Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Επ.Καθ. Παθολογίας Λοιμώξεων ΕΚΠΑ
ΚΛΙΝΙΚΟ ΦΡΟΝΤΙΣΤΗΡΙΟ Ενδονοσοκομειακές Λοιμώξεις Διαχείριση Αντιβιοτικών Μαρία Σουλή Επ.Καθ. Παθολογίας Λοιμώξεων ΕΚΠΑ ΠΓΝ ΑΤΤΙΚΟΝ

2
“Drug resistance follows the drug like a faithful shadow.”
- Paul Erhlich Πολύ προφητικά τα λόγια του …Erhlich, a German-born physician and scientist in the fields of hematology, immunology, and chemotherapy and Nobel Prize winner in 1908, recognized early on that drug-resistance was a complicating issue when treating certain disease states. Now, although his statement of “Drug Resistance follows the drug like a faithful shadow” was more relevant at that time to cancer-chemotherapy, he recognized this as being important for antimicrobial therapy as well – he originally discovered Arsphenamine, or Salvarsan, the first known medical treatment of syphilis. Δεν αναφερονται μόνο στα αντιβιοτικα που δεν είχαν ακόμα ανακαλυφθεί - πολλα κοινα χαρακτηριστικα Η αντοχή στη δραση του φαρμάκου το ακολουθει πιστα σαν να είναι η σκια του

3
Το ίδιο πίστευε και ο Φλεμινγκ, ο πατερας της πενικιλλίνης
Το ίδιο πίστευε και ο Φλεμινγκ, ο πατερας της πενικιλλίνης. What premonitions both of these gentlemen had! Drs. Ehrilich and Fleming had envisioned the development of antibiotic resistance that would follow the discovery of each class of antibiotics as you can see on this timeline through out the past 80 years or so. In a Science magazine article published in 1992, it is estimated that for the seven major classes of known antibiotics, resistance has developed within 1–4 years from the time of clinical introduction of the drug.χρονοδιαγραμμα Nature Reviews: Drug Discovery. 2007: 6; 8-12.

4
ANTIBIOTIKA FACTS >30-50% των νοσηλευομένων ασθενών λαμβάνουν αντιβιοτικά Για 50% αντιβιοτικών στους νοσηλευόμενους ασθενείς η χρήση τους κρίνεται ακατάλληλη (ένδειξη, επιλογή, δοσολογία, διάρκεια) Η υπερκατανάλωση αντιβιοτικών είναι ο κυριότερος παράγων κινδύνου της μικροβιακής αντοχής Η χρήση αντιβιοτικών είναι ο κυριότερος παράγων κινδύνου για λοίμωξη από C.difficile Σε ΗΠΑ και Ευρωπη Up to 85% of patients with CDAD have antibiotic exposure in the 28 days before infection (Chang HT ICHE 2007)
 Η υπερκατανάλωση αντιβιοτικών είναι ο κυριότερος παράγων κινδύνου της μικροβιακής αντοχής. Η χρήση αντιβιοτικών είναι ο κυριότερος παράγων κινδύνου για λοίμωξη από C.difficile. Σε ΗΠΑ και Ευρωπη. Up to 85% of patients with CDAD have antibiotic exposure in the 28 days before infection (Chang HT ICHE 2007)")
5
Κατανάλωση Αντιβιοτικών και Μικροβιακή Αντοχή
Παθογόνο και Είδος αντιβιοτικού Αύξηση κινδύνου Εντεροβακτηριακά Carb-R & Καρβαπενέμες 15 x Ψευδομονάδα Carb-R & Καρβαπενέμες 7 x Εντεροβακτηριακά που παράγουν ESBL & Κεφαλοσπορίνες 6-29 x K.pneunoniae COL-R & Κολιμυκίνη 5 x Σε όλες τις μελέτες η προηγούμενη χρήση αντιβιοτικών αναγνωρίζεται ως σημαντικος παραγοντας κινδύνου για λοίμωξη από ανθεκτικα παθογόνα Patel G Infect Control Hosp Epidemiol 2008;29:1099 Zaoutis TE Pediatrics 2005;114:942 Talon D Clin Microbiol Infect 2000;6:376 Kontopidou F Clin Microbiol Infect 2011; 17:E9 Voor in ‘t holt A AAC 2014

6
Κατανάλωση Αντιβιοτικών και Μικροβιακή Αντοχή
Annual prevalence of imipenem resistance among P. aeruginosa isolates in 45 long-term acute care hospitals (LTACHs) during 2002 and/or 2003, according to the rate of carbapenem use (rp0.41; Pp.004). Gould et al. ICHE 2006 Kim et al. JID 1999 Antoniadou et al. JAC 2006
 during 2002 and/or 2003, according to the rate of carbapenem use (rp0.41; Pp.004). Gould et al. ICHE Kim et al. JID Antoniadou et al. JAC")
7
Κατανάλωση Αντιβιοτικών και Μικροβιακή Αντοχή
Antibiotic Use and Antibiotic Resistance Rates for Methicillin-Resistant S. aureus and Carbapenemase-Producing Klebsiella Bacteremia Isolates Pathogen Country Antibiotic Usage* (DDDs/1000 inhabitants) Rate of Resistance* K.pneumoniae Greece The Netherlands 38 11 38% 0.2% MRSA 51% 1.6% * Data for Bartlett JG et al. Clin Infect Dis 2013
 Rate of Resistance* K.pneumoniae. Greece. The Netherlands % 0.2% MRSA. 51% 1.6% * Data for Bartlett JG et al. Clin Infect Dis")
8
Αυξημένη πιθανότητα θανάτου Μεγαλύτερη διάρκεια νοσηλείας
Αυξημένο κόστος νοσηλείας Οι επιπτωσεις της ΜΑ είναι σοβαρες και για τον ασθενη και για το Σ Υγειας

9
The total economic cost of antibiotic resistance to the U. S
The total economic cost of antibiotic resistance to the U.S.economy: $20 billion in excess direct healthcare costs, with additional costs to society for lost productivity as high as $35 billion a year Το κοστος για την αμερικανικη οικονομια από τα πολυανθεκτικα ανερχεται σε ….για την παροχη υπηρεσιων υγειας και επιπλεον …για την απωλεια παραγωγικοτητας

10
Of those deaths, two-thirds are due to Gram-negative bacteria
Each year, patients die from an infection caused by MDR bacteria Of those deaths, two-thirds are due to Gram-negative bacteria Infections due MDR bacteria resulted in approximately 2.5 million extra hospital days As a comparison, each year in the EU, about persons are killed in a road accident Τελικός Απολογισμός στην ΕΕ… αυξηση της διαρκειας νοσηλειας κατά

11
Campaign to Prevent Antimicrobial Resistance in Healthcare Settings
Directed Rx Less antibiotics Στρατηγική 4 βασικοι πυλώνες Μειωση επιπτωσης λοιμωξεων συνεπαγεται μειωση της αναγκης χορηγησης αντιβιοτικων Χρηση των αντιβιοτικων με Συνεση Σωστή και εγκαιρη διαγνωση ώστε η χρηση αντιβιοτικων να είναι Κατευθυνομενη και όχι εμπειρικη Προληψη της διασπορας της αντοχης με την εφαρμογη της υγιεινης των χεριων και Wisely Hand Hygiene

12
SIDP, APUA, CDC, WHO endorsed
Clin Infect Dis 2007, 2011

14
Antibiotic Stewardship : Ορισμός
Πρόγραμμα συντονισμένων παρεμβάσεων για την παρακολούθηση και βελτίωση της χρήσης των αντιβιοτικών Προωθεί την επιλογή του κατάλληλου αντιμικροβιακού (είδος, δόση, χρόνος έναρξης, διάρκεια και οδός χορήγησης) Σκοπός: το βέλτιστο κλινικό αποτέλεσμα, η ελάχιστη τοξικότητα, η ελάχιστη πίεση επιλογής στις χλωρίδες (αποφυγή της μικροβιακής αντοχής) και η μείωση του κόστους Τρεχων ορισμός Antimicrobial stewardship refers to coordinated interventions designed to improve and measure the appropriate use of antimicrobial agents by promoting the selection of the optimal antimicrobial drug regimen including dosing, duration of therapy, and route of administration. The major objectives of antimicrobial stewardship are to achieve best clinical outcomes related to antimicrobial use while minimizing toxicity and other adverse events, thereby limiting the selective pressure on bacterial populations that drives the emergence of antimicrobial-resistant strains. Antimicrobial stewardship may also reduce excessive costs attributable to suboptimal antimicrobial use. Εχει σχεδιαστεί ώστε … Εκθετοντας τον ασθενή στην ελαχιστη δυνατη τοξικοτητα Μειωση κόστους από την ακαταλληλη χρήση αντιβιοτικων SHEA/ IDSA/ PIDS Policy Statement 2012
 Σκοπός: το βέλτιστο κλινικό αποτέλεσμα, η ελάχιστη τοξικότητα, η ελάχιστη πίεση επιλογής στις χλωρίδες (αποφυγή της μικροβιακής αντοχής) και η μείωση του κόστους. Τρεχων ορισμός. Antimicrobial stewardship refers to coordinated interventions designed to improve and measure the appropriate use of antimicrobial. agents by promoting the selection of the optimal antimicrobial drug regimen including dosing, duration of therapy, and route of administration. The major objectives of antimicrobial stewardship are to achieve best clinical outcomes related to antimicrobial use while minimizing toxicity and other adverse events, thereby limiting the selective pressure on bacterial populations that drives the emergence of antimicrobial-resistant strains. Antimicrobial stewardship. may also reduce excessive costs attributable to suboptimal antimicrobial use. Εχει σχεδιαστεί ώστε … Εκθετοντας τον ασθενή στην ελαχιστη δυνατη τοξικοτητα. Μειωση κόστους από την ακαταλληλη χρήση αντιβιοτικων. SHEA/ IDSA/ PIDS Policy Statement")
15
Antibiotic Stewardship Programs (ASP): Προϋποθέσεις
Ομάδα Διαχείρισης Αντιβιοτικών Λοιμωξιολόγος Κλινικός Μικροβιολόγος Κλινικός Φαρμακοποιός Επιδημιολόγος Τα μέλη της πρέπει να έχουν εκπαιδευθεί στη Διαχείριση Αντιβιοτικών H ομάδα θεωρείται τμήμα της λειτουργίας του ιατρικού τμήματος και διευθύνεται από τον Λοιμωξιολόγο Ελαχιστες Προϋποθέσεις Creation of a multidisciplinary interprofessional antimicrobial stewardship team that is physician directed or supervised (coordinated). Πυρήνας της ομάδας At a minimum, 1 or more members of the team should have training in antimicrobial stewardship-inclusion of an IT is optimal number of team members may vary on the basis of the size and complexity of the facility They should be compensated for their time!! ASP is an important component of patient safety SHEA/ IDSA/ PIDS Policy Statement 2012
. Πυρήνας της ομάδας. At a minimum, 1 or more members of the team should have training in antimicrobial stewardship-inclusion of an IT is optimal. number of team members may vary on the basis of the size and complexity of the facility. They should be compensated for their time!! ASP is an important component of patient safety. SHEA/ IDSA/ PIDS Policy Statement")
16
Owens R. Diagn Microbiol Infect Dis 2008
Τμήματα όπως Συνεργάζεται με το τμήμα του Infection Control και την ομάδα των λοιμωξιολόγων που κάνει τη συμβουλευτική στα τμήματα, με το φαρμακείο και την επιτροπή φαρμάκων του νοσοκομείου (ΑΙΙΙ) Owens R. Diagn Microbiol Infect Dis 2008
 Owens R. Diagn Microbiol Infect Dis")
17
Antibiotic Stewardship Programs (ASP) : IDSA guidelines
Η ομάδα λειτουργεί στα πλαίσια του Quality Assurance και της ασφάλειας των ασθενών (ΑΙΙΙ) Είναι σημαντικό να έχει την υποστήριξη της διοίκησης στην εξασφάλιση υποδομών και εξουσιοδότησης (ΑΙΙΙ) Το σχέδιο δράσης που θα προτείνει πρέπει να έχει την έγκριση της Διοίκησης, των διευθυντών των τμημάτων και του λοιπού ιατρικού προσωπικού ώστε να εξασφαλισθεί η συνεργασία τους Ποιοτητα παρεχομενων υπηρεσιων υγειας appropriate use of antimicrobial agents has become a focus of patient safety and quality assurance along with medication errors, allergy identification, and drug-drug interactions Prior to program implementation, the antimicrobial stewardship strategic plan should be presented to and approved by the chiefs of professional services, hospital medical staff executive committee, and/or other medical staff governing bodies, to ensure their acceptance and support
 Είναι σημαντικό να έχει την υποστήριξη της διοίκησης στην εξασφάλιση υποδομών και εξουσιοδότησης (ΑΙΙΙ) Το σχέδιο δράσης που θα προτείνει πρέπει να έχει την έγκριση της Διοίκησης, των διευθυντών των τμημάτων και του λοιπού ιατρικού προσωπικού ώστε να εξασφαλισθεί η συνεργασία τους. Ποιοτητα παρεχομενων υπηρεσιων υγειας. appropriate use of antimicrobial agents has become a focus of patient safety and quality assurance. along with medication errors, allergy identification, and drug-drug interactions. Prior to program implementation, the antimicrobial stewardship. strategic plan should be presented to and approved by the chiefs. of professional services, hospital medical staff executive committee, and/or other medical staff governing bodies, to ensure their acceptance and support.")
18
Antibiotic Stewardship Programs (ASP): Προϋποθέσεις
Κατευθυντήριες Οδηγίες Βασίζονται σε εθνικά ή τοπικά δεδομένα αντοχής και επιδημιολογίας και σε δεδομένα από αξιόπιστες κλινικές μελέτες (evidence-based) Διαμορφώνονται από ομάδα ειδικών ώστε να είναι «κοινής αποδοχής» RCT απέδειξαν μείωση κατανάλωσης αντιβιοτικών, διάρκειας i.v. αγωγής, διάρκεια νοσηλείας, χωρίς αύξηση θνητότητας ή επιπλοκών από την εφαρμογή τους Ποτέ δεν είναι η μοναδική παρέμβαση Δεν γνωρίζουμε την συμβολή τους στην μείωση της αντοχής Περιορισμός για την ευρεία εφαρμογή τους είναι ότι δεν προβλέπεται στρατηγική ελέγχου! Πρέπει να εξασφαλίζεται feed-back προς την ομάδα στην οποία απευθύνονται (κατανάλωση αντιβιοτικών, έκβαση ασθενών, quality indicators…) Institutional guidelines (κανονες συνταγογραφησης σε επίπεδο ιδρύματος) for the management of common infection syndromes-κλινικα μονοπατια (clinical pathways για διαγνωση θεραπεια και διαρκεια) ΟΔΗΓΙΕΣ=Although physicians usually agree, in principle, with national guidelines, the absence of accompanying strategies for local implementation often presents a formidable barrier, Antimicrobial stewardship programs can facilitate multidisciplinary development of evidence-based practice guidelines that incorporate local microbiology and resistance patterns. Απουσια δεδομενων δεν σημαινει απουσια αποτελεσματος SHEA/ IDSA/ PIDS Policy Statement 2012
 Διαμορφώνονται από ομάδα ειδικών ώστε να είναι «κοινής αποδοχής» RCT απέδειξαν μείωση κατανάλωσης αντιβιοτικών, διάρκειας i.v. αγωγής, διάρκεια νοσηλείας, χωρίς αύξηση θνητότητας ή επιπλοκών από την εφαρμογή τους. Ποτέ δεν είναι η μοναδική παρέμβαση. Δεν γνωρίζουμε την συμβολή τους στην μείωση της αντοχής. Περιορισμός για την ευρεία εφαρμογή τους είναι ότι δεν προβλέπεται στρατηγική ελέγχου! Πρέπει να εξασφαλίζεται feed-back προς την ομάδα στην οποία απευθύνονται (κατανάλωση αντιβιοτικών, έκβαση ασθενών, quality indicators…) Institutional guidelines (κανονες συνταγογραφησης σε επίπεδο ιδρύματος) for the management of common infection syndromes-κλινικα μονοπατια (clinical pathways για διαγνωση θεραπεια και διαρκεια) ΟΔΗΓΙΕΣ=Although physicians usually agree, in principle, with national guidelines, the absence of accompanying strategies for local implementation often presents a formidable barrier, Antimicrobial stewardship programs can facilitate multidisciplinary development of evidence-based practice guidelines that incorporate local microbiology and resistance patterns. Απουσια δεδομενων δεν σημαινει απουσια αποτελεσματος. SHEA/ IDSA/ PIDS Policy Statement")
19
Antibiotic Stewardship Programs (ASP): Προϋποθέσεις
Σχεδιασμός παρεμβάσεων για τον περιορισμό • της άσκοπης χρήσης συνδυασμού αντιβιοτικών (μόνο σε αυστηρά καθορισμένες ενδείξεις !!) • της χρήσης ευρέως φάσματος αντιβιοτικών αναιτιολόγητα • της χρήσης αντιβιοτικών για μη λοιμώδη σύνδρομα • της χρήσης αντιβιοτικών για τη θεραπεία του «αποικισμού» A formulary limited to non-duplicative antibiotics with demonstrated clinical need Συνδυασμοί αντιβιοτικών: συστήνονται στην αρχική εμπειρική κάλυψη στους βαρέως πάσχοντες με παράγοντες κινδύνου για λοίμωξη από MDR για διεύρυνση φάσματος (AII)-δεν συστήνονται για πρόληψη αντοχής (ανεπαρκή δεδομένα για τα περισσότερα παθογόνα-CII) Multidrug regimens with unnecessarily redundant antimicrobial spectra. • Antibiotic therapy for the management of nonbacterial syndromes or cultures that represent contamination or routine colonization. • Empiric regimens that are either inadequately or excessively broad spectrum for infection syndromes. • Regimens that do not adequately treat infections caused by culture-confirmed pathogens. SHEA/ IDSA/ PIDS Policy Statement 2012
 • της χρήσης ευρέως φάσματος αντιβιοτικών αναιτιολόγητα. • της χρήσης αντιβιοτικών για μη λοιμώδη σύνδρομα. • της χρήσης αντιβιοτικών για τη θεραπεία του «αποικισμού» A formulary limited to non-duplicative antibiotics with demonstrated clinical need. Συνδυασμοί αντιβιοτικών: συστήνονται στην αρχική εμπειρική κάλυψη στους βαρέως πάσχοντες με παράγοντες κινδύνου για λοίμωξη από MDR για διεύρυνση φάσματος (AII)-δεν συστήνονται για πρόληψη αντοχής (ανεπαρκή δεδομένα για τα περισσότερα παθογόνα-CII) Multidrug regimens with unnecessarily redundant antimicrobial spectra. • Antibiotic therapy for the management of nonbacterial syndromes or cultures that represent contamination or routine colonization. • Empiric regimens that are either inadequately or excessively broad spectrum for infection syndromes. • Regimens that do not adequately treat infections caused by culture-confirmed pathogens. SHEA/ IDSA/ PIDS Policy Statement")
20
Antibiotic Stewardship Programs (ASP): Προϋποθέσεις
Περιορισμένο Αντιβιόγραμμα Παρακολούθηση της κατανάλωσης αντιβιοτικών Παρακολούθηση των ποσοστών αντοχής Προοπτική επιτήρηση και συγχρόνως παρέμβαση για την ακατάλληλη χρήση αντιβιοτικών Δυνατότητα παρακολουθησης και … Ανα τακτα χρονικα διαστηματα για την γνωση της επιδημιολογιας στο κάθε νοσοκομειο Εθνικη καταναλωση και εθνικα ποσοστα αντοχης SHEA/ IDSA/ PIDS Policy Statement 2012

21
Prospective audit with intervention and feedback (AI)
Antibiotic Stewardship Programs (ASP) : IDSA guidelines Εφαρμογή: Υπάρχουν δυο προτεινόμενες στρατηγικές Καθημερινά έλεγχος των συνταγών αντιβιοτικών. Αν υπάρχουν παρατηρήσεις γίνεται παρέμβαση είτε με συζήτηση, είτε τηλεφωνικά είτε με σημείωση στο φάκελο του ασθενούς είτε ηλεκτρονικά Prospective audit with intervention and feedback (AI) Για να χορηγηθεί αντιβιοτικό εκτός του περιορισμένου αντιβιογράμματος χρειάζεται «εξουσιοδότηση» ή αιτιολόγηση και έγκριση από τον λοιμωξιολόγο Formulary restriction and preauthorization (AII) Μπορεί να συνδυάζονται 1) Academic detailing – κάθε περιπτωση ασθενους συζητειται χωριστα με ατομο της ομαδας αντιβιοτικων που είναι ειδικα εκπαιδευμενος Σε μικροτερα νοσοκομεια που δεν μπορει αυτό να γινει καθημερινα εχει δειχθει σε κλινικη μελετη ότι αρκει ο ελεγχος 3 φορες την εβδομαδα (3 days per week to review patients receiving multiple, prolonged, or high-cost courses of antimicrobial Therapy) 2) Για συγκεκριμενα ‘προωθημενα’ αντιβιοτικα (μπαινουν σε απολυτο περιορισμό) μονο οποιος εχει εξουσιοδοτηση ή εφόσον υπάρχει ατιολόγηση και γραπτή έγκριση… Antibiotics may be prescribed only: • For certain approved clinical indications • By certain physicians (i.e., infectious diseases specialists)
 : IDSA guidelines. Εφαρμογή: Υπάρχουν δυο προτεινόμενες στρατηγικές. Καθημερινά έλεγχος των συνταγών αντιβιοτικών. Αν υπάρχουν παρατηρήσεις γίνεται παρέμβαση είτε με συζήτηση, είτε τηλεφωνικά είτε με σημείωση στο φάκελο του ασθενούς είτε ηλεκτρονικά. Prospective audit with intervention and feedback (AI) Για να χορηγηθεί αντιβιοτικό εκτός του περιορισμένου αντιβιογράμματος χρειάζεται «εξουσιοδότηση» ή αιτιολόγηση και έγκριση από τον λοιμωξιολόγο. Formulary restriction and preauthorization (AII) Μπορεί να συνδυάζονται. 1) Academic detailing – κάθε περιπτωση ασθενους συζητειται χωριστα με ατομο της ομαδας αντιβιοτικων που είναι ειδικα εκπαιδευμενος. Σε μικροτερα νοσοκομεια που δεν μπορει αυτό να γινει καθημερινα εχει δειχθει σε κλινικη μελετη ότι αρκει ο ελεγχος 3 φορες την εβδομαδα (3 days per week to review patients receiving multiple, prolonged, or high-cost courses of antimicrobial Therapy) 2) Για συγκεκριμενα ‘προωθημενα’ αντιβιοτικα (μπαινουν σε απολυτο περιορισμό) μονο οποιος εχει εξουσιοδοτηση ή εφόσον υπάρχει ατιολόγηση και γραπτή έγκριση… Antibiotics may be prescribed only: • For certain approved clinical indications. • By certain physicians (i.e., infectious diseases specialists)")
22
Prospective audit with intervention and feedback (AI)
Antibiotic Stewardship Programs (ASP) : IDSA guidelines Πλεονεκτήματα - Μειονεκτήματα Ο γιατρός διατηρεί την αυτονομία του-εθελοντική η εφαρμογή των συστάσεων Έγκαιρη έναρξη εμπειρικής/κατάλληλης αγωγής Εκπαιδευτικός χαρακτήρας Δίνει κίνητρο Απαιτεί «εργατικό δυναμικό» και χρόνο Prospective audit with intervention and feedback (AI) Απώλεια αυτονομίας του θεράποντος Διαταραχή σχέσεων Καθυστέρηση στην έναρξη κατάλληλης αγωγής Περιορισμός ενός αντιβιοτικού οδηγεί σε υπερ-συνταγογράφηση κάποιου άλλου Η επιτυχία εξαρτάται από το «ποιος» δίνει την έγκριση Formulary restriction and preauthorization (AII) Squeezing the resistance balloon Μελετες εδειξαν την μειωση χρησης και της αντοχής στο υπο περιορισμον αντιβιοτικο και αύξηση της αντοχής σε καποιο άλλο (πχ κεφταζιντιμη – καρβαπενεμη) Τα αποτελεσματα εξαρτωνται σημαντικα από το ποιος μπορει να δωσει τη σχετικη εγκριση πχ ο εξειδικευομενος ή ο ειδικος λοιμωξιολογος (ποιος εχει επιφορτιστει) 2) Αμεσος και απολυτος ελεγχος στα αντιβιοτικα, πρεπει να υπαρχει προβλεψη για τις εκτος ωραριου αναγκες εγκρισης (αν το αντιβιοτικο ζητηθει εκτος ωραριου ή σε αργιες)
 : IDSA guidelines. Πλεονεκτήματα - Μειονεκτήματα. Ο γιατρός διατηρεί την αυτονομία του-εθελοντική η εφαρμογή των συστάσεων. Έγκαιρη έναρξη εμπειρικής/κατάλληλης αγωγής. Εκπαιδευτικός χαρακτήρας. Δίνει κίνητρο. Απαιτεί «εργατικό δυναμικό» και χρόνο. Prospective audit with intervention and feedback (AI) Απώλεια αυτονομίας του θεράποντος. Διαταραχή σχέσεων. Καθυστέρηση στην έναρξη κατάλληλης αγωγής. Περιορισμός ενός αντιβιοτικού οδηγεί σε υπερ-συνταγογράφηση κάποιου άλλου. Η επιτυχία εξαρτάται από το «ποιος» δίνει την έγκριση. Formulary restriction and preauthorization (AII) Squeezing the resistance balloon. Μελετες εδειξαν την μειωση χρησης και της αντοχής στο υπο περιορισμον αντιβιοτικο και αύξηση της αντοχής σε καποιο άλλο (πχ κεφταζιντιμη – καρβαπενεμη) Τα αποτελεσματα εξαρτωνται σημαντικα από το ποιος μπορει να δωσει τη σχετικη εγκριση πχ ο εξειδικευομενος ή ο ειδικος λοιμωξιολογος (ποιος εχει επιφορτιστει) 2) Αμεσος και απολυτος ελεγχος στα αντιβιοτικα, πρεπει να υπαρχει προβλεψη για τις εκτος ωραριου αναγκες εγκρισης (αν το αντιβιοτικο ζητηθει εκτος ωραριου ή σε αργιες)")
23
Prospective audit with intervention and feedback (ΑΙ)
Αρκετές συγκριτικές προοπτικές κλινικές μελέτες έχουν δείξει μείωση της κατανάλωσης αντιβιοτικών (20-50%), βελτίωση της χρήσης αντιβιοτικών και μείωση του κόστους φαρμάκων χωρίς αύξηση θνητότητας ή υποτροπής της λοίμωξης Λιγότερες μελέτες έχουν δείξει παράλληλα και μείωση της αντοχής (ειδικά των Gram αρνητικών) και μείωση της συχνότητας του C.difficile Αποκλιμάκωση σε αντιβιοτικά στενότερου εύρους ή p.os αγωγή Kαλή αποδοχή και συμμόρφωση με τις συστάσεις, manpower & labor- intensive Αποδεδειγμενα από τυχαιοποιημενες κλινικες μελετες μειωνει την ασκοπη χρήση αντιβιοτικών, βελτιωνει τη χρήση των αντιβιοτικων ως προς ειδος-διαρκεια-οδο χορηγησης-ελεγχο τοξικοτητας και αλληλεπιδρασεων και μειωνει το κοστος της νοσηλειας χωρις αυξηση θνητοτητας ή υποτροπης της λοιμωξης στην ομάδα της παρεμβασης και μειωση της επιπτωσης C.difficile Απαιτει περισσότερο εργατικό δυναμικο (labor intensive) Often physicians may be uncomfortable with making recommendations without laying eyes on the patients in question Fraser et al, Arch Intern Med 1997; Shrivasan et al, Arch Intern Med 2004; Bantar et al, CID 2003; Ruttiman et al, CID 2004; Carling et al, ICHE 2003; LaRocco et al, CID 2003
, βελτίωση της χρήσης αντιβιοτικών και μείωση του κόστους φαρμάκων χωρίς αύξηση θνητότητας ή υποτροπής της λοίμωξης. Λιγότερες μελέτες έχουν δείξει παράλληλα και μείωση της αντοχής (ειδικά των Gram αρνητικών) και μείωση της συχνότητας του C.difficile. Αποκλιμάκωση σε αντιβιοτικά στενότερου εύρους ή p.os αγωγή. Kαλή αποδοχή και συμμόρφωση με τις συστάσεις, manpower & labor- intensive. Αποδεδειγμενα από τυχαιοποιημενες κλινικες μελετες μειωνει την ασκοπη χρήση αντιβιοτικών, βελτιωνει τη χρήση των αντιβιοτικων ως προς ειδος-διαρκεια-οδο χορηγησης-ελεγχο τοξικοτητας και αλληλεπιδρασεων και μειωνει το κοστος της νοσηλειας χωρις αυξηση θνητοτητας ή υποτροπης της λοιμωξης στην ομάδα της παρεμβασης και μειωση της επιπτωσης C.difficile. Απαιτει περισσότερο εργατικό δυναμικο (labor intensive) Often physicians may be uncomfortable with making recommendations without laying eyes on the patients in question. Fraser et al, Arch Intern Med 1997; Shrivasan et al, Arch Intern Med 2004; Bantar et al, CID 2003; Ruttiman et al, CID 2004; Carling et al, ICHE 2003; LaRocco et al, CID")
24
Formulary restriction and preauthorization (AII)
Προοπτικές μελέτες έχουν δείξει ότι η εφαρμογή της προέγκρισης και του περιορισμένου αντιβιογράμματος οδηγεί σε μείωση της κατανάλωσης αντιβιοτικών και του κόστους αλλά τα αποτελέσματα ως προς τη μείωση της αντοχής δεν είναι τόσο ξεκάθαρα Η πλήρης απαγόρευση μιας ομάδας αντιβιοτικών μπορεί να οδηγήσει σε αντισταθμιστική αύξηση της κατανάλωσης και αντοχής σε άλλη ομάδα αντιβιοτικών (Squeezing the Resistance Balloon Effect) Συχνά μέτρο ελέγχου επιδημίας Η επιδραση στην αντοχη ήταν βραχυχρόνια και όχι σε όλες τις μελετες (σε μερικες αυξηση της αντοχης) Τα αποτελεσματα του ως προς τη μείωση της αντοχής δεν είναι τοσο ξεκαθαρα από τις υπαρχουσες κλινικες μελετες ‘squeezing the balloon’ effect, whereby reduction in resistance to the first class is simply replaced by resistance to the second class A restricted formulary should combine restriction of “high resistance potential antibiotics” with the unrestricted use of “low resistance potential antibiotics” Coleman et al, Am J Med 1991; Rahal et al, JAMA 1998; White et al, CID1997; Gross et al CID 2001
 Συχνά μέτρο ελέγχου επιδημίας. Η επιδραση στην αντοχη ήταν βραχυχρόνια και όχι σε όλες τις μελετες (σε μερικες αυξηση της αντοχης) Τα αποτελεσματα του ως προς τη μείωση της αντοχής δεν είναι τοσο ξεκαθαρα από τις υπαρχουσες κλινικες μελετες. ‘squeezing the balloon’ effect, whereby reduction in resistance to the first class is simply replaced by resistance to the second class. A restricted formulary should combine restriction of high resistance potential. antibiotics with the unrestricted use of low resistance potential antibiotics Coleman et al, Am J Med 1991; Rahal et al, JAMA 1998; White et al, CID1997; Gross et al CID")
25
Συμπληρωματικές στρατηγικές
Antibiotic Stewardship Programs (ASP) : IDSA guidelines Συμπληρωματικές στρατηγικές Εγκαιρη μετάβαση από i.v. σε p.os θεραπεία (ΑΙ) Αποκλιμάκωση με βάση τα αποτελέσματα των κ/ων (μείωση κατανάλωσης αντιβιοτικών, ανεπιθύμητων ενεργειών και κόστους-ΑΙΙ) Βελτίωση της δοσολογίας με εφαρμογή των δεδομένων PK-PD (ΑΙΙ) This can result in reduced length of hospital stay, health care costs, and potential complications due to intravenous access., με βαση κλινικα κριτηρια εφοσον υπαρχουν εναλλακτικα φαρμακα με καλη βιοδιαθεσιμοτητα Στοχευμενη θεραπεια (e.g., age, renal function, and weight), causative organism and site of infection (e.g., endocarditis, meningitis, and osteomyelitis) Βανκομυκινη, κολιμυκινη, β-λακταμες παρατεταμενη εγχυση, μια φορα/ημ αμινογλυκοσιδες Για να εξασφαλίσθει η καταλληλότητα της αρχικης εμπειρικης θεραπειας
 : IDSA guidelines. Συμπληρωματικές στρατηγικές. Εγκαιρη μετάβαση από i.v. σε p.os θεραπεία (ΑΙ) Αποκλιμάκωση με βάση τα αποτελέσματα των κ/ων (μείωση κατανάλωσης αντιβιοτικών, ανεπιθύμητων ενεργειών και κόστους-ΑΙΙ) Βελτίωση της δοσολογίας με εφαρμογή των δεδομένων PK-PD (ΑΙΙ) This can result in reduced length of hospital stay, health care costs, and potential complications due. to intravenous access., με βαση κλινικα κριτηρια εφοσον υπαρχουν εναλλακτικα φαρμακα με καλη βιοδιαθεσιμοτητα. Στοχευμενη θεραπεια. (e.g., age, renal function, and weight), causative organism and site of infection (e.g., endocarditis, meningitis, and osteomyelitis) Βανκομυκινη, κολιμυκινη, β-λακταμες παρατεταμενη εγχυση, μια φορα/ημ αμινογλυκοσιδες. Για να εξασφαλίσθει η καταλληλότητα της αρχικης εμπειρικης θεραπειας.")
26
Συμπληρωματικές στρατηγικές
Antibiotic Stewardship Programs (ASP) : IDSA guidelines Συμπληρωματικές στρατηγικές Εκπαίδευση (βασική προϋπόθεση για αλλαγή συνταγογραφικών συνηθειών, παθητική, μόνη της χωρίς ενεργό παρέμβαση δεν προσφέρει-ΒΙΙ) Αιτιολογημένη φόρμα και αυτόματη διακοπή (μείωση κατανάλωσης αλλά όχι βελτίωση χρήσης αντιβιοτικών-BII) Antimicrobial cycling (δεν συστήνεται, χωρίς μακροπρόθεσμα καλά αποτελέσματα-CII) Μια στρατηγικη που σταματα στην εκπαιδευση …Μακροπροθεσμα αποτελεσματα Πληρης απομακρυνση ενός αντιβιοτικου για μεγαλο χρονικο διαστημα και αντικατασταση του από άλλο Σημαντικο ποσοστο ασθενων στις μελετες επαιρνε κατι άλλο για διαφορους ιατρικούς λογους, σε περιβαλλον που ενδημει η πολυαντοχη δεν υπαρχουν αρκετα αντιβιοτικα δραστικα για να εφαρμοσθει, ο μηχανισμός αντοχής που επιλεγεται παραμενει στον μικροβιακο πληθυσμό που ενδημεί και ξαναεπιλεγεται Καταλληλη στρατηγική για την διακοπή της περιεγχειρητικης χ/ξης the failures of well-intended antibiotic cycling programs are a testimony to the challenges associated with programs lack of understanding of resistance determinants.
 : IDSA guidelines. Συμπληρωματικές στρατηγικές. Εκπαίδευση (βασική προϋπόθεση για αλλαγή συνταγογραφικών συνηθειών, παθητική, μόνη της χωρίς ενεργό παρέμβαση δεν προσφέρει-ΒΙΙ) Αιτιολογημένη φόρμα και αυτόματη διακοπή (μείωση κατανάλωσης αλλά όχι βελτίωση χρήσης αντιβιοτικών-BII) Antimicrobial cycling (δεν συστήνεται, χωρίς μακροπρόθεσμα καλά αποτελέσματα-CII) Μια στρατηγικη που σταματα στην εκπαιδευση …Μακροπροθεσμα αποτελεσματα. Πληρης απομακρυνση ενός αντιβιοτικου για μεγαλο χρονικο διαστημα και αντικατασταση του από άλλο. Σημαντικο ποσοστο ασθενων στις μελετες επαιρνε κατι άλλο για διαφορους ιατρικούς λογους, σε περιβαλλον που ενδημει η πολυαντοχη δεν υπαρχουν αρκετα αντιβιοτικα δραστικα για να εφαρμοσθει, ο μηχανισμός αντοχής που επιλεγεται παραμενει στον μικροβιακο πληθυσμό που ενδημεί και ξαναεπιλεγεται. Καταλληλη στρατηγική για την διακοπή της περιεγχειρητικης χ/ξης. the failures of well-intended antibiotic cycling programs are a testimony to the challenges associated. with programs lack of understanding of resistance determinants.")
27
Enterobacteriaceae ESBL (+)
Isolation of key resistance types from ventilator-associated pneumonia patients at an intensive care unit in northern Spain from 2000–2003.The white bars are total incidence and the black bars indicate the proportion with the key resistance:1, Acinetobacter, carbapenemresistance;2,Enterobacteriaceae,extended-spectrum - lactamases; 3, Pseudomonas aeruginosa, anyresistance;4, Staphylococcus aureus, meticillinresistance;and5, Enterococcus faecalis, irrespectiveofresistance.Theempirical agents rotatedinthecyclingperiod,orsequentiallywithheldintherestrictiveperiod,were carbapenems,piperacillin/tazobactam and oxyimino-cephalosporins. A hint of potential benefit nevertheless is given by the work of Sandiumenge et al. (Fig. 1) [29]. In successive 11-month periods from 2000 to 2003 at a single ICU in Spain, these authors tested the effects of (i) antibiotic choice based on patient-specific factors, (ii) cycling of cephalosporins, TZP and carbapenems, (iii) restriction of one of these drug classes for 4-month periods and (iv) allocating successive patients to the different antibiotic regimens. There are many potential confounders, notably underlying national resis- tance trends. Nevertheless, the results suggest that resistance and infection rates were highestwhenselection pressure wasmost con- centrated, and least when use was heterogeneous. Further studies are needed to test these conclusions, which support very different models of stewardship to those now standard in the UK. 3. P.aeruginosa MDR 4. MRSA 5. E.faecalis MDR Acinetobacter Carb-R Enterobacteriaceae ESBL (+)
 [29]. In successive 11-month periods from 2000 to 2003 at a single ICU in Spain, these authors tested the effects of (i) antibiotic choice based on patient-specific factors, (ii) cycling of cephalosporins, TZP and carbapenems, (iii) restriction of one of these drug classes for 4-month periods and (iv) allocating successive patients to the different antibiotic regimens. There are many potential confounders, notably underlying national resis- tance trends. Nevertheless, the results suggest that resistance and infection rates were highestwhenselection pressure wasmost con- centrated, and least when use was heterogeneous. Further studies are needed to test these conclusions, which support very different models of stewardship to those now standard in the UK. 3. P.aeruginosa MDR. 4. MRSA. 5. E.faecalis MDR. Acinetobacter Carb-R. Enterobacteriaceae ESBL (+)")
28
SHEA/ IDSA/ PIDS RECOMMENDATIONS 2012
Η εφαρμογή Προγράμματος Επιτήρησης της Χρήσης Αντιβιοτικών πρέπει να γίνεται μέσα από ανάλογο νομοθετικό πλαίσιο για όλα τα επίπεδα Παροχής Υπηρεσιών Υγείας Εκπαίδευση για την αντοχή και την ορθολογική χρήση αντιβιοτικών όλων όσων συνταγογραφούν –Προαπαιτούμενο Τα δεδομένα κατανάλωσης αντιβιοτικών σε εθνικό επίπεδο πρέπει να είναι διαθέσιμα στους γιατρούς Πρωτοβαθμια περιθαλψη, Μοναδες βραχειας νοσηλειας, μοναδες ΤΝ… Integration of clinical decision support technology into EHRs + Integration of clinical decision support technology into e-prescribing mechanisms= απαιτουμενο από τις ασφαλιστικες εταιρειες …for those in training programs as well as for all prescribing clinicians that teach about the science behind, the principles of, and the tools essential for the practice of effective antimicrobial stewardship-Education about antimicrobial resistance and stewardship should be incorporated into curriculum requirements for medical students and postgraduate residents and fellows (αξιολογηση της επαρκειας?) Ακαδημαϊκοι και κρατικοι φορεις αλλα και η φαρμακοβιομηχανια στα πλαισια εγκρισης για την κυκλοφορια νεου φαρμακου εκπαιδευση για την αριστη χρηση ενός αντιβιοτικου και τροπους προληψης της αναπτυξης αντοχης σε αυτό Καταναλωση αντιβιοτικων σε κοινοτητα και νοσοκομεια=We believe that these data are critical to being able to monitor antimicrobial use and its relationship to antimicrobial resistance
 Ακαδημαϊκοι και κρατικοι φορεις αλλα και η φαρμακοβιομηχανια στα πλαισια εγκρισης για την κυκλοφορια νεου φαρμακου εκπαιδευση για την αριστη χρηση ενός αντιβιοτικου και τροπους προληψης της αναπτυξης αντοχης σε αυτό. Καταναλωση αντιβιοτικων σε κοινοτητα και νοσοκομεια=We believe that these data are critical to being able to monitor antimicrobial use and its relationship to antimicrobial resistance.")
29
Antibiotic Stewardship Programs (ASP):
Ο Ρόλος του Μικροβιολογικού Εργαστηρίου Εξαιρετικά σημαντικός Ταχεία διάγνωση (παρακολούθηση αποικισμού, φαινοτυπικά τεστ, μοριακός έλεγχος, MALDI-TOF…) Ερμηνεία ελέγχου ευαισθησίας με βάση τα κλινικά όρια ευαισθησίας (πχ καρβαπενέμες) Ενημέρωση θεραπόντων και της ομάδας ASP για τροποποίηση αγωγής Ανίχνευση και διερεύνηση επιδημιών Περιορισμένο αντιβιόγραμμα σαν μέθοδος antibiotic stewardship MALDI-TOF MS platforms offers significantly improved turnaround time as compared to conventional culture methods from which AMS will undoubtedly benefit next-generation sequence technology (rapid MRSA detection through mecA, rapid ESBL or carbapenemase detection…) Recently introduced methods can be target-specific, such as polymerase chain reaction (PCR) methods to detect a single microbe such as MRSA or to detect 17 respiratory tract viruses or a resistance mechanism 16S rRNA analysis
 Ερμηνεία ελέγχου ευαισθησίας με βάση τα κλινικά όρια ευαισθησίας (πχ καρβαπενέμες) Ενημέρωση θεραπόντων και της ομάδας ASP για τροποποίηση αγωγής. Ανίχνευση και διερεύνηση επιδημιών. Περιορισμένο αντιβιόγραμμα σαν μέθοδος antibiotic stewardship. MALDI-TOF MS platforms offers significantly improved turnaround time as compared to. conventional culture methods from which AMS will undoubtedly benefit. next-generation sequence technology (rapid MRSA detection through mecA, rapid ESBL or carbapenemase detection…) Recently introduced methods can be target-specific, such as polymerase chain reaction (PCR) methods to detect a single microbe such. as MRSA or to detect 17 respiratory tract viruses or a resistance mechanism. 16S rRNA analysis.")
30
Clinical Decision Support Systems
Antibiotic Stewardship Programs (ASP): Ο Ρόλος της Πληροφορικής Η ηλεκτρονική παραγγελία των αντιβιοτικών και η τροφοδότηση του συστήματος με δεδομένα του φακέλου του ασθενούς (Electronic Health Records) και τις τοπικές κατευθυντήριες οδηγίες μπορεί να οδηγήσει σε: Βελτιστοποίηση της δοσολογίας Μείωση παρενεργειών Αποφυγή αλληλεπιδράσεων και αδόκιμων συνδυασμών Πρόληψη ιατρικών λαθών Στοχευμένη θεραπεία με βάση τις κ/ες Hλεκτρονική Kαταγραφή δεδομένων βοηθά στην μέτρηση της κατανάλωσης αντιβιοτικών, του κόστους, της αντοχής των νοσοκομειακών μικροβίων, στην επιτήρηση αναδυόμενων φαινοτύπων αντοχής και στην ανίχνευση επιδημιών Clinical Decision Support Systems=Requires existing electronic records and electronic prescribing system to be effective. Δημογραφικα (ηλικια, ΣΒ, φύλο…) αλλεργιες, αλλα φαρμακα, νεφρικη-ηπατικη βιολογια, σταθμη φαρμακων, αναντιστοιχια μεταξυ κ/ων και χορηγουμενου αντιβιοτικου… Επι του παρόντος τετοιου ειδους πολύπλοκη υποστήριξη από τα νοσοκομειακά συστήματα μηχανογραφησης δεν είναι διαθεσιμη στα περισσότερα νοσοκομεια Clinical decision support systems have also been adopted by many institutions in order to support ASP efforts. These systems have been shown to decrease adverse events, shorten length of stay, decrease cost and improve empiric, therapeutic and surgical prophylactic use of antimicrobials. However, implementation of CDSS has various barriers and limitations. Current systems should only serve as a support for clinicians and not a replacement for human ASP personnel in view of the complexity of patient factors. Clinical Decision Support Systems
: Ο Ρόλος της Πληροφορικής. Η ηλεκτρονική παραγγελία των αντιβιοτικών και η τροφοδότηση του συστήματος με δεδομένα του φακέλου του ασθενούς (Electronic Health Records) και τις τοπικές κατευθυντήριες οδηγίες μπορεί να οδηγήσει σε: Βελτιστοποίηση της δοσολογίας. Μείωση παρενεργειών. Αποφυγή αλληλεπιδράσεων και αδόκιμων συνδυασμών. Πρόληψη ιατρικών λαθών. Στοχευμένη θεραπεία με βάση τις κ/ες. Hλεκτρονική Kαταγραφή δεδομένων βοηθά στην μέτρηση της κατανάλωσης αντιβιοτικών, του κόστους, της αντοχής των νοσοκομειακών μικροβίων, στην επιτήρηση αναδυόμενων φαινοτύπων αντοχής και στην ανίχνευση επιδημιών. Clinical Decision Support Systems=Requires existing electronic records and electronic prescribing system to be effective. Δημογραφικα (ηλικια, ΣΒ, φύλο…) αλλεργιες, αλλα φαρμακα, νεφρικη-ηπατικη βιολογια, σταθμη φαρμακων, αναντιστοιχια μεταξυ κ/ων και χορηγουμενου αντιβιοτικου… Επι του παρόντος τετοιου ειδους πολύπλοκη υποστήριξη από τα νοσοκομειακά συστήματα μηχανογραφησης δεν είναι διαθεσιμη στα περισσότερα νοσοκομεια. Clinical decision support systems have also been adopted by many institutions in order to support ASP efforts. These systems. have been shown to decrease adverse events, shorten length of stay, decrease cost and improve empiric, therapeutic and surgical. prophylactic use of antimicrobials. However, implementation of CDSS has various barriers and limitations. Current. systems should only serve as a support for clinicians and not a replacement for human ASP personnel in view of the complexity. of patient factors. Clinical Decision Support Systems.")
31
Antibiotic Stewardship Programs (ASP): Ο Ρόλος της Πληροφορικής
Clin Infect Dis 2013;57:1145 90% of physicians in USA access drug information via a mobile app 40% use a mobile app once or twice a day Over 1200 apps for HCP were identified Many apps involve diagnosis and patient management, creating a need for regulations and oversight by the US Food and Drug Administration use of medical applications (apps) and eBooks has surged with the introduction of smartphones. With these technological advances, the steward can access a large amount of medical knowledge with the tap of a finger at the patient’s bedside. However, connectivity alone does not affect patient care; how an app or an eBook is used is the true test
 and eBooks has. surged with the introduction of smartphones. With these technological advances, the steward can access a large amount of medical knowledge with the tap of a finger. at the patient’s bedside. However, connectivity alone does not affect patient care; how an app or an eBook is used is the true test.")
32
Α smartphone application for the delivery of antimicrobial prescribing policy
E.Charani et al. JAC 2013

33
Antibiotic Stewardship Programs (ASP): Ο Ρόλος του Αλλεργιολόγου
The impact of penicillin skin testing on clinical practice and antimicrobial stewardship Rimawi RH et al. J Hosp Med 2013 Από 146 ασθενείς με αναφερόμενο ιστορικό αλλεργίας στην πενικιλλίνη, το PST (PRE-PEN) ήταν αρνητικό σε 145 και όλοι έλαβαν με ασφάλεια β-λακτάμη χωρίς αλλεργική αντίδραση. Η αρνητική προγνωστική αξία του PST ήταν 100% Η αποκλιμάκωση που έγινε απέφερε κέρδος $82.000 Είναι ο νεος συμμαχος του λοιμωξιολογου Ο ΑΠΟΧΑΡΑΚΤΗΡΙΣΜΟΣ ΤΩΝ ΑΣΘΕΝΩΝ ΠΟΥ ΑΝΑΦΕΡΟΥΝ ΑΛΛΕΡΓΙΑ ΣΕ ΑΝΤΙΒΙΟΤΙΚΑ, ΜΕΤΑ ΑΠΟ ΚΑΤΑΛΛΗΛΟ ΕΛΕΓΧΟ, ΕΙΝΑΙ ΕΝΑ ΕΠΙΠΛΕΟΝ ΕΡΓΑΛΕΙΟ ΤΟΥ «ΠΡΟΓΡΑΜΜΑΤΟΣ ΔΙΑΧΕΙΡΙΣΗΣ ΑΝΤΙΒΙΟΤΙΚΩΝ»
 ήταν αρνητικό σε 145 και όλοι έλαβαν με ασφάλεια β-λακτάμη χωρίς αλλεργική αντίδραση. Η αρνητική προγνωστική αξία του PST ήταν 100% Η αποκλιμάκωση που έγινε απέφερε κέρδος $ Είναι ο νεος συμμαχος του λοιμωξιολογου. Ο ΑΠΟΧΑΡΑΚΤΗΡΙΣΜΟΣ ΤΩΝ ΑΣΘΕΝΩΝ ΠΟΥ ΑΝΑΦΕΡΟΥΝ ΑΛΛΕΡΓΙΑ ΣΕ ΑΝΤΙΒΙΟΤΙΚΑ, ΜΕΤΑ ΑΠΟ ΚΑΤΑΛΛΗΛΟ ΕΛΕΓΧΟ, ΕΙΝΑΙ ΕΝΑ ΕΠΙΠΛΕΟΝ ΕΡΓΑΛΕΙΟ ΤΟΥ «ΠΡΟΓΡΑΜΜΑΤΟΣ ΔΙΑΧΕΙΡΙΣΗΣ ΑΝΤΙΒΙΟΤΙΚΩΝ»")
34
Clin Infect Dis 2013 Απροθυμία παρέμβασης στις θεραπευτικές οδηγίες των συναδέλφων- «Σεβασμός στην Αυτονομία Συνταγογράφησης» Αποδεκτή η παρέκκλιση από τις κατευθυντήριες οδηγίες όσον αφορά τους υψηλά ιστάμενους στην ιεραρχία (Seniors)- «Η προσωπική εμπειρία» των ανωτέρων τους το επιτρέπει (expert opinion) Ο ανώτερος στην ιεραρχία άμεσα ή έμμεσα κατευθύνει την συνταγογράφηση …the behavior of clinical leaders or seniors influences practice of junior doctors. To influence the antimicrobial prescribing…, interventions need to address prescribing etiquette and use clinical leadership … to influence practice. Ποιοι είναι οι κοινωνικοι παραγοντες που επηρεαζουν την συνταγογραφική συμπεριφορα σε 4 νοσοκομεια στο Λονδίνο Συνεντευξη πανω σε συγκεκριμενο ερωτηματολογιο σε γιατρους διαφορων ειδικοτητων και βαθμίδων, φαρμακοποιους, νοσηλευτες και μαίες Ώστε να σχεδιαστουν παρεμβασεις που θα αλλαξουν την συμπεριφορα αυτων που συνταγογραφούν Που εμπιπτουν στις κατευθυντηριες οδηγίες When developing an institutional program, it is important to know the audience who need to be advised on the benefits of the program, understand their concerns, and develop effective messages to communicate those benefits and overcome their concerns
- «Η προσωπική εμπειρία» των ανωτέρων τους το επιτρέπει (expert opinion) Ο ανώτερος στην ιεραρχία άμεσα ή έμμεσα κατευθύνει την συνταγογράφηση. …the behavior of clinical leaders or seniors influences practice of junior doctors. To influence the antimicrobial prescribing…, interventions. need to address prescribing etiquette and use clinical leadership … to influence practice. Ποιοι είναι οι κοινωνικοι παραγοντες που επηρεαζουν την συνταγογραφική συμπεριφορα σε 4 νοσοκομεια στο Λονδίνο. Συνεντευξη πανω σε συγκεκριμενο ερωτηματολογιο σε γιατρους διαφορων ειδικοτητων και βαθμίδων, φαρμακοποιους, νοσηλευτες και μαίες. Ώστε να σχεδιαστουν παρεμβασεις που θα αλλαξουν την συμπεριφορα αυτων που συνταγογραφούν. Που εμπιπτουν στις κατευθυντηριες οδηγίες. When developing an institutional program, it is important to know the audience who need to be advised on the. benefits of the program, understand their concerns, and develop effective messages to communicate those benefits. and overcome their concerns.")
35
Antimicrobial stewardship interventions have mainly been conducted at the postgraduate level, aiming at changing the behavior of professionals. This has proven extremely difficult and frustrating. This is, in our opinion, a missed opportunity for the future. It seems obvious that antimicrobial stewardship is likely to be more successful when started much earlier, at the time when knowledge, attitude and behavior of professionals are being shaped. Education on prudent antimicrobial prescribing should start early in the undergraduate curriculum, preferably in the third year of undergraduate training. The teaching of principles preparing for antimicrobial stewardship should be guaranteed by the development of learning outcomes and competencies and the appropriate evaluation. • Postgraduate education should then focus on implementation and measurement of practice, with additional supportive and restrictive measures.

36
To help address the growing problem of antimicrobial resistance, efforts should be
undertaken to ensure that our future doctors are well educated in the principles and practices of appropriate use of antibiotics and antimicrobial stewardship. Mean correct knowledge score (11 items) was 51%, Students wanted further education on antibiotic prescribing, and areas of lack of confidence were found. Final-year students at seven European medical schools were invited to participate in an online survey in 2012. Students at all schools felt mostconfident in diagnosing an infection and least confident in choosing combination therapies, choosing the correct dose and interval of administration and not prescribing in cases of diagnostic uncertainty Clin Infect Dis 2013;57:631
 was 51%, Students wanted further education on antibiotic prescribing, and areas of lack of confidence were. found. Final-year students at seven European medical schools were invited to participate in an online survey in Students at all schools felt mostconfident in diagnosing an infection and least confident in choosing. combination therapies, choosing the correct dose and interval of administration and not prescribing in cases of. diagnostic uncertainty. Clin Infect Dis 2013;57:631.")
37
Τα αποτελεσματα των προγραμματων «πολιτικησ αντιβιοτικων»

38
Τα Προγράμματα Διαχείρισης Αντιβιοτικών
Μειώνουν την κατανάλωση αντιβιοτικών (22-36%) και εξοικονομούν χρήματα ( $ ετησίως) έτσι ώστε να είναι αυτοχρηματοδοτούμενα
 και εξοικονομούν χρήματα ( $ ετησίως) έτσι ώστε να είναι αυτοχρηματοδοτούμενα.")
39
μεθ JAC 2011 24 μελέτες συμπεριελήφθησαν
Περιορισμός αντιβιοτικού/προέγκριση (6) Συμβουλευτική από λοιμωξιολόγο (5) Εφαρμογή οδηγιών και πρωτοκόλλων αποκλιμάκωσης (2) Εφαρμογή οδηγιών για προφύλαξη (2) Ελεγχος των αντιβιοτικών συγκεκριμένη ημέρα (3) Computer assisted decision support (6) Είδη παρεμβάσεων The quality of research was poor, with only 3 randomized controlled trials We identified six intervention types: studies of antibiotic restriction or preapproval (six studies); formal infectious diseases physician consultation (five); implementation of guidelines or protocols for de-escalation (two); guidelines for antibiotic prophylaxis or treatment in intensive care (two); formal reassessment of antibiotics on a pre-specified day of therapy (three); and implementation of computer- assisted decision support (six). Κινολονες, 3ης γενιας Κ και ESBLs, καρβαπενεμες-ψευδομοναδα, Μείωση χρήσης αντιβιοτικών (κατά 11-38% DDDs/1000 ημ.ασθ.) Μείωση κόστους (US$ 5–10/ημ.ασθ) Μικρότερη διάρκεια αντιβιοτικών, καλύτερη χρήση και λιγότερες ανεπιθύμητες ενέργειες Χωρίς αύξηση στην επίπτωση ΝΛ, διάρκεια νοσηλείας και θνητότητα Παρεμβάσεις με διάρκεια >6 μήνες έδειξαν μείωση της αντοχής για κάποια παθογόνα σε μερικές από τις μελέτες
 Συμβουλευτική από λοιμωξιολόγο (5) Εφαρμογή οδηγιών και πρωτοκόλλων αποκλιμάκωσης (2) Εφαρμογή οδηγιών για προφύλαξη (2) Ελεγχος των αντιβιοτικών συγκεκριμένη ημέρα (3) Computer assisted decision support (6) Είδη παρεμβάσεων. The quality of research was poor, with only 3 randomized controlled trials. We identified six intervention types: studies of antibiotic restriction or preapproval. (six studies); formal infectious diseases physician consultation (five); implementation of guidelines. or protocols for de-escalation (two); guidelines for antibiotic prophylaxis or treatment in intensive care (two); formal reassessment of antibiotics on a pre-specified day of therapy (three); and implementation of computer- assisted decision support (six). Κινολονες, 3ης γενιας Κ και ESBLs, καρβαπενεμες-ψευδομοναδα, Μείωση χρήσης αντιβιοτικών (κατά 11-38% DDDs/1000 ημ.ασθ.) Μείωση κόστους (US$ 5–10/ημ.ασθ) Μικρότερη διάρκεια αντιβιοτικών, καλύτερη χρήση και λιγότερες ανεπιθύμητες ενέργειες. Χωρίς αύξηση στην επίπτωση ΝΛ, διάρκεια νοσηλείας και θνητότητα. Παρεμβάσεις με διάρκεια >6 μήνες έδειξαν μείωση της αντοχής για κάποια παθογόνα σε μερικές από τις μελέτες.")
40
Targeted antibiotic consumption and nosocomial C.difficile disease
Tertiary-care hospital, Quebec, Μετα-αναλυση των μελετων που εχουν δημοσιευθει επιβεβαιωνει την θετικη επιδραση του περιορισμου της χρησης αντιβιοτικων και της μειωσης της επιπτωσης… Valiquette, et al. Clin Infect Dis 2007;45:S112.

41
Interventions to improve antibiotic prescribing practices for hospital inpatients
Βιβλιογραφία Σύγκριση παρεμβάσεων «αυστηρού περιορισμού» και «αλλαγής συμπεριφοράς» 89 μελέτες (randomized clinical trials, controlled clinical trials, controlled before and after studies, interrupted time series), 95 παρεμβάσεις The main comparison is between interventions that had a restrictive element and those that were purely persuasive. Restrictive interventions were implemented through restriction of the freedom of prescribers to select some antibiotics. Persuasive interventions used one or more of the following methods for changing professional behaviour: dissemination of educational resources, reminders, audit and feedback, or educational outreach. Restrictive interventions could contain persuasive elements. Ειδος-διαρκεια-οδός χορήγησης The results had to include interpretable data (με καποιο μετρήσιμο μεγεθος) about the effect of the intervention on antibiotic prescribing or microbial outcomes or relevant clinical outcomes Davey et al. Cochrane Database Syst Rev 2013
, 95 παρεμβάσεις. The main comparison is between interventions that had a restrictive element and those that were purely persuasive. Restrictive interventions were implemented through restriction of the freedom of prescribers to select some antibiotics. Persuasive interventions used one or more of the following methods for changing professional behaviour: dissemination of educational resources, reminders, audit and feedback, or educational outreach. Restrictive interventions could contain persuasive elements. Ειδος-διαρκεια-οδός χορήγησης. The results had to include interpretable data (με καποιο μετρήσιμο μεγεθος) about the effect of the intervention on antibiotic prescribing or microbial outcomes or relevant clinical outcomes. Davey et al. Cochrane Database Syst Rev")
42
Interventions to improve antibiotic prescribing practices for hospital inpatients
Οι παρεμβάσεις «περιορισμού» είχαν σημαντικότερη επίδραση στην «ποσότητα συνταγογράφησης» εντός του πρώτου μήνα και στην «επιδημιολογία» μετά το 6μηνο. Οι παρεμβάσεις «αλλαγής συμπεριφοράς» αποδίδουν τα ίδια καλά αποτελέσματα μετά από μήνες Οι παρεμβάσεις που στόχευαν στη «μείωση χρήσης αντιβιοτικών» έδειξαν μείωση της επίπτωσης C.difficile, μείωση των ανθεκτικών Gram (-), VRE, MRSA χωρίς αύξηση της θνητότητας Οι παρεμβάσεις που στόχευαν σε «καταλληλότερη θεραπεία» έδειξαν μείωση της θνητότητας Meta-analysis of 52 ITS studies was used to compare restrictive versus purely persuasive interventions Restrictive interventions had significantly greater impact on prescribing outcomes at one month (32%, 95% confidence interval (CI) 2% to 61%, P = 0.03) and on microbial outcomes at 6 months (53%, 95% CI 31% to 75%, P = 0.001) but there were no significant differences at 12 or 24 months Interventions intended to decrease excessive prescribing were associated with reduction in Clostridium difficile infections and colonization or infection with aminoglycoside- or cephalosporin-resistant gram-negative bacteria, methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus faecalis. Meta-analysis of clinical outcomes showed that four interventions intended to increase effective prescribing for pneumonia were associated with significant reduction in mortality (risk ratio 0.89, 95% CI 0.82 to 0.97), whereas nine interventions intended to decrease excessive prescribing were not associated with significant increase in mortality (risk ratio 0.92, 95% CI 0.81 to 1.06). Η στρατηγική «αυστηρού περιορισμού» δίνει ταχύτερα αποτελέσματα και ίσως είναι προτιμότερη όταν υπάρχει επείγουσα ανάγκη πχ ελεγχος επιδημίας… Davey et al. Cochrane Database Syst Rev 2013
, VRE, MRSA χωρίς αύξηση της θνητότητας. Οι παρεμβάσεις που στόχευαν σε «καταλληλότερη θεραπεία» έδειξαν μείωση της θνητότητας. Meta-analysis of 52 ITS studies was used to compare restrictive versus purely persuasive interventions. Restrictive interventions had significantly greater impact on prescribing outcomes at one month (32%, 95% confidence interval (CI) 2% to 61%, P = 0.03) and on microbial outcomes at 6 months (53%, 95% CI 31% to 75%, P = 0.001) but there were no significant differences at 12 or 24 months. Interventions intended to decrease excessive prescribing were associated with reduction in Clostridium difficile infections and colonization or infection with aminoglycoside- or cephalosporin-resistant gram-negative bacteria, methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus faecalis. Meta-analysis of clinical outcomes showed that four interventions intended to increase effective prescribing for pneumonia were associated with significant reduction in mortality (risk ratio 0.89, 95% CI 0.82 to 0.97), whereas nine interventions intended to decrease excessive prescribing were not associated with significant increase in mortality (risk ratio 0.92, 95% CI 0.81 to 1.06). Η στρατηγική «αυστηρού περιορισμού» δίνει ταχύτερα αποτελέσματα και ίσως είναι προτιμότερη όταν υπάρχει επείγουσα ανάγκη πχ ελεγχος επιδημίας… Davey et al. Cochrane Database Syst Rev")
43
Surviving Sepsis Campaign: EARLY GOAL-DIRECTED THERAPY
Κάθε ώρα καθυστέρησης στην έναρξη κατάλληλων αντιβιοτικών αυξάνει τη θνητότητα κατά 7% στον σηπτικό ασθενή EARLY GOAL-DIRECTED THERAPY Delayed antibiotic therapy is associated with a worse outcome for patients presenting with a severe acute infection. Each hour of delay in the administration of antibiotic therapy in the first six hours is associated with an average decrease in survival of more than 7% [5]. It is therefore advised to start antibiotics as soon as possible whenever sepsis is considered. Although rapid and adequate antibiotic therapy is of great importance, it is obvious that aggressive strategies can easily lead to a high consumption of broad-spectrum antimicrobial agents Κινδυνος υπερθεραπειας, υπερκαταναλωσης συνδυασμού αντιβιοτικων, η μοριακη διαγνωστικη αν και βελτιωνεται δεν μπορει να διαχωρισει με ασφαλεια τους ασθενεις που θα οφεληθουν από την προσεγγιση αυτη Kumar A et al. Crit Care Med 2006

44
Για τον βαρέως πάσχοντα ασθενή
ΑΠΟΚΛΙΜΑΚΩΣΗ Κλινική πορεία του ασθενούς Αποτελέσματα καλλιεργειών Βιολογικοί Δείκτες Σε ώρες a critical reassessment of therapy after 2 or 3 days Αμεση εναρξη ευρεως φασματος αντιβιοτικων αλλα …

45
Συμπληρωματικά Εργαλεία : BIOMARKERS
ΑΠΟΚΛΙΜΑΚΩΣΗ Συμπληρωματικά Εργαλεία : BIOMARKERS Διάκριση σήψης από SIRS Προγνωστικός δείκτης Λήψη κλινικών αποφάσεων Sens, Spec: 75-80% PCT Μεταβολή τις πρώτες 72±12h Point of care diagnostic tests=Mostly undergoing research evaluation. Diagnosis of non-bacterial etiologies may help reduce antibiotic prescription Wacker: Recently, a meta-analysis including 30 high-quality studies totaling 3244 patients found that, in fact, PCT can differentiate effectively between sepsis and SIRS of noninfectious origin, with an area under the receiver operating characteristic curve of 0.85 [95% confidence interval (CI) 0.81–0.88] The results were similar for medical, surgical, or pediatric patients. At the median cutoffs used in the different studies, approximately 1.0mg/l, the calculated sensitivity and specificity of PCT each were around 75–80%. <0.5mg/l or > 2.0mg/l Διαστρωμάτωση κινδύνου A more than 80% decrease from baseline PCT levels during that time had a negative predictive value to exclude ICU mortality of ~90%. Such a PCT decrease might help to identify individuals at reduced risk, who thus would be good early ICU discharge candidates. Conversely, no change or an increase in PCT within this time frame had a positive predictive value for ICU mortality of around 35–50%; such kinetics may help to detect patients who are at high mortality risk and thus likely to require treatment escalation Guidance using measurements taken at longer intervals, that is, 72–96 h, may be a preferable strategy Individualized antibiotic therapy decisions with procalcitonin-based algorithms pro-adrenomedullin (pro-ADM) and soluble triggering receptor expressed on myeloid cells-1 (sTREM-1), and a biomarker combination is likely to be a future approach This biomarker is upregulated in response to microbial toxins and certain bacterial-specific proinflammatory mediators [e.g., interleukin (IL)-1b, tumour necrosis factor-a, and IL-6], and is downregulated as these substances decrease in the circulation during recovery. However, concentrations of this peptide also rise following major trauma, severe burns and certain malignancies, meaning that on its own it is not specific enough to serve as a diagnostic marker of sepsis. Several meta-analyses have assessed PCT as a marker of sepsis with conflicting findings. A recent meta-analysis of PCT [Wacker 2013] that analyzed 30 studies with 3244 patients may be of assistance here, showing a pooled sensitivity of 077 [95% confidence interval (CI) 072–081] and a pooled specificity of 079 (95% CI 074–084). These findings show that PCT may still have a role in the diagnosis of sepsis. (Εχει αξία ως …) It has potential to assist as part of sepsis prediction algorithms, but there is currently insufficient evidence to support its use as an independent diagnostic tool. H PCT και λιγότερο η CRP έχουν χρησιμοποιηθεί σαν εργαλείο για συντομότερη διάρκεια αγωγής, ή de-escalation (As a biomarker for infection, PCT is more sensitive and specific than C-reactive protein) Φαίνεται ότι μπορει να βοηθήσει στην λήψη… On the other hand, 1, or preferably, 2 normal PCT levels in the hypotensive patient virtually eliminates invasive bacterial infection as an etiology; the negative predictive value is >95% Sequential PCT levels are an excellent guide to the duration of antibacterial therapy Εναρξη & Διακοπή αντιβιοτικών Wacker C et al. Lancet Infect Dis 2013 Schuetz P et al. Crit Care 2013 Schuetz P et al. Clin Infect Dis 2012
 0.81–0.88] The results were similar for medical, surgical, or pediatric patients. At the median cutoffs used in. the different studies, approximately 1.0mg/l, the calculated sensitivity and specificity of PCT each were around 75–80%. <0.5mg/l or > 2.0mg/l. Διαστρωμάτωση κινδύνου. A more than 80% decrease from baseline PCT levels during that time had a negative predictive value to. exclude ICU mortality of ~90%. Such a PCT decrease might help to identify individuals at reduced risk, who thus would. be good early ICU discharge candidates. Conversely, no change or an increase in PCT within this time. frame had a positive predictive value for ICU mortality of around 35–50%; such kinetics may. help to detect patients who are at high mortality risk and thus likely to require treatment escalation. Guidance using measurements taken at longer intervals, that is, 72–96 h, may be a preferable strategy. Individualized antibiotic therapy decisions with procalcitonin-based algorithms. pro-adrenomedullin (pro-ADM) and soluble triggering receptor expressed on myeloid. cells-1 (sTREM-1), and a biomarker combination is likely to be a future approach. This biomarker is upregulated in response to microbial toxins and certain bacterial-specific proinflammatory mediators [e.g., interleukin (IL)-1b, tumour necrosis factor-a, and IL-6], and is downregulated as these substances decrease in the circulation during recovery. However, concentrations of this peptide also rise following major trauma, severe burns and certain malignancies, meaning that on its own it is not. specific enough to serve as a diagnostic marker of sepsis. Several meta-analyses have assessed PCT as a marker of sepsis with conflicting findings. A recent meta-analysis of PCT [Wacker 2013] that analyzed 30 studies with 3244 patients may be of assistance. here, showing a pooled sensitivity of 077 [95% confidence interval (CI) 072–081] and a pooled specificity of 079 (95% CI 074–084). These findings. show that PCT may still have a role in the diagnosis of sepsis. (Εχει αξία ως …) It has potential to assist as part of sepsis prediction algorithms, but there is currently insufficient evidence to support its use as an independent diagnostic tool. H PCT και λιγότερο η CRP έχουν χρησιμοποιηθεί σαν εργαλείο για συντομότερη διάρκεια αγωγής, ή de-escalation (As a biomarker for infection, PCT is more sensitive and specific than C-reactive protein) Φαίνεται ότι μπορει να βοηθήσει στην λήψη… On the other hand, 1, or preferably, 2 normal PCT levels in the hypotensive patient virtually eliminates invasive. bacterial infection as an etiology; the negative predictive value is >95% Sequential PCT levels are an excellent guide to the duration of antibacterial therapy. Εναρξη & Διακοπή αντιβιοτικών. Wacker C et al. Lancet Infect Dis Schuetz P et al. Crit Care Schuetz P et al. Clin Infect Dis")
46
Διακοπή θεραπείας Procalcitonin to initiate or discontinue
antibiotics in acute respiratory tract infections Schuetz P et al. Cochrane Database Syst Rev 2012 Διακοπή θεραπείας Still, adherence rates to the PCT protocol were variable, and lower in these ICU trials compared with settings with lower-risk patients Overall, there was no difference in mortality in PCT group patients compared with control patients (5.7% vs 6.3%; adjusted OR, 0.94; 95% CI, .71–1.23). This was consistent across clinical settings and ARI diagnoses Στους ασθενεις της ΜΕΘ PCT χρήσιμη για την εγκαιρη διακοπή της θεραπειας και όχι της αποφυγής έναρξης αντιβιοτικων lower prescription rates in primary care (predominantly among patients with upper ARI and bronchitis), and lower duration of antibiotic courses in ED and ICU patients (with CAP and VAP)
. This was consistent across clinical settings and ARI diagnoses. Στους ασθενεις της ΜΕΘ PCT χρήσιμη για την εγκαιρη διακοπή της θεραπειας και όχι της αποφυγής έναρξης αντιβιοτικων. lower prescription rates in primary care (predominantly among patients with upper ARI and bronchitis), and lower duration of antibiotic courses in ED and ICU patients (with CAP and VAP)")
47
2011 Διάρκεια θεραπείας 6 RCTs, 1476 pts France, Belgium, Switzerland, Germany Heterogeneous ICU patient population Days without AB (23-37% increase) Days of AB exposure/1000 pts (20-23% reduction) Days on AB for the 1st infectious episode (21-38% reduction) AB exposure 20-38% did not significantly impact antimicrobial exposure in the study assessing treatment initiation only Length of ICU stay was significantly decreased in 2 studies but was unchanged in the others The failure of PCT guidance to meaningfully influence the decision to initiate antimicrobial use in ICU patients contrasts with its success in safely reducing antimicrobial initiation in patients with respiratory tract infections the generalizability of these results to other settings remains to be elucidated. Also, formal cost-effectiveness analysis was not performed in any of the studies under review and is not addressed here Χωρις καμια δυσμενη επιδραση στην εκβαση των ασθενων In most studies, use of antimicrobials was strongly discouraged for PCT levels of <0.25 μg/L and discouraged for PCT levels of <0.50 μg/L. Antimicrobial use was encouraged for PCT levels >0.50 μg/L and strongly encouraged for PCT levels ≥1 μg/L. Procalcitonin guidance was associated with significantly reduced antimicrobial exposure (effect sizes, 19.5%–38%) in all 5 studies assessing its impact on treatment duration but did not significantly impact antimicrobial exposure in the study assessing treatment initiation only Length of ICU stay (decrease in 2 studies), Length of hospital stay, Days free of mechanical ventilation, Relapse of infection and Mortality: unaffected by the use of PCT algorithms
 Days of AB exposure/1000 pts (20-23% reduction) Days on AB for the 1st infectious episode (21-38% reduction) AB exposure % did not significantly impact antimicrobial exposure in the study assessing treatment initiation only. Length of ICU stay was significantly decreased in 2 studies but was unchanged in the others. The failure of PCT guidance to meaningfully influence the decision to initiate antimicrobial use in ICU patients contrasts with its success in safely reducing antimicrobial initiation in patients with respiratory tract infections the generalizability of these results to other settings remains to be elucidated. Also, formal cost-effectiveness analysis was not performed in any of the studies under review and is not addressed here. Χωρις καμια δυσμενη επιδραση στην εκβαση των ασθενων. In most studies, use of antimicrobials was strongly discouraged for PCT levels of <0.25 μg/L and discouraged for PCT levels of <0.50 μg/L. Antimicrobial use was encouraged for PCT levels >0.50 μg/L and strongly encouraged for PCT levels ≥1 μg/L. Procalcitonin guidance was associated with significantly reduced antimicrobial exposure (effect sizes, 19.5%–38%) in all 5 studies assessing its impact on treatment duration but did not significantly impact antimicrobial exposure in the study assessing treatment initiation only. Length of ICU stay (decrease in 2 studies), Length of hospital stay, Days free of mechanical ventilation, Relapse of infection and Mortality: unaffected by the use of PCT algorithms.")
48
Μικρότερη Διάρκεια Θεραπείας
8 ημέρες για VAP 7 ημέρες για πυελονεφρίτιδα 10 ημέρες για σηπτική αρθρίτιδα 3-5 ημέρες για ήπια CAP Χωρις δυσμενη επίδραση στην πρόγνωση 8 vs 15 d for VAP 7 vs 14 d for UTI cipro Acute hematogenous for children 3 vs 8 d for mild CAP Chastre et al. 2003, Sandberg et al. 2012, Pertola et al. 2010, el Moussaoui R et al. 2006

49
Comply with guidelines Include indication/dose/duration
Get Smart Single dose for surgical prophylaxis Obtain cultures first History Comply with guidelines Include indication/dose/duration Then Focus Clinical review Check microbiology Stop Switch to oral Change Continue OPAT At 48 hours Καμπανια bacterial culture results, radiological results and response to initial therapy And re-evaluate at 72 hours outpatient parenteral antibiotic therapy (OPAT)
")
50
33 χώρες 947 νοσοκομεία 231000 ασθενείς
Η πλέον πρόσφατη αποτύπωση του προβλήματος των ενδονοσοκομειακών λοιμώξεων στην Ευρωπαϊκή Ενωση (ΕΕ) προέρχεται από τη Μελέτη Επιπολασμού των Νοσοκομειακών Λοιμώξεων και της Κατανάλωσης Αντιβιοτικών στα Ευρωπαϊκά Νοσοκομεία (Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Hospitals ), που δημοσιεύθηκε τον Ιούλιο 2013 ( Η μελέτη διοργανώθηκε και συντονίστηκε από το ΕCDC. Συμμετείχαν 33 ευρωπαϊκές χώρες (μεταξύ των οποίων και η Ελλάδα) και περισσότεροι από ασθενείς σε 947 νοσοκομεία. Η πρωτη μελετη σε ολη την Ευρωπη, μετά από εκπαιδευση των συμμετεχόντων ιατρων και νοσηλευτων στη μεθοδολογια καταγραφης του ECDC (ομοιομορφια και αξιοπιστια) Ελλαδα=37 νοσοκομεια, ασθενεις
 προέρχεται από τη Μελέτη Επιπολασμού των Νοσοκομειακών Λοιμώξεων και της Κατανάλωσης Αντιβιοτικών στα Ευρωπαϊκά Νοσοκομεία (Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Hospitals ), που δημοσιεύθηκε τον Ιούλιο 2013 ( Η μελέτη διοργανώθηκε και συντονίστηκε από το ΕCDC. Συμμετείχαν 33 ευρωπαϊκές χώρες (μεταξύ των οποίων και η Ελλάδα) και περισσότεροι από ασθενείς σε 947 νοσοκομεία. Η πρωτη μελετη σε ολη την Ευρωπη, μετά από εκπαιδευση των συμμετεχόντων ιατρων και νοσηλευτων στη μεθοδολογια καταγραφης του ECDC (ομοιομορφια και αξιοπιστια) Ελλαδα=37 νοσοκομεια, ασθενεις.")
51
Ποσοστό Νοσηλευομένων που Λαμβάνουν Αντιβιοτικά
Ευρωπαϊκή Ενωση 35% Ελλάδα 54.7% >1 είδος αντιβιοτικού/ασθενή Eυρώπη: 35 ( ) % των νοσηλευομένων λαμβάνουν αντιβιοτικά Ελλάδα: 54,7 (51,7-57,7) % των νοσηλευομένων λαμβάνουν αντιβιοτικά 1.6 αντιβιοτικά/ασθενή
 % των νοσηλευομένων λαμβάνουν αντιβιοτικά. Ελλάδα: 54,7 (51,7-57,7) % των νοσηλευομένων λαμβάνουν αντιβιοτικά. 1.6 αντιβιοτικά/ασθενή.")
52
ΕΛΛΑΔΑ: ΚΑΤΑΝΑΛΩΣΗ ΑΝΤΙΒΙΟΤΙΚΩΝ ΣΤΑ ΝΟΣΟΚΟΜΕΙΑ, PPS 2011-2012
ΕΕ 16% 9.5% Ποιότητα Surgical prophylaxis accounted for 16% of antimicrobials used στην ΕΕ, and was excessively prolonged for more than one day in 59% of the cases. The prevalence of patients receiving at least one antimicrobial agent was 35.0% (country range 21.4–54.7%). A total of antimicrobial agents was reported in patients: 70.9% of the patients received one antimicrobial, 23.4% received two and 5.7% received three or more antimicrobials. The overall prevalence of antimicrobial use extrapolated to the total number of occupied beds in Europe was 32.7% (95% confidence interval 29.4–36.2%). Η χωρα με το μεγαλυτερο ποσοστο νοσηλευομενων ασθενων υπο αντιμικροβιακή αγωγή …Το …% των χορηγουμενων αντιβιοτικων διδεται για Μπορουμε να μειωσουμε κατά 20% το ποσό των χορηγουμενων αντιβιοτικων αν εφαρμοσουμε τις διεθνεις οδηγιες για 1 δοση χπρ. One has to bear in mind that the percentage of prolonged surgical prophylaxis is overestimated in the PPS, because a different recall period is used for surgical prophylaxis (24 hours before 8 am on the survey day) and a treatment given for more than one day has a higher probability of being captured in the PPS study than a treatment given for one day only. Nonetheless, comparing this indicator between hospitals (and countries) using the same methodology is valid, and countries with a high percentage of prolonged surgical prophylaxis (Figure 69) may consider specific measures in this area.
. A. total of antimicrobial agents was reported in patients: 70.9% of the patients received one. antimicrobial, 23.4% received two and 5.7% received three or more antimicrobials. The overall prevalence of. antimicrobial use extrapolated to the total number of occupied beds in Europe was 32.7% (95% confidence. interval 29.4–36.2%). Η χωρα με το μεγαλυτερο ποσοστο νοσηλευομενων ασθενων υπο αντιμικροβιακή αγωγή …Το …% των χορηγουμενων αντιβιοτικων διδεται για. Μπορουμε να μειωσουμε κατά 20% το ποσό των χορηγουμενων αντιβιοτικων αν εφαρμοσουμε τις διεθνεις οδηγιες για 1 δοση χπρ. One has to bear in mind that the percentage of prolonged surgical prophylaxis is overestimated in the PPS, because a different recall period is used for surgical prophylaxis (24 hours before 8 am on the survey day) and a treatment given for more than one day has a higher probability of. being captured in the PPS study than a treatment given for one day only. Nonetheless, comparing this indicator between hospitals (and countries) using the same methodology is valid, and countries with a high percentage of prolonged surgical prophylaxis (Figure 69) may consider specific measures in this area.")
53
80% Εναντι 60% της χειρουργικης προφύλαξης στο σύνολο της ΕΕ
One has to bear in mind that the percentage of prolonged surgical prophylaxis is overestimated in the PPS, because a different recall period is used for surgical prophylaxis (24 hours before 8 am on the survey day) and a treatment given for more than one day has a higher probability of being captured in the PPS study than a treatment given for one day only. Nonetheless, comparing this indicator between hospitals (and countries) using the same methodology is valid, and countries with a high percentage of prolonged surgical prophylaxis (Figure 69) may consider specific measures in this area.
 and a treatment given for more than one day has a higher probability of. being captured in the PPS study than a treatment given for one day only. Nonetheless, comparing this indicator. between hospitals (and countries) using the same methodology is valid, and countries with a high percentage of. prolonged surgical prophylaxis (Figure 69) may consider specific measures in this area.")
54
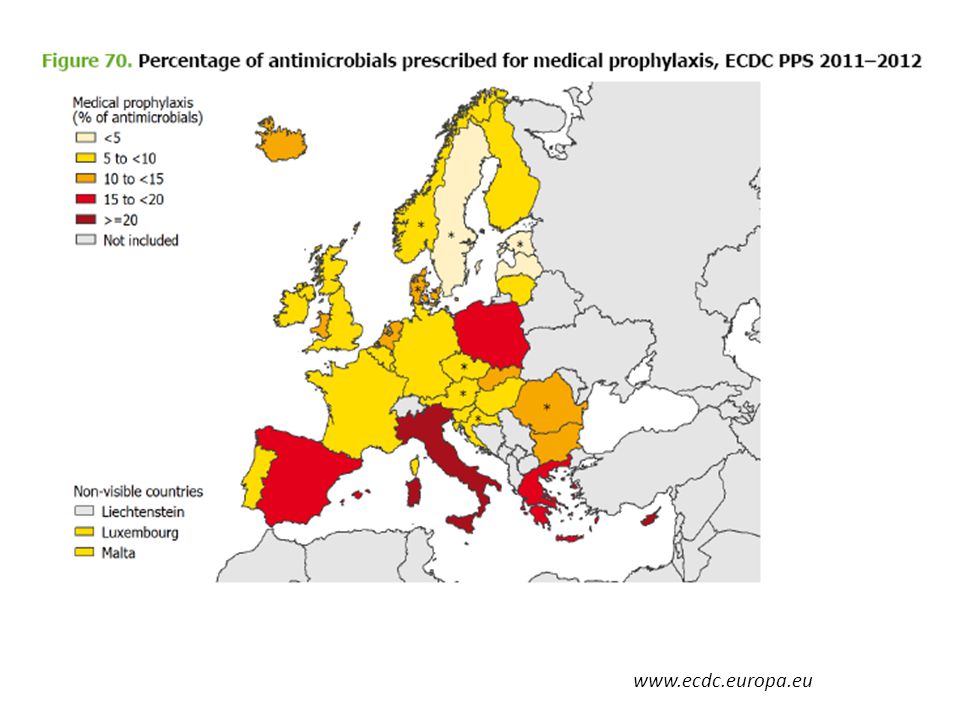
a considerable proportion of medical prophylaxis was prescribed for the prevention of urinary tract infections and prevention of fungal infections
55
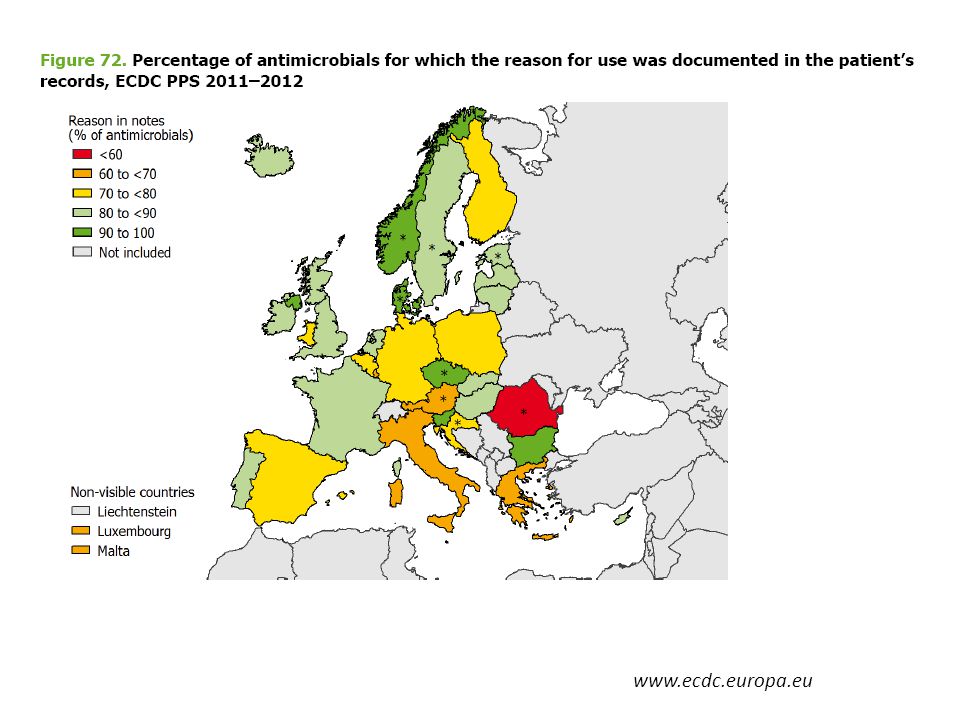
Αιτιολογημενη χορήγηση
56
Ποσοστά αντοχής στις Καρβαπενέμες
K.pneumoniae : 30-75% P.aeruginosa : 28-52% A.baumannii: 83-96%

57
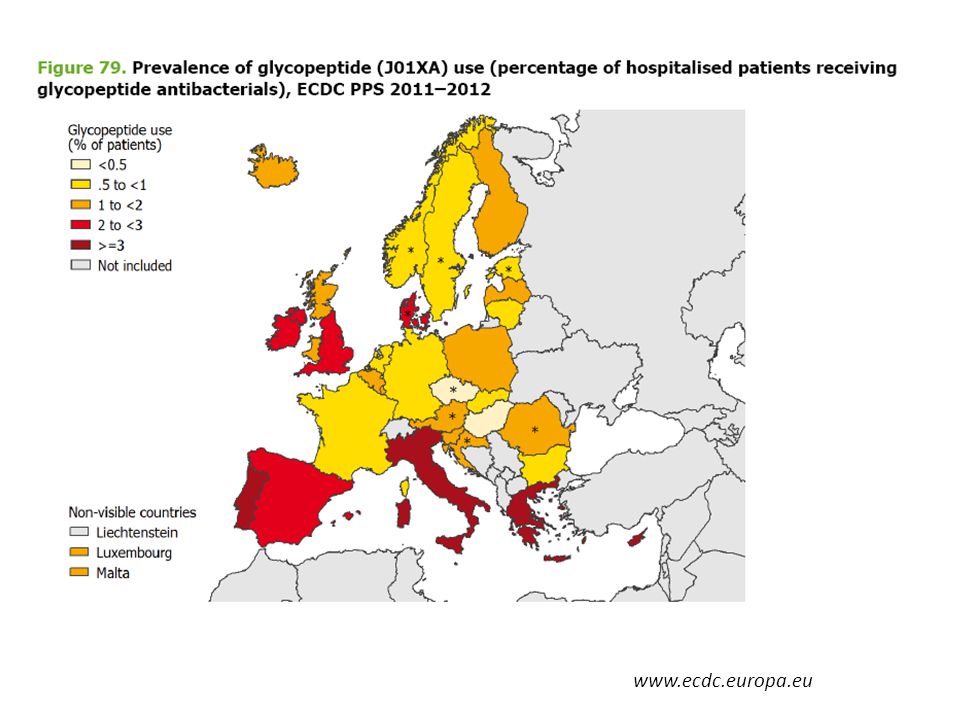
Σουηδία-Σκωτια >20% των νοσοκομειακων παθογονων
58
ΕΛΛΑΔΑ: ΚΑΤΑΝΟΜΗ ΝΟΣΟΚΟΜΕΙΑΚΩΝ ΠΑΘΟΓΟΝΩΝ, PPS 2011-2012
Αντίθετα από τον μεσο όρο των 33 χωρων της ΕΕ που συμμετείχαν όπου, ο σταφυλόκοκκος ήταν το 2ο συχνότερο παθογόνο μετα το κολοβακτηρίδιο στις νοσοκομειακες λοιμωξεις και 3ος ο εντερόκοκκος

59
Πότε χρειάζεται συνδυασμός αντιβιοτικών στην Ελληνική πραγματικότητα?
Αρχική εμπειρική θεραπεία στον βαρέως πάσχοντα σηπτικό ασθενή Αρχική εμπειρική θεραπεία στον ασθενή με HAP/VAP με παράγοντες κινδύνου Προηγούμενη νοσηλεία Λήψη αντιβιοτικών Ανοσοκαταστολή Διαμονή σε οίκο ευγηρίας Γνωστός αποικισμός 1.6 αντιβιοτικα/ασθενή Για διευρυνση του φασματος, ειδικα σε ασθενείς με προηγουμενη νοσηλεια και λήψη αντιβιοτικων-but there is insufficient evidence showing a benefit of a second agent for continued therapy once pathogens and antimicrobial susceptibilities are known The findings from this review as well as from several meta-analyses do not support the use of combination antimicrobial therapy for definitive treatment of infections with Gram-negative bacteria. It should be noted that combination therapy may have some value in a specific subset of patients with severe sepsis, and well-controlled randomized studies are necessary to answer this question. Λοίμωξη από K.pneumoniae που παράγει καρβαπενεμάση VAP από P.aeruginosa (για τις πρώτες 5 ημ.)
")
60
Στοχευμένη αντιμικροβιακή αγωγή στην Ελληνική πραγματικότητα
Περιττός ο συνδυασμός φαρμάκων με αντιαναερόβιο φάσμα (καρβαπενέμη ή συνδυασμοί με αναστολέα + μετρονιδαζόλη) Σπάνια χρειάζεται συνδυασμός με αντισταφυλοκοκκικό (10ο σε συχνότητα νοσοκομειακό παθογόνο στα Ελληνικά νοσοκομεία, συχνότητα 3%) Δεν έχει αποδειχθεί ότι οι συνδυασμοί αντιβιοτικών για τα Gram-αρνητικά υπερτερούν της μονοθεραπείας με εξαίρεση την Carb-R K.pneumoniae Ο αποικισμός δεν πρέπει να θεραπεύεται Αποκλιμάκωση της καρβαπενέμης τύπου 2 σε ερταπενέμη, όπου είναι δυνατόν Με την εννοια της συνεργειας-ουτε για ουδετεροπενικους, ουτε για Acinetobacter Αν δεν υπαρχουν άλλες επιλογες
 Σπάνια χρειάζεται συνδυασμός με αντισταφυλοκοκκικό (10ο σε συχνότητα νοσοκομειακό παθογόνο στα Ελληνικά νοσοκομεία, συχνότητα 3%) Δεν έχει αποδειχθεί ότι οι συνδυασμοί αντιβιοτικών για τα Gram-αρνητικά υπερτερούν της μονοθεραπείας με εξαίρεση την Carb-R K.pneumoniae. Ο αποικισμός δεν πρέπει να θεραπεύεται. Αποκλιμάκωση της καρβαπενέμης τύπου 2 σε ερταπενέμη, όπου είναι δυνατόν. Με την εννοια της συνεργειας-ουτε για ουδετεροπενικους, ουτε για Acinetobacter. Αν δεν υπαρχουν άλλες επιλογες.")
61
Σύγχρονη Ελληνική Πραγματικότητα:
Επείγουσα Ανάγκη για Ελληνικές Κατευθυντήριες Οδηγίες για τη χρήση καρβαπενεμών και κολιμυκίνης στα ελληνικά νοσοκομεία Αυστηρότερη επιτήρηση της εφαρμογής των οδηγιών για τη 1 δόση περιεγχειρητικής προφύλαξης στα ελληνικά νοσοκομεία

62
Sir Alexander Fleming, Nobel Prize Lecture, June 1945
“…. the public will demand [the drug and]…then will begin an era…of abuses. The microbes are educated to resist penicillin and a host of penicillin-fast organisms is bred out… which can be passed to other individuals…until they reach someone who gets a septicemia or a pneumonia which penicillin cannot save. In such cases the thoughtless person playing with penicillin is morally responsible for the death of the man who finally succumbs to infection with the penicillin-resistant organism. I hope this evil can be averted.” Sir Alexander Fleming, Nobel Prize Lecture, June 1945 Antimicrobial stewardship is a patient safety issue and a public health issue and must be taken seriously in all aspects of the continuum of patient care Improving antibiotic use is a public health imperative • Antibiotics are the only drug where use in one patient can impact the effectiveness in another. If everyone does not use antibiotics well, we will all suffer the consequences. Antibiotics are a shared resource, (and becoming a scarce resource). Antibiotics are societal drugs. Each individual use contributes to the sum total of society's antibiotic exposure LEVY SB 1997
. Antibiotics are societal drugs. Each individual use contributes to the sum total of society s antibiotic exposure LEVY SB")
Παρόμοιες παρουσιάσεις












 1 1.>")






