Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Από τη Βιολογία του Οστικού Μεταβολισμού στη Θεραπευτική της Οστικής Νόσου των Κακοηθειών και της Οστεοπόρωσης Eυάγγελος Τέρπος, Αιματολόγος

2
Αιμοποιητικά Κύτταρα και Κύτταρα του Οστού: Στενή Διασύνδεση

3
Τα κύτταρα του οστού

4
Walsh et al, Annu Rev Immunol 2006;24:2.1

5
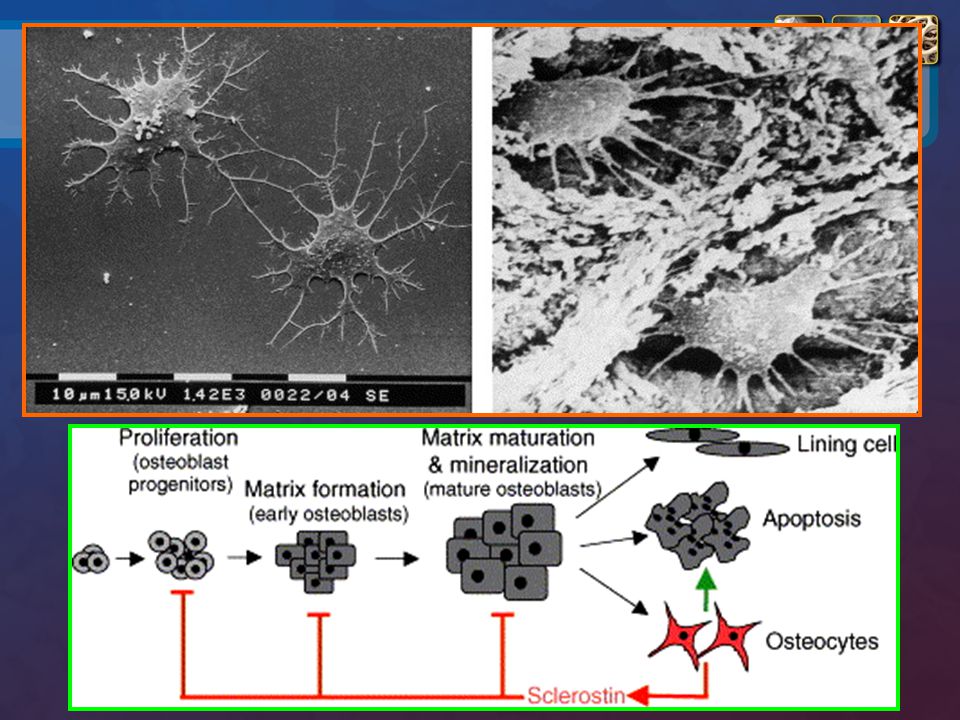
Φυσιολογία του Οστικού Μεταβολισμού
Seeman E, et al. N Engl J Med. 2006;354(21): van Bezooijen RL, et al. Cytokine Growth Factor Rev. 2005;16(3):
: van Bezooijen RL, et al. Cytokine Growth Factor Rev. 2005;16(3):")
6
Wnt Signaling και Οστεοβλάστες
Piters E, et al. Arch Biochem Biophys. 2008;473:112-6.

10
Οστικός μεταβολισμός και RANKL
CFU-M Πρόδρομος οστεοκλάστης Αυξητικοί παράγοντες Ορμόνες Κυτταροκίνες Πολυπύρηνος οστεοκλάστης In the presence of low levels of macrophage colony-stimulating factor (M-CSF), Receptor Activator of Nuclear Factor-kappa B (RANK) Ligand is essential for osteoclast formation, function, and survival.1-4 Osteoclasts are the cells responsible for resorbing bone. Many different factors (eg, PTH, TNF, IL-1) can lead to bone loss, but they all stimulate the expression of RANK Ligand by osteoblasts and other cells (eg, activated T cells). Maturation of pre-fusion osteoclasts to multinucleated osteoclasts and finally to activated osteoclasts is initiated when RANK Ligand binds to RANK on the preosteoclast and mature osteoclast.5 In addition to being expressed on osteoclasts and osteoclast progenitors, RANK has been observed on cartilage cells (chondrocytes), mammary gland epithelial cells, and trophoblast cells.6,7 The RANK Ligand polypeptide is a type II transmembrane protein found on the surface of expressing cells as well as in a proteolytically released (cleaved) soluble form.3 1. Yasuda H, et al. Osteoclast Differentiation Factor is a Ligand for Osteoprotegerin Osteoclastogenesis-inhibitory Factor and is Identical to Trance/RANKL. Proc Natl Acad Sci Usa. 1998;95:3597–602. 2. Fuller K, et al. TRANCE is Necessary and Sufficient for Osteoblast-mediated Activation of Bone Resorption in Osteoclasts. J Exp Med. 1998;188:997–1001. 3. Lacey DL, et al. Osteoprotegerin Ligand is a Cytokine That Regulates Osteoclast Differentiation and Activation. Cell. 1998;93:165–76. 4. Lacey DL, et al. Osteoprotegerin Ligand Modulates Murine Osteoclast Survival in Vitro and in Vivo. Am J Pathol. 2000;157: 5. Boyle WJ, et al. Osteoclast Differentiation and Activation. Nature. 2003;423: 6. Fata JE, et al. The Osteoclast Differentiation Factor Osteoprotegerin-ligand is Essential for Mammary Gland Development. Cell :103:41-50. 7. Hsu H, et al. Tumor Necrosis Factor Receptor Family Member RANK Mediates Osteoclast Differentiation and Activation Induced by Osteoprotegerin Ligand. Proc Natl Acad Sci. 1999:96: Ώριμος οστεοκλάστης Οστεοβλάστες Οστούν CFU-M = colony forming unit macrophage Boyle et al, Nature 2003;423:337-42
, Receptor Activator of Nuclear Factor-kappa B (RANK) Ligand is essential for osteoclast formation, function, and survival.1-4 Osteoclasts are the cells responsible for resorbing bone. Many different factors (eg, PTH, TNF, IL-1) can lead to bone loss, but they all stimulate the expression of RANK Ligand by osteoblasts and other cells (eg, activated T cells). Maturation of pre-fusion osteoclasts to multinucleated osteoclasts and finally to activated osteoclasts is initiated when RANK Ligand binds to RANK on the preosteoclast and mature osteoclast.5 In addition to being expressed on osteoclasts and osteoclast progenitors, RANK has been observed on cartilage cells (chondrocytes), mammary gland epithelial cells, and trophoblast cells.6,7 The RANK Ligand polypeptide is a type II transmembrane protein found on the surface of expressing cells as well as in a proteolytically released (cleaved) soluble form Yasuda H, et al. Osteoclast Differentiation Factor is a Ligand for Osteoprotegerin Osteoclastogenesis-inhibitory Factor and is Identical to Trance/RANKL. Proc Natl Acad Sci Usa. 1998;95:3597– Fuller K, et al. TRANCE is Necessary and Sufficient for Osteoblast-mediated Activation of Bone Resorption in Osteoclasts. J Exp Med. 1998;188:997– Lacey DL, et al. Osteoprotegerin Ligand is a Cytokine That Regulates Osteoclast Differentiation and Activation. Cell. 1998;93:165– Lacey DL, et al. Osteoprotegerin Ligand Modulates Murine Osteoclast Survival in Vitro and in Vivo. Am J Pathol. 2000;157: Boyle WJ, et al. Osteoclast Differentiation and Activation. Nature. 2003;423: Fata JE, et al. The Osteoclast Differentiation Factor Osteoprotegerin-ligand is Essential for Mammary Gland Development. Cell. 2000:103: Hsu H, et al. Tumor Necrosis Factor Receptor Family Member RANK Mediates Osteoclast Differentiation and Activation Induced by Osteoprotegerin Ligand. Proc Natl Acad Sci. 1999:96: Ώριμος. οστεοκλάστης. Οστεοβλάστες. Οστούν. CFU-M = colony forming unit macrophage. Boyle et al, Nature 2003;423:")
11
Οστεοσκλήρυνση σε έλλειψη RANKL
Προκλινικά μοντέλα ποντικιών Here is a mouse RANK Ligand knockout model as a surrogate for dosing of Denosumab. This mouse study shows increased bone density by removing RANK Ligand. Φυσιολογικό RANKL knockout

12
Oστεοπροτεγερίνη (OPG): ανασταλτής του RANKL
CFU-M RANK OPG Πρόδρομος οστεοκλάστης Αυξητικοί παράγοντες Ορμόνες Κυτταροκίνες Πολυπύρηνος οστεοκλάστης Ώριμος οστεοκλάστης Οστεοβλάστες

13
OPG: Πειράματα σε knock-out ποντίκια
* OPG +/+ OPG +/- OPG -/- 50 40 30 20 10 -10 BV%TV K Bucay et al; Genes Dev 1998;12:1260

14
Η σχέση μεταξύ RANKL/OPG οδηγεί την οστεοκλαστική δραστηριότητα
RANK Ligand OPG Σταματά τη δράση των OCs Προάγει την ενεργοποίηση των OCs Οστεοκλαστική δραστηριότητα OC = οστεοκλάστης The relative balance between RANK Ligand and OPG is regulated by cytokines and hormones and determines osteoclast activity. Alterations of the RANK Ligand/OPG ratio are critical in the pathogenesis of bone diseases that result in increased bone resorption. Unopposed RANK Ligand (i.e., an elevated RANK Ligand/OPG ratio) within the skeleton promotes bone loss, while restoring a balanced RANK Ligand/OPG ratio or inhibiting RANK Ligand decreases osteoclast activation and bone resorption. In many diseases involving increased bone resorption, RANK Ligand expression is upregulated by osteoclastogenic factors (growth factors, hormones, cytokines) while OPG expression is simultaneously downregulated.1-3 Hofbauer LC, et al. Clinical implications of the osteoprotegerin/RANKL/RANK system for bone and vascular diseases. JAMA. 2004;292:490-5. Lacey DL, et al. Osteoprotegerin Ligand is a Cytokine that Regulates Osteoclast Differentiation and Activation. Cell. 1998;93:165–76 Boyle WJ, et al. Osteoclast Differentiation and Activation. Nature. 2003;423: Hofbauer et al, JAMA 2004;292:490-5. Lacey et al, Cell 1998;93: Boyle et al, Nature 2003;423:
 within the skeleton promotes bone loss, while restoring a balanced RANK Ligand/OPG ratio or inhibiting RANK Ligand decreases osteoclast activation and bone resorption. In many diseases involving increased bone resorption, RANK Ligand expression is upregulated by osteoclastogenic factors (growth factors, hormones, cytokines) while OPG expression is simultaneously downregulated.1-3. Hofbauer LC, et al. Clinical implications of the osteoprotegerin/RANKL/RANK system for bone and vascular diseases. JAMA. 2004;292: Lacey DL, et al. Osteoprotegerin Ligand is a Cytokine that Regulates Osteoclast Differentiation and Activation. Cell. 1998;93:165–76. Boyle WJ, et al. Osteoclast Differentiation and Activation. Nature. 2003;423: Hofbauer et al, JAMA 2004;292: Lacey et al, Cell 1998;93: Boyle et al, Nature 2003;423:")
15
Μεταστατική Οστική Νόσος
5-ετής παγκόσμια επίπτωση σε χιλιάδες1 Συχνότητα οστικών μεταστάσεων στον καρκίνο2 Διάμεση επιβίωση, Mήνες2-4 Mυέλωμα 144 38-84 Ca νεφρού 480 12-24 Mελάνωμα 533 6 Ca κύστης 1.000 40 6 - 9 Περισσότερο βλαστικές Περισσότερο λυτικές Ca θυρεοειδούς 475 60 48 Incidence of bone metastases in cancers High incidence of bone metastases sets the stage for skeletal complications A wide range of cancer types is associated with a high incidence of skeletal involvement, and the resulting lesions vary in radiographic appearance across a continuum from osteolytic to osteoblastic Approximately 80% of patients with multiple myeloma have radiographic evidence of predominantly osteolytic bone destruction The prevalence (number of cases worldwide during a 5-year period) of bone metastases is greatest in breast and prostate cancer, reflecting both the high incidence and the relatively long clinical courses of these tumors.1 These 2 cancers probably account for more than 80% of cases of metastatic bone disease. Bone metastases associated with breast cancer are typically a mixture of osteolytic, mixed, and osteoblastic lesions, whereas prostate carcinoma is usually associated with sclerotic (osteoblastic) lesions Bone metastases cause considerable morbidity—including pain, impaired mobility, pathologic fracture, spinal-cord or nerve-root compression, and hypercalcemia of malignancy (HCM)2 References Ferlay J, Bray F, Pisani P, Parkin DM. IARC Globocon Cancer Incidence, Mortality, and Prevalence. Coleman RE. Skeletal complications of malignancy. Cancer. 1997;80: Ca πνεύμονος 1.394 6 - 7 Ca μαστού 3.860 40-65 Ca προστάτη 1.555 35-60 Ferlay J, et al. IARC Globocan Cancer Incidence, Mortality, and Prevalence. 2. Coleman RE. Cancer Treat Rev. 2001;27: Coleman RE. Cancer. 1997;80: Zekri J et al. Int J Oncol. 2001;19:
 of bone metastases is greatest in breast and prostate cancer, reflecting both the high incidence and the relatively long clinical courses of these tumors.1 These 2 cancers probably account for more than 80% of cases of metastatic bone disease. Bone metastases associated with breast cancer are typically a mixture of osteolytic, mixed, and osteoblastic lesions, whereas prostate carcinoma is usually associated with sclerotic (osteoblastic) lesions. Bone metastases cause considerable morbidity—including pain, impaired mobility, pathologic fracture, spinal-cord or nerve-root compression, and hypercalcemia of malignancy (HCM)2. References. Ferlay J, Bray F, Pisani P, Parkin DM. IARC Globocon Cancer Incidence, Mortality, and Prevalence. Coleman RE. Skeletal complications of malignancy. Cancer. 1997;80: Ca πνεύμονος Ca μαστού Ca προστάτη Ferlay J, et al. IARC Globocan Cancer Incidence, Mortality, and Prevalence. 2. Coleman RE. Cancer Treat Rev. 2001;27: Coleman RE. Cancer. 1997;80: Zekri J et al. Int J Oncol. 2001;19:")
16
Συμπαγείς Όγκοι-Οστικές Μεταστάσεις: Παθοφυσιολογία (1)
Mundy GR, Nat Rev Cancer 2002;584:71

17
Συμπαγείς Όγκοι-Οστικές Μεταστάσεις: Παθοφυσιολογία (2)
Mundy GR, Nat Rev Cancer 2002;584:71

18
Ο βιολογικός δρόμος RANK/RANKL/OPG
Hofbauer et al; Cancer 2001;92:460

19
sRANKL/OPG στον ορό ασθενών με οστικές μεταστάσεις
CONTROL PROSTATE BREAST LUNG 120 100 80 60 40 20 p=0.005 p=0.014 p=0.08 sRANKL/OPG Mountzios et al. Αcta Oncol 2007;46:221-9

20
Πολλαπλούν Μυέλωμα Το πολλαπλούν μυέλωμα χαρακτηρίζεται από τον μονοκλωνικό πολλαπλασιασμό και συσσώρευση ανώμαλων πλασματοκυτ-τάρων στο μυελό των οστών.

21
Η οστική νόσος στο Πολλαπλούν Μυέλωμα
Συχνότερη επιπλοκή της νόσου (70-80%) Οστεολύσεις (70%), διάχυτη οστεοπενία (10-15%) Πολύ σπάνια αυξημένη οστεοβλαστική δραστηριότητα (οστεοσκληρυ-ντικό μυέλωμα)
 Οστεολύσεις (70%), διάχυτη οστεοπενία (10-15%) Πολύ σπάνια αυξημένη οστεοβλαστική δραστηριότητα (οστεοσκληρυ-ντικό μυέλωμα)")
24
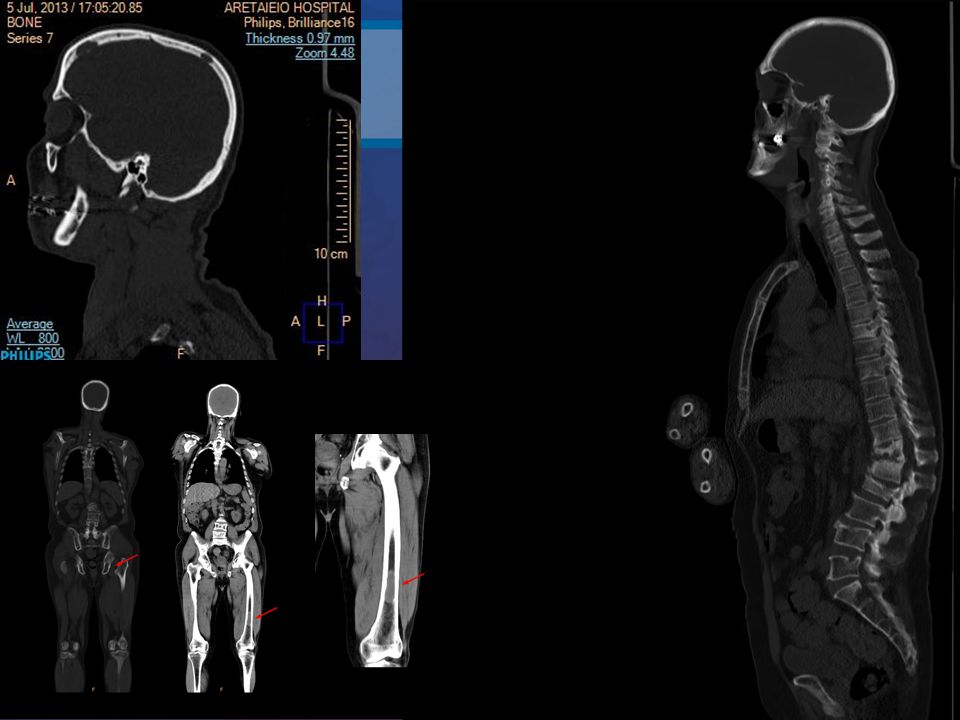
Whole-body CT: μακρά οστά

25
Whole-body CT: εξωοστικές μάζες

26
MRI: πιο ευαίσθητη από την κλασσική ακτινογραφία
Ανίχνευση οζωδών εστιών: MRI: 74% Απλές ακτινογραφίες: 56% 52% από 267 ασθενείς με αρνητικές ακτινογραφίες έχουν θετική MRI MRI: πιο ευαίσθητη σε ΣΣ, λεκάνη και στέρνο Walker et al. J Clin Oncol 2007;25:1121-8

27
Νέα κριτήρια ΠΜ Definition of Multiple Myeloma
Clonal bone marrow plasma cells ≥10% or biopsy proven bony or extramedullary plasmacytoma and ANY ONE OR MORE OF THE FOLLOWING MYELOMA DEFINING EVENTS Evidence of end organ damage that can be attributed to the underlying plasma cell proliferative disorder, specifically Hypercalcemia: Serum calcium >0.25 mmol/L (> 1mg/dL) above upper limit of normal or > 2.75 mmol/L (> 11 mg/dL) Renal insufficiency: Creatinine Clearance <40 ml/minute or Serum creatinine > 2mg/dL Anemia: Normochromic, normocytic with a hemoglobin value of >2 g/dL below the lower limit of normal or a hemoglobin value <10 g/dL Bone lesions: one or more osteolytic lesions on skeletal radiography, CT, or PET-CT, or Any one or more of the following biomarkers of malignancy Clonal bone marrow plasma cell percentage* ≥ 60% Involved/uninvolved serum free light chain ratio‡ ≥100 >1 focal lesions on magnetic resonance imaging studies Rajkumar VS et al. Lancet Oncol 2014; in press.
 above upper limit of normal or > 2.75 mmol/L (> 11 mg/dL) Renal insufficiency: Creatinine Clearance <40 ml/minute or Serum creatinine > 2mg/dL. Anemia: Normochromic, normocytic with a hemoglobin value of >2 g/dL below the lower limit of normal or a hemoglobin value <10 g/dL. Bone lesions: one or more osteolytic lesions on skeletal radiography, CT, or PET-CT, or. Any one or more of the following biomarkers of malignancy. Clonal bone marrow plasma cell percentage* ≥ 60% Involved/uninvolved serum free light chain ratio‡ ≥100. >1 focal lesions on magnetic resonance imaging studies. Rajkumar VS et al. Lancet Oncol 2014; in press.")
28
Η οστική νόσος στο ΠΜ: παθοφυσιολογία
Oστεοβλάστης CD138 OPG (-) ↓ bALP, ↓ osteocalcin Mυελωματικά κύτταρα RANKL sclerostin, activin-A DKK1, sFRP-2, IL-3, IL-7 a4b1 integrin RANKL BMSCs VCAM-1 RANKL IL-11, IL-1b, bFGF TNFa, M-CSF RANK (-) OPG IL-6 MIP-1a, MIP-1b, SDF-1a, IL-3, HGF, OPN Πρόδρομος οστεοκλάστης Ενεργοποιημένοι OCs Οστική αποδόμηση TRACP-5b Προϊόντα αποδομής Κολλαγόνου τύπου-1: NTX, ICTP, CTX Terpos E & Dimopoulos MA. Ann Oncol 2005;16:
 ↓ bALP, ↓ osteocalcin. Mυελωματικά κύτταρα. RANKL. sclerostin, activin-A. DKK1, sFRP-2, IL-3, IL-7. a4b1 integrin. RANKL. BMSCs. VCAM-1. RANKL. IL-11, IL-1b, bFGF. TNFa, M-CSF. RANK. (-) OPG. IL-6. MIP-1a, MIP-1b, SDF-1a, IL-3, HGF, OPN. Πρόδρομος. οστεοκλάστης. Ενεργοποιημένοι OCs. Οστική αποδόμηση. TRACP-5b. Προϊόντα αποδομής. Κολλαγόνου τύπου-1: NTX, ICTP, CTX. Terpos E & Dimopoulos MA. Ann Oncol 2005;16:")
29
Οστεοκλάστης: κύτταρο «κλειδί» στην επιβίωση του μυελωματικού κυττάρου
Οστεοκλάστης: κύτταρο «κλειδί» στην επιβίωση του μυελωματικού κυττάρου Μετά 14 ημέρες: καλλιέργεια μυελωματικών κυττάρων χωρίς OC με OC Abe et al, Blood 2004;104:2484

30
Oστεοκλάστες–οστεοβλάστες και ανάπτυξη των μυελωματικών κυττάρων
MM MM+OC MM+OB MM+OC+OB 1 2 3 4 5 6 7 BrdU (%) P<0.04 P<0.02 P<0.0003 P<0.002 Yaccoby et al. Haematologica 2006;91:192–9
 P<0.04. P<0.02. P< P< Yaccoby et al. Haematologica 2006;91:192–9.")
31
Μειωμένη οστεοβλαστική δραστηριότητα στο ΠΜ
Μειωμένη οστεοβλαστική δραστηριότητα στο ΠΜ 86 35 40 45 N = GROUP MM Stage 3 MM Stage1/2 MGUS Controls Lg bALP 2.5 2.0 1.5 1.0 .5 0.0 90 122 116 67 151 149 130 159 p<0.001 Politou et al. Br J Haematol 2004;126:686-9

32
DKK-1 στο ΠΜ GROUP Controls MGUS MM LG DKK - 1
22 18 32 N = GROUP Controls MGUS MM LG DKK - 1 2.6 2.4 2.2 2.0 1.8 1.6 1.4 1.2 1.0 .8 Politou et al. Ιnt J Cancer 2006;119:

33
Η σκληροστίνη στο ΠΜ mean value: 0.31±0.20 0.26±0.29 0.48±0.46 ±SD
p=0.01 p=0.004 Terpos et al. Int J Cancer 2012;131:

34
Η ακτιβίνη Α στο μυελό ασθενών με ΠΜ
NS ** *p < 0.05 NS 150 100 50 Activin A (pg/mL) MM 0–1 OL MM > 1 OL Non-MM * 3,500 3,000 Mean 1,884 2,500 **p < 0.01 2,000 Mean 1,300 Activin A (pg/mL) 1,500 Mean 299 1,000 500 Mean8.2 Διάμεσα επίπεδα activin A MM 0–1 OL: pg/mL MM > 1 OL: pg/mL Non-MM: 30.6 pg/mL OC BMSC OB MM Vallet S, et al. Proc Natl Acad Sci. 2010;107:
 MM 0–1 OL. MM > 1 OL. Non-MM. * 3,500. 3,000. Mean 1,884. 2,500. **p < ,000. Mean 1,300. Activin A (pg/mL) 1,500. Mean , Mean8.2. Διάμεσα επίπεδα activin A MM 0–1 OL: pg/mL. MM > 1 OL: pg/mL. Non-MM: 30.6 pg/mL. OC. BMSC. OB. MM. Vallet S, et al. Proc Natl Acad Sci. 2010;107:")
35
Η ακτιβίνη-Α στο ΠΜ

36
Αυξητικοί παράγοντες (TGF-b, IGFs, FGFs, PDGFs, BMPs)
Ο RANKL προάγει την ανάπτυξη όγκων που εκφράζουν RANK Κυτταροκίνες και αυξητικοί παράγοντες (IL-6, IL-8, IL-1, PGE2, TNF-, CSF-1, PTHrP) Καρκινικά κύτταρα που εκφράζουν RANK RANK RANKL Οστεοβλάστες Αυξητικοί παράγοντες (TGF-b, IGFs, FGFs, PDGFs, BMPs) Οστική αποδόμηση Ca2+ Tumor cells may also express RANK and may be able to directly influence bone lesion progression by interacting with RANK Ligand. Tometsko et al1 showed that RANK is expressed on breast (MDA-231) and prostate (PC3) cancer cells. Therefore, it has been suggested that RANK Ligand in the bone microenvironment may activate tumor-localized RANK in a paracrine manner to induce the expression of osteotropic factors (IL-1 and IL-6), angiogenic factors (IL-8), metalloproteinases, chemoattractants, and COX-2. These factors in turn promote tumor growth and proliferation, osteoclast recruitment to the site of bone metastases, and osteoclast maturation. Bhatia et al2 studied the expression patterns of RANK and RANK Ligand by immunohistochemistry in various breast cancer tumor cells (nonneoplastic, infiltrating ductal carcinoma [IDC], and breast cancer bony metastases). They found that all tumor cells expressed RANK; however, RANK Ligand was primarily expressed in nonmetastatic tumor cells. These findings led the authors to hypothesize that, in the absence of tumor-expressed RANK Ligand, tumor-localized RANK may interact with RANK Ligand at the surface of osteoblasts, thus targeting the tumor to the bone surface. They further hypothesized that this tumor-osteoblast interaction may lead to secondary activation of osteoclasts, thus leading to increased osteolysis at the site of metastasis. Therefore, results of these preliminary studies suggest that inhibition of RANK Ligand signaling can disrupt tumor growth and proliferation and may prevent bone metastases. 1. Tometsko M, Armstrong A, Miller R, et al. RANK Ligand directly induces osteoclastogenic, angiogenic, chemoattractive, and invasive factors on RANK-expressing human cancer cells MDA-MB-231 and PC3. ASBMR Abstract 1095. 2. Bhatia P, Sanders MM, Hansen MF. Expression of receptor activator of nuclear factor-B ligand is inversely correlated with metastatic phenotype in breast carcinoma. Clin Cancer Res. 2005;11: Roodman, N Engl J Med 2004;350:
 Καρκινικά κύτταρα που εκφράζουν RANK. RANK. RANKL. Οστεοβλάστες. Αυξητικοί παράγοντες (TGF-b, IGFs, FGFs, PDGFs, BMPs) Οστική αποδόμηση. Ca2+ Tumor cells may also express RANK and may be able to directly influence bone lesion progression by interacting with RANK Ligand. Tometsko et al1 showed that RANK is expressed on breast (MDA-231) and prostate (PC3) cancer cells. Therefore, it has been suggested that RANK Ligand in the bone microenvironment may activate tumor-localized RANK in a paracrine manner to induce the expression of osteotropic factors (IL-1 and IL-6), angiogenic factors (IL-8), metalloproteinases, chemoattractants, and COX-2. These factors in turn promote tumor growth and proliferation, osteoclast recruitment to the site of bone metastases, and osteoclast maturation. Bhatia et al2 studied the expression patterns of RANK and RANK Ligand by immunohistochemistry in various breast cancer tumor cells (nonneoplastic, infiltrating ductal carcinoma [IDC], and breast cancer bony metastases). They found that all tumor cells expressed RANK; however, RANK Ligand was primarily expressed in nonmetastatic tumor cells. These findings led the authors to hypothesize that, in the absence of tumor-expressed RANK Ligand, tumor-localized RANK may interact with RANK Ligand at the surface of osteoblasts, thus targeting the tumor to the bone surface. They further hypothesized that this tumor-osteoblast interaction may lead to secondary activation of osteoclasts, thus leading to increased osteolysis at the site of metastasis. Therefore, results of these preliminary studies suggest that inhibition of RANK Ligand signaling can disrupt tumor growth and proliferation and may prevent bone metastases. 1. Tometsko M, Armstrong A, Miller R, et al. RANK Ligand directly induces osteoclastogenic, angiogenic, chemoattractive, and invasive factors on RANK-expressing human cancer cells MDA-MB-231 and PC3. ASBMR Abstract Bhatia P, Sanders MM, Hansen MF. Expression of receptor activator of nuclear factor-B ligand is inversely correlated with metastatic phenotype in breast carcinoma. Clin Cancer Res. 2005;11: Roodman, N Engl J Med 2004;350:")
37
Έκφραση του RANK σε συμπαγείς όγκους
Expression Καρκινικά κύτταρα μαστού Immunohistochemistry was performed on breast primary and metastatic primary tumors. You can see here that both tumor types express RANK. Note if asked: Penninger paper would lead to a hypothesis that there would be an even greater RANK expression by a breast CA bone metastasis. Breast M347 in House RANK Antibody Antigen name: hRANK-Fc Mouse Monoclonal IgG1 Selected as the cleanest of 3 hybridoma proteins during previous IHC work 2002 Prostate Chemicon Polyclonal RANK Antibody RANK Expression Κύτταρα καρκίνου προστάτη σε οστική μετάσταση Jones et al, Nature 2006;440:692-6.

38
Αναστολή του RANKL από OPG
Χωρίς οστεολύσεις OPG Dose (mg/kg) 0.3 1 3 2 4 * # Lesions / Mouse 0.3 1 3 60 120 180 OPG Dose (mg/kg) * # of OC / mm2 Tumor Area In this experiment, nude mice were injected with (MDA-231 into left ventricle) breast cancer cells resulting in bone metastases that were associated with osteolytic lesions. 4 groups of mice were treated with different doses of OPG (0, 0.3, 1, and 3 mg/kg) 3 times per week for 4 weeks, starting immediately after innoculation. There was a dose dependent decrease in the number and area of radiologically evident bone lesions; and you can see on the radiograph that OPG treatment at the highest dose completely prevented the radiographic appearance of osteolytic lesions (radiograph on the right). You may note the increased radio-opacity of the tibial and femoral metaphyseal growth plates, this increase is a normal response to OPG by growing mice. Their resorption of the secondary spongiosa is inhibited and trabecular bone accumulates. In this breast cancer metastasis model, RANK Ligand inhibition was associated with dose-dependent and significant decrease in both frequency and size of skeletal tumors (top chart on right) and a significant decrease in the number of osteoclasts within the tumor (with a maximum reduction of 90% at 3 mg/kg, p<0.01) (bottom chart on right). Morony S, et al. Osteoprotegerin Inhibits Osteolysis and Decreases Skeletal Tumor Burden in Syngeneic and Nude Mouse Models of Experimental Bone Metastasis. Cancer Res ;61: Control Αναστολή του RANKL από OPG Morony et al. Cancer Res 2001;61(11):4432-6
 * # Lesions / Mouse OPG Dose (mg/kg) * # of OC / mm2 Tumor Area. In this experiment, nude mice were injected with (MDA-231 into left ventricle) breast cancer cells resulting in bone metastases that were associated with osteolytic lesions. 4 groups of mice were treated with different doses of OPG (0, 0.3, 1, and 3 mg/kg) 3 times per week for 4 weeks, starting immediately after innoculation. There was a dose dependent decrease in the number and area of radiologically evident bone lesions; and you can see on the radiograph that OPG treatment at the highest dose completely prevented the radiographic appearance of osteolytic lesions (radiograph on the right). You may note the increased radio-opacity of the tibial and femoral metaphyseal growth plates, this increase is a normal response to OPG by growing mice. Their resorption of the secondary spongiosa is inhibited and trabecular bone accumulates. In this breast cancer metastasis model, RANK Ligand inhibition was associated with dose-dependent and significant decrease in both frequency and size of skeletal tumors (top chart on right) and a significant decrease in the number of osteoclasts within the tumor (with a maximum reduction of 90% at 3 mg/kg, p<0.01) (bottom chart on right). Morony S, et al. Osteoprotegerin Inhibits Osteolysis and Decreases Skeletal Tumor Burden in Syngeneic and Nude Mouse Models of Experimental Bone Metastasis. Cancer Res. 2001;61: Control. Αναστολή του RANKL από OPG. Morony et al. Cancer Res 2001;61(11):")
39
Η αναστολή του RANKL αναστέλλει τις οστικές μεταστάσεις σε ζωϊκό μοντέλο καρκίνου προστάτη
50 40 30 20 10 Basal Vehicle sRANK-Fc * BAP (U/L) 25 15 5 uNTx (nM BCE/mM creatinine) RANK Ligand Inhibition (RANK:Fc) X-ray Osteoblastic bone metastases Prostate Cancer LuCaP 35 HU / SCID Model, Rx Initiated at 6 Weeks Inhibition of RANK Ligand blocks normal osteoclast differentiation and activity, resulting in significantly decreased bone turnover.1 Serum and urine were collected from mice in basal, sRANK-Fc, and vehicle treatment groups at the time of their euthanasia. Urine NTx (top graph) and serum BAP (bottom graph) levels are reported as bone collagen equivalents (BCE) normalized to urine creatinine levels. Data are reported as mean ± SD. Data were analyzed using one-way ANOVA and Fisher’s protected least significant difference for post hoc analysis. (n= 6 to 9 mice per group) Mice treated with sRANK-Fc had lower levels of serum BAP and urine NTx compared with vehicle-treated mice (P < 0.01).1 1. Zhang J, et al. Cancer Res. 2003;63: Zhang J, et al. Cancer Res. 2003;63:
 uNTx (nM BCE/mM creatinine) RANK Ligand Inhibition. (RANK:Fc) X-ray. Osteoblastic bone metastases. Prostate Cancer LuCaP 35 HU / SCID Model, Rx Initiated at 6 Weeks. Inhibition of RANK Ligand blocks normal osteoclast differentiation and activity, resulting in significantly decreased bone turnover.1. Serum and urine were collected from mice in basal, sRANK-Fc, and vehicle treatment groups at the time of their euthanasia. Urine NTx (top graph) and serum BAP (bottom graph) levels are reported as bone collagen equivalents (BCE) normalized to urine creatinine levels. Data are reported as mean ± SD. Data were analyzed using one-way ANOVA and Fisher’s protected least significant difference for post hoc analysis. (n= 6 to 9 mice per group) Mice treated with sRANK-Fc had lower levels of serum BAP and urine NTx compared with vehicle-treated mice (P < 0.01) Zhang J, et al. Cancer Res. 2003;63: Zhang J, et al. Cancer Res. 2003;63:")
40
ΑΝΤΙΣΤΕΟΛΥΤΙΚΑ ΦΑΡΜΑΚΑ ΣτιΣ οΣτικεΣ μεταΣταΣειΣ και την οΣτικη νοΣο του μυελωματοΣ

41
Διφωσφονικά άλατα Induce apoptosis Inhibit migration
Terpos et al. Ann Oncol 2009; 20(8):
:")
42
Διφωσφονικά άλατα: η κύρια θεραπεία στην οστική νόσο του μυελώματος

43
Δράση των αμινοδιφωσφονικών

44
Zολεδρονικό οξύ έναντι παμιδρονάτης
Rosen et al. Cancer 2003;98:

45
Zολεδρονικό οξύ και Ca πνεύμονος
Rosen et al. J Clin Oncol 2003;16:3150-7 Rosen et al. Cancer 2004;100:

46
ONJ: χαρακτηριστικά • οίδημα ή φλεγμονή Σημεία • “βαριά γνάθος”
Συμπτώματα • “βαριά γνάθος” • μούδιασμα στη γνάθο • πόνος σε δόντι • γενικευμένος πόνος στη γνάθο Σημεία • οίδημα ή φλεγμονή • εκτεθειμένο οστούν στη στοματική κοιλότητα • έλκος που αποτυγχάνει να ιαθεί • αυτόματη απώλεια δοντιών

48
Συχνότητα της Οστεονέκρωσης στο Μυέλωμα
Cumulative incidence of death Cumulative incidence of ONJ 1-year 2-years 3-years 4-years % OS 97% 88% 79% 67% % ONJ (95%CI) 1% (0.2%-5%) 4.9% (2.5%-8.5%) 8.5% (5%-13%) 11.6% (7.2%-17.1%)
 1% (0.2%-5%) 4.9% (2.5%-8.5%) 8.5% (5%-13%) 11.6% (7.2%-17.1%)")
49
Denosumab: Μηχανισμοί Δράσης
Y denosumab CFU-M OPG Y RANKL Πρόδρομοι οστεοκλάστες RANK Y Κυτταροκίνες, αυξητικοί παράγοντες Πολυπύρηνοι οστεοκλάστες RANKL Y Osteoprotegrin, also known as OPG, is an endogenous decoy receptor secreted by osteoblast precursors. Binding of OPG to RANK Ligand such that RANKL does not bind to osteoclast RANK causes the osteoclast to undergo apoptosis as well as halt the maturation and activation of additional osteoclasts. Remember that denosumab is a fully human antibody with high specificity for RANK Ligand, while OPG has other potential targets or functions. But, OPG is used in non-primate preclinical models to demonstrate the effects of RANK Ligand blockade. From Medical Affairs: Denosumab is an investigational, fully human monoclonal antibody that appears to specifically (and with high affinity) bind and neutralize Receptor Activator of Nuclear Factor kappa B ligand (RANK ligand).1 RANK ligand has been identified as the primary mediator of osteoclast formation, function, and survival. By preventing RANK Ligand from binding to its receptor, RANK, osteoclast differentiation, activation, and survival are inhibited (right side of figure).1,2 1. Bekker PJ, Holloway DL, Rasmussen AS, et al. A single-dose placebo-controlled study of denosumab, a fully human monoclonal antibody to RANKL, in postmenopausal women. J Bone Miner Res. 2004;19: 2. Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation. Nature. 2003;423: Oστεοκλάστης Ώριμοι οστεοκλάστες οστεοβλάστες Οστούν Boyle et al. Nature 2003; 423:
 bind and neutralize Receptor Activator of Nuclear Factor kappa B ligand (RANK ligand).1 RANK ligand has been identified as the primary mediator of osteoclast formation, function, and survival. By preventing RANK Ligand from binding to its receptor, RANK, osteoclast differentiation, activation, and survival are inhibited (right side of figure).1,2. 1. Bekker PJ, Holloway DL, Rasmussen AS, et al. A single-dose placebo-controlled study of denosumab, a fully human monoclonal antibody to RANKL, in postmenopausal women. J Bone Miner Res. 2004;19: Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation. Nature. 2003;423: Oστεοκλάστης. Ώριμοι οστεοκλάστες. οστεοβλάστες. Οστούν. Boyle et al. Nature 2003; 423:")
50
Η αναστολή του RANKL «σπάει» το φαύλο κύκλο οστικής καταστροφής-επέκτασης του όγκου
Καρκινικά κύτταρα στο οστούν Άμεση δράση στα καρκινικά κύτταρα? Κυτταροκίνες και αυξητικοί παράγοντες (IL-6, IL-8, IL-1, PGE-2, TNF-, CSF-1, PTHrP) Αυξητικοί παράγοντες (TGF-b, IGFs, FGFs, PDGFs, BMPs) Denosumab RANKL Οστεοκλάστης RANKL There may be additional benefit of RANK Ligand blockade. As was presented earlier, there is a balance between osteoclasts and osteoblasts. RANK Ligand is necessary for the osteoclast formation, function, and survival. Bone resorption from the osteoclasts releases growth factors, including large amounts of calcium which is itself a growth factor, and these stimulate tumor cells. The tumor grows and secretes additional growth factors and cytokines which stimulate the osteoblast, which then secretes RANKL and the vicious cycle continues. Blocking RANKL can block the cycle. However, there is also a potential additional benefit since some cancer cells have also been shown to express RANK, such that RANK Ligand blockade may halt a potential additional stimulatory pathway on the tumors directly. Οστική αποδόμηση Οστεοβλάστης RANKL Οστούν RANK Roodman, N Engl J Med 2004;350:
 Αυξητικοί παράγοντες (TGF-b, IGFs, FGFs, PDGFs, BMPs) Denosumab. RANKL. Οστεοκλάστης. RANKL. There may be additional benefit of RANK Ligand blockade. As was presented earlier, there is a balance between osteoclasts and osteoblasts. RANK Ligand is necessary for the osteoclast formation, function, and survival. Bone resorption from the osteoclasts releases growth factors, including large amounts of calcium which is itself a growth factor, and these stimulate tumor cells. The tumor grows and secretes additional growth factors and cytokines which stimulate the osteoblast, which then secretes RANKL and the vicious cycle continues. Blocking RANKL can block the cycle. However, there is also a potential additional benefit since some cancer cells have also been shown to express RANK, such that RANK Ligand blockade may halt a potential additional stimulatory pathway on the tumors directly. Οστική αποδόμηση. Οστεοβλάστης. RANKL. Οστούν. RANK. Roodman, N Engl J Med 2004;350:")
51
Denosumab έναντι ΖΟ στον καρκίνο του μαστού
1,00 HR = 0,82 (95% CI: 0,71–0,95) P = 0,01 (ανωτερότητα)* P < 0,001 (μη κατωτερότητα) 0,75 Ποσοστό χωρίς SRE 0,50 0,25 Denosumab significantly delayed time to first SRE by 18% versus zoledronic acid (HR, 0.82; 95% CI, 0.710.95; P <0.001 noninferiority; P = 0.01 superiority.) The treatment effect of denosumab was consistent over time. Median time to first on-study SRE was 26.4 months for the zoledronic acid group and had not been reached for the denosumab group at the time of the analysis. Reference Stopeck AT, Lipton A, Body J-J, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 2010;28:5132–9. Ζολεδρονικό οξύ (n = 1.020) Denosumab (n = 1.026) 3 6 9 12 15 18 21 24 27 Μήνες Αρ. ασθενών που διατρέχουν κίνδυνο Ζολεδρονικό οξύ IV 1020 829 676 584 498 427 296 191 94 29 Denosumab SC 1026 839 697 602 514 437 306 189 99 26 Stopeck AT, et al. J Clin Oncol 2010;28:51329
 P = 0,01 (ανωτερότητα)* P < 0,001 (μη κατωτερότητα) 0,75. Ποσοστό χωρίς SRE. 0,50. 0,25. Denosumab significantly delayed time to first SRE by 18% versus zoledronic acid (HR, 0.82; 95% CI, 0.710.95; P <0.001 noninferiority; P = 0.01 superiority.) The treatment effect of denosumab was consistent over time. Median time to first on-study SRE was 26.4 months for the zoledronic acid group and had not been reached for the denosumab group at the time of the analysis. Reference. Stopeck AT, Lipton A, Body J-J, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 2010;28:5132–9. Ζολεδρονικό οξύ (n = 1.020) Denosumab (n = 1.026) Μήνες. Αρ. ασθενών που διατρέχουν κίνδυνο. Ζολεδρονικό οξύ IV Denosumab SC Stopeck AT, et al. J Clin Oncol 2010;28:51329.")
52
Denosumab έναντι ΖΟ στον καρκίνο του προστάτη
XGEVA™ PI, 2010: 11,Table 2 Fizazi K, et al. Lancet 2011;377: 816,Figure 2 HR = 0,82 (95% CI, 0,71–0,95) P 0,001 (μη κατωτερότητα) P = 0,008 (ανωτερότητα) 1,00 0,75 Ποσοστό Ασθενών Χωρίς SRE 0,50 Εκτίμηση Kaplan-Meier του Διάμεσου Αριθμού Μηνών 0,25 Key Points Denosumab significantly delayed the time to first on-study SRE by 18% compared with zoledronic acid (HR = 0.82; 95% CI, 0.71–0.95; P .001 for noninferiority and P = for superiority)1 The median (95% CI) time to first on-study SRE was 20.7 months in the denosumab group and months in the zoledronic acid group, a difference of 3.6 months1 Between-group divergence is evident beginning at 3 months after initiation of treatment2 References XGEVA™ (denosumab) prescribing information, Amgen. Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377: Denosumab Ζολεδρονικό οξύ 20.7 XGEVA™ PI, 2010: 11,Table 2 17.1 0,00 3 6 9 12 15 18 21 24 27 Fizazi K, et al. Lancet 2011;377: 816,Figure 2 Μήνας Μελέτης Ασθενείς που Διατρέχουν Κίνδυνο: Ζολεδρονικό οξύ 951 733 544 407 299 207 140 93 64 47 Denosumab 950 758 582 472 361 259 168 115 70 39 Fizazi K, et al. Lancet. 2011;377:813–822.
 P 0,001 (μη κατωτερότητα) P = 0,008 (ανωτερότητα) 1,00. 0,75. Ποσοστό Ασθενών Χωρίς SRE. 0,50. Εκτίμηση Kaplan-Meier του Διάμεσου Αριθμού Μηνών. 0,25. Key Points. Denosumab significantly delayed the time to first on-study SRE by 18% compared with zoledronic acid (HR = 0.82; 95% CI, 0.71–0.95; P .001 for noninferiority and P = .008 for superiority)1. The median (95% CI) time to first on-study SRE was 20.7 months in the denosumab group and 17.1 months in the zoledronic acid group, a difference of 3.6 months1. Between-group divergence is evident beginning at 3 months after initiation of treatment2. References. XGEVA™ (denosumab) prescribing information, Amgen. Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377: Denosumab. Ζολεδρονικό οξύ XGEVA™ PI, 2010: 11,Table , Fizazi K, et al. Lancet 2011;377: 816,Figure 2. Μήνας Μελέτης. Ασθενείς που Διατρέχουν Κίνδυνο: Ζολεδρονικό οξύ Denosumab Fizazi K, et al. Lancet. 2011;377:813–822.")
53
Denosumab έναντι ZΟ στο ΠΜ
Key endpoints: Primary: Time to the first on-study SRE (non-inferiority test) Secondary: Time to the first-and-subsequent SRE (superiority test, using multiple event analysis); time to the first on-study SRE (superiority test) Dmab (120 mg SC) + placebo IV, q 4 weeks ZOL (4 mg IV) + placebo SC, q 4 weeks Event-driven (until ~800 patients have ≥ 1 on-study SRE) R Study, N = 1,520 Newly diagnosed MM and plan to receive primary, frontline antimyeloma therapies ≥ 1 bone lesion ECOG performance status = 0, 1, or 2, and adequate organ function No prior antimyeloma, denosumab, or IVBP therapy No oral BPs for > 1 year Status: Recruiting participants BP, Bisphosphonate; Dmab , Denosumab; ECOG , Eastern Cooperative Oncology Group; SRE, Skeletal- related event; ZOL , Zoledronic acid. Terpos et al. ESMO 2014
 Secondary: Time to the first-and-subsequent SRE (superiority test, using multiple event analysis); time to the first on-study SRE (superiority test) Dmab (120 mg SC) + placebo IV, q 4 weeks. ZOL (4 mg IV) + placebo SC, q 4 weeks. Event-driven (until ~800 patients have ≥ 1 on-study SRE) R. Study, N = 1,520. Newly diagnosed MM and plan to receive primary, frontline antimyeloma therapies. ≥ 1 bone lesion. ECOG performance status = 0, 1, or 2, and adequate organ function. No prior antimyeloma, denosumab, or IVBP therapy. No oral BPs for > 1 year. Status: Recruiting participants. BP, Bisphosphonate; Dmab , Denosumab; ECOG , Eastern Cooperative Oncology Group; SRE, Skeletal- related event; ZOL , Zoledronic acid. Terpos et al. ESMO")
54
Sotatercept στο Μυέλωμα
MPT + 4 cycles of sotatercept, g/kg Placebo 0.1 0.3 0.5 n 6 8 Time from start of treatment (days) 169/ET 85 Hip BMD, change from baseline (%) 4 2 –2 –3 3 1 –1 Placebo 0.1 mg/kg 0.3 mg/kg 0.5 mg/kg change from baseline (%) Lumbar BMD, Without bisphosphonates With bisphosphonates All patients Lumbar BMD, maximum change from baseline (%) 7 5 3 1 –1 –2 6 4 2 Placebo 0.1 mg/kg 0.3 mg/kg 0.5 mg/kg
 169/ET. 85. Hip BMD, change from baseline (%) –2. – –1. Placebo. 0.1 mg/kg. 0.3 mg/kg. 0.5 mg/kg. change from baseline (%) Lumbar BMD, Without bisphosphonates. With bisphosphonates. All patients. Lumbar BMD, maximum change from baseline (%) –1. – Placebo. 0.1 mg/kg. 0.3 mg/kg. 0.5 mg/kg.")
55
BHQ880 (αντι-Dkk1) και Zoλεδρονικό οξύ στο Μυέλωμα
Key endpoints (phase II): Primary: Time to first SRE and change in bone marker levels Secondary: Safety, tolerability, pharmacokinetic profile, assess potential immunogenicity, binding kinetics (free and BHQ880-bound DKK1), biochemical markers of bone formation, resorption, and metabolism, pharmacodynamics Medium-dose BHQ880, IV q 28 days + ZOL (4 mg), IV q 28 days High-dose BHQ880, IV q 28 days + ZOL (4 mg), IV q 28 days Low-dose BHQ880, IV q 28 days + ZOL (4 mg), IV q 28 days Placebo, IV q 28 days + ZOL (4 mg), IV q 28 days R (N = 267) Symptomatic relapsed/refractory MM not requiring bortezomib Measureable serum/urine M-protein OR free light-chain concentration ≥ 1 SRE and current/planned ZOL treatment MTD and DLT to be determined in phase Ib 9 months Status: Completed DLT, Dose-limiting toxicity; MTD, Maximum tolerated dose; q = Every; ZOL, Zoledronic acid Clinical Trials.gov Identifier: NCT
: Primary: Time to first SRE and change in bone marker levels. Secondary: Safety, tolerability, pharmacokinetic profile, assess potential immunogenicity, binding kinetics (free and BHQ880-bound DKK1), biochemical markers of bone formation, resorption, and metabolism, pharmacodynamics. Medium-dose BHQ880, IV q 28 days + ZOL (4 mg), IV q 28 days. High-dose BHQ880, IV q 28 days + ZOL (4 mg), IV q 28 days. Low-dose BHQ880, IV q 28 days + ZOL (4 mg), IV q 28 days. Placebo, IV q 28 days + ZOL (4 mg), IV q 28 days. R. (N = 267) Symptomatic relapsed/refractory MM not requiring bortezomib. Measureable serum/urine M-protein OR free light-chain concentration. ≥ 1 SRE and current/planned ZOL treatment. MTD and DLT to be determined in phase Ib. 9 months. Status: Completed. DLT, Dose-limiting toxicity; MTD, Maximum tolerated dose; q = Every; ZOL, Zoledronic acid. Clinical Trials.gov Identifier: NCT")
56
Συμπεράσματα για την Οστική Νόσο του Μυελώματος και τις Οστικές Μεταστάσεις
Η oστική νόσος στο ΠΜ οφείλεται σε αυξημένη οστεοκλαστική δραστηριότητα και μειωμένη οστική παραγωγή. Διφωσφονικά: κύρια φάρμακα για το ΠΜ και τις οστικές μεταστάσεις Οι βιολογικοί δρόμοι των RANK/RANKL/OPG, MIP-1α είναι σημαντικοί όχι μόνο για την ενεργοποίηση των οστεοκλαστών και την ανάπτυξη της οστικής νόσου στις κακοήθειες. Έτσι αποτελούν θεραπευτικούς στόχους (αnti-RANKL, denosumab). Ο βιολογικός δρόμος Wnt εμπλέκεται στην αδρανοποίηση των οστεοβλαστών (Dkk-1, σκληροστίνη). Νέα φάρμακα που στοχεύουν τα μόρια αυτά (αντι-Dkk1, αντι-SOST, αντι-ακτιβίνη Α) έχουν ήδη εισέλθει σε μελέτες φάσης 2 στο ΠΜ και προβλέπεται να αλλάξουν την αντιμετώπιση της οστικής νόσου του ΠΜ τα επόμενα χρόνια.
. Ο βιολογικός δρόμος Wnt εμπλέκεται στην αδρανοποίηση των οστεοβλαστών (Dkk-1, σκληροστίνη). Νέα φάρμακα που στοχεύουν τα μόρια αυτά (αντι-Dkk1, αντι-SOST, αντι-ακτιβίνη Α) έχουν ήδη εισέλθει σε μελέτες φάσης 2 στο ΠΜ και προβλέπεται να αλλάξουν την αντιμετώπιση της οστικής νόσου του ΠΜ τα επόμενα χρόνια.")
57
ΕφαρμογεΣ τηΣ οΣτεοανοΣολογιαΣ Σε αλλα νοΣηματα των οΣτων

58
1. Μετεμμηνοπαυσιακή οστεοπόρωση
Η ελάττωση των οιστρογόνων μετά την εμμηνόπαυση σχετίζεται με ταχεία επίμονη αύξηση του ρυθμού με τον οποίο το οστό αποδομείται. Σε μια σειρά πειραμάτων σε ωοθηκεκτομηθέντα ποντίκια, αλλά χωρίς Τ-λεμφοκύτταρα, δεν υπήρχε απώλεια οστού μετά την ωοθηκεκτομή, αποδεικνύοντας ότι τα Τ-λεμφοκύτταρα είναι απαραίτητα για τη διαδικασία αυτή. Έχει βρεθεί ότι γυναίκες με μετεμηνοπαυσιακή οστεοπόρωση έχουν αυξημένα επίπεδα RANKL στον ορό τους.

59
Αντι-RANKL (denosumab) στη μετεμμηνοπαυσιακή οστεοπόρωση (McClung et al, NEJM 2006;354:821)
 στη μετεμμηνοπαυσιακή οστεοπόρωση (McClung et al, NEJM 2006;354:821)")
60
Romosozumab (Αντι-sclerostin)
. McClung MR, et al. N Engl J Med. 2014;370:

61
2. Oστεοπόρωση στη ρευματοειδή αρθρίτιδα
Βασικό γνώρισμα στη Ρευματοειδή Αρθρίτιδα είναι η ταχεία καταστροφή του περιαρθρικού οστού που ακολουθείται συχνά από δευτερογενή οστεοπόρωση. Οι OCs βρίσκονται σε μεγάλο αριθμό στη θέση της οστικής αποδόμησης και φαίνεται να παίζουν σημαντικό ρόλο, ενώ η ενεργοποίησή τους σχετίζεται σημαντικά με την υπερπαραγωγή RANKL από τα Τ-λεμφοκύτταρα.

62
Oστεοπόρωση στη ρευματοειδή αρθρίτιδα (2)
Schett et al, Nat Clin Pract Rheumatol 2005;1:47-54

63
RA AS Gonzales-Alvaro et al, Ann Rheum Dis 2007;66:1675-8
Kim et al, Rheumatology 2006;45:

64
Μean change in MRI erosion score From baseline to 6 months
Αντι-RANKL (denosumab) στη ρευματοειδή αρθρίτιδα 2.5 2.0 Methotrexate + denosumab every 6 months for 12 months 1.5 Μean change in MRI erosion score From baseline to 6 months 1.0 0.5 Placebo N=67 Denosumab 60 mg (N=67) Denosumab 180 mg (N=68) Cohen et al, Arthritis Rheum 2008;58:
 στη ρευματοειδή αρθρίτιδα Methotrexate + denosumab. every 6 months for 12 months Μean change in MRI erosion score. From baseline to 6 months Placebo. N=67. Denosumab. 60 mg. (N=67) Denosumab. 180 mg. (N=68) Cohen et al, Arthritis Rheum 2008;58:")
65
3. OPG και πρωτοπαθής οστεοαρθρίτις του γόνατος
Pilichou et al, Clin Biochem 2008;41:746-9

66
Θαλασσαιμία και Οστεοπόρωση

67
Οστεοπόρωση και Θαλασσαιμία
Η οστεοπόρωση αποτελεί σημαντικό πρόβλημα στους ενήλικες ασθενείς με β-θαλασσαιμία Επίπτωση: 40%-60% Μέση ετήσια απώλεια οστικής μάζας στην ΟΜΣΣ: –1.36% ΟΜΣΣ 89% Ισχίο % Καρπός 73% Dresner Pollack et al. Br J Haematol 2000;111:

68
Παράγοντες που συντελούν στην απώλεια οστικής μάζας στη Θαλασσαιμία (1)
Επέκταση του μυελού των οστών Μηχανική διακοπή της οστικής παραγωγής Λέπτυνση του οστικού φλοιού ευθραυστότητας του οστού Διαταραχές της λειτουργίας των ενδοκρινών αδένων Υπογοναδισμός Υπερφόρτωση με σίδηρο της υπόφυσης Υπερφόρτωση με σίδηρο των όρχεων και ωοθηκών Διαταραχές στο σύστημα αυξητικής ορμόνης/αυξητικού παράγοντα τύπου ινσουλίνης 1 Several acquired factors contribute to the pathogenesis of thalassaemia-induced osteoporosis Bone marrow expansion is a major contributor to osteoporosis, and is thought to physically block bone mineralisation, leading to cortical thinning and bone fragility (particularly in long bones) Hypogonadism is also common among patients with thalassaemia Because bone is a primary target for steroid hormones, particularly oestrogen, hypogonadism profoundly reduces BMD Other common endocrine imbalances in thalassaemia (eg, the growth hormone/IGF-1 signaling axis) also contribute to altered bone metabolism Voskaridou et al. Br J Haematol. 2004;127: 68
 Hypogonadism is also common among patients with thalassaemia. Because bone is a primary target for steroid hormones, particularly oestrogen, hypogonadism profoundly reduces BMD. Other common endocrine imbalances in thalassaemia (eg, the growth hormone/IGF-1 signaling axis) also contribute to altered bone metabolism. Voskaridou et al. Br J Haematol. 2004;127:")
69
Παράγοντες που συντελούν στην απώλεια οστικής μάζας στη Θαλασσαιμία (2)
Υπερφόρτωση με σίδηρο και θεραπείες αποσιδήρωσης Υπερφόρτωση με σίδηρο στα οστά Διαταραχή στην ωρίμανση των οστεοβλαστών τοπικής επιμετάλλωσης Θεραπεία με δεσφεριοξαμίνη διαφοροποίησης και πολλαπλασιασμού των οστεοβλαστών παραγωγής οστικού κολλαγόνου απόπτωση των οστεοβλαστών Έλλειψη βιταμινών και ηλεκτρολυτών Έλλειψη βιταμίνης D Έλλειψη ψευδαργύρου Συσχέτιση με χαμηλή οστική μάζα στη θαλασσαιμία Διαταραχή στη σχέση οστεοβλαστών και οστεοκλαστών Iron overload and chelation therapies also contribute to osteoporosis Iron deposition in bone leads to impaired maturation of bone cells and localised decreases in bone mineralisation, resulting in bone fragility High-dose chelation therapy (eg, desferoxamine) impairs osteoblast growth, reduces osteoblast survival, and inhibits the formation of collagen—the main organic component of bone matrix Patients with thalassaemia frequently develop vitamin and mineral deficiencies Vitamin D deficiency is associated with low BMD Zinc deficiency, which is prevalent among patients with thalassaemia, is also associated with low BMD, potentially through its effects on osteoclast activity and on enzymes required for new bone formation King JC. Am J Clin Nutr. 1996;64(3): Voskaridou et al. Br J Haematol. 2004;127(2): 69
 impairs osteoblast growth, reduces osteoblast survival, and inhibits the formation of collagen—the main organic component of bone matrix. Patients with thalassaemia frequently develop vitamin and mineral deficiencies. Vitamin D deficiency is associated with low BMD. Zinc deficiency, which is prevalent among patients with thalassaemia, is also associated with low BMD, potentially through its effects on osteoclast activity and on enzymes required for new bone formation. King JC. Am J Clin Nutr. 1996;64(3): Voskaridou et al. Br J Haematol. 2004;127(2):")
70
Oστεοπόρωση στη β-θαλασσαιμία και βιολογικός δρόμος RANKL/OPG (1)
Παράμετρος Ασθενείς (N=26) (μέση±SD) Μάρτυρες (N=30) p-value OPG (pmol/L) sRANKL (pmol/L) OPG/sRANKL 2,6±1,6 5,6±3,8 0,4±0,4 4,0±0,4 4,6±1,4 0,8±0,2 0,002 0,09 0,006 Voskaridou et al. Br J Haematol 2003;123:730-7
 (μέση±SD) Μάρτυρες. (N=30) p-value. OPG (pmol/L) sRANKL (pmol/L) OPG/sRANKL. 2,6±1,6. 5,6±3,8. 0,4±0,4. 4,0±0,4. 4,6±1,4. 0,8±0,2. 0,002. 0,09. 0,006. Voskaridou et al. Br J Haematol 2003;123:")
71
Oστεοπόρωση στη β-θαλασσαιμία και βιολογικός δρόμος RANKL/OPG (2)
Παράμετρος Ασθενείς (ν=54) (m±SD) Μάρτυρες p-value OPG (pmol/L) sRANKL (pmol/L) OPG/sRANKL 3,0±1,3 8,1±2,8 0,4±0,2 3,6±1,4 4,5±1,2 0,8±0,2 NS <0,0001 Ισχυρή συσχέτιση μεταξύ BMD ΟΜΣΣ και κεφαλής μηριαίου με OPG/sRANKL Morabito et al. J Βone Miner Res 2004;19:722-7
 (m±SD) Μάρτυρες. p-value. OPG (pmol/L) sRANKL (pmol/L) OPG/sRANKL. 3,0±1,3. 8,1±2,8. 0,4±0,2. 3,6±1,4. 4,5±1,2. 0,8±0,2. NS. <0,0001. Ισχυρή συσχέτιση μεταξύ BMD ΟΜΣΣ και κεφαλής μηριαίου. με OPG/sRANKL. Morabito et al. J Βone Miner Res 2004;19:")
72
Δείκτες οστικού μεταβολισμού στη ΜΘ
Παράμετρος Μάρτυρες (mean±S.D.) N=30 Ασθενείς N=26 p-value Δείκτες οστικής αποδόμησης NTX (nM BCE/mM creat.) D-PYR (pmol/mmol creat.) TRACP-5b (U/L) Δείκτες οστικής παραγωγής OC (ng/mL) bALP (IU/L) BMD (T-score) Lumbar spine Femoral neck Forearm 36.9±10.3 14.1±7.2 3.2±0.9 7.9±3.7 19.8±4.0 177.5±106.9 22.0±20.7 6.2±3.9 11.1±8.5 27.2±12.3 -2.58 ± -0.85 -1.70 ± -0.70 -3.28 ± -1.34 <0.001 0.04 0.032 <0.01 Voskaridou et al. Br J Haematol 2003;123:730-7
 N=30. Ασθενείς. N=26. p-value. Δείκτες οστικής αποδόμησης. NTX (nM BCE/mM creat.) D-PYR (pmol/mmol creat.) TRACP-5b (U/L) Δείκτες οστικής παραγωγής. OC (ng/mL) bALP (IU/L) BMD (T-score) Lumbar spine. Femoral neck. Forearm. 36.9± ± ± ± ± ± ± ± ± ± ± ± ± < <0.01. Voskaridou et al. Br J Haematol 2003;123:")
73
Dickkopf-1 στη Θαλασσαιμία
(n=22) (n=66) Voskaridou et al. Haematologica 2009;94:725-8
 (n=66) Voskaridou et al. Haematologica 2009;94:")
74
Σκληροστίνη και ΜΘ p<0.001
Voskaridou et al. Horm Metab Res 2012;44:909-13

75
ΖΟ στη ΜΘ ZOL q6m ZOL q3m 2 T-score –2 –4 –6 L1-L4 Baseline
–2 –4 –6 L1-L4 Baseline L1-L4 12 mo L1-L4 36 mo Femoral neck Baseline Femoral neck 12 mo Femoral neck 36 mo ZOL q6m ZOL q3m P = .02 P < .01 T-score The group treated with zoledronic acid every 6 months during the first year had shown a marginal improvement in lumbar spine and femoral neck BMD during treatment However, we now found that lumbar spine BMD was significantly improved at 36 months in this cohort As reported at 12 months’ follow-up, lumbar spine BMD was significantly increased compared with baseline in the group receiving zoledronic acid every 3 months At 36 months’ follow-up, this improvement was maintained In addition, femoral neck BMD continued to improve in this arm Femoral neck BMD at 36 months was significantly better than at 12 months Thus, zoledronic acid continues to provide anti-resorptive benefits for a prolonged period after completion of therapy Voskaridou E, et al. Haematologica. 2008;93(10):
:")
76
Συμπεράσματα για τη Θαλασσαιμία
H οστεοπόρωση στη θαλασσαιμία αποτελεί σημαντικό πρόβλημα για τους ασθενείς και η βιολογία της είναι πολυπαραγοντική Οι δείκτες οστικού μεταβολισμού χρησιμοποιούνται στην παρακολούθηση της αντι-οστεοπορωτικής αγωγής και επικουρούν τη μέτρηση της BMD, που αποτελεί την καλύτερη παράμετρο της αποτελεσματικότητοσ της αγωγής Η ανακάλυψη της εμπλοκής του βιολογικού δρόμου των RANK/RANKL/OPG και Wnt στην παθογένεια της οστικής απώλειας στη Θαλασσαιμία ανοίγουν το δρόμο για τη χρήση νεότερων φαρμάκων (αντι-RANKL, αντι-Dkk1) και σε συνδυασμό με τις μέχρι σήμερα καθιερωμένες θεραπείες μπορεί να βοηθήσουν σημαντικά στην αντιμετώπιση της οστικής απώλειας στη Θαλασσαιμία
 και σε συνδυασμό με τις μέχρι σήμερα καθιερωμένες θεραπείες μπορεί να βοηθήσουν σημαντικά στην αντιμετώπιση της οστικής απώλειας στη Θαλασσαιμία.")
77
Άλλα Αιματολογικά Νοσήματα και Οστεοπόρωση

78
Αιμορροφιλία και οστεοπόρωση (1)
20 40 60 80 normal osteopenia osteoporosis Femoral neck Total clinical score Total radiological score 50%-60% N=90 Katsarou et al. Ann Hematol 2010;89:67-74

79
N=35 (39%) FN LS Percent HIV - negative HIV - positive Percent 25 50
24.39 31.71 43.9 29.03 70.97 25 50 75 100 normal osteopenia osteoporosis HIV - negative HIV - positive Percent FN N=35 (39%) 50 42.86 7.143 15.15 63.64 21.21 25 75 100 normal osteopenia osteoporosis HIV - negative HIV - positive Percent LS
 normal. osteopenia. osteoporosis. HIV - negative. HIV - positive. Percent. LS.")
80
Αιμορροφιλία και οστεοπόρωση (2)
Μάρτυρες Ασθενείς NTX (nM BCE/mM creatinine) 19,4 (15,4-24) 16,1 (12,1-20,4) 0,018 CTX (ng/ml) 0,61 (0,45-0,86) 0,47 (0,40-0,58) 0,028 TRAPC-5b(U/L) 2,75 (2,21-3,32) 1,38 (1,14-1,63) <0,001 OC (ng/mL) 14,19 (8,73-18,59) 15,72 (13,08-20,98) 0,023 bAPL (U/L) 20,07 (14,52-25,88) 16,97 (12,32-21,71) 0,043
 19,4 (15,4-24) 16,1 (12,1-20,4) 0,018. CTX (ng/ml) 0,61 (0,45-0,86) 0,47 (0,40-0,58) 0,028. TRAPC-5b(U/L) 2,75 (2,21-3,32) 1,38 (1,14-1,63) <0,001. OC (ng/mL) 14,19 (8,73-18,59) 15,72 (13,08-20,98) 0,023. bAPL (U/L) 20,07 (14,52-25,88) 16,97 (12,32-21,71) 0,043.")
81
Λέμφωμα και Οστεοπόρωση μετά Θεραπεία
Ν=66 με DLBCL μετά 6 R-CHOP

82
RANKL: βασικό μόριο στην οστεοπόρωση που σχετίζεται με τα στεροειδή
Τα στεροειδή αυξάνουν την παραγωγή RANKL κι ελαττώνουν την παραγωγή OPG από τους οστεοβλάστες. Αυξάνουν την παραγωγή Dkk-1 και μειώνουν τη δράση των οστεοβλαστών Glucocorticoid-induced osteoporosis is a common and serious complication of systemic glucocorticoid use, and represents the most prevalent form of secondary osteoporosis.1 Glucocorticoid-induced osteoporosis is characterized by increased bone resorption and decreased bone formation.2 Glucocorticoid exposure enhances RANK Ligand expression and inhibits OPG production by osteoblasts3, and it also suppresses OPG serum levels in vivo, thus elevating the RANK Ligand/OPG ratio.4 An elevated RANK Ligand/OPG ratio within the skeleton promotes bone loss, by increasing osteoclast activation and bone resorption. Lukert B, et al. Glucocorticoid-induced Osteoporosis: Pathogenesis and Management. Ann Intern Med. 1990;112:352–64 Hofbauer LC, Schoppet M. Clinical Implications of the Osteoprotegerin/RANKL/RANK System for Bone and Vascular Diseases. JAMA. 2004;292:490-5. Hofbauer LC, et al. Stimulation of Osteoprotegerin Ligand and Inhibition of Osteoprotegerin Production by Glucocorticoids in Human Osteoblastic Lineage Cells. Endocrinol. 1999;140: Sasaki N, et al. Glucocorticoid Decreases Circulating Osteoprotegerin (OPG). Nephrol Dial Transplant. 2001;16: RANK Ligand Αυξημένη οστεοκλαστική δραστηριότητα = OPG
. Nephrol Dial Transplant. 2001;16: RANK Ligand. Αυξημένη οστεοκλαστική. δραστηριότητα. = OPG.")
83
Συμπεράσματα Tα οστικά κύτταρα επηρεάζονται από κυτταροκίνες που παράγονται από λεμφοκύτταρα, μακροφάγα και πλασματοκύτταρα. Η ανακάλυψη του βιολογικού δρόμου των RANK/RANKL/OPG και Wnt απέδειξε τη συσχέτιση μεταξύ ανοσολογικής απάντησης και οστικού μεταβολισμού στην παθογένεια των οστικών μεταστάσεων, αυτοάνοσων νοσημάτων και αιματολογικών νόσων με οστική συμμετοχή, όπως το μυέλωμα, η θαλασσαιμία και η αιμορροφιλία. Χημειοθεραπεία σχετίζεται με απώλεια οστικής μάζας στα λεμφώματα Nεότερα φάρμακα παρασκευάζονται στοχεύοντας τα μόρια αυτά (denosumab, BHQ880, romosozumab).
.")
84
Σας ευχαριστώ πολύ

Παρόμοιες παρουσιάσεις


 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")


















