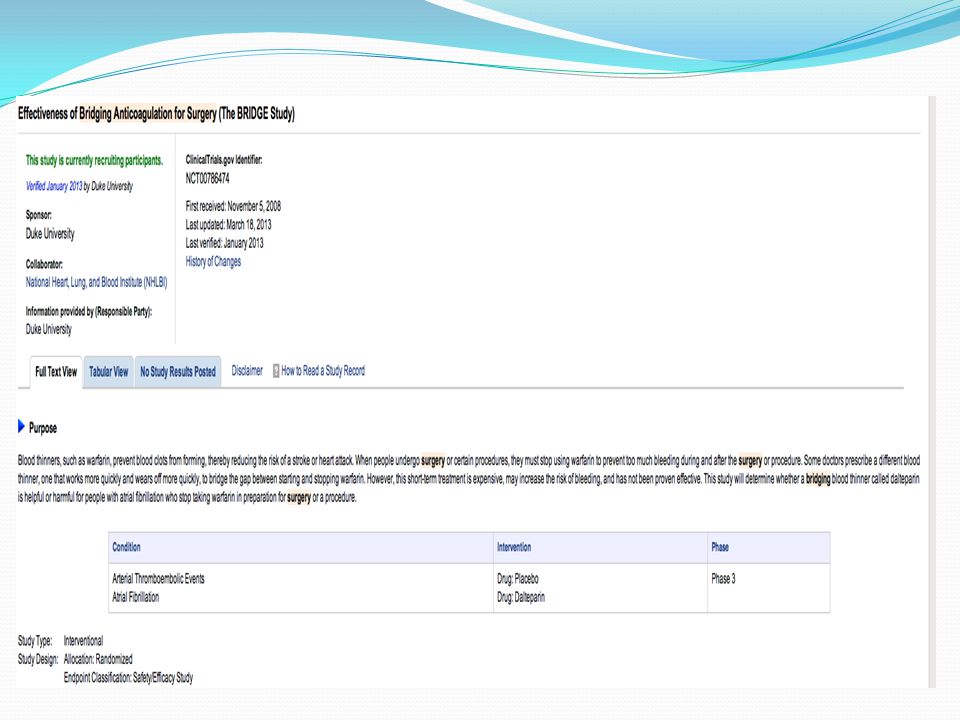
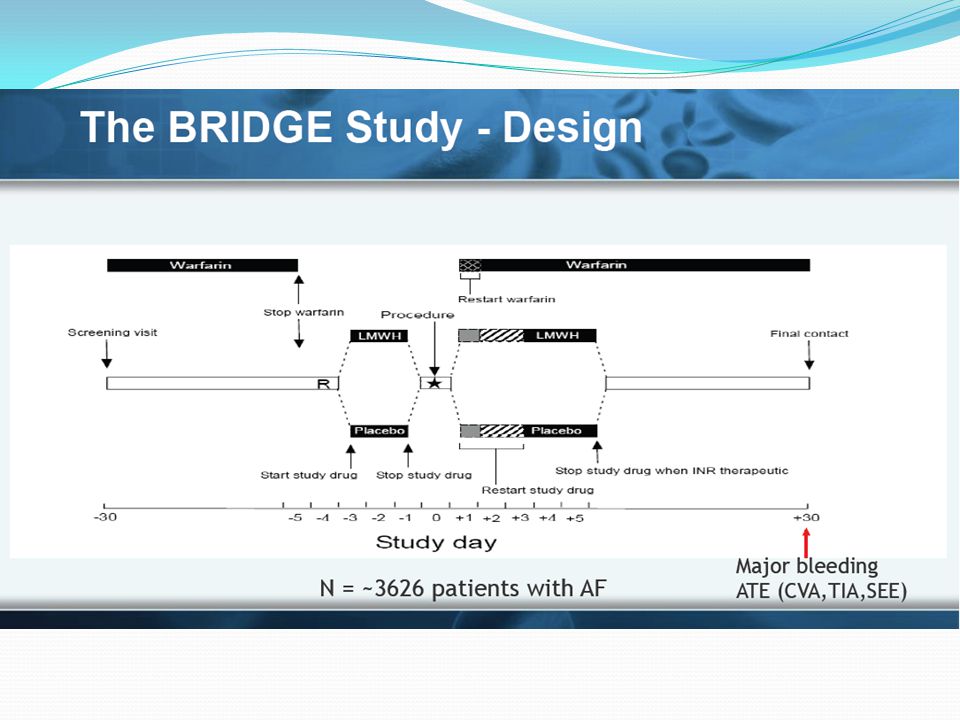
Randomized controlled trials (RCTs) are ongoing to establish best practices for patients who are receiving antithrombotic therapy and require surgery. RCTs are assessing the need for LMWH bridging in warfarin-treated patients who require surgery: PERIOP-2 (clinicaltrials.gov/NCT ) – funded by CIHR BRIDGE (clinicaltrials.gov/NCT ) – funded by NIH BRUISECONTROL (clinicaltrials.gov/NCT )
 are ongoing to establish best practices for patients who are receiving antithrombotic therapy and require surgery. RCTs are assessing the need for LMWH bridging in warfarin-treated patients who require surgery: PERIOP-2 (clinicaltrials.gov/NCT ) – funded by CIHR. BRIDGE (clinicaltrials.gov/NCT ) – funded by NIH. BRUISECONTROL (clinicaltrials.gov/NCT )")
60
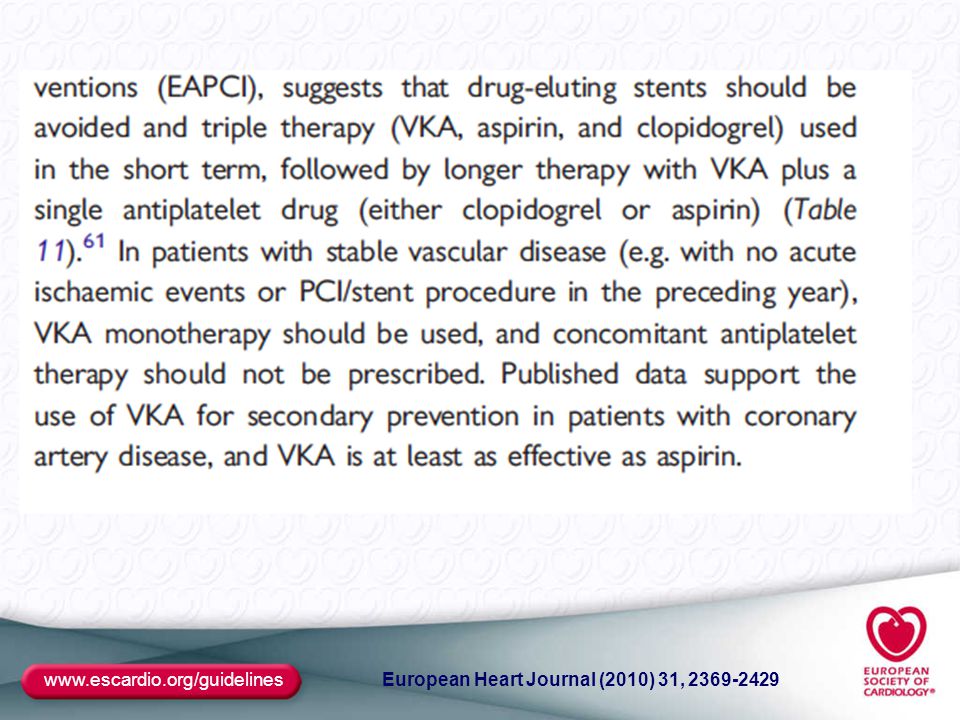
10) 3 χρόνια μετά και αφού η ασθενής έχει πέσει σε μόνιμη κολπική μαρμαρυγή, η ασθενής ξυπνάει με πόνο στο στήθος και στο εφημερεύον νοσοκομείο διαγιγνώσκεται STEMI και γίνεται πρωτογενής αγγειοπλαστική. Ποιά αγωγή θα ακολουθήσουμε; 1) Διπλή αντιαιμοπεταλική 2) Διπλή αντιαιμοπεταλική, Κουμαρινικά 3) Διπλή αντιαιμοπεταλική, Rivaroxaban 4) Διπλή αντιαιμοπεταλική, Dabigatran 5) Διπλή αντιαιμοπεταλική, Apixaban 6) Κλοπιδογρέλη, βαρφαρίνη
 Διπλή αντιαιμοπεταλική. 2) Διπλή αντιαιμοπεταλική, Κουμαρινικά. 3) Διπλή αντιαιμοπεταλική, Rivaroxaban. 4) Διπλή αντιαιμοπεταλική, Dabigatran. 5) Διπλή αντιαιμοπεταλική, Apixaban. 6) Κλοπιδογρέλη, βαρφαρίνη.")
64
WOEST ESC, Hotline III, Munchen, August 28th, 2012 The WOEST Trial: First randomised trial comparing two regimens with and without aspirin in patients on oral anticoagulant therapy undergoing coronary stenting Willem Dewilde, Tom Oirbans, Freek Verheugt, Johannes Kelder, Bart De Smet, Jean-Paul Herrman, Tom Adriaenssens, Mathias Vrolix, Antonius Heestermans, Marije Vis, Saman Rasoul, Kaioum Sheikjoesoef, Tom Vandendriessche, Carlos Van Mieghem, Kristoff Cornelis, Jeroen Vos, Guus Brueren, Nicolien Breet and Jurriën ten Berg The WOEST Trial= What is the Optimal antiplatElet and anticoagulant therapy in patients with oral anticoagulation and coronary StenTing (clinicaltrials.gov NCT ) |
 |")
65
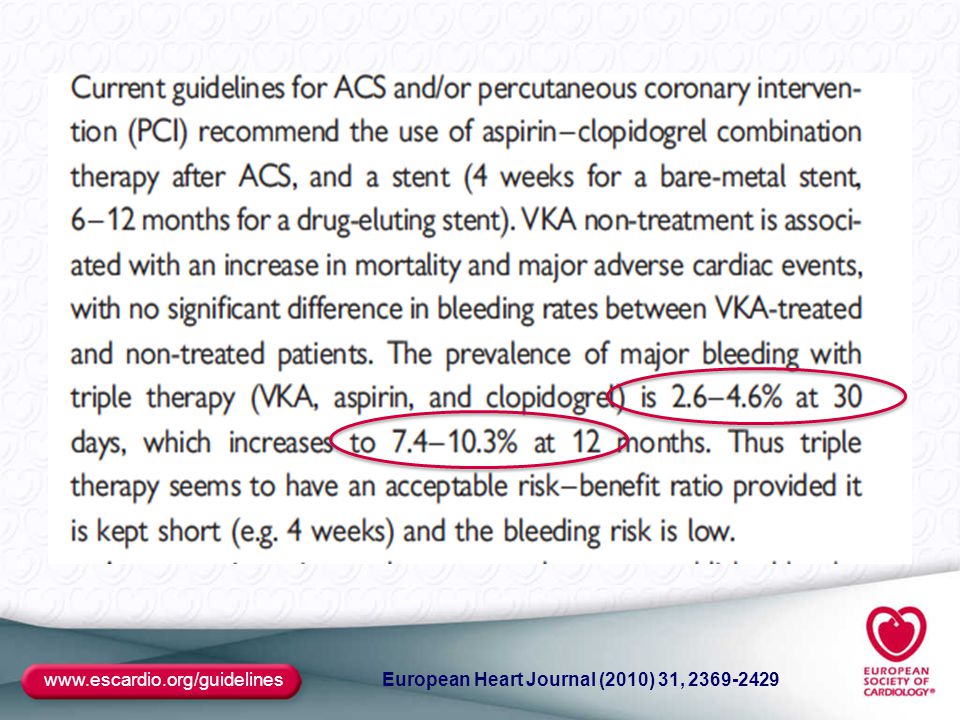
WOEST Background 1/ Long term oral anticoagulant therapy (OAC) is obligatory (class I) in: - most patients with atrial fibrillation - patients with mechanical heart valves 2/ Over 30% of these patients have concomitant ischemic heart disease. When these patients need to undergo percutaneous coronary stenting, there is also an indication for aspirin and clopidogrel. 3/ Triple therapy (OAC, aspirin and clopidogrel) is recommended according to the guidelines but is also known to increase the risk of major bleeding. Major bleeding increases mortality. 4/ No prospective data available. |
 is recommended according. to the guidelines but is also known to increase the risk of major bleeding. Major bleeding increases mortality. 4/ No prospective data available. |")
66
Study Design-1 WOEST Inclusion criteria:
1/ Indication for OAC for at least 1 year 2/ One coronary lesion eligible for PCI 3/ Age over 18 Exclusion criteria: 1/ History of intracranial bleeding 2/ Cardiogenic shock during hospitalisation 3/ Peptic ulcer in the previous 6 months 4/ TIMI major bleeding in the previous year 5/ Contra-indication for aspirin or clopidogrel 6/ Thrombocytopenia (platelet count less than 50,000 per ml) 7/ Pregnancy 8/ Age >80 |
 7/ Pregnancy. 8/ Age >80. |")
67
Study Design-2 WOEST 1:1 Randomisation: Double therapy group:
OAC + 75mg Clopidogrel qd 1 month minimum after BMS 1 year after DES Triple therapy group OAC + 75mg Clopidogrel qd + 80mg Aspirin qd 1 month minimum after BMS 1 year after DES Follow up: 1 year Primary Endpoint: The occurence of all bleeding events (TIMI criteria) Secondary Endpoints: Combination of stroke, death, myocardial infarction, stent thrombosis and target vessel revascularisation - All individual components of primary and secondary endpoints |
 Secondary Endpoints: Combination of stroke, death, myocardial infarction, stent thrombosis and. target vessel revascularisation. - All individual components of primary and secondary endpoints. |")
68
Primary Endpoint: Total number of TIMI bleeding events
WOEST Primary Endpoint: Total number of TIMI bleeding events Days Cumulative incidence of bleeding 30 60 90 120 180 270 365 0 % 10 % 20 % 30 % 40 % 50 % 284 210 194 186 181 173 159 140 n at risk: 279 253 244 241 236 226 208 Triple therapy group Double therapy group 44.9% 19.5% p<0.001 HR= %CI[ ] |

69
Bleeding in triple therapy group and aspirin compliance
WOEST Bleeding in triple therapy group and aspirin compliance Days free fromany TIMI bleeds 30 60 90 120 180 270 365 0 % 25 % 50 % 75 % 100 % 284 210 194 186 181 173 159 140 n at risk: 279 253 244 241 236 226 208 Triple therapy group Double therapy group Free from bleeding curve Triple therapy group Days 30 60 90 120 180 270 365 OAC Clopidogrel Aspirin The Kaplan Meier curve of the aspirin compliance is comparable to the reversed curve of the bleeding events in the triple therapy group

70
Secondary Endpoint (Death, MI,TVR, Stroke, ST)
WOEST Secondary Endpoint (Death, MI,TVR, Stroke, ST) Days Cumulative incidence 30 60 90 120 180 270 365 0 % 5 % 10 % 15 % 20 % 284 272 266 261 252 242 223 n at risk: 279 276 273 263 258 234 Triple therapy group Double therapy group 17.7% 11.3% p=0.025 HR= %CI[ ]
 Days. Cumulative incidence % 5 % 10 % 15 % 20 % n at risk: Triple therapy group. Double therapy group. 17.7% 11.3% p= HR= %CI[ ]")
71
All-Cause Mortality WOEST Triple therapy group Double therapy group
7.5 % Triple therapy group Double therapy group 6.4% HR= %CI[ ] p=0.027 5 % Cumulative incidence of death 2.6% 2.5 % 0 % 30 60 90 120 180 270 365 Days n at risk: 284 281 280 280 279 277 270 252 279 278 276 276 276 275 274 256

72
WOEST Conclusions First randomized trial to address the optimal antiplatelet therapy in patients on OAC undergoing coronary stenting In this study which was specifically designed to detect bleeding events, the bleeding rate was higher than expected Primary endpoint was met: OAC plus clopidogrel causes less bleeding than triple antithrombotic therapy, but now shown in a randomized way Secondary endpoint was met: with double therapy there is no excess of thrombotic/thromboembolic events: stroke, stent thrombosis, target vessel revascularisation, myocardial infarction or death Less all-cause mortality with double therapy |

73
● κίτρινες πλάκες του δέρματος των βλεφάρων
● οφείλονται σε εναπόθεση χοληστερόλης ● απαντούν και σε άτομα χωρίς υπερχοληστερολαιμία

74
Ευχαριστώ πολύ για την προσοχή σας

Παρόμοιες παρουσιάσεις

 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")


















