Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
‘‘Highlights EAU, Μαδρίτη 2015’’ Γεώργιος Ι. Παπαδόπουλος, MD, PhD, FEBU Επιμελητής Α’ Ουρολογικής Κλινικής ΓΝΑ ‘‘Γ. ΓΕΝΝΗΜΑΤΑΣ’’ ΝΙΜΤΣ, 16 Δεκεμβρίου 2015

2
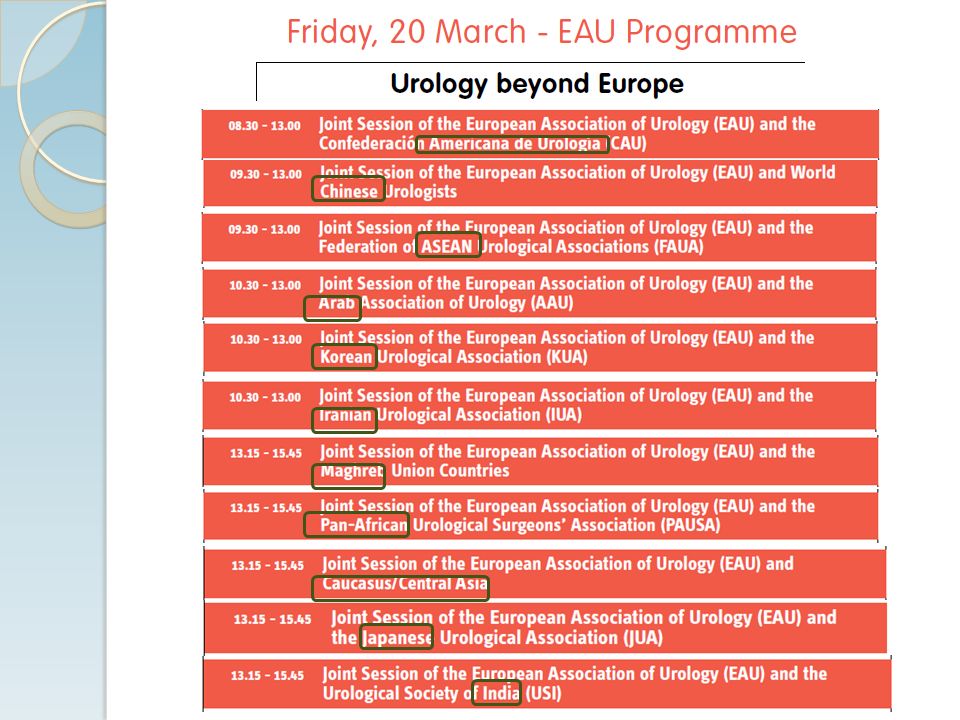
Εισαγωγή Σύνεδροι > 12.000 Webcasts: 1.815 Abstracts: 1.173 e-posters: 225 Posters: 875 Videos: 76 ESU courses: 45

3
presenting original unpublished data sharing ideas The EAU Congress provides a forum for presenting original unpublished data and sharing ideas for urological innovation as well as disseminating evidence-based knowledge of primary clinical relevance. Urologists and affiliated professionals attending the EAU Congress will be able to: innovative techniques and scientific advances - Review innovative techniques and scientific advances in the field of urology and its subspecialties; latest data - Review the latest data and emerging trends from studies in clinical and translational research; knowledge of evidence-based approaches - Enhance their knowledge of evidence-based approaches to the management of urological disease; new knowledge - Gain new knowledge on emerging diagnostic and risk- assessment strategies in the management of urological disease; practical knowledge and skills - Enhance their practical knowledge and skills by educational activities, including hands-on training and courses; new developments - Gain exposure to new developments in drugs and new cutting- edge technology in the field of pharmaceutical research and medical technology through visiting the EAU Congress Exhibition; Communicatecollaboratenetwork - Communicate, collaborate and network with representatives of a large international audience – medical professionals, national urological societies, patient groups, medical industry and the media. Στόχοι

5
Καρκίνος προστάτη Results → 843 Βασική έρευνα → 184 (128 - 56) Screening → 184 (120 - 64) Σταδιοποίηση → 44 (28 - 16) Αντιμετώπιση → 431 (299 - 132) Active surveillance, focal, ablative → 58 Surgery, Radiotherapy, Brachytherapy → 216 Recurrence after local disease → 39 Systemic treatment → 42 Survivorship & supportive care → 76
 Screening → 184 ( ) Σταδιοποίηση → 44 ( ) Αντιμετώπιση → 431 ( ) Active surveillance, focal, ablative → 58 Surgery, Radiotherapy, Brachytherapy → 216 Recurrence after local disease → 39 Systemic treatment → 42 Survivorship & supportive care → 76")
6
Ουροθηλιακοί όγκοι Results → 423 Βασική έρευνα → 121 (84 - 37) Διάγνωση → 37 (24 - 13) Σταδιοποίηση → 26 (18 - 8) Αντιμετώπιση NMIBC → 51 (33 - 18) Αντιμετώπιση MIBC → 167 Xειρουργική → 111 (74 - 37) Μη χειρουργική → 27 (17 - 10) UCC Ανωτέρου Ουροποιητικού → 50 (35 - 15)
 Διάγνωση → 37 ( ) Σταδιοποίηση → 26 (18 - 8) Αντιμετώπιση NMIBC → 51 ( ) Αντιμετώπιση MIBC → 167 Xειρουργική → 111 ( ) Μη χειρουργική → 27 ( ) UCC Ανωτέρου Ουροποιητικού → 50 ( )")
7
Καρκίνος νεφρού Results → 393 Βασική έρευνα → 67 (46 - 21) Διάγνωση → 58 (40 - 18) Aντιμετώπιση → 268 (181 - 85) Non-organ sparing → 78 Nephron-sparing → 130 Non-surgical → 25 Systemic treatment → 35
 Διάγνωση → 58 ( ) Aντιμετώπιση → 268 ( ) Non-organ sparing → 78 Nephron-sparing → 130 Non-surgical → 25 Systemic treatment → 35")
8
Λιθίαση Results → 244 Βασική έρευνα/Φαρμακευτική θεραπεία → 46 (33 -13) ESWL → 37 (25 -12) PCNL/Open → 90 (62 - 28) URS → 71 (49 - 22)
 ESWL → 37 (25 -12) PCNL/Open → 90 ( ) URS → 71 ( )")
9
Male LUTS Results → 185 Βασική έρευνα → 50 (34 - 16) Διάγνωση/Aξιολόγηση → 52 (36 - 16) Φαρμακευτική αντιμετώπιση → 45 (33 - 12) Χειρουργική θεραπεία → 38 (25 - 13)
 Διάγνωση/Aξιολόγηση → 52 ( ) Φαρμακευτική αντιμετώπιση → 45 ( ) Χειρουργική θεραπεία → 38 ( )")
10
Screening → Κίνδυνος υπερδιάγνωσης/υπερθεραπείας Protect trial → p εμφάνισης Gleason 6 → Προσοχή στην ερμηνεία!

12
PCa - Λεμφαδενεκτομή increased morbidity tumour staging oncologic benefit Extended lymphadenectomy is associated with increased morbidity (longer hospital stay, longer operating room time, intraoperative bleeding, intraoperative complications including obturator nerve or vascular injury) and tumour staging in patients with prostate cancer at high risk. The oncologic benefit can be demonstrated with a longer follow-up time.

14
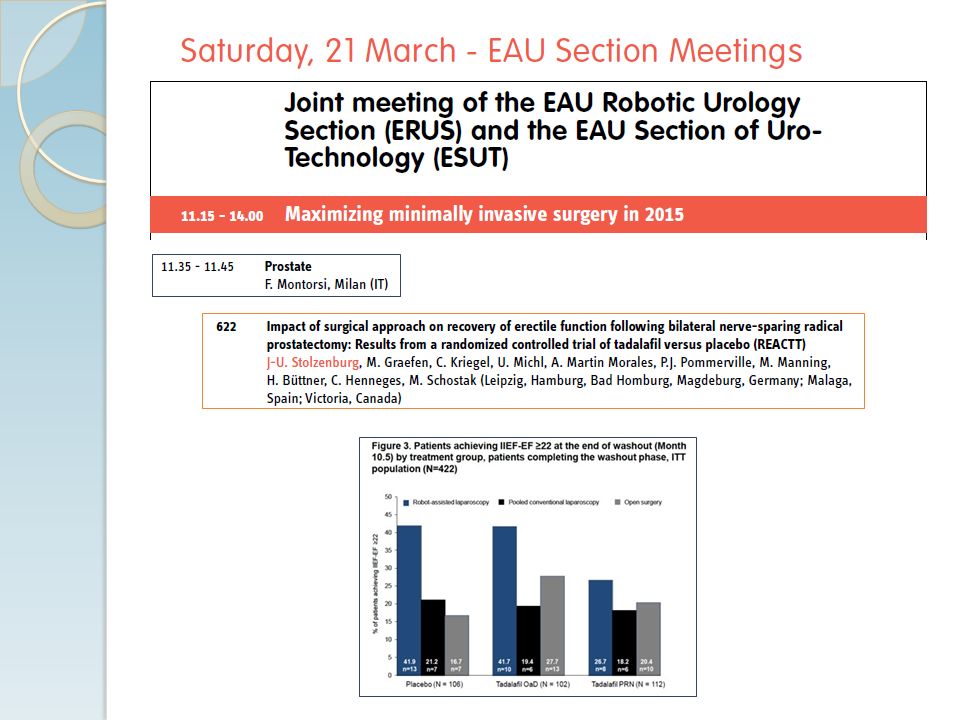
There are multiple mechanisms of resistance, and the resistance is at the cellular and genetic levels. Some resistance are induced by treatment and some are pre-existing (and rapid) The combination of standard androgen deprivation therapy (ADT) and six cycles of docetaxel significant improved overall survival compared to standard ADT alone in men with hormone sensitive prostate cancer (790 pts)
 The combination of standard androgen deprivation therapy (ADT) and six cycles of docetaxel significant improved overall survival compared to standard ADT alone in men with hormone sensitive prostate cancer (790 pts).")
15
Arv 7 → Μη ανταπόκριση σε Abiraterone, Enzalutamide → XMΘ Prior response to ADT (< 16m) → XMΘ Gl 8-10 → XMΘ ADT σε CRPC Καθημερινή πρακτική/Guidelines → Συνέχιση Abiraterone + ADT (SPARE trial → preliminary results → YES) Enzalutamide + ADT.... XMΘ + ΑDT (2 trials)
.")
16
PREVAIL - TERRAIN The studied population represented a traditional early CRPC patient group and the updated data confirmed a robust benefit of enzalutamide over placebo in overall survival. Biomarkers → Resistance Adverse effects Enzalutamide is transforming the treatment for this disease because of its benefits for progression-free survival and delayed PSA progression. Adverse effects Bicalutamide → ‘‘Aδύναμος αντίπαλος’’

17
Aξιόπιστοι δείκτες στα βιολογικά υγρά Ούρα → nearly all tumour parts, non-invasive BCG → Gold-standard BCG + MMC ( recurrence rate)
")
18
cannot yet be considered Robot-assisted radical cystectomy (RARC) is feasible… but RARC cannot yet be considered as a standard treatment for invasive bladder cancer, surgeon makes the difference Regarding RARC, our initial expectations are not yet met. Why not? Because the surgeon makes the difference, not the instrument Surgeon experience institutional volume Surgeon experience and institutional volume strongly predict favourable outcome after open RC or RARC advantages The clear advantages for RARC are less blood loss and transfusion rates, but which are counter- balanced by long operative time and high costs.

19
ρομποτικής μερικής νεφρεκτομής Εφικτή, ογκολογικά άρτια, αποδεκτή καμπύλη εκμάθησης Open → χ/κός χρόνος Robotic → Απώλεια αίματος, χρόνος νοσηλείας Κόστος; (Ιατρικό, κοινωνικό...)
")
20
Χ/ο υψηλών απαιτήσεων Νοσηρότητα/θνητότητα Θρομβεκτομή ‘’Neoadjuvant’’ (NOT ‘’presurgical’’) therapy with TKIs, mTOR → DFS, OS? Νεότερα αντι-Τ (λεμφοκύτταρα) φάρμακα CTLA-4, PD-1
 φάρμακα CTLA-4, PD-1.")
21
Λιθίαση preventive medical therapy Most patients with stones will consider preventive medical therapy to avoid recurrent pain or a surgical procedure. In contrast, most urologists perceive that patients prefer to avoid medication even if it means tolerating several acute stone events and/or surgical procedures.

22
Λιθίαση Mini, Ultra-mini, micro- procedures Nέα Τεχνολογία στην FURS (Robot-assisted, SWL-combined)
")
23
‘’Erosion’’ → ‘’Exposure’’, ‘’perforation’’

24
ED → Ολιστική προσέγγιση Stem cells (embryonic, adult) → Eνδοσηραγγώδης έγχυση Gene therapy LESW → Βελτίωση κυκλοφορίας Kιρσοκήλη - Υπογονιμότητα Μη αποφρακτική αζωοσπερμία → Διόρθωση κιρσοκήλης → TESE - ICSI
 → Eνδοσηραγγώδης έγχυση Gene therapy LESW → Βελτίωση κυκλοφορίας Kιρσοκήλη - Υπογονιμότητα Μη αποφρακτική αζωοσπερμία → Διόρθωση κιρσοκήλης → TESE - ICSI")
25
Best abstract (Oncology) Metastasized and non-metastasized Seminoma can be completely discriminated with a two small RNAs combination of two small RNAs, irrespective of the subtype (lymphogen or occult metastasized), if measured in primary tumour or in peripheral blood. About one third of all differentially expressed small RNAs are detected in tumour tissue and peripheral blood.

26
Best abstract (Non-Oncology) costsresistant The adherence to EAU Guidelines on antibiotic prophylaxis reduced related costs and the prevalence of resistant bacteria. Συνετή χρήση αντιβιοτικών Αποφυγή όπου δεν είναι απαραίτητα Guidelines Eναλλακτικές μέθοδοι

Παρόμοιες παρουσιάσεις















. ΣΥΓΚΟΠΤΙΚΗ ΚΡΙΣΗ Αιφνίδια και σύντομη απώλεια συνείδησης που προκαλείται από ανεπαρκή εγκεφαλική αιμάτωση λόγω μειωμένης.>")


 ωφελέειν ή μη βλάπτειν ωφελέειν = θεραπευτική παρέμβαση μη βλάπτειν = ασφάλεια ασθενών.>")

