Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Οξύ στεφανιαίο σύνδρομο και διακοπή του καπνίσματος: ουδέν κακόν αμιγές καλού! Γεώργιος Σ. Γκουμάς MD, PhD, FESC Αν. Διευθυντής Β Καρδιολογικής Κλινικής, Ευρωκλινική Αθηνών Μέλος Διοικητικού Συμβουλίου ΕΚΘΑ ΕΛΛΗΝΙΚΟ ΚΟΛΕΓΙΟ ΘΕΡΑΠΕΙΑΣ ΤΗΣ ΑΘΗΡΟΣΚΛΗΡΩΣΗΣ

2
ΔΗΛΩΣΗ ΣΥΓΚΡΟΥΣΗΣ ΣΥΜΦΕΡΟΝΤΩΝ Καμία σχετική με τη συγκεκριμένη ομιλία

3
Το κάπνισμα είναι μια χρόνια νόσος Οι περισσότεροι ασθενείς που προσπαθούν να κόψουν το κάπνισμα δεν θα πετύχουν αποχή 6 μηνών και θα υποτροπιάσουν, ενώ και οι μισοί από αυτούς που απέχουν από το κάπνισμα στους 6 μήνες θα υποτροπιάσουν μέσα στα επόμενα 8 χρόνια. Λιγότεροι από το 5% που προσπαθούν να διακόψουν το κάπνισμα εξακολουθούν να απέχουν 1 χρόνο μετά.

4
Φαρμακευτική αγωγή για τη διακοπή του καπνίσματος Οι κλινικοί ιατροί θα πρέπει να ενθαρρύνουν όλα τα πρόσωπα που επιχειρούν να διακόψουν το κάπνισμα να χρησιμοποιούν αποτελεσματικά φάρμακα για τη θεραπεία της εξάρτησης από την νικοτίνη εκτός αν υπάρχει αντένδειξη ή αν πρόκειται για ειδικούς πληθυσμούς, για τους οποίους δεν υπάρχουν επαρκή στοιχεία για την αποτελεσματικότητα τους (level of evidence Α) US Department of Health and Human Services, Public Health Service, 2008 www.surgeongeneral.gov/tobacco/treating_tobacco_use08.pdf
 US Department of Health and Human Services, Public Health Service,")
5
ACS in Smokers Morbidity and mortality are substantially increased among patients who continue to smoke following hospitalization for an acute coronary syndrome (ACS) Smoking cessation is of critical importance in these patients, yet less than a third of smokers who experience an ACS are able to remain abstinent following hospital discharge U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. 2004. Eisenberg MJ, et al. J Am Coll Cardiol. 2013;61:524–532.

6
ACS in Smokers Hospitalization for an acute cardiovascular event provides an important opportunity for quitting smoking. Smokers are often strongly motivated to quit because the risks of smoking are now personal. Most hospitals are smoke-free, requiring smokers to stop smoking at least temporarily. So the question is, can you prevent them from relapsing once they leave? The duration of hospitalization for acute myocardial infarction is usually brief and the hospital stay is busy, so it is difficult to gain the patient’s full attention for smoking-cessation counseling

7
ACS in Smokers Some clinicians are hesitant to add a smoking-cessation medication on top of a number of other medications that have been initiated or continued in the context of myocardial infarction and other medical conditions. Clinicians also may be concerned about the safety of smoking- cessation medications in patients with heart disease.

8
Nicotine medications increase heart rate, blood pressure, and myocardial contractility and have the potential to cause endothelial dysfunction and coronary vasoconstriction Υποκατάστατα Νικοτίνης (NRT)
")
9
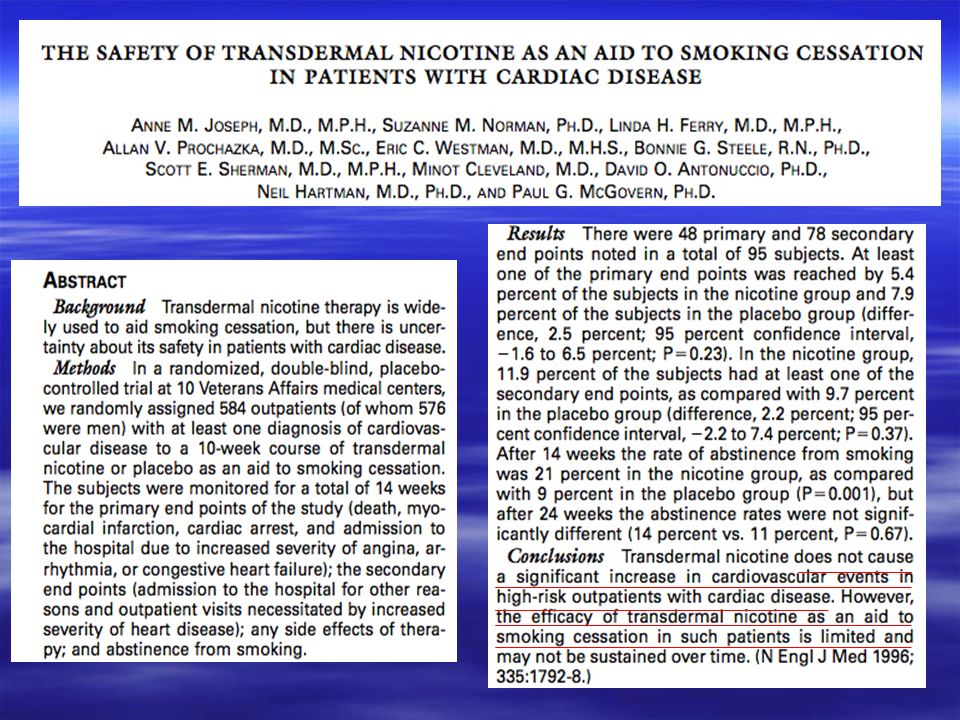
Όχι μετά από πρόσφατο ΕΜ ασταθή στηθάγχη επικίνδυνες για τη ζωή αρρυθμίες Ναι σταθερή στεφανιαία νόσος Αν και αποτελεί συνηθισμένη πρακτική τόσο στην Αμερική όσο και στις Ευρωπαϊκές χώρες η χορήγηση NRT σε ασθενείς μετά από οξύ στεφανιαίο σύνδρομο, ωστόσο δεν υπάρχουν τυχαιοποιημένες μελέτες. Υποκατάστατα Νικοτίνης (NRT)
.")
10
OEM AEE Hubbard et al Tobacco Control 2005 >30 000 χρήστες NRT -861 με ιστορικό CVD -506 με ιστορικό ΑΕΕ Στις 56 πρώτες ημέρες από την έναρξη της θεραπείας ο κίνδυνος για KA συμβάματα δεν αυξήθηκε σημαντικά Υποκατάστατα Νικοτίνης

12
Woolf Κ. Am J Cardiol 2012 NRT use after ACS was not associated with an increased risk of adverse cardiovascular events NRT was prescribed on hospital discharge

13
-Δεν αυξάνονται τα επίπεδα του μονοξειδίου του άνθρακα και δεν τροποποιείται η πηκτικότητα που αποτελούν τους κύριους μηχανισμούς αύξησης των ΚΑ συμβαμάτων λόγω του καπνίσματος Benowitz et al. J Am Coll Cardiol 1997 - Παρόλο που η χρησιμοποίηση NRT είναι λιγότερο επικίνδυνη σε σχέση με το κάπνισμα, ο κίνδυνος που σχετίζεται με NRT, δεν πρέπει να υποεκτιμάται σε ασθενείς με μειωμένη στεφανιαία εφεδρεία και αυξημένο κίνδυνο εμφάνισης επεισοδίων ισχαιμίας -Μικρότερη αύξηση των επιπέδων νικοτίνης συγκριτικά με το κάπνισμα. Γιατί η NRT λιγότερο επικίνδυνη από το κάπνισμα; Υποκατάστατα Νικοτίνης

15
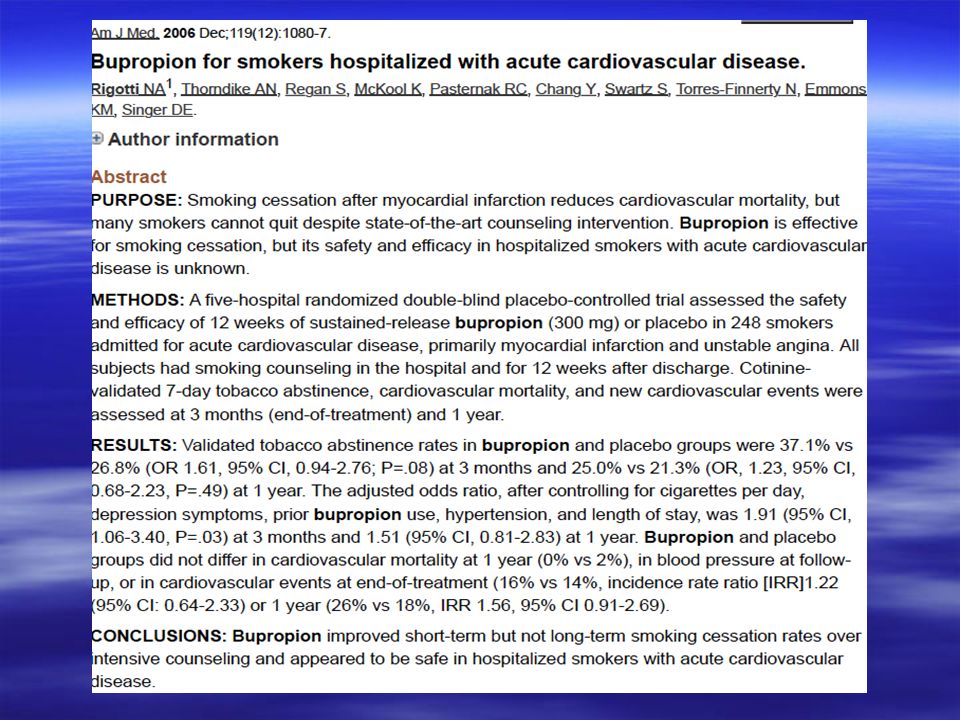
Planer et al. Arch Intern Med. 2011 Χορήγηση βουπροπιόνης κατά τη διάρκεια της νοσηλείας και για 8 εβδομάδες Δεν παρατηρήθηκε αύξηση των κλινικών συμβαμάτων ή αύξηση της πίεσης Η βουπροπιόνη δεν αύξησε το ποσοστό αποχής από το κάπνισμα. Η πιθανότητα διακοπής του καπνίσματος αυξανόταν σε αυτούς που κατά τη διάρκεια της νοσηλείας τους αντιμετωπίστηκαν επεμβατικά και μειωνόταν σε αυτούς που εμφάνισαν παρενέργειες από τη βουπροπιόνη (πχ ζαλάδα)
.")
19
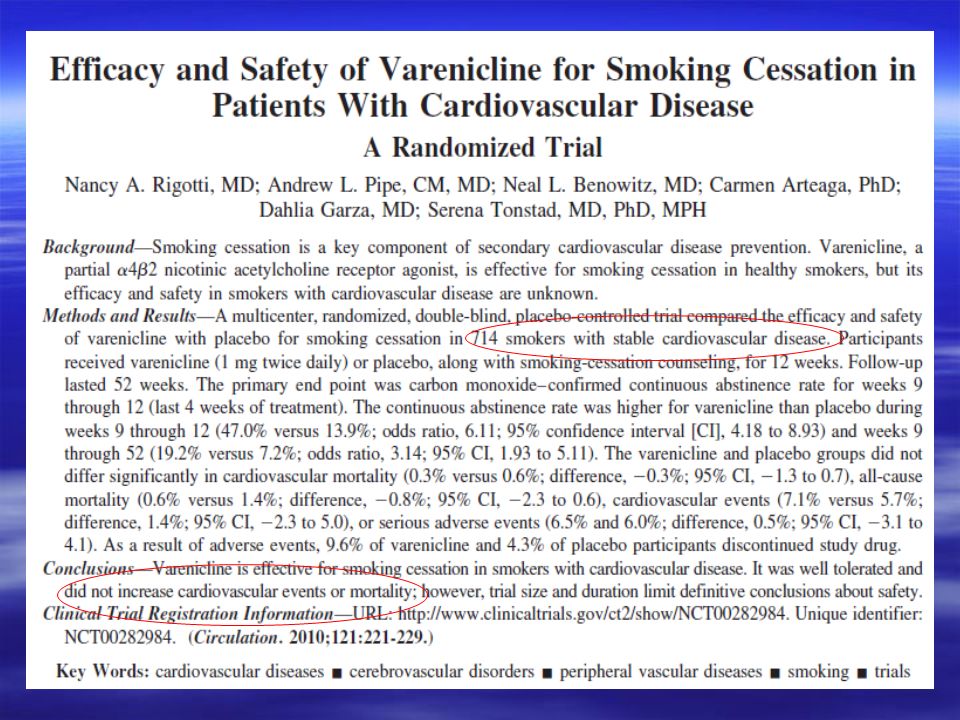
CMAJ Hays’ Commentary CMAJ July 2011 “Ο αυξημένος κίνδυνος εμφάνισης σοβαρών Κ/Α συμβαμάτων θα πρέπει να μετριαστεί από την σπανιότητα αυτών των συμβαμάτων μεταξύ των συμμετεχόντων ασθενών και στις δύο ομάδες θεραπείας (1.06% σε ασθενείς υπό θεραπεία με βαρενικλίνη και 0.82% σε ασθενείς υπό θεραπεία με εικονικό φάρμακο) “Το ποσοστό ασθενών που «χάθηκαν» (δεν κατέστη δυνατή η παρακολούθηση και η επικοινωνία μαζί τους μέχρι το τέλος της μελέτης) κατά τη διάρκεια της μελέτης ήταν μεγαλύτερο στην ομάδα του εικονικού φαρμάκου […] γεγονός που μεροληπτεί υπέρ της αναφοράς λιγότερων συμβαμάτων στην ομάδα του εικονικού φαρμάκου” “Το καλύτερο συμπέρασμα από την ανάλυση θα ήταν η ανάγκη για μελέτες με μεγαλύτερη ακρίβεια και επαρκή στατιστική ισχύ” “Το χειρότερο συμπέρασμα θα ήταν για τους επαγγελματίες υγείας να εγκατέλειπαν τη χρήση της βαρενικλίνης” “Είναι η βαρενικλινη ένα ασφαλές φάρμακο? Διάφορες τυχαιοποιημένες κλινικές μελέτες και μετα-αναλύσεις αναφέρουν ότι είναι. Είναι η βαρενικλίνη ένα ακίνδυνο φάρμακο? Σαφώς όχι, όπως παρουσίασε η μετα-ανάλυση αυτή του Singh. Ωστόσο, ο κίνδυνος εμφάνισης σοβαρών Κ/Α συμβαμάτων είναι μικρός, και αντισταθμίζεται σε μεγάλο βαθμό από τα οφέλη της μείωσης των πραγματικά επιβλαβών επιδράσεων του καπνίσματος”
![CMAJ Hays’ Commentary CMAJ July 2011 Ο αυξημένος κίνδυνος εμφάνισης σοβαρών Κ/Α συμβαμάτων θα πρέπει να μετριαστεί από την σπανιότητα αυτών των συμβαμάτων μεταξύ των συμμετεχόντων ασθενών και στις δύο ομάδες θεραπείας (1.06% σε ασθενείς υπό θεραπεία με βαρενικλίνη και 0.82% σε ασθενείς υπό θεραπεία με εικονικό φάρμακο) Το ποσοστό ασθενών που «χάθηκαν» (δεν κατέστη δυνατή η παρακολούθηση και η επικοινωνία μαζί τους μέχρι το τέλος της μελέτης) κατά τη διάρκεια της μελέτης ήταν μεγαλύτερο στην ομάδα του εικονικού φαρμάκου […] γεγονός που μεροληπτεί υπέρ της αναφοράς λιγότερων συμβαμάτων στην ομάδα του εικονικού φαρμάκου Το καλύτερο συμπέρασμα από την ανάλυση θα ήταν η ανάγκη για μελέτες με μεγαλύτερη ακρίβεια και επαρκή στατιστική ισχύ Το χειρότερο συμπέρασμα θα ήταν για τους επαγγελματίες υγείας να εγκατέλειπαν τη χρήση της βαρενικλίνης Είναι η βαρενικλινη ένα ασφαλές φάρμακο.](http://images.slideplayer.gr/32/9979987/slides/slide_19.jpg "Διάφορες τυχαιοποιημένες κλινικές μελέτες και μετα-αναλύσεις αναφέρουν ότι είναι. Είναι η βαρενικλίνη ένα ακίνδυνο φάρμακο. Σαφώς όχι, όπως παρουσίασε η μετα-ανάλυση αυτή του Singh. Ωστόσο, ο κίνδυνος εμφάνισης σοβαρών Κ/Α συμβαμάτων είναι μικρός, και αντισταθμίζεται σε μεγάλο βαθμό από τα οφέλη της μείωσης των πραγματικά επιβλαβών επιδράσεων του καπνίσματος .")
21
FDA Drug Safety Communication (June 16, 2011) Ο FDA ενημέρωσε το κοινό ότι το Chantix (varenicline) μπορεί να σχετίζεται με έναν μικρό, αυξημένο κίνδυνο κάποιων Κ/Α ανεπιθύμητων ενεργειών σε ασθενείς με Κ/Α νόσο. Ο FDA συνεχίζει να αξιολογεί την Κ/Α ασφάλεια του Chantix και ζητά από τη Pfizer να διεξάγει μία μεγάλη, συνδυαστική ανάλυση (μετά-ανάλυση) των τυχαιοποιημένων, ελεγχόμενων με εικονικό φάρμακο κλινικών μελετών. Ο FDA θα ενημερώσει το κοινό όταν υπάρξει κάποια επιπρόσθετη πληροφορία σχετικά. Οι εγκεκριμένες οδηγίες του φαρμάκου στην Αμερική έχουν ανανεωθεί (July 2011) – –Περιλαμβάνουν τα δεδομένα αποτελεσματικότητας της βαρενικλίνης στη διακοπή του καπνίσματος σε ασθενείς με Κ/Α νόσο – –Έχει προστεθεί συμβουλή στους ασθενείς με Κ/Α νόσο να πληροφορούν τους ιατρούς τους για οποιαδήποτε αλλαγή παρατηρήσουν ως προς τα Κ/Α συμπτώματα κατά τη διάρκεια που λαμβάνουν το CHANTIX και να καλούν τα επείγοντα αμέσως εάν παρατηρήσουν συμπτώματα καρδιακής προσβολής (ΕΜ)
 των τυχαιοποιημένων, ελεγχόμενων με εικονικό φάρμακο κλινικών μελετών. Ο FDA θα ενημερώσει το κοινό όταν υπάρξει κάποια επιπρόσθετη πληροφορία σχετικά. Οι εγκεκριμένες οδηγίες του φαρμάκου στην Αμερική έχουν ανανεωθεί (July 2011) – –Περιλαμβάνουν τα δεδομένα αποτελεσματικότητας της βαρενικλίνης στη διακοπή του καπνίσματος σε ασθενείς με Κ/Α νόσο – –Έχει προστεθεί συμβουλή στους ασθενείς με Κ/Α νόσο να πληροφορούν τους ιατρούς τους για οποιαδήποτε αλλαγή παρατηρήσουν ως προς τα Κ/Α συμπτώματα κατά τη διάρκεια που λαμβάνουν το CHANTIX και να καλούν τα επείγοντα αμέσως εάν παρατηρήσουν συμπτώματα καρδιακής προσβολής (ΕΜ).")
23
-Περισσότερες Μελέτες -Διαφορά στη Μεθοδολογία, πχ εξετάστηκαν μόνο τα συμβάματα κατά τη διάρκεια της θεραπείας The absolute difference in risk for the primary outcome did not reach statistical significance (risk difference = 0.27%, 95% CI - 0.10% to 0.63%). Prochaska et al BMJ 2012

24
1) the study end points were pre-specified 2) the composite end point focused on ischemic events; 3) all serious CV events were adjudicated by an independent adjudication committee blind to treatment assignment 4) subject-level data were available, making it possible to conduct a time-to-first-event analysis rather than a meta- analysis of summary data.
 the study end points were pre-specified 2) the composite end point focused on ischemic events; 3) all serious CV events were adjudicated by an independent adjudication committee blind to treatment assignment 4) subject-level data were available, making it possible to conduct a time-to-first-event analysis rather than a meta- analysis of summary data.")
25
Νεώτερα δεδομένα HR analysis for MACE+ for treatment plus 30 days MACE+: MACE plus new onset, worsening or any procedure for peripheral vascular disease, hospitalization for unstable angina, and performance of coronary revascularization. Ware J et al. Am J of Therapeutics 2013

26
Smoking is a major risk factor for coronary artery disease (1) while acute coronary syndromes are the most dangerous manifestation of atherosclerosis. Individual counselling for smoking cessation during and after hospitalization has shown limited efficacy (2). We examined the efficacy of varenicline in combination with an intensive individual counselling program for smoking cessation for patients admitted to our hospital with a diagnosis of acute coronary syndrome. Background and Aims Varenicline in combination with intense individual counselling for smoking cessation in patients with an acute coronary syndrome Goumas G, Athanassias D, Kribas P,, Alexopoulos N, Papamichail N, Roumeliotaki G, Richter D. 2 nd Cardiology Department, Athens Euroclinic During 6 months of follow-up, one patient died (death not related to varenicline) and one was lost to follow- up. Among 54 remaining patients, the rate of abstinence (fig.1) was 76 % at 1 month, 71 % at 3 months and it remained 71 % through 6 months after their hospitalization. Among the 56 patients, 48 underwent coronary vascularisation (41 PTCA, 7 CABG). All 7 patients that underwent CABG quit smoking. In this population of ACS varenicline was well tolerated: 14 patients reported nausea and 3 reported insomnia, but no one discontinued treatment because of the side effects. Varenicline administration showed to be as safe and probably better tolerated than in the general population. Conclusion The combination of varenicline with an intensive individual counselling program appears to be an extremely efficient policy for smoking cessation after an acute coronary syndrome, but also a safe one. 56 sequential patients (mean age 52.4 y, all white, 40 male, 16 female) with unstable angina or acute myocardial infarction (NSTEMI or STEMI) were included in the study. Treatment with varenicline was initiated in all patients on the second day of their admission and was also prescribed along with their other medication after their discharge (0.5 mg once daily for 3 days, 0.5 mg twice daily for 4 days, and then 1.0 mg twice daily for a total of 12 weeks), the quitting patients were given a second three months varenicline treatment period to prevent relapses. Furthermore, all patients underwent intensive individual counselling program which included 30 minutes ofbedside counselling twice during hospitalisation (2 nd Methods Treatment with varenicline continued after month 3 only in those who had stopped smoking. Smoking behaviour was assessed by self-report 1, 3 and 6 months after hospitalization. The prevalence of abstinence at 1, 3 and 6 months after hospital discharge was the primary outcome of our study. Results Figure 1. Abstinence rate at 1, 3 and 6 months 1.Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: a systematic review. JAMA. 2003;290:86 –97. 2.Hajek P, Taylor TZ, Mills P. Brief intervention during hospital admission to help patients to give up smoking after myocardial infarction and bypass surgery: randomised controlled trial. BMJ 2002;324:87-9. References day and day of discharge), printed material with advices, 30 minutes counselling during their re- evaluation visits at our outpatient cardiology department, 1 and 3 months after hospitalization and 6 nurse-initiated counselling calls.
. We examined the efficacy of varenicline in combination with an intensive individual counselling program for smoking cessation for patients admitted to our hospital with a diagnosis of acute coronary syndrome. Background and Aims Varenicline in combination with intense individual counselling for smoking cessation in patients with an acute coronary syndrome Goumas G, Athanassias D, Kribas P,, Alexopoulos N, Papamichail N, Roumeliotaki G, Richter D. 2 nd Cardiology Department, Athens Euroclinic During 6 months of follow-up, one patient died (death not related to varenicline) and one was lost to follow- up. Among 54 remaining patients, the rate of abstinence (fig.1) was 76 % at 1 month, 71 % at 3 months and it remained 71 % through 6 months after their hospitalization. Among the 56 patients, 48 underwent coronary vascularisation (41 PTCA, 7 CABG). All 7 patients that underwent CABG quit smoking. In this population of ACS varenicline was well tolerated: 14 patients reported nausea and 3 reported insomnia, but no one discontinued treatment because of the side effects. Varenicline administration showed to be as safe and probably better tolerated than in the general population. Conclusion The combination of varenicline with an intensive individual counselling program appears to be an extremely efficient policy for smoking cessation after an acute coronary syndrome, but also a safe one. 56 sequential patients (mean age 52.4 y, all white, 40 male, 16 female) with unstable angina or acute myocardial infarction (NSTEMI or STEMI) were included in the study. Treatment with varenicline was initiated in all patients on the second day of their admission and was also prescribed along with their other medication after their discharge (0.5 mg once daily for 3 days, 0.5 mg twice daily for 4 days, and then 1.0 mg twice daily for a total of 12 weeks), the quitting patients were given a second three months varenicline treatment period to prevent relapses. Furthermore, all patients underwent intensive individual counselling program which included 30 minutes ofbedside counselling twice during hospitalisation (2 nd Methods Treatment with varenicline continued after month 3 only in those who had stopped smoking. Smoking behaviour was assessed by self-report 1, 3 and 6 months after hospitalization. The prevalence of abstinence at 1, 3 and 6 months after hospital discharge was the primary outcome of our study. Results Figure 1. Abstinence rate at 1, 3 and 6 months 1.Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: a systematic review. JAMA. 2003;290:86 –97. 2.Hajek P, Taylor TZ, Mills P. Brief intervention during hospital admission to help patients to give up smoking after myocardial infarction and bypass surgery: randomised controlled trial. BMJ 2002;324:87-9. References day and day of discharge), printed material with advices, 30 minutes counselling during their re- evaluation visits at our outpatient cardiology department, 1 and 3 months after hospitalization and 6 nurse-initiated counselling calls..")
28
Study Design Multicenter –40 Canadian and US centers Double-blind Randomized Placebo-controlled Investigator-initiated –Funding & study drug/placebo from Pfizer Inc. –No role in design, conduct, analysis, or reporting EV TA

29
Trial Schematic EV TA Randomization Smokers Hospitalized for ACS Informed Consent & Eligibility Assessment Baseline Visit & 1 st Dose In-Hospital Follow-Up Visits Telephone: Weeks 1, 2 & 8 Clinic: Weeks 4, 12 & 24 Primary Endpoint Smoking abstinence at Week 24 Low-Intensity Counselling at Baseline & All Follow-Up Contacts Varenicline for 12 Weeks Placebo for 12 Weeks

30
Inclusion/Exclusion Main Inclusion Criteria –Age ≥ 18 years and motivated to quit smoking –Smoke ≥ 10 cigarettes/day on average in the past year –Hospitalized with ACS Main Exclusion Criteria –History of neuropsychiatric disorders –Prior varenicline use, or use of smoking cessation pharmacotherapy at the time of ACS –Cardiogenic shock or renal impairment at randomization –Hepatic impairment prior to ACS –Excessive alcohol use, or current use of: marijuana, non- cigarette tobacco products, OTC stimulants or anorectics EV TA

31
Endpoints Primary Endpoint (ITT) –7-day point prevalence abstinence at week 24 Self-reported abstinence in past week and exhaled CO ≤ 10 ppm Secondary Endpoints (ITT) –Continuous abstinence at week 24 Self-reported abstinence since baseline and exhaled CO ≤ 10 ppm at all follow-up visits up to and including week 24 –≥ 50% reduction in daily cigarette consumption at week 24 Safety Endpoints –Side effects, SAEs, MACE, neuropsychiatric events –SAEs adjudicated by an EEC (blinded to treatment status) –Trial monitored by an external DSMB EV TA
 –7-day point prevalence abstinence at week 24 Self-reported abstinence in past week and exhaled CO ≤ 10 ppm Secondary Endpoints (ITT) –Continuous abstinence at week 24 Self-reported abstinence since baseline and exhaled CO ≤ 10 ppm at all follow-up visits up to and including week 24 –≥ 50% reduction in daily cigarette consumption at week 24 Safety Endpoints –Side effects, SAEs, MACE, neuropsychiatric events –SAEs adjudicated by an EEC (blinded to treatment status) –Trial monitored by an external DSMB EV TA")
32
Trial Flow EV TA Smoking Status for ITT Analysis* n=148 Patients Randomized n=302 Placebo n=151Varenicline n=151 Died n=2 Withdrew Consent n=9 Lost to Follow-Up n=16 Died n=0 Withdrew Consent n=10 Lost to Follow-Up n=18 Treatment Weeks 1-12 Died n=1 Withdrew Consent n=0 Lost to Follow-Up n=5 Died n=0 Withdrew Consent n=2 Lost to Follow-Up n=7 Follow-Up Weeks 13-24 Smoking Status for ITT Analysis* n=151 Week 24 * Assumed that patients who withdrew or who were lost to follow-up returned to smoking at their baseline rate

33
Primary Endpoint p<0.001 p=0.012 p<0.001 EV TA NNT: 6.8 ↓ Primary Endpoint

34
Safety Endpoints Varenicline (n = 151) Placebo (n = 151) P- Value SAEs Within 30 Days of Treatment Discontinuation, n (%) Patients with any SAE 18 (11.9)17 (11.3)>0.99 Composite MACE 6 (4.0)7 (4.6)>0.99 Death 2 (1.3)00.50 Myocardial infarction 3 (2.0) 1.00 Unstable angina 1 (0.7)5 (3.3)0.21 Other cardiovascular events 3 (2.0)2 (1.3)>0.99 Neuropsychiatric events Seizure, suicidal ideation 00---- Other 1 (0.7)0>0.99 Other 9 (6.0)8 (5.3)>0.99 Most Common Side Effects – 12-Week Cumulative, n (%) Insomnia 27 (17.9)19 (12.6)0.26 Nausea 21 (13.9)13 (8.6)0.20 Abnormal dreams 23 (15.2)7 (4.6)<0.01 EV TA
 Placebo (n = 151) P- Value SAEs Within 30 Days of Treatment Discontinuation, n (%) Patients with any SAE 18 (11.9)17 (11.3)>0.99 Composite MACE 6 (4.0)7 (4.6)>0.99 Death 2 (1.3)00.50 Myocardial infarction 3 (2.0) 1.00 Unstable angina 1 (0.7)5 (3.3)0.21 Other cardiovascular events 3 (2.0)2 (1.3)>0.99 Neuropsychiatric events Seizure, suicidal ideation Other 1 (0.7)0>0.99 Other 9 (6.0)8 (5.3)>0.99 Most Common Side Effects – 12-Week Cumulative, n (%) Insomnia 27 (17.9)19 (12.6)0.26 Nausea 21 (13.9)13 (8.6)0.20 Abnormal dreams 23 (15.2)7 (4.6)<0.01 EV TA")
35
Limitations Only enrolled patients motivated to quit smoking –Smoking abstinence rates likely optimistic vs. real-world Small sample size –Limits ability to definitively address the cardiovascular safety of varenicline Smokers represent a challenging patient population –As with other smoking cessation trials, a not insubstantial number of patients withdrew or were lost to follow-up Low-intensity counseling –High-intensity counselling could have improved quit rates EV TA

36
ACS in Smokers Managing withdrawal with nicotine-replacement therapy in- hospital in the context of ACS is extremely important in addition to, based on EVITA trial, starting varenicline to prevent relapse Varenicline will reduce the craving for cigarettes, but the impact is not immediate. Using nicotine-replacement therapy will immediately affect that craving. So the combination of the two may be very powerful.

37
ACS in Smokers Effective counseling in the hospital for all smokers Effective transition from inpatient to outpatient smoking cessation treatment, with a minimum of 1-month follow-up and preferably longer Personalized prescription of medication Management of co-occurring mental health conditions, such as depression

38
ACS in Smokers Beyond short-term, acute-care measures, smoking-cessation treatment should be consistent with a chronic disease model, similar to management of other diseases, such as hypertension and diabetes. At present, the quit rates for smokers after myocardial infarction are higher than those for the general population of smokers, yet given the enormous health risks, still much too low.

40
Ευχαριστώ πολύ για την προσοχή σας

Παρόμοιες παρουσιάσεις











, Performance Indicators (PIs), Key Performance Indicators (KPIs)>")




. ΣΥΓΚΟΠΤΙΚΗ ΚΡΙΣΗ Αιφνίδια και σύντομη απώλεια συνείδησης που προκαλείται από ανεπαρκή εγκεφαλική αιμάτωση λόγω μειωμένης.>")


 ωφελέειν ή μη βλάπτειν ωφελέειν = θεραπευτική παρέμβαση μη βλάπτειν = ασφάλεια ασθενών.>")
