Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Η αντιμετώπιση της παχυσαρκίας (Νεώτερα δεδομένα) ΝΙΚΟΛΑΟΣ Λ ΚΑΤΣΙΛΑΜΠΡΟΣ
 ΝΙΚΟΛΑΟΣ Λ ΚΑΤΣΙΛΑΜΠΡΟΣ")
2
289 VAGUE Ph.

3
292

4
293

5
Ethnicity: Caucasian (Yudkin) vs Indian (Yajnik) 24 kg/m 2 20 kg/m 2 Body fat 9.1% 21.2%
 vs Indian (Yajnik) 24 kg/m 2 20 kg/m 2 Body fat 9.1% 21.2%")
6
299

7
Effects of 4 weight-loss diets differing in fat, protein and carbohydrate on fat mass and visceral adipose tissue, for 6 months (Results from the POUNDS LOST trial) R.J. de Souza et al, Am J Clin Nutr 2012; 95: 614-625 Body fat Abdominal fat Subcutaneous fat Fat loss (kg) -5-5 0 -3-3 -2-2 -1 -4-4 p<0.0001 vs. baseline p≥0.29 between diets p<0.0001 vs. baseline p≥0.29 between diets 4.2 2.3 1.5 0.9 Visceral fat Participants regained ≈40% of these losses by 2 years, with no differences between diets (p ≥ 0.23)
 p< vs. baseline p≥0.29 between diets p< vs. baseline p≥0.29 between diets Visceral fat Participants regained ≈40% of these losses by 2 years, with no differences between diets (p ≥ 0.23).")
8
Σχεδιασμός Διαιτητικού Σχήματος (1) Υπολογισμός Ενεργειακών Αναγκών: –RMR Χ 1,3 έως 1,7 –Νομογράμματα –Πίνακες
 Υπολογισμός Ενεργειακών Αναγκών: –RMR Χ 1,3 έως 1,7 –Νομογράμματα –Πίνακες")
9
Σχεδιασμός Διαιτητικού Σχήματος (2) Απλός κανόνας: 22 Kcal/Kg για διατήρηση Σ.Β Αν κατά 500kcal/ημέρα 0,5 Kg/εβδομάδα Με την πρόοδο της δίαιτας μειώνεται το αποτέλεσμα
 Απλός κανόνας: 22 Kcal/Kg για διατήρηση Σ.Β Αν κατά 500kcal/ημέρα 0,5 Kg/εβδομάδα Με την πρόοδο της δίαιτας μειώνεται το αποτέλεσμα")
10
Σχεδιασμός Διαιτητικού Σχήματος (3) 1200 Κcal/ημ : Γυναίκες 1500 Κcal/ημ : Άνδρες (Λαμβάνεται υπ’όψιν φύλο, αλλά όχι Σ.Β.)
 1200 Κcal/ημ : Γυναίκες 1500 Κcal/ημ : Άνδρες (Λαμβάνεται υπ’όψιν φύλο, αλλά όχι Σ.Β.)")
11
Χαρακτηριστικά “Συνηθισμένων” Διαιτών Απισχνάσεως (1) Υδατάνθρακες: –100 γρ ή περισσότερο »Εξοικονόμηση λευκωμάτων »Πρόληψη κετώσεως »Αποφυγή μεγάλων μεταβολών στο ισοζύγιο του ύδατος Πρωτεΐνες –Τουλάχιστον 0,8 γρ/Kg/ημέρα + 1,75 γρ υψηλής ποιότητας μικτής προελεύσεως πρωτεΐνης ανά 100 θερμίδες ενεργειακού ελλείμματος Λίπος: –30% ή < 30% των θερμίδων
 Υδατάνθρακες: –100 γρ ή περισσότερο »Εξοικονόμηση λευκωμάτων »Πρόληψη κετώσεως »Αποφυγή μεγάλων μεταβολών στο ισοζύγιο του ύδατος Πρωτεΐνες –Τουλάχιστον 0,8 γρ/Kg/ημέρα + 1,75 γρ υψηλής ποιότητας μικτής προελεύσεως πρωτεΐνης ανά 100 θερμίδες ενεργειακού ελλείμματος Λίπος: –30% ή < 30% των θερμίδων")
12
Χαρακτηριστικά “Συνηθισμένων” Διαιτών Απισχνάσεως (2) Οινόπνευμα: –Καθόλου ή ελάχιστο Βιταμίνες, μέταλλα, ηλεκτρολύτες: –Τουλάχιστον τις (RDA) –Αν <1200 Kcalσυμπληρώματα βιταμινών και μετάλλων Φυτικές ίνες: –20-30 γρ/ημέρα Χοληστερόλη –200 χιλ ή λιγότερο /ημέρα Νερό: –Τουλάχιστον 1 λίτρο /ημέρα ή 1 κ.εκ. ανά θερμίδα/ημέρα

13
PGMJ Online First, published on November 16, 2014 as 10.1136/postgradmedj-2014-133103 Healthy eating: an NHS priority A sure way to improve health outcomes for NHS staff and the public Aseem Malhotra, Mahiben Maruthappu, Terence Stephenson Adopting a Mediterranean diet after a myocardial infarction is almost three times as effective at reducing mortality than taking a statin.(18) A recent randomiszed study published in the Annals of Internal Medicine showed that an energy-unrestricted higher-fat and low-refined-carbohydrate diet (restricting carbohydrates without fibre) resulted in more weight loss and a better lipid profile than a low-fat diet at 1 year A recent longitudinal cohort study involving 175 countries showed that, for every additional c150 sugar-based kilocalories consumed daily (typical of a can of cola)compared with calories from another source, there was an 11-fold increase in the prevalence of developing type 2 diabetes independent of body mass index and physical activity levels.(14) it is estimated that increasing population consumption of fruit and vegetables by one portion per day and nut consumption by two servings a week would prevent 5.2 million deaths from cardiovascular disease globally within just 1 year. Να μην μετράμε μόνο τις θερμίδες – Ποιότητα Διατροφής

14
Very-low-calorie diet: a quick therapeutic tool to improve b cell function in morbidly obese patients with type 2 diabetes Ilaria Malandrucco et alAm J Clin Nutr 2012;95:609–13.

15
Η ΔΙΑΡΚΕΙΑ ΤΟΥ ΓΕΥΜΑΤΟΣ ΕΠΗΡΕΑΖΕΙ ΤΗ ΜΕΤΑΓΕΥΜΑΤΙΚΗ ΑΠΟΚΡΙΣΗ ΤΩΝ ΑΝΟΡΕΞΙΟΓΟΝΩΝ ΟΡΜΟΝΩΝ PYY ΚΑΙ GLP-1 ● Η κατανάλωση ενός γεύματος με βραδύ ρυθμό οδηγεί σε μεγαλύτερες μεταγευματικές συγκεντρώσεις των ανορεξιογόνων γαστρεντερικών ορμονών από την ταχεία κατανάλωση, ευοδώνοντας έτσι την επέλευση του κορεσμού Kokkinos A, le Roux CW, Alexiadou K, Tentolouris N, Vincent RP, Kyriaki D, Perrea D, Ghatei MA, Bloom SR, Katsilambros N, J Clin Endocrinol Metab October 2009 [Epub ahead of print]
![Η ΔΙΑΡΚΕΙΑ ΤΟΥ ΓΕΥΜΑΤΟΣ ΕΠΗΡΕΑΖΕΙ ΤΗ ΜΕΤΑΓΕΥΜΑΤΙΚΗ ΑΠΟΚΡΙΣΗ ΤΩΝ ΑΝΟΡΕΞΙΟΓΟΝΩΝ ΟΡΜΟΝΩΝ PYY ΚΑΙ GLP-1 ● Η κατανάλωση ενός γεύματος με βραδύ ρυθμό οδηγεί σε μεγαλύτερες μεταγευματικές συγκεντρώσεις των ανορεξιογόνων γαστρεντερικών ορμονών από την ταχεία κατανάλωση, ευοδώνοντας έτσι την επέλευση του κορεσμού Kokkinos A, le Roux CW, Alexiadou K, Tentolouris N, Vincent RP, Kyriaki D, Perrea D, Ghatei MA, Bloom SR, Katsilambros N, J Clin Endocrinol Metab October 2009 [Epub ahead of print]](http://images.slideplayer.gr/32/9803502/slides/slide_15.jpg "Η ΔΙΑΡΚΕΙΑ ΤΟΥ ΓΕΥΜΑΤΟΣ ΕΠΗΡΕΑΖΕΙ ΤΗ ΜΕΤΑΓΕΥΜΑΤΙΚΗ ΑΠΟΚΡΙΣΗ ΤΩΝ ΑΝΟΡΕΞΙΟΓΟΝΩΝ ΟΡΜΟΝΩΝ PYY ΚΑΙ GLP-1 ● Η κατανάλωση ενός γεύματος με βραδύ ρυθμό οδηγεί σε μεγαλύτερες μεταγευματικές συγκεντρώσεις των ανορεξιογόνων γαστρεντερικών ορμονών από την ταχεία κατανάλωση, ευοδώνοντας έτσι την επέλευση του κορεσμού Kokkinos A, le Roux CW, Alexiadou K, Tentolouris N, Vincent RP, Kyriaki D, Perrea D, Ghatei MA, Bloom SR, Katsilambros N, J Clin Endocrinol Metab October 2009 [Epub ahead of print]")
16
-4 -3 -2 0 1 2 3 4 5 6 036912 (Andersen et al. JAMA 1999;281:335) Weight change (kg) Time (months) Least active Middle active Most active Επαναπρόσληψη βάρους ανάλογα με το επίπεδο σωματικής δραστηριότητας
 Weight change (kg) Time (months) Least active Middle active Most active Επαναπρόσληψη βάρους ανάλογα με το επίπεδο σωματικής δραστηριότητας.")
17
Long-Term Persistence to Hormonal Adaptations to Weight Loss Sumithran P et al, N Engl J Med 2011;365:1597-1604 n=50 overweight/obese patients, no diabetes 10-week weight loss program very low energy diet (OPTIFAST) measurements at baseline, 10 and 62 weeks at 10 weeks stop diet circulating levels of: leptin, ghrelin, PYY, GIP, GLP-1, amylin, pancreatic polypeptide, cholecystokinin, insulin subjective ratings of hunger and appetite
 measurements at baseline, 10 and 62 weeks at 10 weeks stop diet circulating levels of: leptin, ghrelin, PYY, GIP, GLP-1, amylin, pancreatic polypeptide, cholecystokinin, insulin subjective ratings of hunger and appetite")
18
Postprandial responses of ghrelin, PYY, amylin and CCK at baseline and after weight loss

19
One year after initial weight reduction, levels of the circulating mediators of appetite that encourage weight regain, DO NOT REVERT to the levels recorded before weight loss. Long-term strategies to COUNTERACT this change may be needed to prevent obesity relapse. Conclusion

20
Ο ρόλος της άσκησης συνοψίζεται ως εξής : ● ● Το κύριο μέσο απώλειας βάρους είναι ο περιορισμός της πρόσληψης ενέργειας μέσω διαίτης ● ● Η φυσική δραστηριότητα είναι χρήσιμη επικουρική παρέμβαση και έχει σημαντικές ευνοϊκές επιδράσεις: - - Διατήρηση του ελεύθερου λίπους ιστού και της οστικής πυκνότητας - - Ανορεξιογόνο δράση - - Υποβοήθηση της διατήρησης του σωματικού βάρους - - Ψυχολογικές επιδράσεις - - Βιοχημικές (π.χ. στα λιπίδια) και άλλες (π.χ. Καρδιοαγγειακές αλλά και σημαντικές στον καρκίνο) ευνοϊκές επιδράσεις
 και άλλες (π.χ. Καρδιοαγγειακές αλλά και σημαντικές στον καρκίνο) ευνοϊκές επιδράσεις.")
21
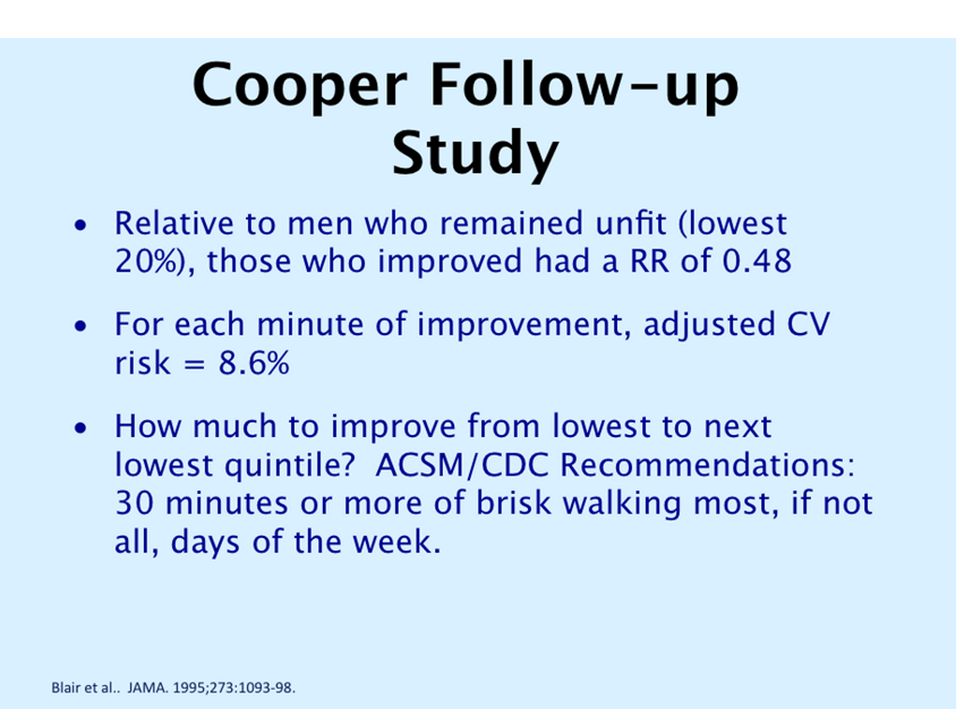
Methods: In a prospective study of 50,339 people, 13,449 had metabolic syndrome at baseline and were followed up for ten years to assess cause-specific mortality. The population was divided into two age groups: those younger than 65 years of age and those older than age 65. Information on their physical activity levels was collected at baseline.

23
ΦΑΡΜΑΚΕΥΤΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΤΗΣ ΠΑΧΥΣΑΡΚΙΑΣ: ΠΑΡΕΛΘΟΝ ● Πρώτο σκεύασμα: θυρεοειδική ορμόνη (1893) για προαγωγή θερμογενέσεως – Δε χρησιμοποιείται λόγω τοξικότητας Φάρμακο Πρώτη Εφαρμογή Μηχανισμός δράσεως Λόγος αποσύρσεως Δινιτροφαινόλη1933Θερμογένεση Βαριά τοξικότητα Αμφεταμίνες1936 Καταστολή πείνας, θερμογένεση Εξάρτηση, κατάχρηση, καρδιοαγγειακά συμβάματα Ανάλογα αμφεταμινών 1939, 1959, 1973 Καταστολή πείνας, θερμογένεση Υπέρταση, καρδιοπάθειες, εγκεφαλικά επεισόδια Aminorex1965 Καταστολή πείνας Πνευμονική υπέρταση Εφεδρίνη-καφεΐνη Δεκαετία 1970 Καταστολή πείνας, θερμογένεση Κυκλοφορεί ακόμη σε ορισμένες χώρες Μαζινδόλη Δεκαετία 1970 Καταστολή πείνας Εξάρτηση, κατάχρηση, καρδιοαγγειακά συμβάματα Φαινφλουραμίνη1963 Καταστολή πείνας Βαλβιδοπάθειες, πνευμονική υπέρταση Δεξφαινφλουραμίνη1985 Καταστολή πείνας Βαλβιδοπάθειες, πνευμονική υπέρταση Ioannides-Demos LL et al, Drugs 2005;65:1391-1418
 για προαγωγή θερμογενέσεως – Δε χρησιμοποιείται λόγω τοξικότητας Φάρμακο Πρώτη Εφαρμογή Μηχανισμός δράσεως Λόγος αποσύρσεως Δινιτροφαινόλη1933Θερμογένεση Βαριά τοξικότητα Αμφεταμίνες1936 Καταστολή πείνας, θερμογένεση Εξάρτηση, κατάχρηση, καρδιοαγγειακά συμβάματα Ανάλογα αμφεταμινών 1939, 1959, 1973 Καταστολή πείνας, θερμογένεση Υπέρταση, καρδιοπάθειες, εγκεφαλικά επεισόδια Aminorex1965 Καταστολή πείνας Πνευμονική υπέρταση Εφεδρίνη-καφεΐνη Δεκαετία 1970 Καταστολή πείνας, θερμογένεση Κυκλοφορεί ακόμη σε ορισμένες χώρες Μαζινδόλη Δεκαετία 1970 Καταστολή πείνας Εξάρτηση, κατάχρηση, καρδιοαγγειακά συμβάματα Φαινφλουραμίνη1963 Καταστολή πείνας Βαλβιδοπάθειες, πνευμονική υπέρταση Δεξφαινφλουραμίνη1985 Καταστολή πείνας Βαλβιδοπάθειες, πνευμονική υπέρταση Ioannides-Demos LL et al, Drugs 2005;65:")
24
ΑΠΟΤΕΛΕΣΜΑΤΙΚΟΤΗΤΑ ΤΗΣ ΟΡΛΙΣΤΑΤΗΣ: ΜΕΛΕΤΗ XENDOS ● Διπλή-τυφλή προοπτική τυχαιοποιημένη μελέτη με ορλιστάτη 120 mg ή placebo τρις/ημ + μεταβολή τρόπου ζωής ● 3305 ασθενείς με BMI ≥30 kg/m 2 και φυσιολογική (79%) ή διαταραγμένη (21%) ανοχή στη γλυκόζη (IGT) ● Μέση απώλεια βάρους 5.8 έναντι 3.0 kg ● Μείωση κινδύνου για εμφάνιση ΣΔ τύπου 2 κατά 37.3% (ιδιαίτερα στους ασθενείς με IGT – μείωση κατά 45.0%) Torgerson JS et al, Diabetes Care 2004;27:155-161
 ή διαταραγμένη (21%) ανοχή στη γλυκόζη (IGT) ● Μέση απώλεια βάρους 5.8 έναντι 3.0 kg ● Μείωση κινδύνου για εμφάνιση ΣΔ τύπου 2 κατά 37.3% (ιδιαίτερα στους ασθενείς με IGT – μείωση κατά 45.0%) Torgerson JS et al, Diabetes Care 2004;27:")
26
Current and Emerging Obesity Therapies Drug Brand name (developer) Stage of development Frequency and route of administra2on Mechanism of ac2on Efficacy * Safety and tolerability concerns Notes Phentermine + topiramate fixed dose combina.on Qsymia (Vivus) Approved July 2012 Once-‐daily oral Noradrenergic agent, an2epilep2c drug 9–10%Birth defect risk, minor eleva2on in heart rate FDA has requested ten post- ‐marke2ng studies and a cardiovascular outcomes trial Lorcaserin Belviq (Arena Approved June and Eisai)2012 Twice-‐daily oral Selec2ve serotonin receptor agonist 3–4% Possible risk of valvulopathy in obese type 2 diabe2cs FDA has requested six post- ‐marke2ng studies and a cardiovascular outcomes trial Bupropion + naltrexone fixed dose combina.on ContraveApproved (Orexigen and September Takeda)2014 Twice-‐daily oral Dopamine and norepinephrine reuptake inhibitor, opioid receptor antagonist 4–5% Minor increase in heart rate and blood pressure Undergoing 10,000 pa2ent FDA- ‐mandated pre-‐marke2ng cardiovascular outcomes trial; Liraglu2de* Victoza ‡ (Novo Nordisk) Phase III ¶ Once- ‐daily injectable Glucagon- ‐like pep2de 1 analogue 5–6% Nausea, hypoglycemia, risk for pancrea22s A lower dose formula2on is on the market for type 2 diabetes Recommended for FDA Approval September 2014 * Mean placebo-‐adjusted weight loss demonstrated in clinical studies. ‡ LiragluRde is marketed as Victoza for type 2 diabetes. ¶ LiragluRde was approved in Europe and in the United States in 2009 and 2010, respecRvely, as a treatment for type 2 diabetes. Recommended for FDA Approval September 2014. Wong et al. Nat Rev Drug Discov. 2012;11:669-‐70. 8

27
Agent Brand Name Drug (kg) Placebo (kg) Net Weight Loss (kg) Duration FDA Approval Topiramate/ phentermine Qsymia10.51.88.7 104 weeks July 2012 Lorcaserin Belviq8.23.4 4.8 52 weeks June 2012 Bupropion / naltrexone Contrave8.21.96.248 weeks Sept. 2014 Liraglu2de* 3.0 mg Victoza10.34.16.2 104 weeks Pending Recommende d for Approval September 2014 Expected Weight Loss with Newly Approved and Investigational And-‐Obesity Medications Powell et al. Clin Pharmacol Ther. 2011;90:40- ‐51. *Not FDA Approved. Recommended for FDA Approval September 2014 15

28
FINDINGS Obesity medications approved for long-term use, when prescribed with lifestyle interventions, produce additional weight loss relative to placebo ranging from approximately 3%of initial weight for orlistat and lorcaserin to 9% for top-dose (15/92 mg) phentermine plus topiramate–extended release at 1 year. The proportion of patients achieving clinically meaningful (at least 5%) weight loss ranges from 37%to 47%for lorcaserin, 35%to 73%for orlistat, and 67%to 70% for top-dose phentermine plus topiramate–extended release. All 3 medications produce greater improvements in many cardiometabolic risk factors than placebo, but no obesity medication has been shown to reduce cardiovascular morbidity or mortality. Most prescriptions are for noradrenergic medications, despite their approval only for short-term use and limited data for their long-term safety and efficacy. CONCLUSIONS AND RELEVANCE Medications approved for long-term obesity treatment, when used as an adjunct to lifestyle intervention, lead to greater mean weight loss and an increased likelihood of achieving clinically meaningful 1-year weight loss relative to placebo. By discontinuing medication in patients who do not respond with weight loss of at least 5%, clinicians can decrease their patients’ exposure to the risks and costs of drug treatment when there is little prospect of long-term benefit. ΦΑΡΜΑΚΑ – ΣΥΓΧΡΟΝΕΣ ΑΠΟΨΕΙΣ Long-term Drug Treatment for Obesity A Systematic and Clinical Review Susan Z. Yanovski, MD; Jack A. Yanovski, MD, PhD JAMA. doi:10.1001/jama.2013.281361 Published online November 14, 2013.
 weight loss ranges from 37%to 47%for lorcaserin, 35%to 73%for orlistat, and 67%to 70% for top-dose phentermine plus topiramate–extended release. All 3 medications produce greater improvements in many cardiometabolic risk factors than placebo, but no obesity medication has been shown to reduce cardiovascular morbidity or mortality. Most prescriptions are for noradrenergic medications, despite their approval only for short-term use and limited data for their long-term safety and efficacy. CONCLUSIONS AND RELEVANCE Medications approved for long-term obesity treatment, when used as an adjunct to lifestyle intervention, lead to greater mean weight loss and an increased likelihood of achieving clinically meaningful 1-year weight loss relative to placebo. By discontinuing medication in patients who do not respond with weight loss of at least 5%, clinicians can decrease their patients’ exposure to the risks and costs of drug treatment when there is little prospect of long-term benefit. ΦΑΡΜΑΚΑ – ΣΥΓΧΡΟΝΕΣ ΑΠΟΨΕΙΣ Long-term Drug Treatment for Obesity A Systematic and Clinical Review Susan Z. Yanovski, MD; Jack A. Yanovski, MD, PhD JAMA. doi: /jama Published online November 14,")
29
Figure 1: Three-dimensional reconstruction of iBAT in a human infant. (a–c) The volume- rendered data set is shown in the sagittal (a), coronal (b) and axial (c) planes. The iBAT is green. Scale bars, 5 cm
 The volume- rendered data set is shown in the sagittal (a), coronal (b) and axial (c) planes. The iBAT is green. Scale bars, 5 cm.")
30
Evidence for two types of brown adipose tissue in humans, Nature Med, On line 21 April 2013, Lidell ME The previously observed supraclavicular depot of brown adipose tissue (BAT) in adult humans was commonly believed to be the equivalent of the interscapular thermogenic organ of small mammals. This view was recently disputed 1 on the basis of the demonstration that this depot consists of beige (also called brite) brown adipocytes, a newly identified type of brown adipocyte that is distinct from the classical brown adipocytes that make up the interscapular thermogenic organs of other mammals. A combination of high-resolution imaging techniques and histological and biochemical analyses showed evidence for an anatomically distinguishable interscapular BAT (iBAT) depot in human infants that consists of classical brown adipocytes, a cell type that has so far not been shown to exist in humans. On the basis of these findings, we conclude that infants, similarly to rodents, have the bona fide iBAT thermogenic organ consisting of classical brown adipocytes that is essential for the survival of small mammals in a cold environment 1
 brown adipocytes, a newly identified type of brown adipocyte that is distinct from the classical brown adipocytes that make up the interscapular thermogenic organs of other mammals. A combination of high-resolution imaging techniques and histological and biochemical analyses showed evidence for an anatomically distinguishable interscapular BAT (iBAT) depot in human infants that consists of classical brown adipocytes, a cell type that has so far not been shown to exist in humans. On the basis of these findings, we conclude that infants, similarly to rodents, have the bona fide iBAT thermogenic organ consisting of classical brown adipocytes that is essential for the survival of small mammals in a cold environment 1.")
31
Μυϊκή άσκηση έκφραση PGC1-α στον σκελετικό μυ έκφραση μεμβρανικής πρωτεΐνης FNDC5 στα μυϊκά κύτταρα Ιριζίνη (μυοκίνη) = ορμόνη της άσκησης + διάσπαση και απελευθέρωση στην κυκλοφορία του αίματος + λιποκύτταρα λευκού λιπώδους ιστού έκφραση UCP-1 χαρακτηριστικά φαιού λίπους Pontus Bostro et al, Nature doi:10.1038/nature10777
 = ορμόνη της άσκησης + διάσπαση και απελευθέρωση στην κυκλοφορία του αίματος + λιποκύτταρα λευκού λιπώδους ιστού έκφραση UCP-1 χαρακτηριστικά φαιού λίπους Pontus Bostro et al, Nature doi: /nature10777")
32
White-to-brown metabolic conversion of human adipocytes by JAK inhibition Moisan A et al Nature Cell Biology (2014) doi:10.1038/ncb3075 Received 13 May 2014 Accepted 31 October 2014 Published online 08 December 2014 We identified two inhibitors of Janus kinase (JAK) activity with no precedent in adipose tissue biology that stably confer brown-like metabolic activity to white adipocytes. Importantly, these metabolically converted adipocytes exhibit elevated UCP1 expression and increased mitochondrial activity

35
Haider A, Yassin A, Doros G, et al. Reductions of weight and waist size in 362 hypogonadal men with obesity grades I to III under long-term treatment with testosterone undecanoate (TU): observational data from two registry studies. Endocr Rev 2014; 35:SUN-0895.
: observational data from two registry studies. Endocr Rev 2014; 35:SUN")
36
ΚΡΙΤΗΡΙΑ ΓΙΑ ΒΑΡΙΑΤΡΙΚΗ ΧΕΙΡΟΥΡΓΙΚΗ ● ● ΒΜΙ≥40 kg/m 2 ή ΒΜΙ ≥35 kg/m 2 με σημαντικές συνυπάρχουσες νοσηρές καταστάσεις σχετιζόμενες με την παχυσαρκία ● ● Ηλικία μεταξύ 16 και 65 ετών ● ● Αποδεκτοί χειρουργικοί κίνδυνοι ● ● Στοιχειοθετημένη αποτυχία μη χειρουργικών προσεγγίσεων για μακροχρόνια απώλεια βάρους ● ● Ψυχολογικά ισορροπημένος ασθενής με ρεαλιστικές προσδοκίες ● ● Ασθενής με επαρκή πληροφόρηση και κίνητρα ● ● Δέσμευση για παρατεταμένες μεταβολές του τρόπου ζωής ● ● Επίλυση προβλημάτων καταχρήσεως ουσιών ή οινοπνεύματος ● ● Απουσία ενεργού σχιζοφρένειας και μη θεραπευομένης σοβαρής καταθλίψεως Από: Schneider BE et al, Diabetes Care 2005; 28: 475-480

37
Steinbrook, R. N Engl J Med 2004;350:1075-1079 ΟΙ ΠΙΟ ΣΥΧΝΕΣ ΒΑΡΙΑΤΡΙΚΕΣ ΕΠΕΜΒΑΣΕΙΣ

38
ΕΠΙΜΗΚΗΣ ΓΑΣΤΡΕΚΤΟΜΗ «ΣΑΝ ΜΑΝΙΚΙ» (SLEEVE GASTRECTOMY)
")
39
Mean Percent Weight Change during a 15-Year Period in the Control Group and the Surgery Group,According to the Method of Bariatric Surgery. Sjöström L et al. N Engl J Med 2007; 357:741-52.

40
n engl j med 357;8 www.nejm.org august 23, 2007 (MORTALITY, SOS STUDY)
")
41
Ενδείξεις βαριατρικής επέμβασης σε άτομα με ΣΔ τύπου 2. Ενδείξεις – ΒΜΙ >35 – Σχετικά πρόσφατη έναρξη ΣΔ (<5 έτη) – Νέα άτομα (<60 ετών) – Αποδεκτός χειρουργικός κίνδυνος – Υψηλό κίνητρο. – Αποτυχημένες προσπάθειες απώλειας με συντηρητικό τρόπο. Αντενδείξεις – Στεφανιαία νόσος – Αλκοολισμός ή διατροφικές διαταραχές – Εγκατεστημένη νεφροπάθεια – Έλλειψη κινήτρου και κοινωνικής υποστήριξης
 – Νέα άτομα (<60 ετών) – Αποδεκτός χειρουργικός κίνδυνος – Υψηλό κίνητρο. – Αποτυχημένες προσπάθειες απώλειας με συντηρητικό τρόπο. Αντενδείξεις – Στεφανιαία νόσος – Αλκοολισμός ή διατροφικές διαταραχές – Εγκατεστημένη νεφροπάθεια – Έλλειψη κινήτρου και κοινωνικής υποστήριξης.")
42
Υπόθεση εγγύς ΓΕΣ Η παράκαμψη τμήματος του εγγύς τμήματος γαστρεντερικού σωλήνα κατά τη διέλευση της τροφής έχει ως αποτέλεσμα αποφυγή έκκρισης παραγόντων που ελαττώνουν την έκκριση της ινσουλίνης ή προάγουν την ινσουλινοαντίσταση (Φαινόμενο αντι-ινκρετίνης) Υπόθεση άπω ΓΕΣ Η γρήγορη διέλευση της τροφής – λόγω παράκαμψης τμήματος του γαστρεντερικού σωλήνα – οδηγεί σε διέγερση L κυττάρων, με αποτέλεσμα την αυξημένη έκκριση ινσουλινοεκκριτικών ορμονών (GLP-1) (Φαινόμενο ινκρετίνης) Πιθανοί νευροενδοκρινικοί μηχανισμοί υποστροφής του ΣΔ Μετά από βαριατρική επέμβαση γαστρικής παράκαμψης
 Υπόθεση άπω ΓΕΣ Η γρήγορη διέλευση της τροφής – λόγω παράκαμψης τμήματος του γαστρεντερικού σωλήνα – οδηγεί σε διέγερση L κυττάρων, με αποτέλεσμα την αυξημένη έκκριση ινσουλινοεκκριτικών ορμονών (GLP-1) (Φαινόμενο ινκρετίνης) Πιθανοί νευροενδοκρινικοί μηχανισμοί υποστροφής του ΣΔ Μετά από βαριατρική επέμβαση γαστρικής παράκαμψης")
43
Multiple Actions of GLP-1 Act to Reduce Hyperglycaemia GLP-1 has multiple actions that reduce hyperglycaemia, including: – Glucose-dependent stimulation of insulin secretion – Glucose-dependent suppression of glucagon secretion – Slowing of gastric emptying – Improvement in β-cell function – Increase in β-cell mass, function, and islet neogenesis (animal studies) In addition, GLP-1 has been associated with reduced food intake and reductions in body weight Drucker DJ. Diabetes Care. 2003;26:2929-2940.

46
Overall, 68.2 % (95 % confidence interval [CI], 66 and 70 %) experienced an initial complete diabetes remission within 5 years after surgery. Among these, 35.1 % (95 % CI, 32 and 38 %) redeveloped diabetes within 5 years. The median duration of remission was 8.3 years. Significant predictors of complete remission and relapse were poor preoperative glycemic control, insulin use, and longer diabetes duration. Άρα αρχικά 1/3 όχι ανταπόκριση και στο 1/3 αυτών που αρχικά παρουσίασαν ύφεση του ΣΔ σημειώθηκε υποτροπή Όμως η αλήθεια έχει και άλλη όψη
![Overall, 68.2 % (95 % confidence interval [CI], 66 and 70 %) experienced an initial complete diabetes remission within 5 years after surgery.](http://images.slideplayer.gr/32/9803502/slides/slide_46.jpg "Among these, 35.1 % (95 % CI, 32 and 38 %) redeveloped diabetes within 5 years. The median duration of remission was 8.3 years. Significant predictors of complete remission and relapse were poor preoperative glycemic control, insulin use, and longer diabetes duration. Άρα αρχικά 1/3 όχι ανταπόκριση και στο 1/3 αυτών που αρχικά παρουσίασαν ύφεση του ΣΔ σημειώθηκε υποτροπή Όμως η αλήθεια έχει και άλλη όψη.")
47
Bariatric Surgery and Prevention of Type 2 Diabetes in Swedish Obese Subjects NEJM, Aug 23, 2012, Carlsson LMS et al

48
Cumulative incidence of fatal and total cardiovascular events (myocardial infarction + stroke) in the control and surgery groups of the Swedish Obese Subjects study. LARS SJÖSTRÖM, 20 Sept 2012

49
GASTRIC BYPASS INDUCES A MORE PRONOUNCED IMPROVEMENT IN POSTPRANDIAL GLUCOSE AND TRIGLYCERIDE LEVELS THAN SLEEVE GASTRECTOMY Alexander Kokkinos, Kleopatra Alexiadou, Nicholas Tentolouris, Nicholas Katsilambros First Department of Propaedeutic Medicine, Athens University Medical School, Laiko General Hospital, Athens, Greece EASD Nutrition Study Group Meeting Rome 2011

50
OBES SURG (2013) 23:31–38 DOI 10.1007/s11695-012-0743-8 Improvement in Cardiovascular Indices After Roux-en-Y Gastric Bypass or Sleeve Gastrectomy for Morbid Obesity Alexander Kokkinos & Kleopatra Alexiadou & Christos Liaskos & Georgia Argyrakopoulou & Ioanna Balla & Nicholas Tentolouris & Ioannis Moyssakis & Nicholas Katsilambros & Irene Vafiadis & Andreas Alexandrou & Theodoros Diamantis
 23:31–38 DOI /s Improvement in Cardiovascular Indices After Roux-en-Y Gastric Bypass or Sleeve Gastrectomy for Morbid Obesity Alexander Kokkinos & Kleopatra Alexiadou & Christos Liaskos & Georgia Argyrakopoulou & Ioanna Balla & Nicholas Tentolouris & Ioannis Moyssakis & Nicholas Katsilambros & Irene Vafiadis & Andreas Alexandrou & Theodoros Diamantis")
51
μεταγευματική υπογλυκαιμία = επιπλοκή χειρουργείου γαστρικής παράκαμψης σοβαρά νευρογλυκοπενικά συμπτώματα = απώλεια συνείδησης, επιληπτικές κρίσεις, τροχαία ατυχήματα θεραπεία: ακαρβόζη, ανάλογα σωματοστατίνης, διαζοξείδη ??? συμπτώματα υπογλυκαιμίας 2-3 ώρες μετά φαγητό εμφάνιση διαταραχής 2-3 χρόνια μετά γαστρική παράκαμψη Μηχανισμοί μετά από γαστρική παράκαμψη... αύξηση κατά 10 φορές των μεταγευματικών συγκεντρώσεων των ινκρετινών GLP-1 και GIP παράκαμψη 12-δακτύλου, ταχεία διάβαση τροφών στο άπω λεπτό έντερο, άνοδος κυκλοφορούντων χολικών οξέων, νευροορμονικοί μηχανισμοί Hypoglycaemia after gastric bypass surgery: diabetes remission in the extreme???

52
Arterial baroreflex sensitivity (BRS) in lean and obese women after glucose ingestion M. Horianopoulou, S. Liatis, D. Perea, N. Tsokos, A. Petsas, I. Skrapari, C. Tsigos, N. Katsilambros Obes Rev 2005;6(Suppl 1):67
:67.")
53
Effect of weight loss on baroreflex sensitivity of women with morbid obesity. BRS BRS prior to gastric bypass 2 months post gastric bypass (mean BMI=49.08) (mean BMI=37.88) 8.97 19.87 Skrapari ISkrapari I, Tentolouris N, Perrea D, Bakoyiannis C, Papazafiropoulou A, Katsilambros NTentolouris NPerrea DBakoyiannis CPapazafiropoulou A Katsilambros N Obesity (Silver Spring). 2007 Jul;15(7):1685-93
 (mean BMI=37.88) Skrapari ISkrapari I, Tentolouris N, Perrea D, Bakoyiannis C, Papazafiropoulou A, Katsilambros NTentolouris NPerrea DBakoyiannis CPapazafiropoulou A Katsilambros N Obesity (Silver Spring) Jul;15(7):")
54
ECO 2012 DIFFERENCES IN ENERGY EXPENDITURE, FAT MASS AND APPETITE SUPPRESSION AFTER GASTRIC BYPASS AND SLEEVE GASTRECTOMY FOR MORBID OBESITY Liaskos C 1, Alexiadou K 1, Tentolouris N 1, Balla I 1, Argyrakopoulou G 1, Alexandrou A 2, Diamantis T 2, Katsilambros N 1, Kokkinos A 1

55
Conclusion: Roux-en-Y gastric bypass and sleeve gastrectomy lead to significant and comparable weight loss, decrease in energy expenditure, fat mass, and hunger, as well as an increase in satiety.

56
Θνητότης ανάλογα με την εμπειρία των κέντρων

57
Review of the key results from the Swedish Obese Subjects (SOS) trial: a prospective controlled intervention study of bariatric surgery LARS SJÖSTRÖM, doi: 10.1111/joim.12012 © 2012 The Association for the Publication of the Journal of Internal Medicine BMI does not predict the effects of surgical treatment on outcomes All current guidelines for bariatric surgery in obese individuals without [84-86] and with diabetes [72-75] are based on BMI alone or in combination with other criteria……………….. the value of BMI as a predictor of treatment effect does not seem to have been evaluated except in the SOS study……………….. BMI did thus not predict the effect of surgery on any of these endpoints By contrast, insulin predicted the treatment effect with respect to mortality (P for interaction=0.013) [35], cardiovascular events (P<0.001) [37] and incidence of diabetes (P=0.007) [38] (data not shown). There was also a strong impaired fasting glucose–treatment interaction with respect to diabetes incidence (p=0.002)[38]. These findings suggest that guidelines for bariatric surgery need to be modified. In order to select those patients who are most likely to benefit from surgery, more importance should be given to metabolic variables and less to BMI.
![Review of the key results from the Swedish Obese Subjects (SOS) trial: a prospective controlled intervention study of bariatric surgery LARS SJÖSTRÖM, doi: /joim © 2012 The Association for the Publication of the Journal of Internal Medicine BMI does not predict the effects of surgical treatment on outcomes All current guidelines for bariatric surgery in obese individuals without [84-86] and with diabetes [72-75] are based on BMI alone or in combination with other criteria………………..](http://images.slideplayer.gr/32/9803502/slides/slide_57.jpg "the value of BMI as a predictor of treatment effect does not seem to have been evaluated except in the SOS study……………….. BMI did thus not predict the effect of surgery on any of these endpoints By contrast, insulin predicted the treatment effect with respect to mortality (P for interaction=0.013) [35], cardiovascular events (P<0.001) [37] and incidence of diabetes (P=0.007) [38] (data not shown). There was also a strong impaired fasting glucose–treatment interaction with respect to diabetes incidence (p=0.002)[38]. These findings suggest that guidelines for bariatric surgery need to be modified. In order to select those patients who are most likely to benefit from surgery, more importance should be given to metabolic variables and less to BMI..")
58
Η οριστική λύση για την παχυσαρκία! Ο κομήτης 67Ρ 150Kg 1,5g

Παρόμοιες παρουσιάσεις














 ωφελέειν ή μη βλάπτειν ωφελέειν = θεραπευτική παρέμβαση μη βλάπτειν = ασφάλεια ασθενών.>")






