Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

2
Αιματοκρίτης Αιμοσφαιρίνη MCV MCH (mean cellular hemoglobin) Αριθμός δικτυοερυθροκυττάρων Αμεση και έμμεση Coombs
 Αριθμός δικτυοερυθροκυττάρων Αμεση και έμμεση Coombs")
3
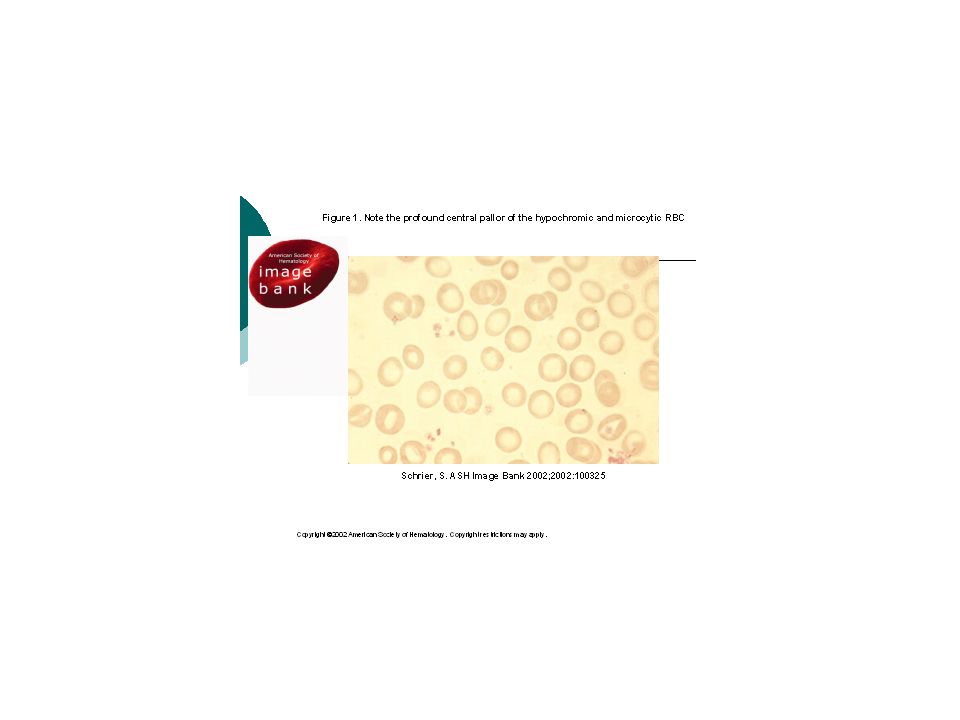
Aναιμία Υπόχρωμη μικροκυτταρική Ορθόχρωμη Μακροκυτταρική Φερριτίνη Χαμηλή Σιδηροπενι κή Φυσιολογική Ηλεκτροφόρηση Hb Θαλασσαι μία Χρονίας νόσου Σιδηροβλαστική ΔΕΚ ΕλατωμμέναΑυξημένα Απλαστική Αιμολυτική Coombs + Αυτοάνοση G6PD Αιμοσφαιρινοπάθειες Μεμβρανοπάθειες Μικροαγγειοπαθητικές Β12 φυλλικό Αλκοόλ Ηπατοπάθεια Απλαστική Χημειοθεραπ εία

4
Περίπτωση 1 Γυναίκα 37 χρονών παρουσιάζεται στα εξωτερικά ιατρεία λόγω αναιμίας Υγιής, φυσιολογική δίαιατα ελαμβανε αντιβίωση για φαρυγγίτιδα Αδυναμία και δεκαδική πυρετική κίνηση

5
- Hemoglobin – 7.9 gr% - MCV – 100 - RDW – 17 - WBC – φυσιολογικά - Platelets - φυσιολογικά

6
Μακροκυτταρική αναιμία - Μεγαλοβλαστική -Αιμολυτική -Μυελοδυσπλαστικό/Απλαστική ΔΕΚ

7
- Reticulocytes – 14% - Corrected reticulocyte count: /% Retics X (measured to the expected Hb ratio)/ 14% x 7.9/15 = 7.4%
/ 14% x 7.9/15 = 7.4%")
8
Μακροκυτταρική αναιμία - Μεγαλοβλαστική ΌΧΙ -Μυελοδυσπλαστικό/Απλαστική ΟΧΙ Αιμολυτική ΝΑΙ

9
Για την επιβεβαίωση χρειαζόμαστε - LDH – υψηλή - Εμμεση χολερυθρίνη υψηλή - Απτοσφαιρίνη χαμηλή Επιβεβαίωση διάγνωσης Αιμολυτική αναιμία

10
ΔΔ αιμολυτικής αναιμίας: - Εσωτερικό του ερυθροκυττάρου (αιμοσφαιρινοπάθεια, ενζυμοπάθεια) -Μεμβράνη του ερυθροκυττάρου - Εξωτερικό του ερυθροκυττάρου (υπερσπληνισμός, μηχανική αιμόλυση, άνοση αιμόλυση, τοξικοί/ φλεγμονώδεις παράγοντες)
 -Μεμβράνη του ερυθροκυττάρου - Εξωτερικό του ερυθροκυττάρου (υπερσπληνισμός, μηχανική αιμόλυση, άνοση αιμόλυση, τοξικοί/ φλεγμονώδεις παράγοντες)")
11
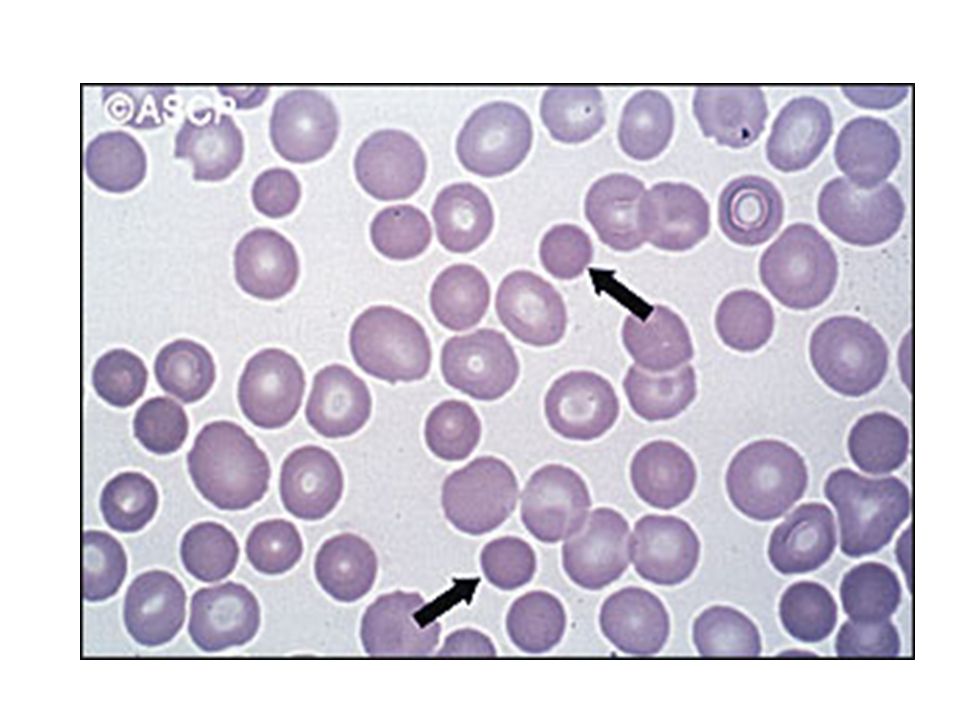
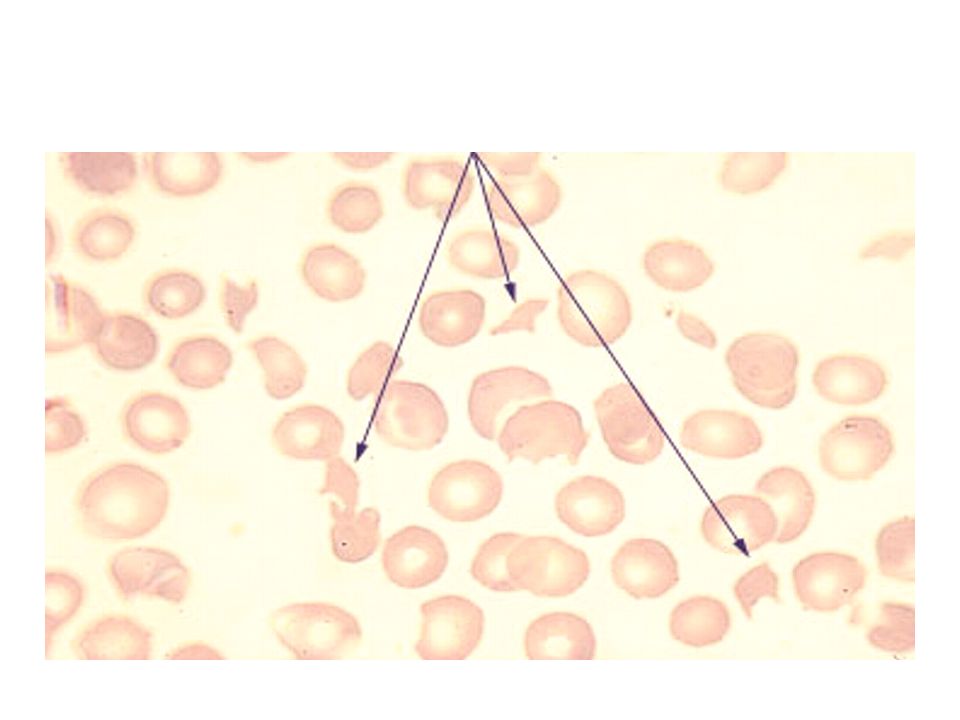
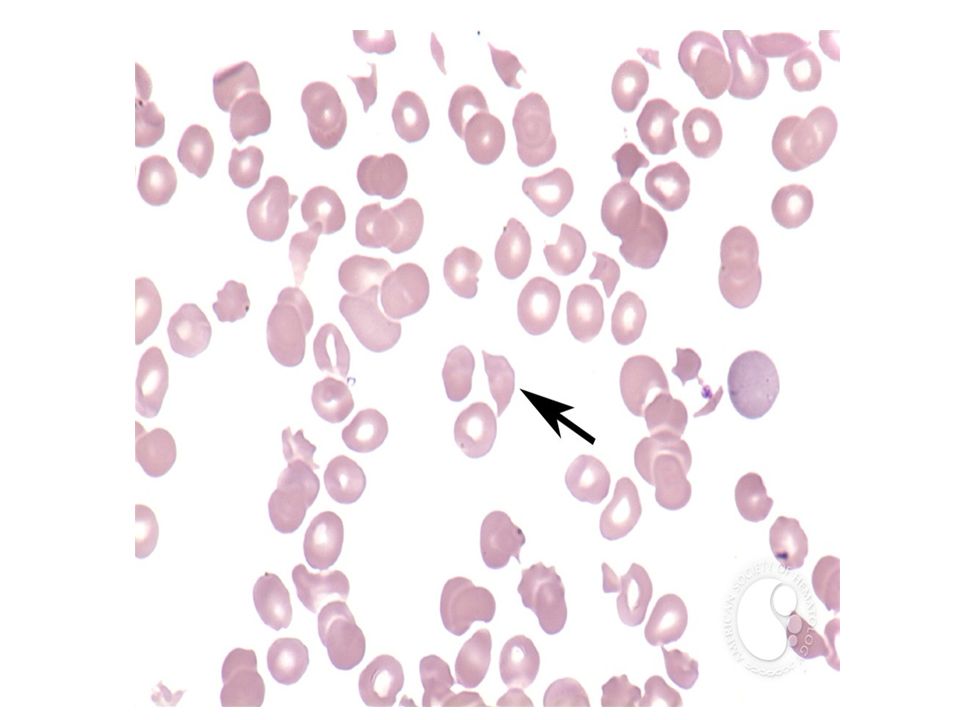
Περιφερικό επίχρισμα - Ανισοκυττάρωση (high RDW) - Πολυχρωματοφιλία (ΔΕΚ) - Σφαιροκύτταρα? Ελλιπτοκύτταρα? Ακανθοκύτταρα? Σχιστοκύτταρα? Δρεπανοκύτταρα?

13
: - Αμεση (Coombs) test – IgG +3
 test – IgG +3")
14
-Μακροκυτταρική -Αυξημένα δικτυερυθροκύτταρα Σφαιροκύτταρα -Θετική Άμεση Coombs Αυτοάνοση Αιμολυτική Αναιμία

15
ΕΡΩΤΗΣΕΙΣ 1. MCV? 2. ΔΕΚ (λειτουργία μυελού) 3. Συμμετοχή άλλων σειρών
 3. Συμμετοχή άλλων σειρών")
16
Περίπτωση 2 Ανδρας 63 ετώνπαρουσιάζεται στο ιατρείο με αδυναμία και αναιμία. Δεν λαμβάνει φάρμακα. Απύρετος Δεν εχει ηπατοσπληνομεγαλία ή λεμφαδενοπάθεια Πορφύρα στα κάτω άκρα

17
Περίπτωση 2 Laboratory evaluation - Set I: Ht 25 Hb 7.8 MCV 102 PLTs 62.000 ΔΕΚ1.2%

18
Αναιμία Μακροκυττάρωση Χαμηλά ΔΕΚ Θρομβοπενία

19
Υψηλό MCV, Χαμηλά ΔΕΚ Μεγαλοβλαστική Μυελοδυσπλαστικά Απλαστική Φάρμακα Αλκοολισμός

20
- B12 και φυλλικό φυσιολογικά Από το ιστορικό αλκοόλ, φάρμακα ΌΧΙ

23
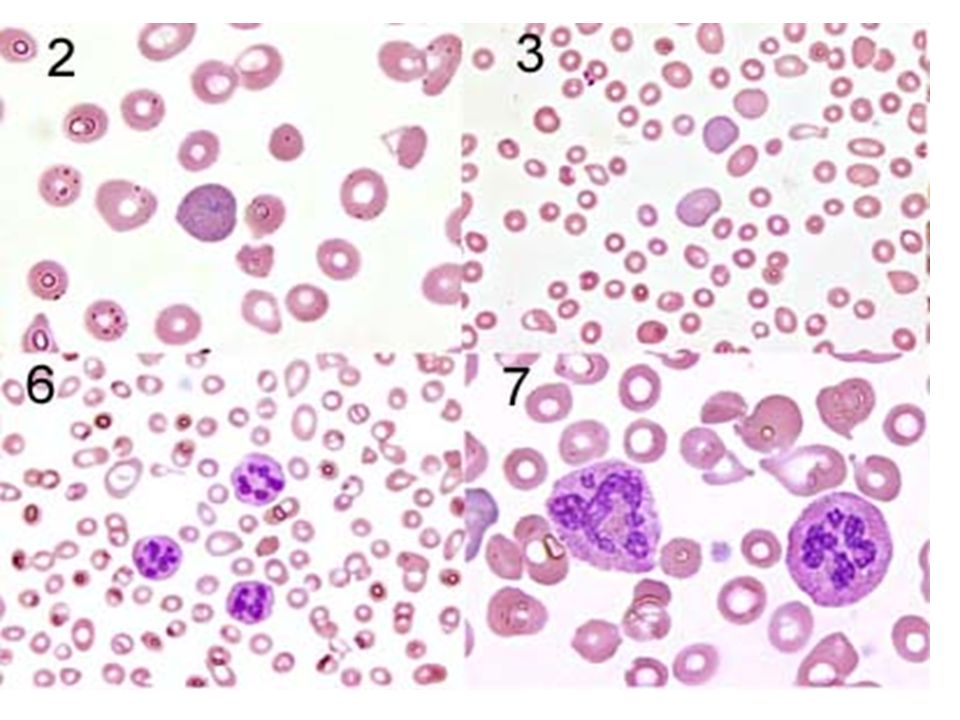
Ringed Sideroblast Iron

24
- Μακροκυτταρική Θρομβοπενία Χαμηλά ΔΕΚ Δυσπλασία Φυσιολογικό Β12, φυλλικό Μυελοδυσπλαστικό

25
Περίπτωση 3 Ένας 66 χρονος άστεγος διακομίζεται λόγω γενικευμένης σύγχυσης, αναφέρεται πτώση από σκάλες Στη φυσική εξέταση υπάρχει ουλή λαπαροτομής στην κοιλιά. Ht 24 Hb 7.8 MCV 108 WBC 2.000 PLTs κ.φ

27
B12 and folate B12 is a known cofactor in 2 enzymatic reactions (1) B12 is a cofactor of methionine synthase which is required to regenerate folate within the cell
 B12 is a cofactor of methionine synthase which is required to regenerate folate within the cell")
30
B1263 pg/mL(211 – 911) Folate13.2 ng/mL(>5.4) RBC Folate805 ng/mL(293 – 809) ?? Μεβαλοβλαστική Ελλειψη Β12

31
B12 deficiency Decreased intake –Veganism Impaired absorption –Gastric Poor stomach acidity Gastrectomy Pernicious anemia –Decreased secretion of intrinsic factor due to gastric atrophy –Chronic pancreatitis Decreased digestive enzyme secretion –Intestinal disease Ileal resection Ileal disease –Chron’s disease –Celiac sprue Fish tapeworm –Diphyllobothrium latum Blind loop –Intestinal bacterial overgrowth

32
Τι εγχείρηση ήταν η ουλή ? Μερική εντερεκτομή, με μέρος του ειλεού

33
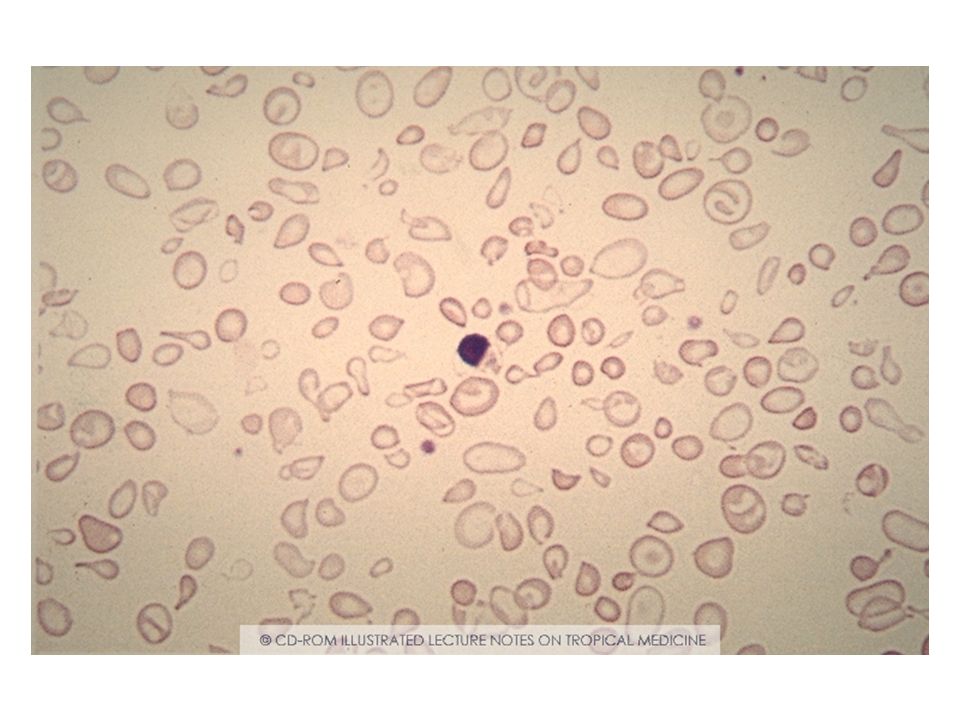
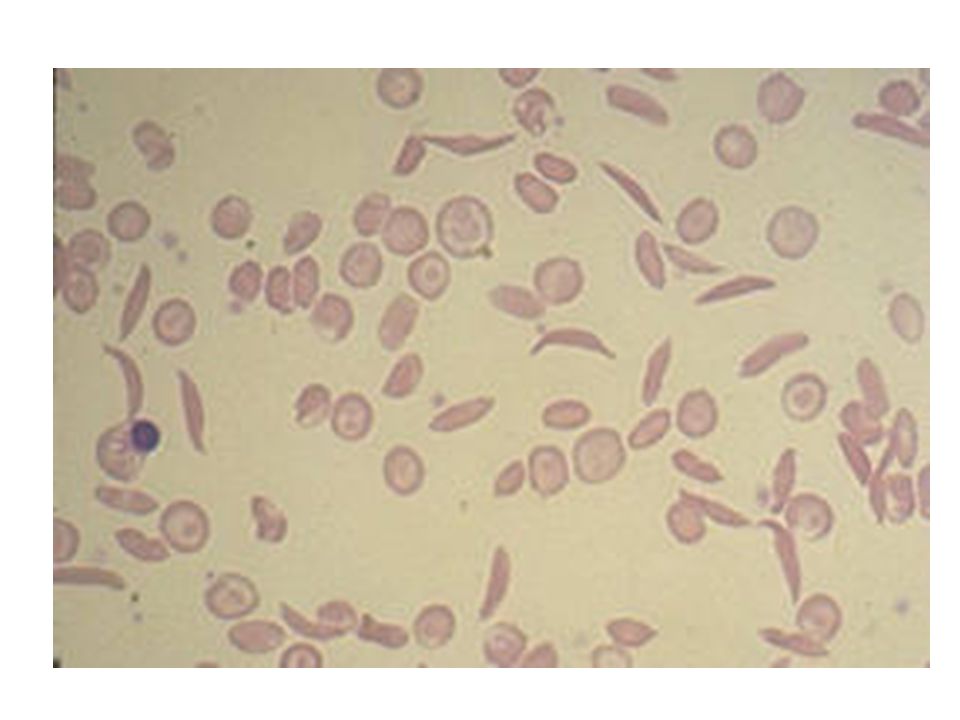
Περίπτωση 4 Αγόρι 12 ετών εμφανίζεται στα Ε.Ι με ωχρότητα και αναιμία ενώ αναφέρει και κόκκινα ούρα Ηt 22 Hb 7.1 MCV 100.2 WBC ΔΕΚ 10.2

34
ΕλλειψηG-6PD

35
Θα μετρήσουμε το ένζυμο? ΌΧΙ δεν αξιολογείται στη φάση της αιμόλυσης γιατί παράγονται νέα ερυθρά ΔΕΚ που μπορεί να έχουν επαρκή ποσότητα

36
Περίπτωση 5 Γυναίκα την 7 η εβδομάδα της κύησης hgb 6, hct 20, MCV 62, RDW 20, platelets 500K

37
Σίδηρος 23 Φερριτίνη 7

38
.

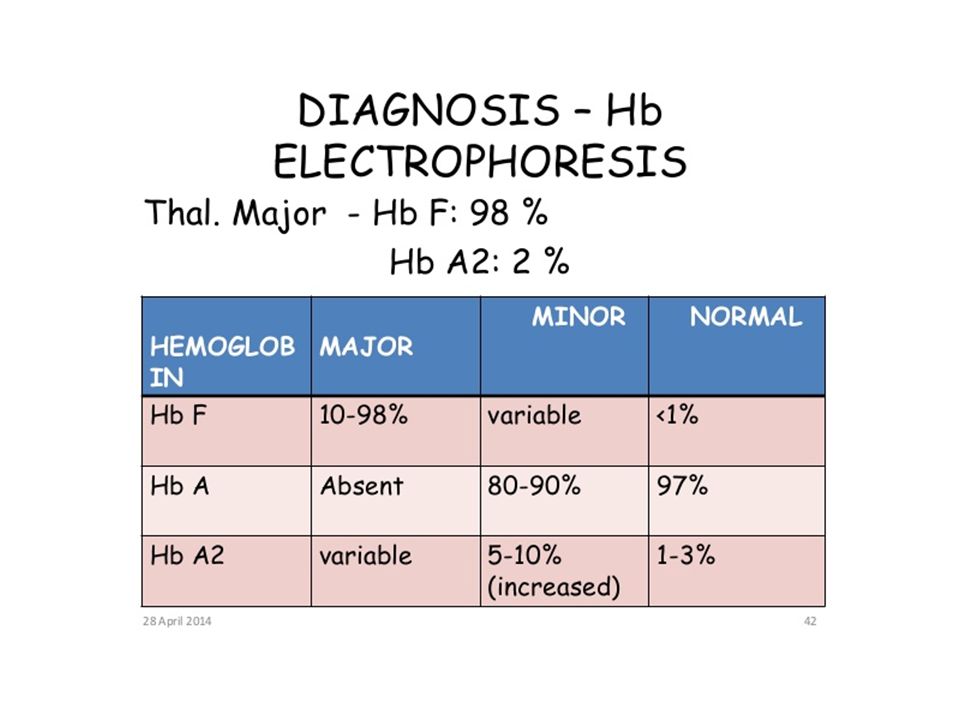
42
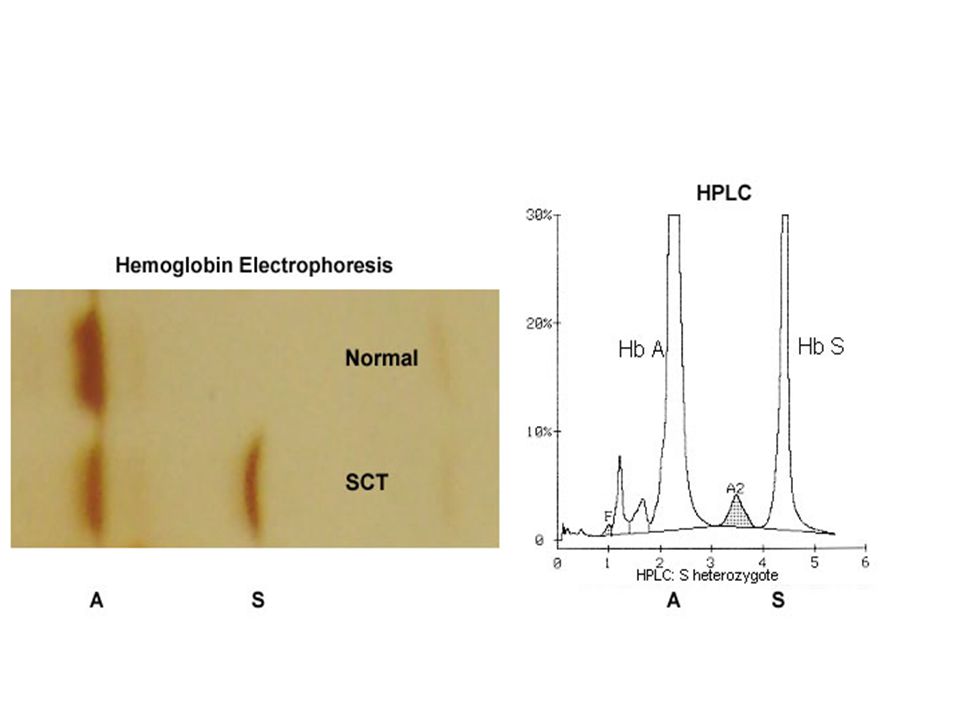
ΔΔ ετερόζυγη β-ΜΑ Η ηλεκτροφόρηση αιμοσφαιρίνης δεν αξιολογείται επί σιδηροπενίας

47
ΜΕΤΑΓΓΙΣΕΙΣ

48
Από τι πεθαίνουν οι ασθενείς με β-ΜΑ?

49
Liver Fe = 3.7-6.8% d wt Heart Fe = 0.6 –1.3% d wt Thyroid Fe = 1.6 – 6.8% d wt Pancreas Fe = 1.4-3.9% d wt Adapted from Modell & Berdoukas, 1984 Tissue Iron Concentrations in Transfusion- dependent Thalassemia Patients

50
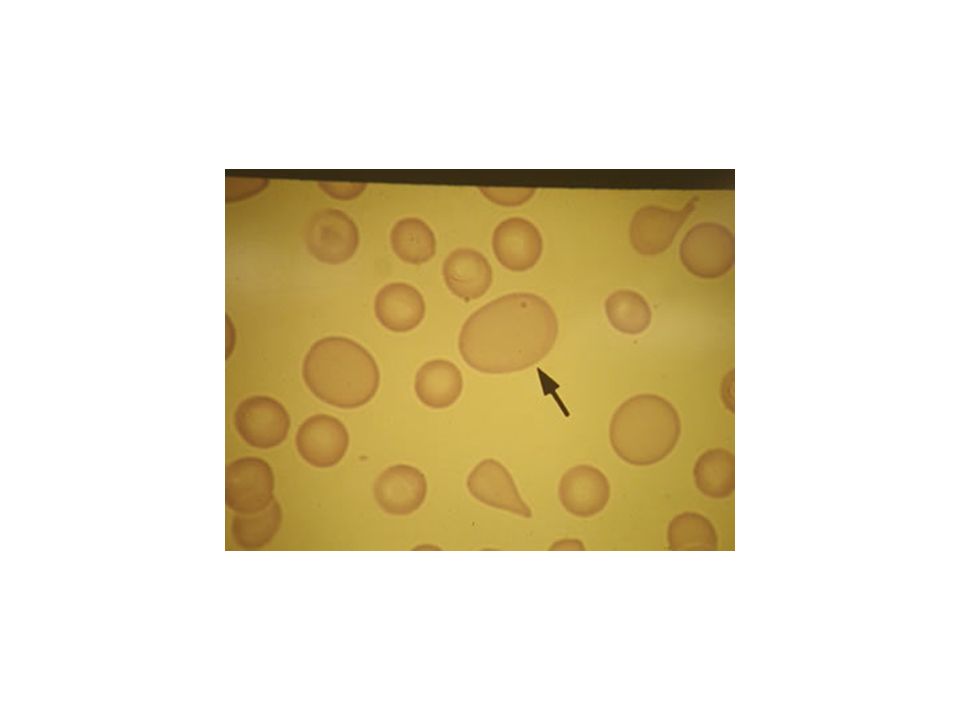
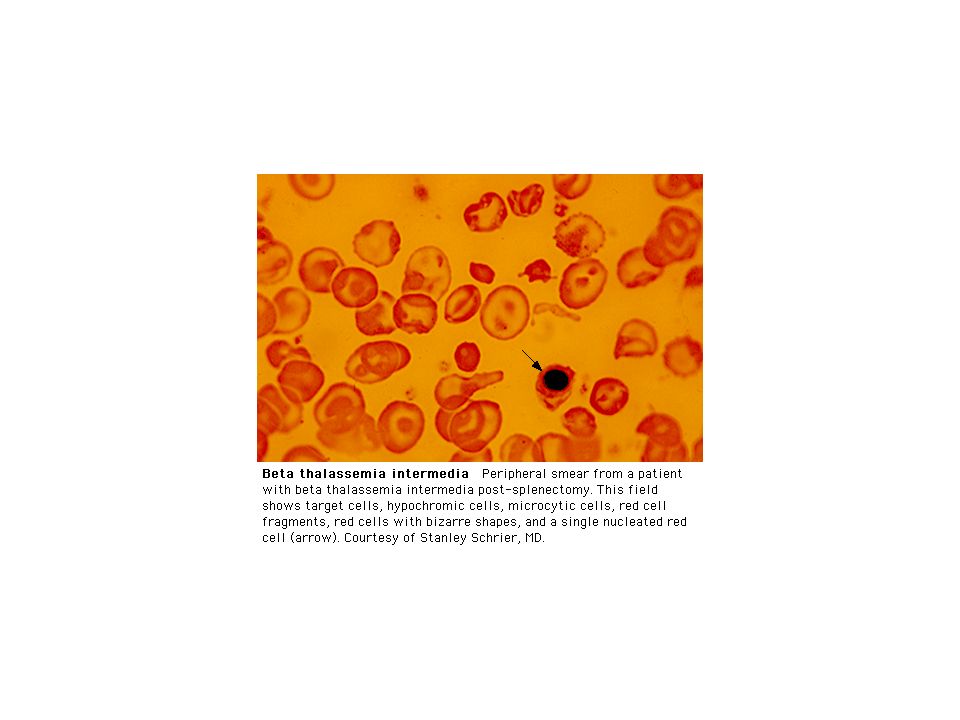
Τι έχει συμβεί στην ασθενή ? Σπληνεκτομή – Howell Jolie

53
Περίπτωση 7 άνδρας 28 ετών με HIVδιακομίζεται στα Ε.Ι λόγω αλλαγής του επιπέδου συνείδησηςΘερμοκρασία 39.2 wbc 4.2, ANC 2200, hgb 7.2, mcv 80, rdw 18, platelets 52K, creatinine 3.2, LDH 4200, bili 2.2

56
ΤΤΡ Θροβοπενία Μ.Α.Α Νευρολογικά συμπτώματα (κεφαλαλγία,αδυναμί α, παραισθήσεις, κώμα) Πυρετό Ευρήματα από τους νεφρούς.
 Πυρετό Ευρήματα από τους νεφρούς.")
58
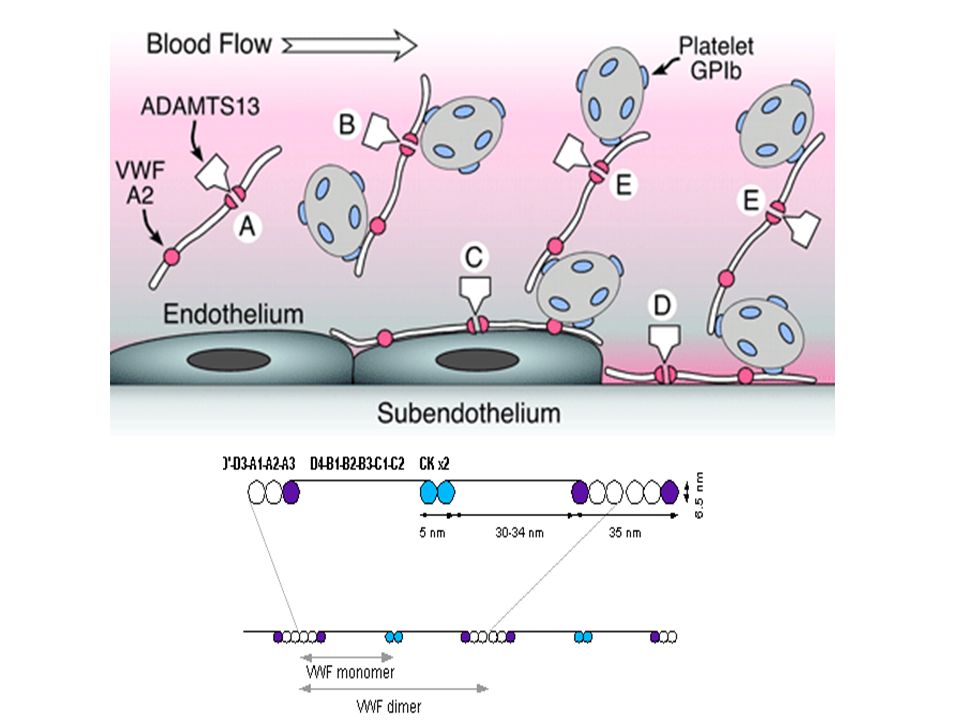
Συσσώρευ ση ΑΜΠ (Triggering event?) Μικροθρόμ βοι Increased shear stress Unfolding of UL- VWF Καταστροφή ερυθρών Δυσλειτουργία οργάνων Αυτοαντίσωμα έναντι ADAMTS-13 Παραμονή UL-VWF στο αίμα Πλασμαφαίρεση απομακρύνει το αντίσωμα και τα UL-VWF αποκαθιστά τη ADAMTS-13 Το ενδοθήλιο εκκρίνει UL-VWF (Triggering event?)
 Μικροθρόμ βοι Increased shear stress Unfolding of UL- VWF Καταστροφή ερυθρών Δυσλειτουργία οργάνων Αυτοαντίσωμα έναντι ADAMTS-13 Παραμονή UL-VWF στο αίμα Πλασμαφαίρεση απομακρύνει το αντίσωμα και τα UL-VWF αποκαθιστά τη ADAMTS-13 Το ενδοθήλιο εκκρίνει UL-VWF (Triggering event )")
59
Θρομβωτική θρομβοπενική πορφύρα

62
Table 29-05 Copyright © 2005 Elsevier Inc. (USA) All rights reserved.
 All rights reserved.")
66
Case 1 27 yo female with a history of lupus presents with a one week history of worsening dyspnea on exertion Reports dark urine Labs: hgb 8, mcv 101, rdw 19, total bili 1.9

72
Case 3 84 yo female living in an assisted living facility admitted for “failure to thrive” Admission labs: WBC 3.2 with normal diff, hgb 8.7, mcv 112, platelets 92K, LDH 1800

75
Case 4 68 yo white female with a 10 year history of poorly controlled type II DM, HTN, CAD presents for routine follow-up. CBC: wbc 7.2 with normal diff, hgb 9.8, hct 28, mcv 82, rdw 11, platelets 252K BMP: creatinine 3.4

80
Case 6 55 yo female with metastatic breast cancer reports worsening fatigue for a few weeks CBC: wbc 6.8 with 1% blasts, hgb 9.1,mcv 102, platelets 86K

82
Case 7 72 yo female with no significant PMH is brought for a routine physical by her daughter She has not seen a doctor in 20 years Daughter notes that mom is increasingly tired and has abdominal distension On exam, patient is pale and has marked splenomegaly CBC: wbc 4.2, hgb 7, hct 20, mcv 94, platelets 72K

85
(Oxidised form) (Reduced form)
 (Reduced form)")
86
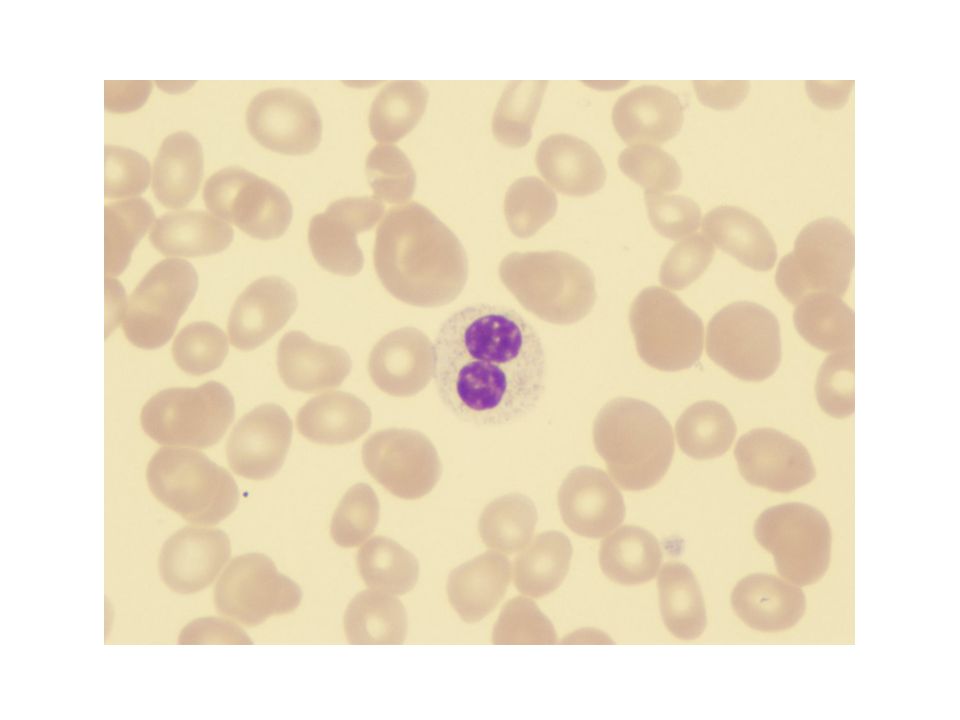
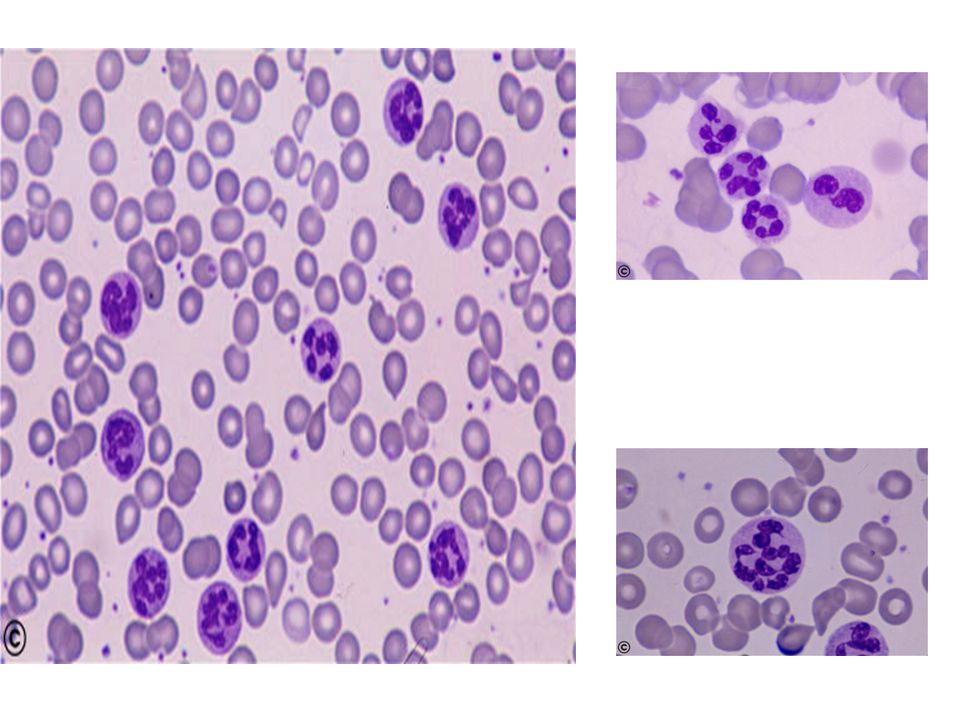
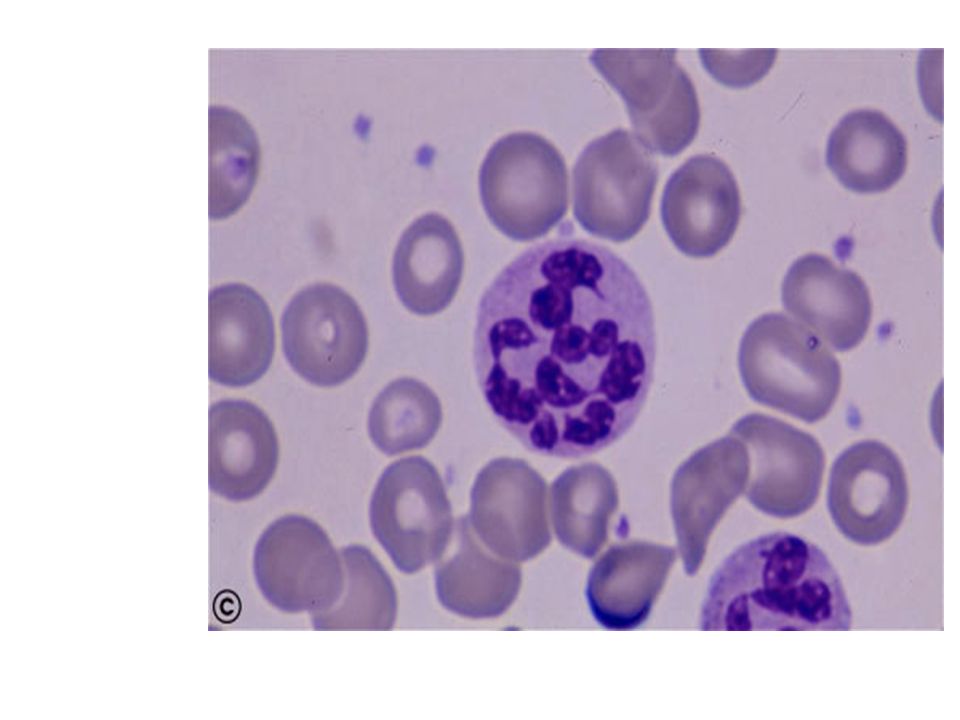
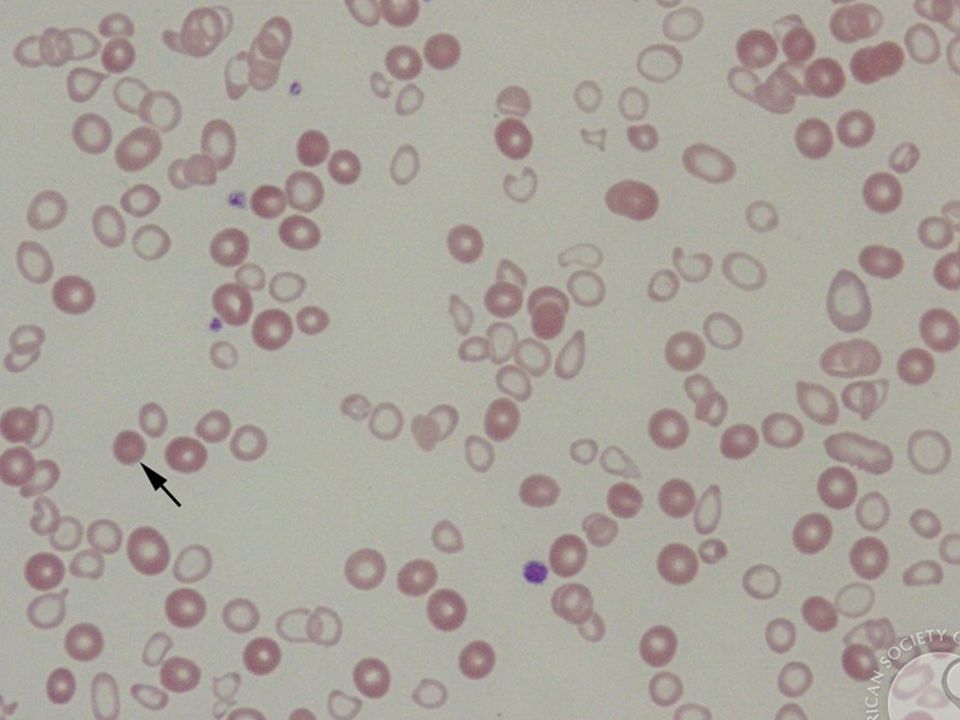
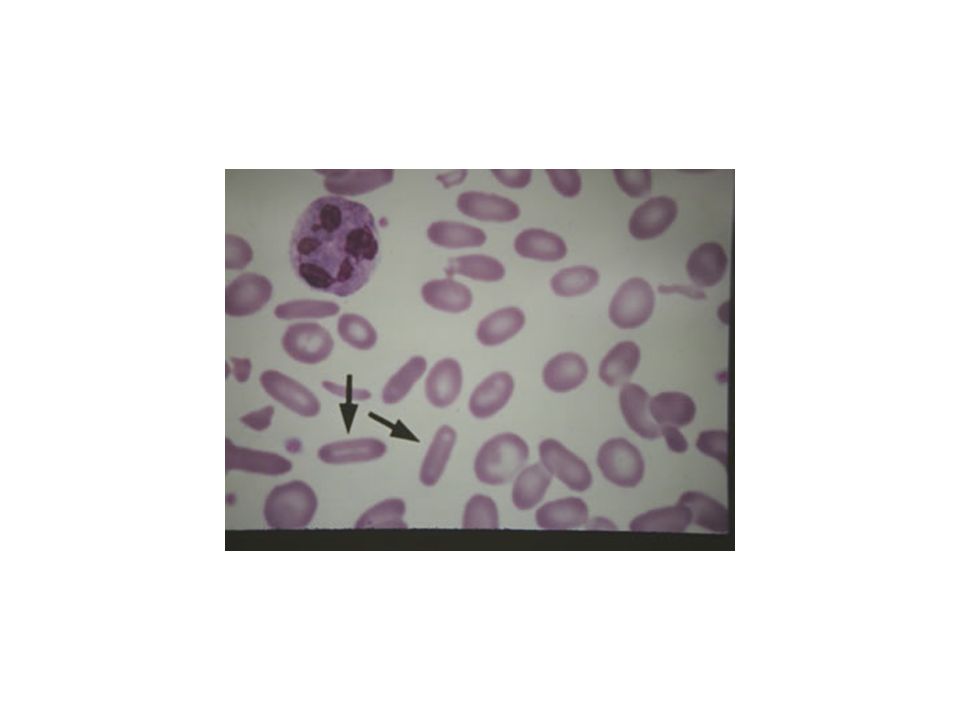
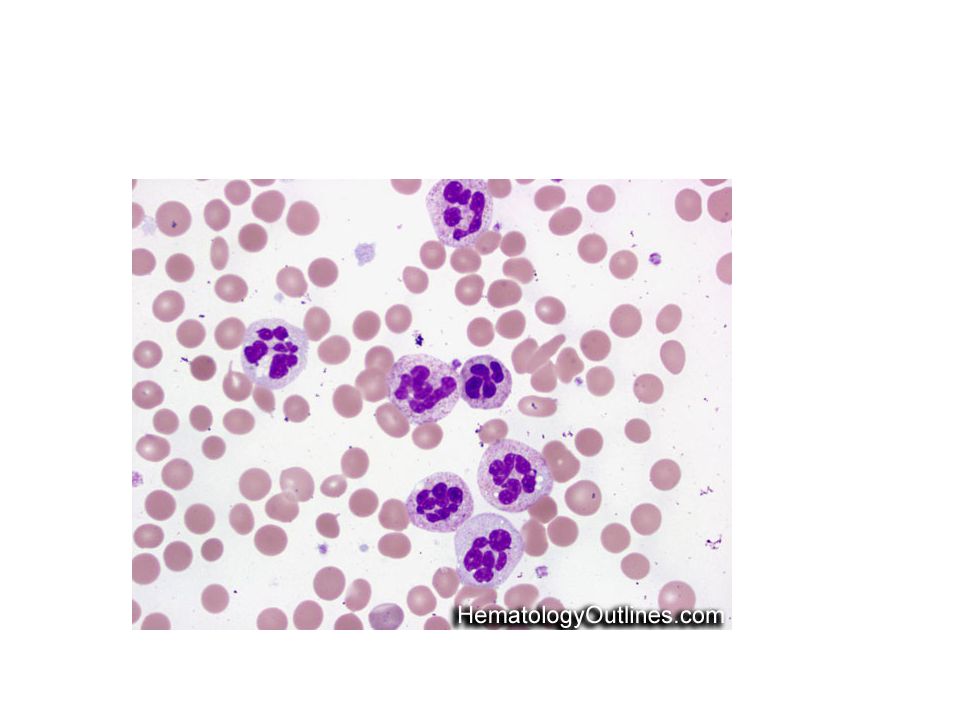
Megaloblastic anemia: Morphology--Blood Peripheral blood –Macro-ovalocytes –Neutrophil nuclear hypersegmentation Very sensitive and specific Normal Megaloblastoid

87
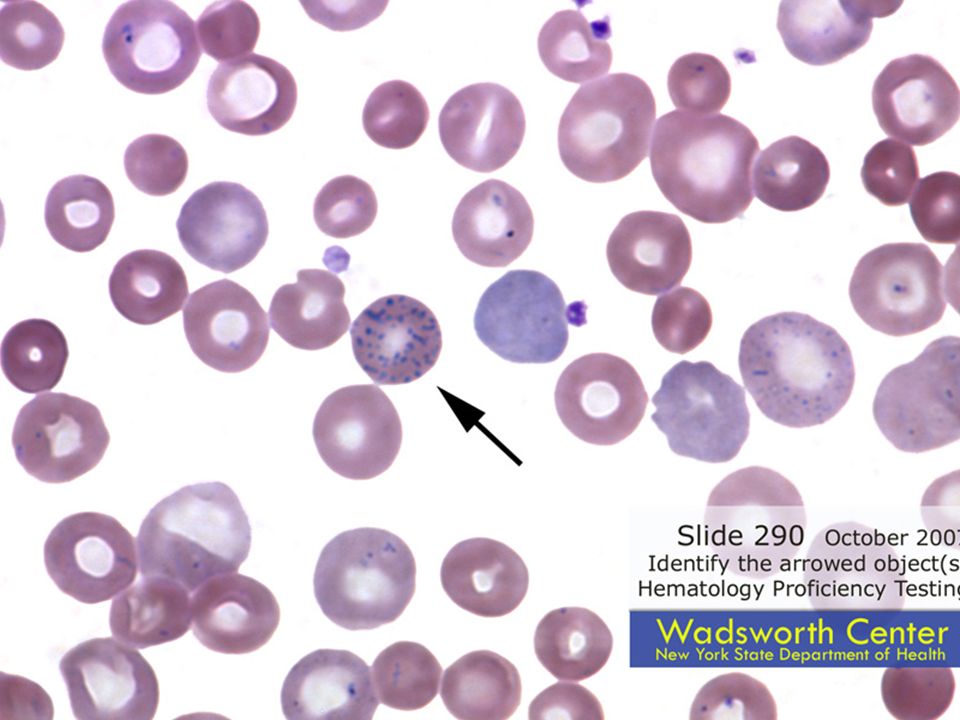
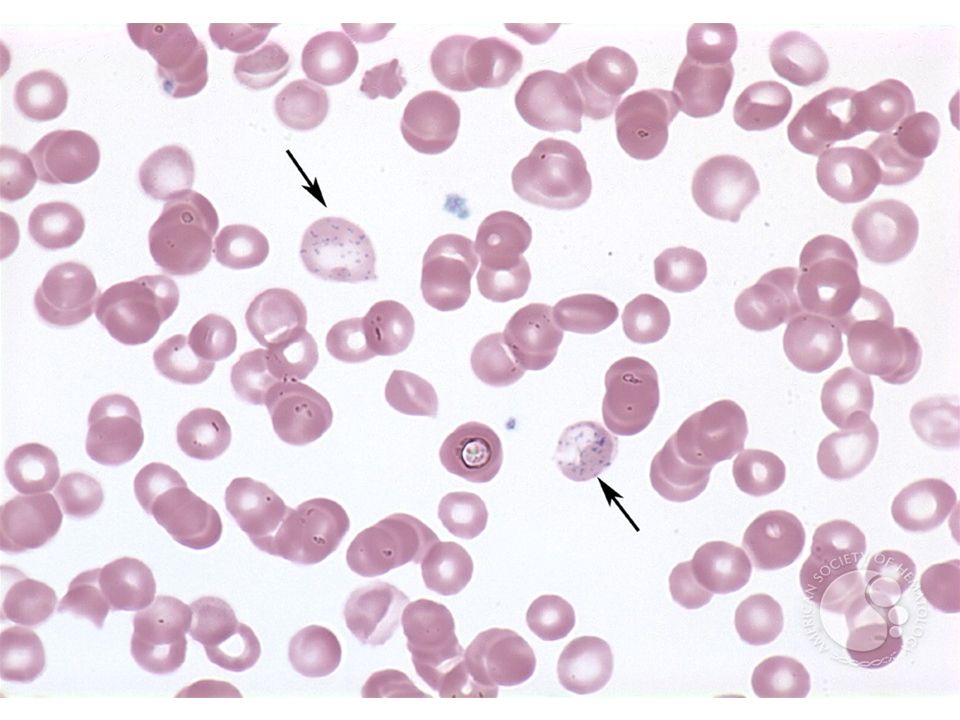
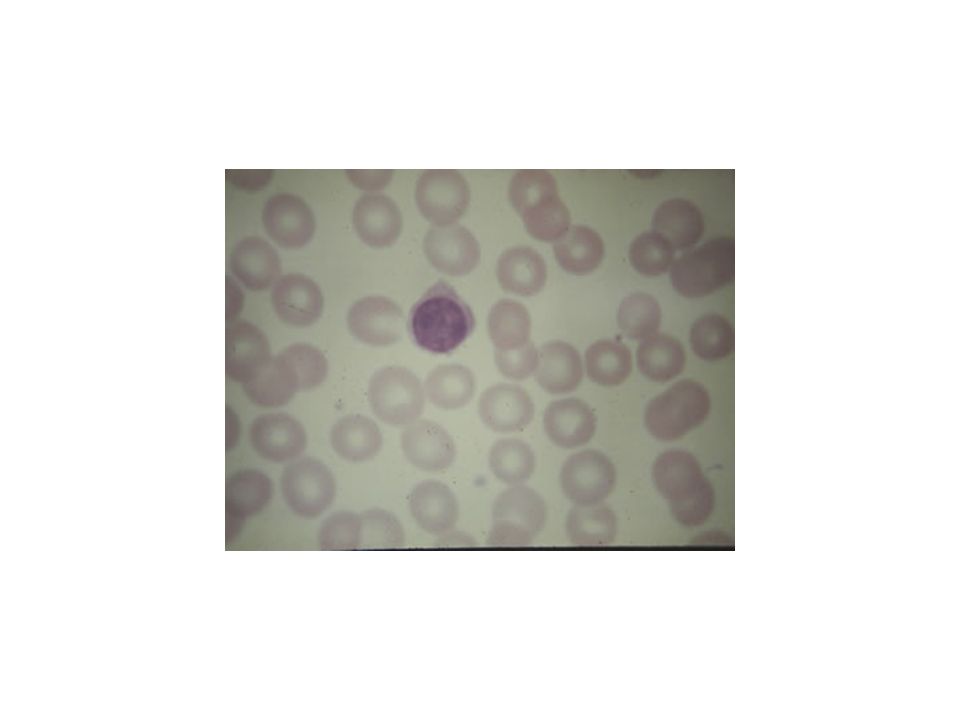
Cabot ring - Ring shaped, thin - May be figure of 8 shaped - Microtubule, remnants of of the mitotic spindle - Rarely seen Howell Jolly body - Round, dark, refractile RBC inclusion - Nuclear remnant - Most commonly seen in hyposplenism Basophilic stippling - Multiple small blue dots dispersed regularly throughout the RBC - RNA complexes

88
Clinical Features:Clinical Features: –Acute drug induced hemolysis: Aspirin, primaquine, quinine, chloroquine, dapsone….Aspirin, primaquine, quinine, chloroquine, dapsone…. –Chronic compensated hemolysis –Infection/acute illness –Neonatal jaundice –Favism

89
Inv:Inv: –e/o non-spherocytic intravascular hemolyis –P. Smear: Bite cells, blister cells, irregular small cells, Heinz bodies, polychromasia –G-6-PD level Treatment:Treatment: –Stop the precipitating drug or treat the infection –Acute transfusions if required

90
2. Pyruvate Kinase Deficiency –AR –Deficient ATP production, Chronic hemolytic anemia –Inv; P. Smear: Prickle cellsP. Smear: Prickle cells Decreased enzyme activityDecreased enzyme activity –Treatment: Transfusion may be requiredTransfusion may be required

91
Hemolobinopathies…

92
Autoimmune Hemolytic Anemia Result from RBC destruction due to RBC autoantibodies: Ig G, M, E, AResult from RBC destruction due to RBC autoantibodies: Ig G, M, E, A Most commonly-idiopathicMost commonly-idiopathic ClassificationClassification –Warm AI hemolysis:Ab binds at 37degree Celsius –Cold AI Hemolysis: Ab binds at 4 degree Celsius

93
1.Warm AI Hemolysis: –Can occurs at all age groups –F > M –Causes: 50% Idiopathic50% Idiopathic Rest - secondary causes:Rest - secondary causes: 1.Lymphoid neoplasm: CLL, Lymphoma, Myeloma 2.Solid Tumors: Lung, Colon, Kidney, Ovary, Thymoma 3.CTD: SLE,RA 4.Drugs: Alpha methyl DOPA, Penicillin, Quinine, Chloroquine 5.Misc: UC, HIV

94
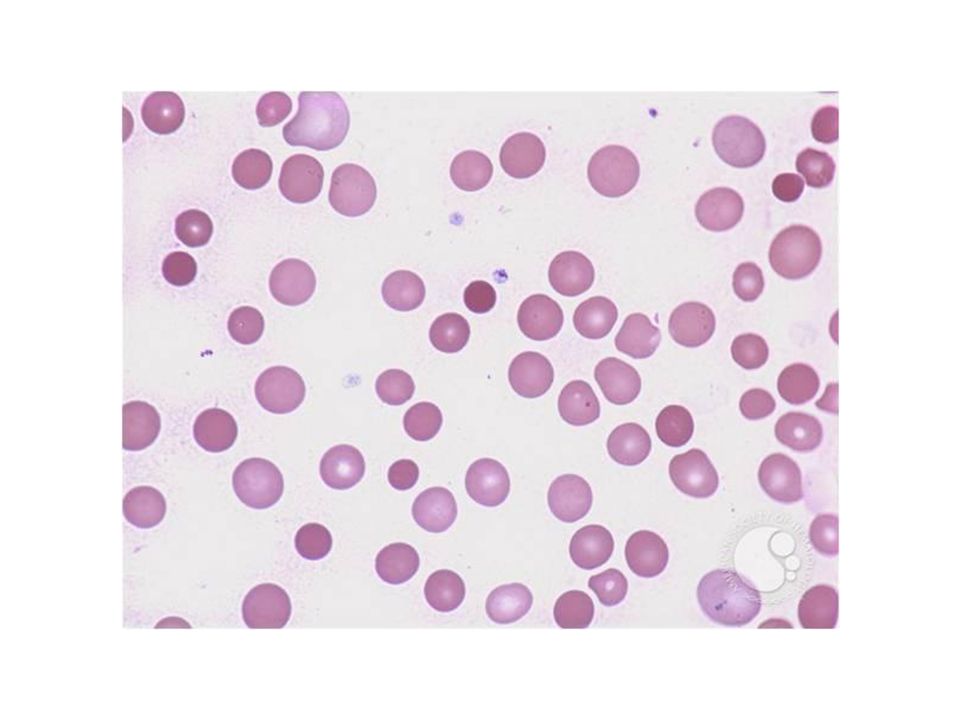
IMMUNOHEMOLYTIC ANEMIA MACROCYTE SPHEROCYTE

95
Direct antiglobulin test demonstrating the presence of autoantibodies (shown here) or complement on the surface of the red blood cell. complement

96
Inv:Inv: –e/o hemolysis, MCV –P Smear: Microspherocytosis, n-RBC –Confirmation: Coomb’s Test / Antiglobulin test TreatmentTreatment –Correct the underlying cause –Prednisolone 1mg/kg po until Hb reaches 10mg/dl then taper slowly and stop –Transfusion: for life threatening problems –If no response to steroids Spleenectomy or, –Immunosuppressive: Azathioprine, Cyclophosphamide

97
2. Cold AI Hemolysis –Usually Ig M –Acute or Chronic form –Chronic: C/F:C/F: –Elderly patients –Cold, painful & often blue fingers, toes, ears, or nose ( Acrocyanosis) Inv:Inv: –e/o hemolysis –P Smear: Microspherocytosis –Ig M with specificity to I or I Ag
 Inv:Inv: –e/o hemolysis –P Smear: Microspherocytosis –Ig M with specificity to I or I Ag.")
98
Other causes of Cold Agglutination:Other causes of Cold Agglutination: –Infection: Mycoplasma pneumonia, Infec Mononucleosis –PCH : Rare cause seen in children in association with cong syphilis

99
Treatment:Treatment: –Treatment of the underlying cause –Keep extremities warm –Steroids treatment –Blood transfusion

100
Non-Immune Acquired Hemolytic Anemia 1. Mechanical Trauma A). Mechanical heart valves, Arterial grafts: cause shear stress damage B).March hemoglobinuria: Red cell damage in capillaries of feet C). Thermal injury: burns D). Microangiopathic hemolytic anemia (MAHA): by passage of RBC through fibrin strands deposited in small vessels disruption of RBC eg: DIC,PIH, Malignant HTN,TTP,HUS
.March hemoglobinuria: Red cell damage in capillaries of feet C). Thermal injury: burns D). Microangiopathic hemolytic anemia (MAHA): by passage of RBC through fibrin strands deposited in small vessels disruption of RBC eg: DIC,PIH, Malignant HTN,TTP,HUS.")
101
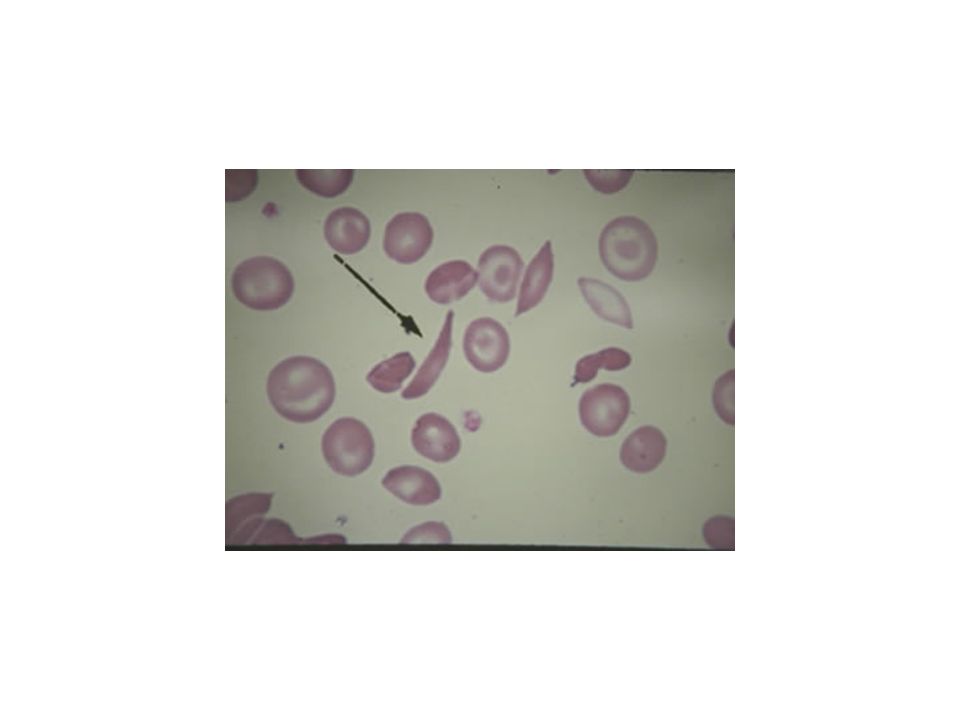
TRAUMATIC HEMOLYSIS

102
Acquired hemolysis 2.Infection F. malaria: intravascular hemolysis: severe called F. malaria: intravascular hemolysis: severe called ‘Blackwater fever’ Cl. perfringens septicemia oxidant denaturation of hemoglobin 3.Chemical/Drugs: oxidant denaturation of hemoglobin Eg: Dapsone, sulphasalazine, Arsenic gas, Cu, Nitrates & Nitrobenzene

103
The direct antiglobulin test was positive for complement (C3d) (++), and IgG (++-). Also was positive for agglutinins of IgM type and had a titer of 1:1024.

104
Serologies for human immunodeficiency virus, hepatitis B and C viruses, and Mycoplasma pneumoniae were negative. Rheumatoid factor and antinuclear antibodies were undetectable.

105
Prednisone therapy was started at a dose of 1 mg/kg intravenously, daily. Hemoglobin level rose to 11 g/dL, concomitantly with the improvement of hemolytic signs.

106
A reduction of positivity of both direct and indirect antiglobulin tests (polyvalent serum + ; C3d + ; IgG+ ), as well as a reduction of cold agglutinin titers (1:128), was observed 8 weeks after corticosteroid therapy.
, as well as a reduction of cold agglutinin titers (1:128), was observed 8 weeks after corticosteroid therapy.")
107
Three months later, corticosteroids were tapered to a maintenance dose of 25 mg daily. Hemolysis recurred again with the fall of hemoglobin to 7 g/dL.

108
The direct antiglobulin test recurred positive for polyvalent serum (+++), complement (+++), and IgG (+++), while cold agglutinin titers again became strongly positive (1:256).
, complement (+++), and IgG (+++), while cold agglutinin titers again became strongly positive (1:256).")
109
Immunophenotyping of bone marrow cells showed that 10% of all the cells were CD20 and CD19 positive.

110
CD20 is widely expressed on B-cells. CD20 could play a role in Ca2+ influx across plasma membranes, maintaining intracellular Ca2+ concentration and allowing activation of B cells.

111
Rituximab is a monoclonal antibody that binds to CD 20 Rituximab was started at the dose of 375 mg/mq once weekly, for a total of 4 doses

112
Hemoglobin value reached 13.5 g/dL just before the third dose, although biochemical signs of hemolysis remained substantially unaltered.

113
At the end of therapy, the hemolytic signs disappeared, the direct and indirect antiglobulin tests became negative, and cold agglutinin titers fell to 1:32 Immunophenotyping of bone marrow cells showed the absence of CD20 and CD19 B cells.

114
Summary of lecture Learning points

115
Approach to Anemia MCV: - Low: Iron deficiency Thalassemia trait Chronic disease Sideroblastic anemia - Normal: Iron deficiency (early) Chronic disease Renal failure
 Chronic disease Renal failure")
116
Approach to Anemia - High: Megaloblastic anemia Hemolytic anemia MDS / Aplastic anemia Drug-related Hypothyroidism Alcoholism Liver disease

117
Approach to Anemia Reticulocyte count: - Adequte (RPI>2): Hemolytic anemias (most) Acute blood loss Liver disease - Inadequate (RPI<2): Iron deficiency Megaloblastic anemia Anemia of chronic disease Bone marrow failure (malignancy, chemotherapy, MDS/Aplastic anemia)
: Hemolytic anemias (most) Acute blood loss Liver disease - Inadequate (RPI<2): Iron deficiency Megaloblastic anemia Anemia of chronic disease Bone marrow failure (malignancy, chemotherapy, MDS/Aplastic anemia)")
118
Approach to Anemia Additional lineage(s) involvement: - Leukopenia: Malignancy Chemotherapy Hypersplenism Drug-related Megaloblastic anemia Aplastic anemia
 involvement: - Leukopenia: Malignancy Chemotherapy Hypersplenism Drug-related Megaloblastic anemia Aplastic anemia")
119
Approach to Anemia - Thrombocytopenia: Malignancy Chemotherapy Hypersplenism Drug-related Megaloblastic anemia Aplastic anemia TTP DIC

120
Approach to Anemia In addition, blood smear always needs to be carefully assessed: Schistocytes? Spherocytes? Target cells? Normoblasts? Spur cells (acanthocytes)? Burr cells? Malignant cells (leukemia, lymphoma)? Malaria parasites? Sickle forms?
. Burr cells. Malignant cells (leukemia, lymphoma). Malaria parasites. Sickle forms .")
121
Anemia With Low MCV and Low Reticulocytes –Iron deficiency –Hereditary defects in hemoglobin synthesis (thalassemia trait) –Defects in heme synthsis (sideroblastic anemia) –Anemia of chronic disease
 –Defects in heme synthsis (sideroblastic anemia) –Anemia of chronic disease")
122
Anemia With Normal MCV and Low Reticulocytes Early or mild iron deficiency anemia Chemotherapy Anemia of chronic disease Anemia of renal failure

123
Anemia with High MCV and Low Reticulocytes Megaloblastic anemia Myelodysplastic syndrome / Aplastic anemia Drug-related anemia Hypothyroidism Alcoholism

124
Anemia with High Reticulocytes Low MCV: - Thalassemia Major (some cases) - Spherocytosis High MCV: - Sickle cell anemia - G-6PD deficiency - Immune hemolytic anemia - Malaria infection
 - Spherocytosis High MCV: - Sickle cell anemia - G-6PD deficiency - Immune hemolytic anemia - Malaria infection")
125
Anemia with Leukopenia and/or Thrombocytopenia Low reticulocytes: - Aplastic anemia/Myelodysplastic syndrome - Chemotherapy - Alcoholism - Megaloblastic anemia High reticulocytes: - TTP / DIC - Hypersplenism

Παρόμοιες παρουσιάσεις



















 ►Μακροκυτταρικές μεγαλοβλαστικές μακροκυττάρωση και μεγαλοβλαστικός μυελός ►Μακροκυτταρικές μη μεγαλοβλαστικές μακροκυττάρωση χωρίς.>")
. ΣΥΓΚΟΠΤΙΚΗ ΚΡΙΣΗ Αιφνίδια και σύντομη απώλεια συνείδησης που προκαλείται από ανεπαρκή εγκεφαλική αιμάτωση λόγω μειωμένης.>")








