Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Αντιβιοτικά Αντιιικά - Αντιμυκητιασικά
Αντιβιοτικά Αντιιικά - Αντιμυκητιασικά Γ. Ντάιος

2
CASE 1 TMP-SMX is excreted in the urine
TMP-SMX should not be given to patients who have folic acid deficiency or who are pregnant TMP-SMX should also not be given to patients with glucose-6-phosphate dehydrogenase deficiency

3
Παίρνουμε ΠΑΝΤΑ καλλιέργειες πριν την έναρξη αντιβιοτικής αγωγής

4
they inhibit successive steps in the folate synthesis pathway (see diagram below).
Folic acid is an essential precursor in the de novo synthesis of the DNA nucleosides thymidine and uridine. Bacteria are unable to take up folic acid from the environment (i.e., the infection host) and, thus, are dependent on their own de novo synthesis - inhibition of the enzyme starves the bacteria of two bases necessary for DNA replication and transcription.
 and, thus, are dependent on their own de novo synthesis - inhibition of the enzyme starves the bacteria of two bases necessary for DNA replication and transcription.")
5
Trimethoprim-Sulphomethoxazole
Απεκκρίνεται στα ούρα Δραστικό έναντι πολλών gr- και gr+ βακτηρίων. Δεν πρέπει να χορηγείται σε άτομα με έλλειψη φυλικού οξέος ή σε εγκυμονούσες Δεν πρέπει να χορηγείται σε άτομα με έλλειψη της G-6-PD

6
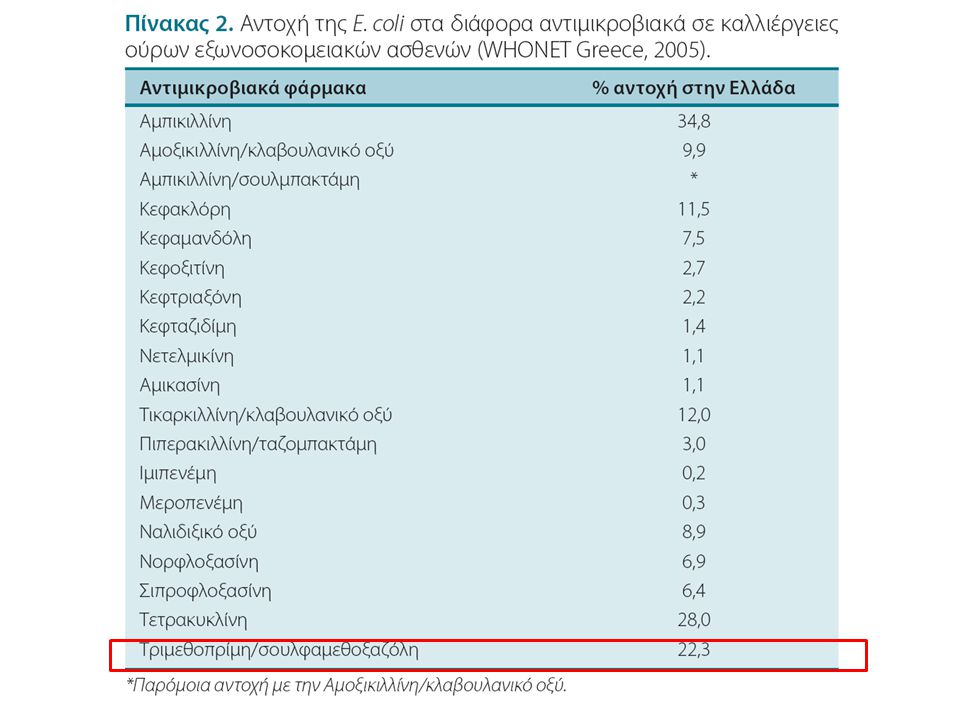
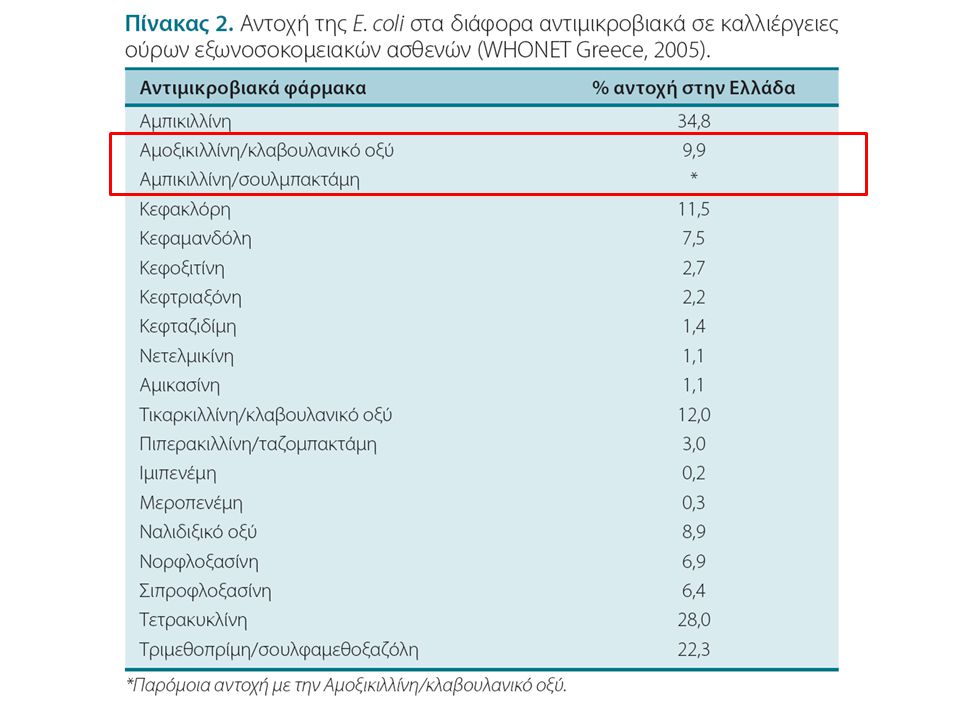
Ποιο είναι το συχνότερο ουροπαθογόνο;

7
Susceptible to cotrimoxazole

11
Some gram- (Neisseria) Treponema pallidum (ωχρό τρεπόνημα)
Penicillin gram+ Some gram- (Neisseria) Treponema pallidum (ωχρό τρεπόνημα) Alexander Flemming Penicillin active against gram+ cocci and some gram- bacteria (neisseria), treponema pallidum Beta-lactams: Penicillins, cephalosporins, monobactams, carbapenems, b-lactamase inhibitors.
 Treponema pallidum (ωχρό τρεπόνημα) Alexander Flemming. Penicillin active against gram+ cocci and some gram- bacteria (neisseria), treponema pallidum. Beta-lactams: Penicillins, cephalosporins, monobactams, carbapenems, b-lactamase inhibitors.")
12
Penicillins Pneumococcus, enterococcus, N. meningitidis, syphilis, listeria, leptospirosis, αναερόβια στόματος Penicillin G, penicillin V (p.o.), procaine penicillin, benzathine penicillin. Benzathine penicillin (Penadur): μακράς δράσης (κάθε 2-4 εβδομάδες) σε σύφιλη, λοιμώδη ενδοκαρδίτιδα, πρόληψη υποτροπής οξέος ρευματικού πυρετού Συνεργική δράση με τις αμινογλυκοσίδες Penicillin V (Ospen)
, procaine penicillin, benzathine penicillin. Benzathine penicillin (Penadur): μακράς δράσης (κάθε 2-4 εβδομάδες) σε σύφιλη, λοιμώδη ενδοκαρδίτιδα, πρόληψη υποτροπής οξέος ρευματικού πυρετού. Συνεργική δράση με τις αμινογλυκοσίδες. Penicillin V (Ospen)")
14
Aminopenicillins extended penicillin’s spectrum to cover more the gram-

15
Aminopenicillins Αμπικιλλίνη, αμοξυκιλλίνη.
Υδρολύονται από τις β-λακταμάσες. Σύνηθες φάσμα της πενικιλλίνης, και επίσης: E.coli, Proteus, H. influenza, H. pylori, N. meningitidis, Shigella, Klebsiella Ιλαροειδές εξάνθημα σε ασθενείς με λοιμώδη μονοπυρήνωση

17
Sulbactam Tazobactam

19
Πενικιλλίνες σε συνδυασμό με αναστολείς των β-λακταμασών
Αμοξυκιλλίνη + κλαβουλανικό οξύ Τικαρκιλλίνη + κλαβουλανικό οξύ * Αμπικιλλίνη + σουλμπακτάμη Πιπερακιλλίνη + ταζομπακτάμη *

20
Αντισταφυλοκοκκικές πενικιλλίνες
Μεθικιλλίνη Οξακιλλίνη Κλοξακιλλίνη Δικλοξακιλλίνη Φλούκλοξακιλλίνη Ναφκιλλίνη Δραστικές έναντι των σταφυλοκοκκικών πενικιλλινασών MSSA: Methicillin-Sensitive Staphylococcus Aureus MRSA: Methicillin-Resistant Staphylococcus Aureus

21
Κεφαλοσπορίνες (Α’, Β’, Γ’, Δ’ γενιάς)
Προοδευτικά το φάσμα δραστικότητας μετακινείται από τα gr+ προς τα gr-. Προοδευτικά η αντοχή στις β-λακταμάσες αυξάνεται. Δραστικότητα έναντι της ψευδομονάδος: κεφταζιδίμη (Γ’), κεφεπίμη (Δ’) A’ πολύ καλή δράση έναντι gr+. Υδρολύονται από τις πενικιλλινάσες B’ Αντοχή στις β-λακταμάσες Γ’ Αντοχή στις β-λακταμάσες, αλλά υδρολύονται από τις ESBL (Extended Spectrum beta-lactamases) Δ’ Αντοχή και στις ESBLs.
, κεφεπίμη (Δ’) A’ πολύ καλή δράση έναντι gr+. Υδρολύονται από τις πενικιλλινάσες. B’ Αντοχή στις β-λακταμάσες. Γ’ Αντοχή στις β-λακταμάσες, αλλά υδρολύονται από τις ESBL (Extended Spectrum beta-lactamases) Δ’ Αντοχή και στις ESBLs.")
22
CASE 1 (cont)
")
23
Clostridia are anaerobic, spore-forming gr+ rods (bacilli)
")
24
VRE, VISA, VRSA Vancomycin is a glycopeptide antibiotic

25
Clostridium difficile
Τα ελάχιστα επίπεδα πρέπει να είναι τουλάχιστον 10 mg/L και τα μέγιστα 30 mg/L. Vancomycin must be given intravenously (IV) for systemic therapy, since it does not cross through the intestinal lining. Vancomycin must be administered in a dilute solution slowly, over at least 60 minutes (maximum rate of 10 mg/minute for doses >500 mg).[17] This is due to the high incidence of pain andthrombophlebitis and to avoid an infusion reaction known as the red man syndrome or red neck syndrome. This syndrome, usually appearing within 4–10 minutes after the commencement or soon after the completion of an infusion, is characterized by flushing and/or an erythematous rash that affects the face, neck, and upper torso. These findings are due to non-specific mast cell degranulation and are not an IgE-mediated allergic reaction. Less frequently, hypotension and angioedema may also occur. Symptoms may be treated or prevented with antihistamines, including diphenhydramine, and are less likely to occur with slow infusion.[26][27]:120-1 Clostridium difficile MRSA: Methicillin Resistant Staphylococcus Aureus
 for systemic therapy, since it does not cross through the intestinal lining. Vancomycin must be administered in a dilute solution slowly, over at least 60 minutes (maximum rate of 10 mg/minute for doses >500 mg).[17] This is due to the high incidence of pain andthrombophlebitis and to avoid an infusion reaction known as the red man syndrome or red neck syndrome. This syndrome, usually appearing within 4–10 minutes after the commencement or soon after the completion of an infusion, is characterized by flushing and/or an erythematous rash that affects the face, neck, and upper torso. These findings are due to non-specific mast cell degranulation and are not an IgE-mediated allergic reaction. Less frequently, hypotension and angioedema may also occur. Symptoms may be treated or prevented with antihistamines, including diphenhydramine, and are less likely to occur with slow infusion.[26][27]: Clostridium difficile. MRSA: Methicillin Resistant Staphylococcus Aureus.")
26
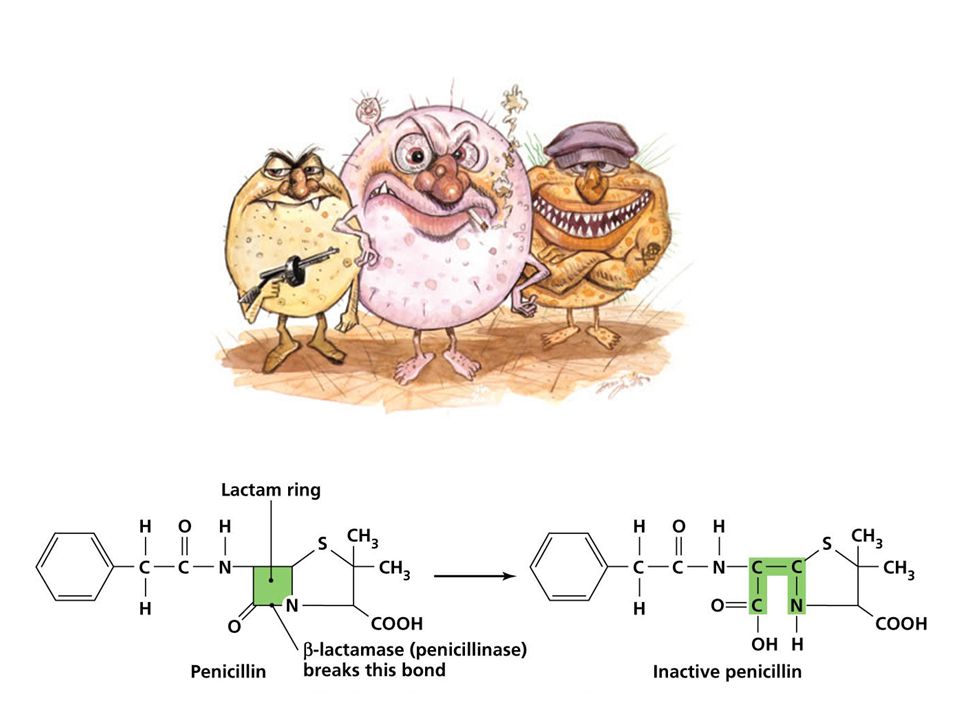
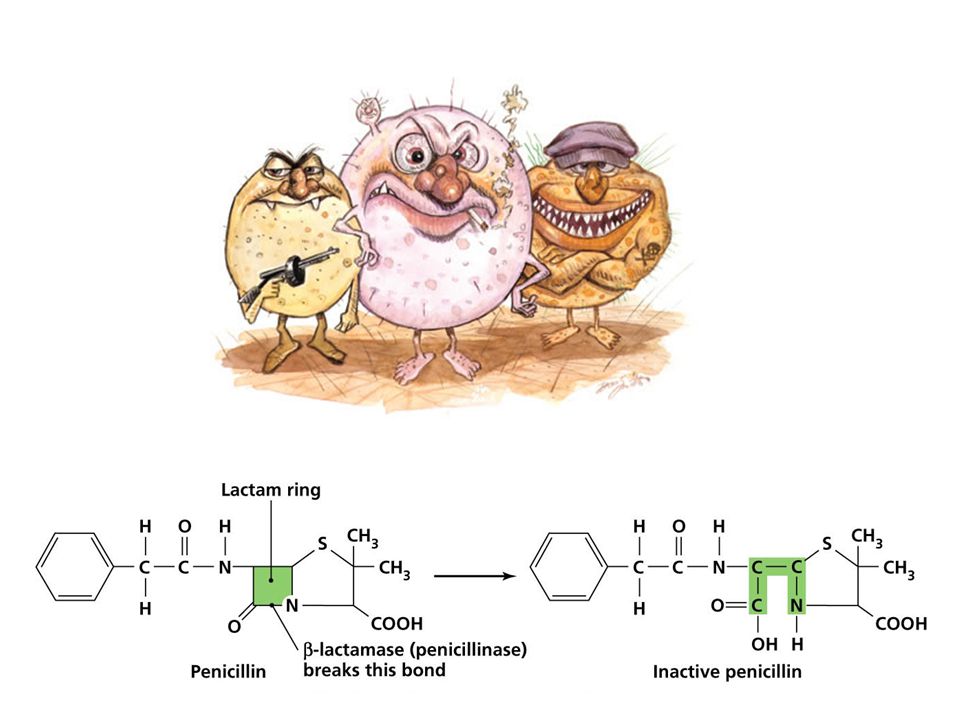
Penicillin Penicillinase

28
Methicillin/Oxacillin
Vancomycin Methicillin/Oxacillin (MSSA) MRSA Penicillin Penicillinase
 MRSA. Penicillin. Penicillinase.")
30
Teicoplanin, Linezolid, Daptomycine, Tigecycline Methicillin/Oxacillin
Vancomycin VRSA, VISA, VRE Methicillin/Oxacillin (MSSA) MRSA Penicillin Penicillinase
 MRSA. Penicillin. Penicillinase.")
31
Τεϊκοπλανίνη (Targocid)
Η τεϊκοπλανίνη και η βανκομυκίνη έχουν το ίδιο αντιμικροβιακό φάσμα και την ίδια αποτελεσματικότητα Η τεϊκοπλανίνη έχει μεγαλύτερο χρόνο ημίσειας ζωής και μπορεί να χορηγηθεί άπαξ ημερησίως Δοσολογία: 6 mg/kg (∼400 mg) άπαξ την πρώτη ημέρα 3 mg/kg (∼200 mg) στη συνέχεια
 άπαξ την πρώτη ημέρα. 3 mg/kg (∼200 mg) στη συνέχεια.")
32
Λινεζολίδη (Zyvoxid) Συνθετική οξαζολιδινόνη. Βακτηριοστατική δράση.
Συνδέεται στο 50S τμήμα του ριβοσώματος και αναστέλει την βακτηριακή πρωτεϊνοσύνθεση. 1/3 των ασθενών που λαμβάνουν λινεζολίδη παρουσιάζει θρομβοπενία Δοσολογία: 600 mg X2 ημερησίως (IV ή p.o.) Δεν χρειάζεται ρύθμιση σε νεφρική ή ηπατική βλάβη
 Δεν χρειάζεται ρύθμιση σε νεφρική ή ηπατική βλάβη.")
33
Δαπτομυκίνη (Cubicin)
Κυκλικό λιποπεπτίδιο Έντονη βακτηριοκτόνος δράση Προκαλεί calcium-dependent εκπόλωση του βακτηριακού κυτταρικού τοιχώματος. Αδρανοποιείται από την επιφανειοδραστική ουσία στις κυψελίδες, και επομένως δεν πρέπει να χρησιμοποιείται σε πνευμονικές λοιμώξεις Μπορεί να προκαλέσει αύξηση της CPK και μυοπάθεια.

34
Τυγεκυκλίνη (Tygacil)
Βακτηριοστατικό, αναστέλει την πρωτεϊνοσύνθεση των μικροβίων Ανήκει στις γλυκυλκυκλίνες (μοιάζει με τις τετρακυκλίνες) Ευρύ φάσμα (gr+, gr-, αναερόβια, αλλά όχι pseudomonas) Δοσολογία: Δόση εφόδου: 100 mg IV 50 mg IV κάθε 12 ώρες. Μεταβολίζεται στο ήπαρ και απεκκρίνεται μέσω των χοληφόρων. Η δόση πρέπει να μειώνεται στο μισό σε ασθενείς με σοβαρή ηπατική ανεπάρκεια (Child-Pugh C). Αντίθετα, δεν χρειάζεται τροποποίηση της δόσης σε ασθενείς με νεφρική ανεπάρκεια. Είναι γενικά καλά ανεκτή και δεν χρειάζεται παρακολούθηση των επιπέδων
 Ευρύ φάσμα (gr+, gr-, αναερόβια, αλλά όχι pseudomonas) Δοσολογία: Δόση εφόδου: 100 mg IV. 50 mg IV κάθε 12 ώρες. Μεταβολίζεται στο ήπαρ και απεκκρίνεται μέσω των χοληφόρων. Η δόση πρέπει να μειώνεται στο μισό σε ασθενείς με σοβαρή ηπατική ανεπάρκεια (Child-Pugh C). Αντίθετα, δεν χρειάζεται τροποποίηση της δόσης σε ασθενείς με νεφρική ανεπάρκεια. Είναι γενικά καλά ανεκτή και δεν χρειάζεται παρακολούθηση των επιπέδων.")
35
CASE 2 Amoxicillin/Clavulanate για 7 ημέρες
Patient with pneumonia, received augmentin Amoxicillin/Clavulanate για 7 ημέρες

37
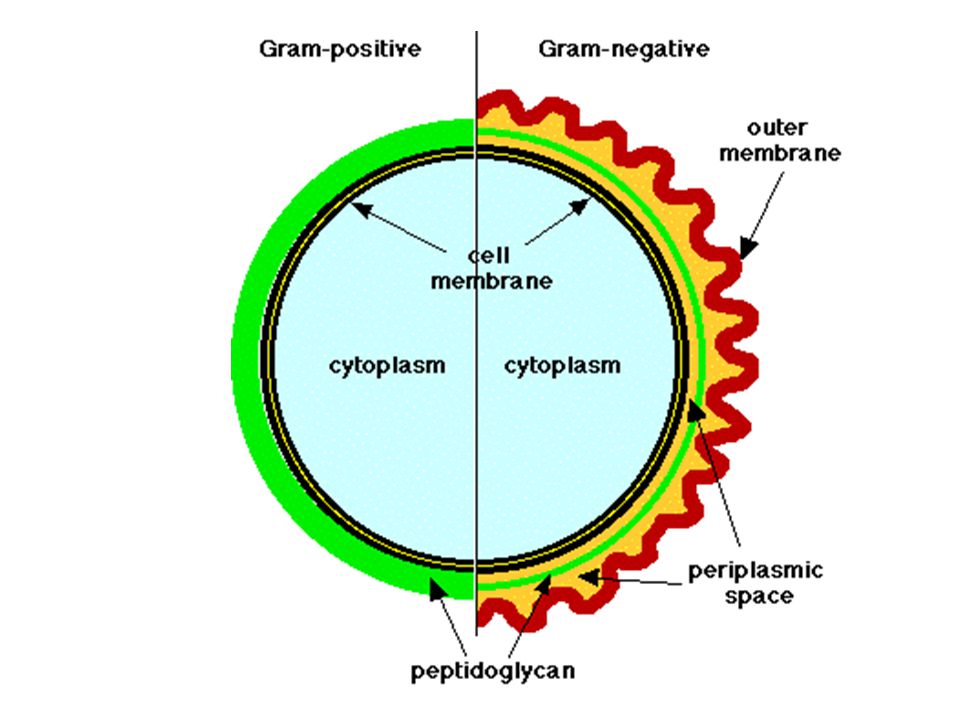
Left: Cell structure of chlamydia
Right: Mechanism of action of b-lactams

38
The mechanism of action of the newer macrolides is similar to that of erythromycin. They bind to the 50S subunit of bacterial ribosomes, leading to inhibition of transpeptidation, translocation, chain elongation and, ultimately, bacterial protein synthesis [1,2]. Compared to clarithromycin, azithromycin is typically given for a shorter period because of the long intracellular half-life (40 to 68 hours) and slow release from tissue sites. Thus, for many infections, a once-daily, five day regimen is as effective as 10 day courses of the other macrolides.
![The mechanism of action of the newer macrolides is similar to that of erythromycin. They bind to the 50S subunit of bacterial ribosomes, leading to inhibition of transpeptidation, translocation, chain elongation and, ultimately, bacterial protein synthesis [1,2].](http://slideplayer.gr/slide/1897121/7/images/38/The+mechanism+of+action+of+the+newer+macrolides+is+similar+to+that+of+erythromycin.+They+bind+to+the+50S+subunit+of+bacterial+ribosomes%2C+leading+to+inhibition+of+transpeptidation%2C+translocation%2C+chain+elongation+and%2C+ultimately%2C+bacterial+protein+synthesis+%5B1%2C2%5D..jpg "Compared to clarithromycin, azithromycin is typically given for a shorter period because of the long intracellular half-life (40 to 68 hours) and slow release from tissue sites. Thus, for many infections, a once-daily, five day regimen is as effective as 10 day courses of the other macrolides.")
39
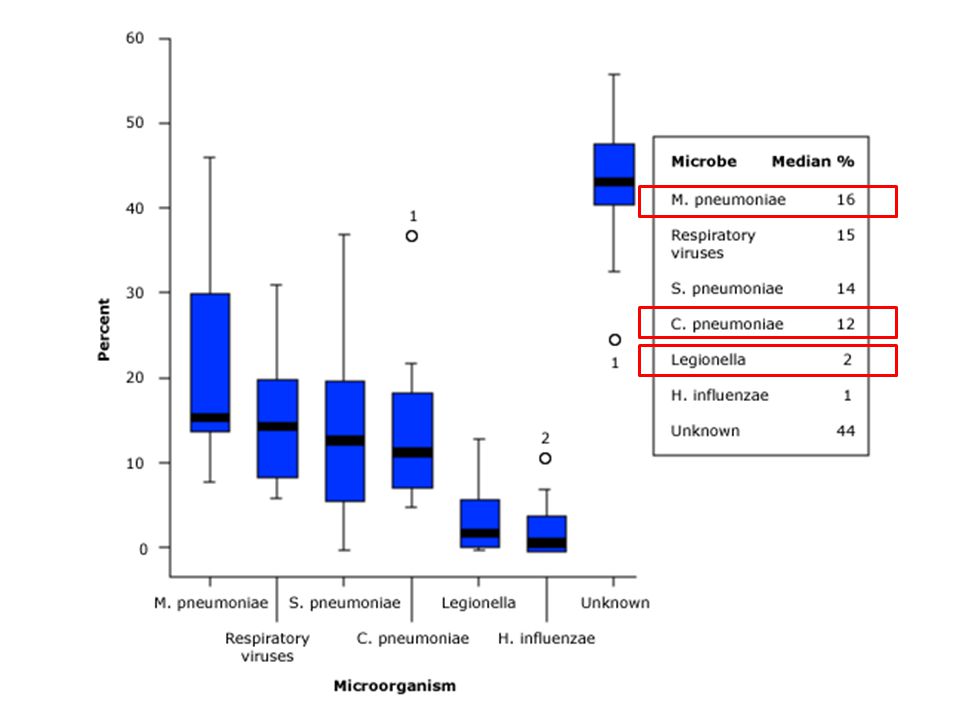
erythromycin-sensitive S. pneumoniae
MACROLIDE SPECTRUM erythromycin-sensitive S. pneumoniae Haemophilus spp, Moraxella catarrhalis Atypical pneumonia pathogens Legionella pneumophila Chlamydia pneumoniae Mycoplasma pneumoniae Gram-negative bacteria Escherichia coli Salmonella spp Yersinia enterocolitica Shigella spp Campylobacter jejuni Vibrio cholerae Neisseria gonorrhoeae Helicobacter pylori. The mechanism of action of the newer macrolides is similar to that of erythromycin. They bind to the 50S subunit of bacterial ribosomes, leading to inhibition of transpeptidation, translocation, chain elongation and, ultimately, bacterial protein synthesis [1,2].

40
The greatest use of the macrolides is in upper respiratory tract infections; azithromycin, clarithromycin, and telithromycin have activity against erythromycin-sensitive S. pneumoniae, Haemophilus spp, Moraxella catarrhalis, and atypical pneumonia pathogens including Legionella pneumophila, Chlamydophila (formerly Chlamydia) pneumoniae, and Mycoplasma pneumoniae. The gram-negative spectrum includes activity against Escherichia coli, Salmonella spp, Yersinia enterocolitica, Shigella spp, Campylobacter jejuni, Vibrio cholerae, Neisseria gonorrhoeae, and Helicobacter pylori.

41
Γιατί όχι μονοθεραπεία με μακρολίδες?
Η αντοχή του S. pneumoniae στις μακρολίδες προσεγγίζει το 40%. Γιατί όχι αμινογλυκοσίδες? Η δράση των αμινογλυκοσιδών είναι περιορισμένη σε περιβάλλον με χαμηλό (όξινο) pH (π.χ. πνεύμονες, βρογχικές εκκρίσεις) The mechanism of action of the newer macrolides is similar to that of erythromycin. They bind to the 50S subunit of bacterial ribosomes, leading to inhibition of transpeptidation, translocation, chain elongation and, ultimately, bacterial protein synthesis [1,2]. - Γιατί η κινολόνες είναι δεύτερη επιλογή; prevent resistance
 pH (π.χ. πνεύμονες, βρογχικές εκκρίσεις) The mechanism of action of the newer macrolides is similar to that of erythromycin. They bind to the 50S subunit of bacterial ribosomes, leading to inhibition of transpeptidation, translocation, chain elongation and, ultimately, bacterial protein synthesis [1,2]. - Γιατί η κινολόνες είναι δεύτερη επιλογή; prevent resistance.")
42
Gentamicin Tobramycin Amikacin Streptomycin Neomycin Kanamycin
Βακτηριοκτόνος δράση έναντι gr- (κυρίως) αλλά και gr+ (ανεπαρκής δράση). Συγκαταλέγονται: pseudomonas aeruginosa, hemophilus influenza). Σημαντική συνέργεια με τα β-λακταμικά αντιβιοτικά (θα πρέπει να μεσολαβεί μεσοδιάστημα 3 ωρών επειδή οι πενικιλλίνες αδρανοποιούν τις αμινογλυκοσίδες) Η ανάπτυξη ανθεκτικότητας των μικροβίων δεν είναι ιδιαίτερο πρόβλημα Χρησιμοποιούνται κυρίως σε σοβαρές λοιμώξεις (σήψη, επιπλεγμένες ουρολοιμώξεις, οστεομυελίτιδες) STOP όταν ταυτοποιηθεί ο μικροοργανισμός Η δράση των αμινογλυκοσιδών είναι περιορισμένη σε περιβάλλον με χαμηλό (όξινο) pH (π.χ. πνεύμονες, βρογχικές εκκρίσεις NOT per os. Monitor levels (Trough and Peak levels) Nephro toxicity Oto toxicity (ίλιγγος, αταξία) Neuro toxicity (νευρομυική σύναψη – αιμωδίες, σπασμούς) Gentamicin Tobramycin Amikacin Streptomycin Neomycin Kanamycin Paromomycin Netilmicin Spectinomycin αμινογλυκοσίδες
 αλλά και gr+ (ανεπαρκής δράση). Συγκαταλέγονται: pseudomonas aeruginosa, hemophilus influenza). Σημαντική συνέργεια με τα β-λακταμικά αντιβιοτικά (θα πρέπει να μεσολαβεί μεσοδιάστημα 3 ωρών επειδή οι πενικιλλίνες αδρανοποιούν τις αμινογλυκοσίδες) Η ανάπτυξη ανθεκτικότητας των μικροβίων δεν είναι ιδιαίτερο πρόβλημα. Χρησιμοποιούνται κυρίως σε σοβαρές λοιμώξεις (σήψη, επιπλεγμένες ουρολοιμώξεις, οστεομυελίτιδες) STOP όταν ταυτοποιηθεί ο μικροοργανισμός. Η δράση των αμινογλυκοσιδών είναι περιορισμένη σε περιβάλλον με χαμηλό (όξινο) pH (π.χ. πνεύμονες, βρογχικές εκκρίσεις NOT per os. Monitor levels (Trough and Peak levels) Nephro toxicity. Oto toxicity (ίλιγγος, αταξία) Neuro toxicity (νευρομυική σύναψη – αιμωδίες, σπασμούς) Gentamicin. Tobramycin. Amikacin. Streptomycin. Neomycin. Kanamycin. Paromomycin. Netilmicin. Spectinomycin. αμινογλυκοσίδες.")
43
Γιατί όχι μονοθεραπεία με μακρολίδες?
Η αντοχή του S. pneumoniae στις μακρολίδες προσεγγίζει το 40%. Γιατί όχι αμινογλυκοσίδες? Η δράση των αμινογλυκοσιδών είναι περιορισμένη σε περιβάλλον με χαμηλό (όξινο) pH (π.χ. πνεύμονες, βρογχικές εκκρίσεις) Γιατί όχι τετρακυκλίνες?
 pH (π.χ. πνεύμονες, βρογχικές εκκρίσεις) Γιατί όχι τετρακυκλίνες")
44
Τετρακυκλίνη Δοξυκυκλίνη Μινοκυκλίνη
Δράση έναντι gr- , gr+ και σε άτυπα. Αυξημένα ποσοστά αντοχής των βακτηρίων Μόνιμη εναπόθεση στα δόντια κίτρινη χροιά αντένδειξη <12 έτη και σε έγκυες

45
Πρόσφατη λοίμωξη υπό Amoxicillin/clavulanate πριν 2 μήνες
CASE 2 (modified) Patient with pneumonia, received augmentin Πρόσφατη λοίμωξη υπό Amoxicillin/clavulanate πριν 2 μήνες
 Patient with pneumonia, received augmentin. Πρόσφατη λοίμωξη υπό Amoxicillin/clavulanate πριν 2 μήνες.")
47
Ciprofloxacin Norfloxacin Ofloxacin Prulifloxacin -----------------
Levofloxacin Moxifloxacin Αναστέλλουν δύο ένζυμα που εμπλέκονται στη σύνθεση του DNA: DNA γυράση και τοποϊσομεράση IV Βακτηριοκτόνος δράση Δραστικότητα έναντι Pseudomonas (cipro-, levo-, moxi-) Καλή διεισδυτικότητα σε νεφρούς, προστάτη, πνεύμονες Ευρεία δράση κυρίως έναντι gr- μικροβίων (οι γ’ γενιάς έχουν επίσης πολύ καλή δράση και έναντι των gr+, της ψευδομονάδος και πολυανθεκτικών gr-). Τενοντίτιδα (Αχίλλειος τένοντας) Αυξανόμενη ανάπτυξη ανθεκτικότητας που σχετίζεται με τη δόση/διάρκεια θεραπείας.
 Καλή διεισδυτικότητα σε νεφρούς, προστάτη, πνεύμονες. Ευρεία δράση κυρίως έναντι gr- μικροβίων (οι γ’ γενιάς έχουν επίσης πολύ καλή δράση και έναντι των gr+, της ψευδομονάδος και πολυανθεκτικών gr-). Τενοντίτιδα (Αχίλλειος τένοντας) Αυξανόμενη ανάπτυξη ανθεκτικότητας που σχετίζεται με τη δόση/διάρκεια θεραπείας.")
48
CASE 3

49
Νοσοκομειακή πνευμονία [hospital-acquired (or nosocomial) pneumonia (HAP)]: Ξεκινά τουλάχιστον 48 ώρες μετά την εισαγωγή στο νοσοκομείο Πνευμονία σχετιζόμενη με αναπνευστήρα [Ventilator-associated pneumonia (VAP)]: Ξεκινά τουλάχιστον ώρες μετά από διασωλήνωση Healthcare-associated pneumonia (HCAP): Συμβαίνει σε μη νοσηλευόμενο ασθενή ο οποίος έχει σημαντική επαφή με μονάδες υγείας, δηλαδή: - έλαβε ενδοφλέβια αγωγή, περιποίηση τραύματος, χημειοθεραπεία τις προηγούμενες 30 ημέρες - διαμένει σε ίδρυμα (οίκο ευγηρίας, μονάδα αποκατάστασης) - πρόσφατη νοσηλεία σε νοσοκομείο για τουλάχιστον 2 ημέρες τις προηγούμενες 90 ημέρες - Προσέλευση στο νοσοκομείο ή σε μονάδα αιμοκάθαρσης τις προηγούμενες 30 ημέρες
![Νοσοκομειακή πνευμονία [hospital-acquired (or nosocomial) pneumonia (HAP)]: Ξεκινά τουλάχιστον 48 ώρες μετά την εισαγωγή στο νοσοκομείο](http://slideplayer.gr/slide/1897121/7/images/49/%CE%9D%CE%BF%CF%83%CE%BF%CE%BA%CE%BF%CE%BC%CE%B5%CE%B9%CE%B1%CE%BA%CE%AE+%CF%80%CE%BD%CE%B5%CF%85%CE%BC%CE%BF%CE%BD%CE%AF%CE%B1+%5Bhospital-acquired+%28or+nosocomial%29+pneumonia+%28HAP%29%5D%3A+%CE%9E%CE%B5%CE%BA%CE%B9%CE%BD%CE%AC+%CF%84%CE%BF%CF%85%CE%BB%CE%AC%CF%87%CE%B9%CF%83%CF%84%CE%BF%CE%BD+48+%CF%8E%CF%81%CE%B5%CF%82+%CE%BC%CE%B5%CF%84%CE%AC+%CF%84%CE%B7%CE%BD+%CE%B5%CE%B9%CF%83%CE%B1%CE%B3%CF%89%CE%B3%CE%AE+%CF%83%CF%84%CE%BF+%CE%BD%CE%BF%CF%83%CE%BF%CE%BA%CE%BF%CE%BC%CE%B5%CE%AF%CE%BF.jpg "Πνευμονία σχετιζόμενη με αναπνευστήρα [Ventilator-associated pneumonia (VAP)]: Ξεκινά τουλάχιστον ώρες μετά από διασωλήνωση. Healthcare-associated pneumonia (HCAP): Συμβαίνει σε μη νοσηλευόμενο ασθενή ο οποίος έχει σημαντική επαφή με μονάδες υγείας, δηλαδή: - έλαβε ενδοφλέβια αγωγή, περιποίηση τραύματος, χημειοθεραπεία τις προηγούμενες 30 ημέρες. - διαμένει σε ίδρυμα (οίκο ευγηρίας, μονάδα αποκατάστασης) - πρόσφατη νοσηλεία σε νοσοκομείο για τουλάχιστον 2 ημέρες τις προηγούμενες 90 ημέρες. - Προσέλευση στο νοσοκομείο ή σε μονάδα αιμοκάθαρσης τις προηγούμενες 30 ημέρες.")
50
Staphylococcus aureus (MRSA) Klebsiella pneumoniae
Πολυανθεκτικότητα - Μultidrug resistance (MDR) Πανανθεκτικότητα - Panresistance Enterococcus faecium Staphylococcus aureus (MRSA) Klebsiella pneumoniae Acinetobacter baumannii Pseudomonas aeruginosa Enterobacteriaceae (Salmonella, Escherichia coli, Yersinia, Shigella)
 Πανανθεκτικότητα - Panresistance. Enterococcus faecium. Staphylococcus aureus (MRSA) Klebsiella pneumoniae. Acinetobacter baumannii. Pseudomonas aeruginosa. Enterobacteriaceae (Salmonella, Escherichia coli, Yersinia, Shigella)")
51
Tygecycline, Colistin, Aztreonam
Carbapenemes: Meropenem, Imipenem, ertapenem Carbapenemase (KPC) Cephalosporins III: Ceftriaxone, Ceftazidime, Cefotaxime Extended Spectrum Beta Lactamases (ESBL) Aminopenicillins, cephalosporins Β-lactamase
 Cephalosporins III: Ceftriaxone, Ceftazidime, Cefotaxime. Extended Spectrum Beta Lactamases (ESBL) Aminopenicillins, cephalosporins. Β-lactamase.")
52
Καρβαπενέμες Meropenem Ertapenem Imipenem /cilastatin
β-λακταμικά αντιβιοτικά Πολύ ευρύ φάσμα (gr+, gr-, αναερόβια, αλλά όχι άτυπα και όχι MRSA) Η Cilastatin αναστέλλει τη νεφρική δεϋδροπεπτιδάση 1 (η οποία αδρανοποιεί την ιμιπενέμη) Υδρολύονται από τις καρβαπενεμάσες. Οι καρβαπενεμάσες δεν αναστέλλονται από τους αναστολείς των β-λακταμικών (κλαβουλανικό, etc.) Πρέπει να φυλάσσονται ως εφεδρικά αντιβιοτικά. Μπορούν να συνδυαστούν με αμινογλυκοσίδες σε σοβαρές λοιμώξεις από ψευδομονάδα ή Enterococcus faecalis. Meropenem Ertapenem Imipenem /cilastatin
 Η Cilastatin αναστέλλει τη νεφρική δεϋδροπεπτιδάση 1 (η οποία αδρανοποιεί την ιμιπενέμη) Υδρολύονται από τις καρβαπενεμάσες. Οι καρβαπενεμάσες δεν αναστέλλονται από τους αναστολείς των β-λακταμικών (κλαβουλανικό, etc.) Πρέπει να φυλάσσονται ως εφεδρικά αντιβιοτικά. Μπορούν να συνδυαστούν με αμινογλυκοσίδες σε σοβαρές λοιμώξεις από ψευδομονάδα ή Enterococcus faecalis. Meropenem. Ertapenem. Imipenem /cilastatin.")
53
Τυγεκυκλίνη (Tygacil)
Βακτηριοστατικό, αναστέλει την πρωτεϊνοσύνθεση των μικροβίων Ανήκει στις γλυκυλκυκλίνες (μοιάζει με τις τετρακυκλίνες) Ευρύ φάσμα (gr+, gr-, αναερόβια, αλλά όχι pseudomonas). Κυρίως έναντι Acinetobacter Baumannii. Δοσολογία: Δόση εφόδου: 100 mg IV 50 mg IV κάθε 12 ώρες. Μεταβολίζεται στο ήπαρ και απεκκρίνεται μέσω των χοληφόρων. Η δόση πρέπει να μειώνεται στο μισό σε ασθενείς με σοβαρή ηπατική ανεπάρκεια (Child-Pugh C). Αντίθετα, δεν χρειάζεται τροποποίηση της δόσης σε ασθενείς με νεφρική ανεπάρκεια. Είναι γενικά καλά ανεκτή και δεν χρειάζεται παρακολούθηση των επιπέδων
 Ευρύ φάσμα (gr+, gr-, αναερόβια, αλλά όχι pseudomonas). Κυρίως έναντι Acinetobacter Baumannii. Δοσολογία: Δόση εφόδου: 100 mg IV. 50 mg IV κάθε 12 ώρες. Μεταβολίζεται στο ήπαρ και απεκκρίνεται μέσω των χοληφόρων. Η δόση πρέπει να μειώνεται στο μισό σε ασθενείς με σοβαρή ηπατική ανεπάρκεια (Child-Pugh C). Αντίθετα, δεν χρειάζεται τροποποίηση της δόσης σε ασθενείς με νεφρική ανεπάρκεια. Είναι γενικά καλά ανεκτή και δεν χρειάζεται παρακολούθηση των επιπέδων.")
54
Colistin (Polymyxin E)
Απομονώθηκε αρχικά το 1949 και χρησιμοποιήθηκε για gr- λοιμώξεις «Νικήθηκε» από τις αμινογλυκοσίδες Βακτηριοκτόνος δράση Συνδέεται με λιποπολυσακχαρίτες και φωσφολιπίδια στην εξωτερική μεμβράνη των gr- βακτηρίων. Στενό αντιβακτηριακό φάσμα (κυρίως για Pseudomonas, Klebsiella και Acinetobacter) Νεφροτοξικότητα (διάμεση νεφρίτιδα), νευροτοξικότητα Δοσολογία Δόση εφόδου: 9,000,000 iu Στη συνέχεια: iu Χ 2
 Νεφροτοξικότητα (διάμεση νεφρίτιδα), νευροτοξικότητα. Δοσολογία. Δόση εφόδου: 9,000,000 iu. Στη συνέχεια: iu Χ 2.")
55
Αντιψευδομοναδικά Aminoglycosides (gentamicin, amikacin, tobramycin)
Quinolones (ciprofloxacin, levofloxacin, moxifloxacin) Cephalosporins (ceftazidime, cefepime, αλλά όχι cefuroxime, ceftriaxone, cefotaxime) Antipseudomonal penicillins: carboxypenicillins (piperacillin, ticarcillin) Carbapenems (meropenem, imipenem, αλλά όχι ertapenem) Polymyxins (colistin) Monobactams (aztreonam)
 Cephalosporins (ceftazidime, cefepime, αλλά όχι cefuroxime, ceftriaxone, cefotaxime) Antipseudomonal penicillins: carboxypenicillins (piperacillin, ticarcillin) Carbapenems (meropenem, imipenem, αλλά όχι ertapenem) Polymyxins (colistin) Monobactams (aztreonam)")
56
Πάντα παίρνουμε καλλιέργειες πριν την αντιβίωση
Τα αντιβιοτικά που επιλέγονται πρέπει να είναι δραστικά σε όλα τα πιθανά παθογόνα Να τροποποιούνται ανάλογα με τα αποτελέσματα των καλλιεργειών (de-escalation/αποκλιμάκωση) Να έχουν επαρκή διείσδυση στην εστία λοίμωξης Να χορηγούνται αρχικά στη μέγιστη επιτρεπτή δοσολογία Να τροποποιούνται σε ασθενείς με νεφρική ανεπάρκεια Να μην είναι της ίδιας ομάδας με αντιμικροβιακά που χορηγήθηκαν το τελευταίο τρίμηνο
 Να έχουν επαρκή διείσδυση στην εστία λοίμωξης. Να χορηγούνται αρχικά στη μέγιστη επιτρεπτή δοσολογία. Να τροποποιούνται σε ασθενείς με νεφρική ανεπάρκεια. Να μην είναι της ίδιας ομάδας με αντιμικροβιακά που χορηγήθηκαν το τελευταίο τρίμηνο.")
57
Viral life cycles vary in their precise details depending on the species of virus, but they all share a general pattern: Attachment to a host cell. Release of viral genes and possibly enzymes into the host cell. Replication of viral components using host-cell machinery. Assembly of viral components into complete viral particles. Release of viral particles to infect new host cells. Amantadine is no longer recommended for treatment of influenza B infection. For the 2008/2009 flu season, the United States' Centers for Disease Control and Prevention (CDC) found that 100% of seasonal H3N2 and 2009 pandemic flu samples tested have shown resistance to adamantanes.[6] The CDC issued an alert to doctors to prescribe the neuraminidase inhibitors oseltamivir andzanamivir instead of amantadine and rimantadine for treatment of current circulating flu.[7][8]
 found that 100% of seasonal H3N2 and 2009 pandemic flu samples tested have shown resistance to adamantanes.[6] The CDC issued an alert to doctors to prescribe the neuraminidase inhibitors oseltamivir andzanamivir instead of amantadine and rimantadine for treatment of current circulating flu.[7][8]")
58
Αμανταδίνη Αναστολέας της πρωτεϊνης Μ2 του ιού της γρίπης Α.
Ο ιός της γρίπης Β δεν έχει Μ2.

59
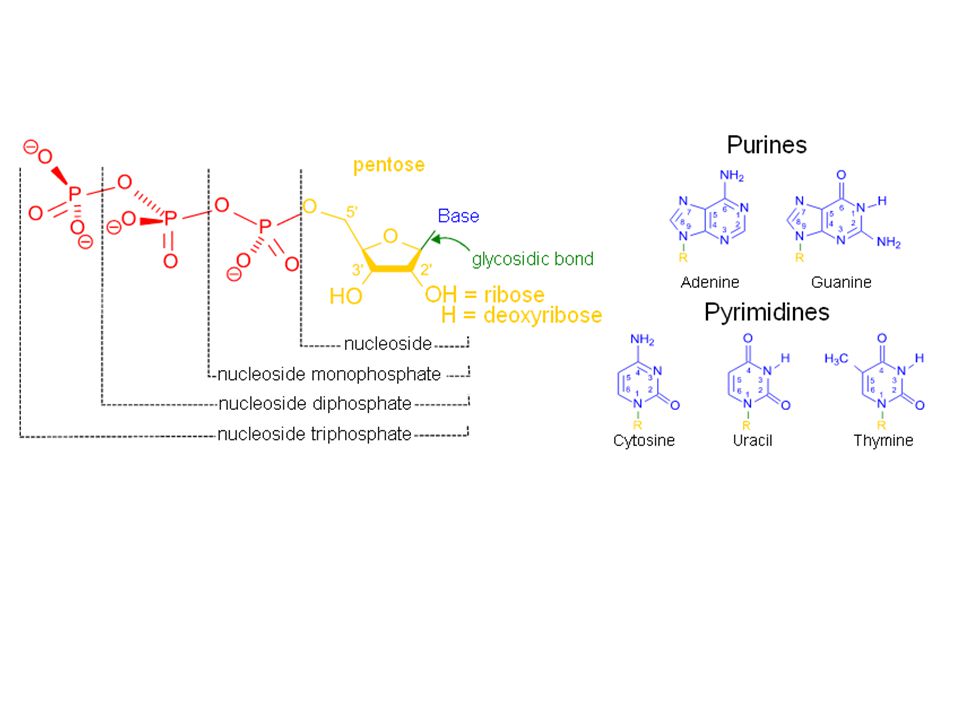
NUCLEOSIDE/NUCLEOTIDE ANALOGUES

61
Nucleoside analog reverse-transcriptase inhibitors
Zidovudine Didanosine Zalcitabine Stavudine Lamivudine (Zeffix) (HBV) Abacavir Emtricitabine Entecavir (Baraclude) Apricitabine Acyclovir / Valacyclovir / famcyclovir * (δραστικότητα έναντι HSV1, HSV2, VZV) Nucleotide analog reverse-transcriptase inhibitors Tenofovir (Viread) Adefovir (Hepsera) Non-nucleoside reverse-transcriptase inhibitors Efavirenz Nevirapine Delavirdine Etravirine Rilpivirine
 (HBV) Abacavir Emtricitabine Entecavir (Baraclude) Apricitabine Acyclovir / Valacyclovir / famcyclovir * (δραστικότητα έναντι HSV1, HSV2, VZV) Nucleotide analog reverse-transcriptase inhibitors. Tenofovir (Viread) Adefovir (Hepsera) Non-nucleoside reverse-transcriptase inhibitors. Efavirenz Nevirapine Delavirdine Etravirine Rilpivirine.")
62
Integrase inhibitor: Raltegravir
Raltegravir (MK-0518, brand name Isentress) is an antiretroviral drug produced by Merck & Co., used to treat HIV infection.[1] It received approval by theU.S. Food and Drug Administration (FDA) in October 2007, the first of a new class of HIV drugs, the integrase inhibitors, to receive such approval
 is an antiretroviral drug produced by Merck & Co., used to treat HIV infection.[1] It received approval by theU.S. Food and Drug Administration (FDA) in October 2007, the first of a new class of HIV drugs, the integrase inhibitors, to receive such approval.")
63
Protease inhibitors

64
HIV/AIDS: Saquinavir, rotnavir, indinavir, nelfinavir, etc.)
Protease inhibitors HIV/AIDS: Saquinavir, rotnavir, indinavir, nelfinavir, etc.) Hepatitis C: Boceprevir Hepatitis C: Telaprevir Protease inhibitors (PIs) are a class of drugs used to treat or prevent infection by viruses, including HIV and Hepatitis C. PIs prevent viral replication by inhibiting the activity of proteases, e.g.HIV-1 protease, enzymes used by the viruses to cleave nascent proteins for final assembly of new virions. Protease inhibitors have been developed or are presently undergoing testing for treating various viruses: HIV/AIDS: antiretroviral protease inhibitors (saquinavir, ritonavir, indinavir, nelfinavir, amprenavir[1] etc.) Hepatitis C: Boceprevir Hepatitis C: Telaprevir Given the specificity of the target of these drugs there is the risk, as in antibiotics, of the development of drug-resistant mutated viruses. To reduce this risk it is common to use several different drugs together that are each aimed at different targets Protease inhibitors can cause a syndrome of lipodystrophy, hyperlipidaemia, diabetes mellitus type 2, and kidney stones Some viruses include an enzyme known as a protease that cuts viral protein chains apart so they can be assembled into their final configuration. HIV includes a protease, and so considerable research has been performed to find "protease inhibitors" to attack HIV at that phase of its life cycle.[17] Protease inhibitors became available in the 1990s and have proven effective, though they can have unusual side effects, for example causing fat to build up in unusual places.[18] Improved protease inhibitors are now in development.
 Hepatitis C: Boceprevir. Hepatitis C: Telaprevir. Protease inhibitors (PIs) are a class of drugs used to treat or prevent infection by viruses, including HIV and Hepatitis C. PIs prevent viral replication by inhibiting the activity of proteases, e.g.HIV-1 protease, enzymes used by the viruses to cleave nascent proteins for final assembly of new virions. Protease inhibitors have been developed or are presently undergoing testing for treating various viruses: HIV/AIDS: antiretroviral protease inhibitors (saquinavir, ritonavir, indinavir, nelfinavir, amprenavir[1] etc.) Hepatitis C: Boceprevir. Hepatitis C: Telaprevir. Given the specificity of the target of these drugs there is the risk, as in antibiotics, of the development of drug-resistant mutated viruses. To reduce this risk it is common to use several different drugs together that are each aimed at different targets. Protease inhibitors can cause a syndrome of lipodystrophy, hyperlipidaemia, diabetes mellitus type 2, and kidney stones. Some viruses include an enzyme known as a protease that cuts viral protein chains apart so they can be assembled into their final configuration. HIV includes a protease, and so considerable research has been performed to find protease inhibitors to attack HIV at that phase of its life cycle.[17] Protease inhibitors became available in the 1990s and have proven effective, though they can have unusual side effects, for example causing fat to build up in unusual places.[18] Improved protease inhibitors are now in development.")
66
Neuraminidase inhibitors Oseltamivir (Tamiflu) – per os
Oseltamivir (Tamiflu) – per os Zanamivir (Relenza) – εισπνεόμενη ή ενδορρινική χορήγηση Laninamivir (Inavir) Peramivir Η Νευραμινιδάση υπάρχει και στον ιό της γρίπης Α και στον Β, και παραμένει αναλλοίωτη παρά τις μεταλλαγές του ιού. μειώνουν τη διάρκεια των συμπτωμάτων κατά περίπου 1 ημέρα Δοσολογία: 75 mg Χ2 ημερησίως Η χημειοπροφύλαξη μειώνει, αλλά δεν εξαλείφει τον κίνδυνο της γρίπης Η πιθανότητα γρίπης επανέρχεται σε συνήθη επίπεδα όταν σταματήσει η λήψη τους Θα πρέπει να χορηγείται παράλληλα και αντιγριπικός εμβολιασμός Oseltamivir is approved for use in persons age one and over. The usual adult dosage for treatment of influenza is 75 mg twice daily for five days, beginning within two days of the appearance of symptoms, with decreased doses for children and patients with renal impairment. It may be given as a preventive measure either during a community outbreak or following close contact with an infected individual. The importance of early treatment is that the NA protein inhibition is more effective within the first 48 hours. If the virus has replicated and infected many cells, the effectiveness of this medication will be severely diminished, especially over time. On December 8, 2009, the Cochrane Collaboration, which reviews medical evidence, in a review published in the British Medical Journal, announced it had reversed its previous findings that the antiviral drug Tamiflu can ward off pneumonia and other serious conditions linked to influenza. They reported an analysis of 20 studies showed Tamiflu offered mild benefits in terms of duration of symptoms for healthy adults if taken within 24 hours of onset of symptoms, but found no clear evidence it prevented lower respiratory tract infections or other complications of influenza
 – per os. Zanamivir (Relenza) – εισπνεόμενη ή ενδορρινική χορήγηση. Laninamivir (Inavir) Peramivir. Η Νευραμινιδάση υπάρχει και στον ιό της γρίπης Α και στον Β, και παραμένει αναλλοίωτη παρά τις μεταλλαγές του ιού. μειώνουν τη διάρκεια των συμπτωμάτων κατά περίπου 1 ημέρα. Δοσολογία: 75 mg Χ2 ημερησίως. Η χημειοπροφύλαξη μειώνει, αλλά δεν εξαλείφει τον κίνδυνο της γρίπης. Η πιθανότητα γρίπης επανέρχεται σε συνήθη επίπεδα όταν σταματήσει η λήψη τους. Θα πρέπει να χορηγείται παράλληλα και αντιγριπικός εμβολιασμός. Oseltamivir is approved for use in persons age one and over. The usual adult dosage for treatment of influenza is 75 mg twice daily for five days, beginning within two days of the appearance of symptoms, with decreased doses for children and patients with renal impairment. It may be given as a preventive measure either during a community outbreak or following close contact with an infected individual. The importance of early treatment is that the NA protein inhibition is more effective within the first 48 hours. If the virus has replicated and infected many cells, the effectiveness of this medication will be severely diminished, especially over time. On December 8, 2009, the Cochrane Collaboration, which reviews medical evidence, in a review published in the British Medical Journal, announced it had reversed its previous findings that the antiviral drug Tamiflu can ward off pneumonia and other serious conditions linked to influenza. They reported an analysis of 20 studies showed Tamiflu offered mild benefits in terms of duration of symptoms for healthy adults if taken within 24 hours of onset of symptoms, but found no clear evidence it prevented lower respiratory tract infections or other complications of influenza.")
67
+polyethyleneglycol (PEG) peginterferon
Interferon α HBV, HCV +polyethyleneglycol (PEG) peginterferon The attachment of polyethylene glycol to a protein (pegylation) reduces its rate of absorption following subcutaneous injection, reduces renal and cellular clearance, and decreases the immunogenicity of the protein. All of these effects tend to enhance the half-life of the pegylated versus the native protein. Both hepatitis B and hepatitis C are treated with IFN-α
 peginterferon. The attachment of polyethylene glycol to a protein (pegylation) reduces its rate of absorption following subcutaneous injection, reduces renal and cellular clearance, and decreases the immunogenicity of the protein. All of these effects tend to enhance the half-life of the pegylated versus the native protein. Both hepatitis B and hepatitis C are treated with IFN-α.")
68
Amphotericin B (AMB) and nystatin are the currently available polyenes, although differing safety profiles have limited nystatin to topical use.1 The polyenes bind to ergosterol present within the fungal cell wall membrane. This process disrupts cell wall permeability by forming oligodendromes functioning as pores with the subsequent efflux of potassium and intracellular molecules causing fungal death. Animal cells contain cholesterol instead of ergosterol and so they are much less susceptible. Amphotericin B is nephrotoxic when given intravenously. Azoles: The inhibition of cytochrome P450 (CYP)-dependent 14-a-demethylase prevents the conversion of lanosterol to ergosterol. This mechanism results in the accumulation of toxic methylsterols and resultant inhibition of fungal cell growth and replication Echinocandins (caspofungin, micafungin, anidulafungin) are synthetic compounds that inhibit the synthesis of b-1,3 glucan, by inhibiting the activity of glucan synthase. This mechanism impairs cell wall integrity and leads to osmotic lysis. Echinocandins may be used for systemic fungal infections in immunocompromised patients, they inhibit the synthesis of glucan in the cell wall via the enzyme 1,3-β glucan synthase: Flucytosine (5FC; Ancobon) is deaminated to 5-fluorouracil by fungal cytosine deaminase. 5- fluorouracil is further converted to 5-fluorodeoxyuridylic acid, which interferes with DNA synthesis. Mammalian cells lack cytosine deaminase allowing for a selective inhibition of fungal organisms Allylamines: Allylamines inhibit squalene epoxidase, another enzyme required for ergosterol synthesis:
-dependent 14-a-demethylase prevents the conversion of lanosterol to ergosterol. This mechanism results in the accumulation of toxic methylsterols and resultant inhibition of fungal cell growth and replication. Echinocandins (caspofungin, micafungin, anidulafungin) are synthetic compounds that inhibit the. synthesis of b-1,3 glucan, by inhibiting the activity of glucan synthase. This mechanism impairs cell. wall integrity and leads to osmotic lysis. Echinocandins may be used for systemic fungal infections in immunocompromised patients, they inhibit the synthesis of glucan in the cell wall via the enzyme 1,3-β glucan synthase: Flucytosine (5FC; Ancobon) is deaminated to. 5-fluorouracil by fungal cytosine deaminase. 5- fluorouracil is further converted to 5-fluorodeoxyuridylic. acid, which interferes with DNA synthesis. Mammalian cells lack cytosine deaminase allowing. for a selective inhibition of fungal organisms. Allylamines: Allylamines inhibit squalene epoxidase, another enzyme required for ergosterol synthesis:")
69
Polyenes Azoles Echinocandines Amphotericin B Nystatin Imidazoles
Bifonazole Butoconazole Clotrimazole Econazole Fenticonazole Isoconazole Ketoconazole Miconazole Omoconazole Oxiconazole Sertaconazole Sulconazole Tioconazole Triazoles Albaconazole Fluconazole Isavuconazole Itraconazole Posaconazole Ravuconazole Terconazole Voriconazole Thiazoles Abafungin Echinocandines Anidulafungin Caspofungin Micafungin

70
- Πτωχή per os απορρόφηση (<5%), επομένως απαιτεί IV χορήγηση
Polyenes Amphotericin B Nystatin Η Amphotericin B παραμένει η κλασσική θεραπεία για πολλές βαριές μυκητιάσεις. Ωστόσο, λόγω της τοξικότητας που συνδέεται με την IV χρήση της και το πιο ασφαλές προφίλ άλλων αντιμυκητιασικών, φυλάσσεται για περιπτώσεις απειλητικών για τη ζωή μυκητιάσεων ή όταν οι εναλλακτικές επιλογές δεν είναι ανεκτές. - Πτωχή per os απορρόφηση (<5%), επομένως απαιτεί IV χορήγηση Ο συνδυασμός με λίπίδια (λιποσωμική) μειώνει την τοξικότητα
, επομένως απαιτεί IV χορήγηση. Ο συνδυασμός με λίπίδια (λιποσωμική) μειώνει την τοξικότητα.")
71
Azoles Imidazoles Bifonazole Butoconazole Clotrimazole Econazole Fenticonazole Isoconazole Ketoconazole Miconazole Omoconazole Oxiconazole Sertaconazole Sulconazole Tioconazole Triazoles Albaconazole Fluconazole (Fungustatin) Isavuconazole Itraconazole Posaconazole Ravuconazole Terconazole Voriconazole (V-fend) Thiazoles Abafungin Γενικά η βιοδιαθεσιμότητά τους δεν είναι ιδιαίτερα πρoβλέψιμη και απαιτείται παρακολούθηση των θεραπευτικών επιπέδων Γενικά η βιοδιαθεσιμότητά τους δεν είναι ιδιαίτερα πρoβλέψιμη και απαιτείται παρακολούθηση των θεραπευτικών επιπέδων Agents within the azole class vary importantly with regards to spectrum of activity, pharmacokinetic profiles, and toxicities [2]. For example, fluconazole has excellent activity against yeasts, but offers no protection against mold infections. An extended spectrum is provided by itraconazole, but inconsistent bioavailability limits use of this agent in severely ill patients. Voriconazole is the first-line agent for the treatment of invasive aspergillosis, but its bioavailability is unpredictable and genetically determined, it is associated with unique side effects (visual hallucinations, rash, transient vision changes, periostitis), and lacks activity against the Mucorales, the agents of mucormycosis. Posaconazole has the broadest spectrum of activity and fewest drug interactions, but absorption is problematic and it is available only as an oral formulation. Thus, it is important for clinicians to appreciate the unique characteristics of each member of this class in order to use azoles appropriately. it has become commonplace to perform therapeutic drug monitoring for voriconazole and posaconazole to assure efficacy in the treatment of serious fungal infections [30,71-74] and, in the case of voriconazole, to avoid toxicity
 Isavuconazole. Itraconazole. Posaconazole. Ravuconazole. Terconazole. Voriconazole (V-fend) Thiazoles. Abafungin. Γενικά η βιοδιαθεσιμότητά τους δεν είναι ιδιαίτερα πρoβλέψιμη και απαιτείται παρακολούθηση των θεραπευτικών επιπέδων. Γενικά η βιοδιαθεσιμότητά τους δεν είναι ιδιαίτερα πρoβλέψιμη και απαιτείται παρακολούθηση των θεραπευτικών επιπέδων. Agents within the azole class vary importantly with regards to spectrum of activity, pharmacokinetic profiles, and toxicities [2]. For example, fluconazole has excellent activity against yeasts, but offers no protection against mold infections. An extended spectrum is provided by itraconazole, but inconsistent bioavailability limits use of this agent in severely ill patients. Voriconazole is the first-line agent for the treatment of invasive aspergillosis, but its bioavailability is unpredictable and genetically determined, it is associated with unique side effects (visual hallucinations, rash, transient vision changes, periostitis), and lacks activity against the Mucorales, the agents of mucormycosis. Posaconazole has the broadest spectrum of activity and fewest drug interactions, but absorption is problematic and it is available only as an oral formulation. Thus, it is important for clinicians to appreciate the unique characteristics of each member of this class in order to use azoles appropriately. it has become commonplace to perform therapeutic drug monitoring for voriconazole and posaconazole to assure efficacy in the treatment of serious fungal infections [30,71-74] and, in the case of voriconazole, to avoid toxicity.")
72
Echinocandines Anidulafungin Caspofungin (Cancidas) Micafungin (Mycamin) Η πρώτη τάξη αντιμυκητιασικών που δρα στο κυτταρικό τοίχωμα των μυκήτων. Μπλοκάρουν την συνθετάση των β-glucans, οι οποίες δεν υπάρχουν στα ανθρώπινα κύτταρα, για αυτό και είναι πιο ασφαλής έναντι της αμφοτερικίνης και των αζολών. Περιορισμένη per os βιοδιαθεσιμότητα πρέπει να χορηγείται IV Καλά ανεκτά και ασφαλή Χρησιμοποιούνται ευρύτατα στη καντιντίαση, είδικά σε ουδετεροπενικούς ασθενείς Τα κυριότερα πλεονεκτήματα έναντι των άλλων αντιμυκητιασικών είναι η δράση έναντι της κάντιντας, και το προφίλ ασφάλειας (δεν προκαλεί νεφρο- ηπατοτοξικότητα, μη σημαντικές αλληλεπιδράσεις με άλλα φάρμακα) Πολύ σπάνια η ανθεκτικότητα
 Πολύ σπάνια η ανθεκτικότητα.")
Παρόμοιες παρουσιάσεις


















>")






