Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Κλινική εικόνα και παθοφυσιολογία του συνδρόμου Cushing
Γ. Ντάιος Πανεπιστημιακή Παθολογική Κλινική & Ομώνυμο Ερευνητικό Εργαστήριο ΠΘ 6ο Ετήσιο Μετεκπαιδευτικό Πρόγραμμα Λάρισα 23/01/2014

2
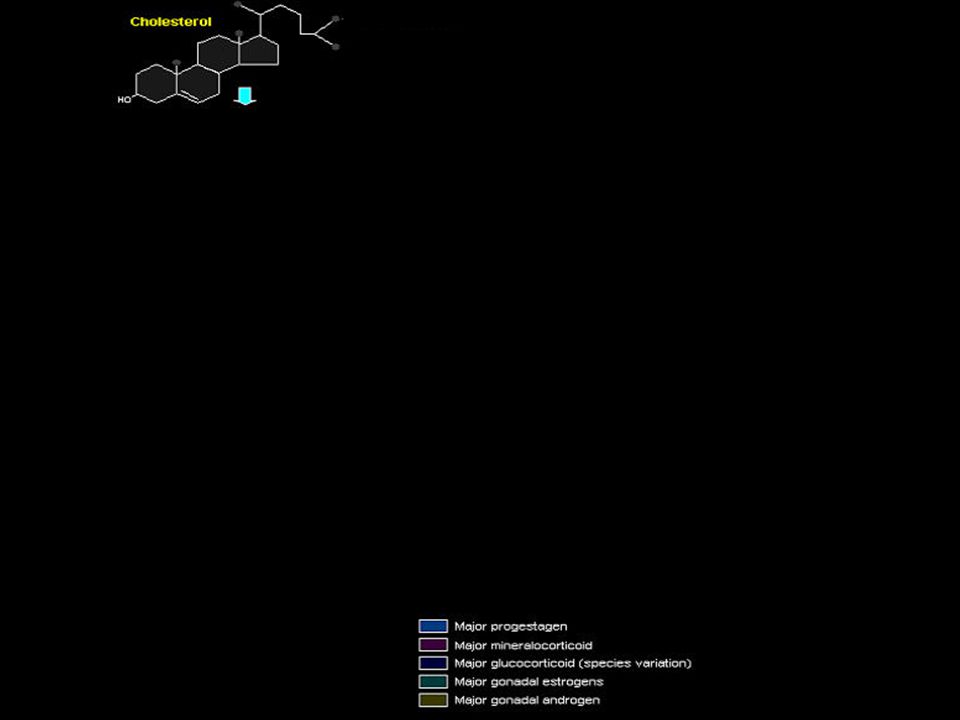
Mια εξωτερική σπειροειδή ζώνη, που παράγει αλατοκορτικοειδή (κυρίως αλδοστερόνη)
Μια μέση στηλιδωτή ζώνη, που παράγει γλυκοκορτικοειδή (κυρίως κορτιζόλη, κορτικοστερόνη και κορτιζόνη) Μια εσωτερική δικτυωτή ζώνη, που παράγει ανδρογόνα
 Μια εσωτερική δικτυωτή ζώνη, που παράγει ανδρογόνα.")
4
Circadian rythm Stress CRH POMC Cortisol ACTH

8
Δράση της κορτιζόλης στον μεταβολισμό των πρωτεϊνών
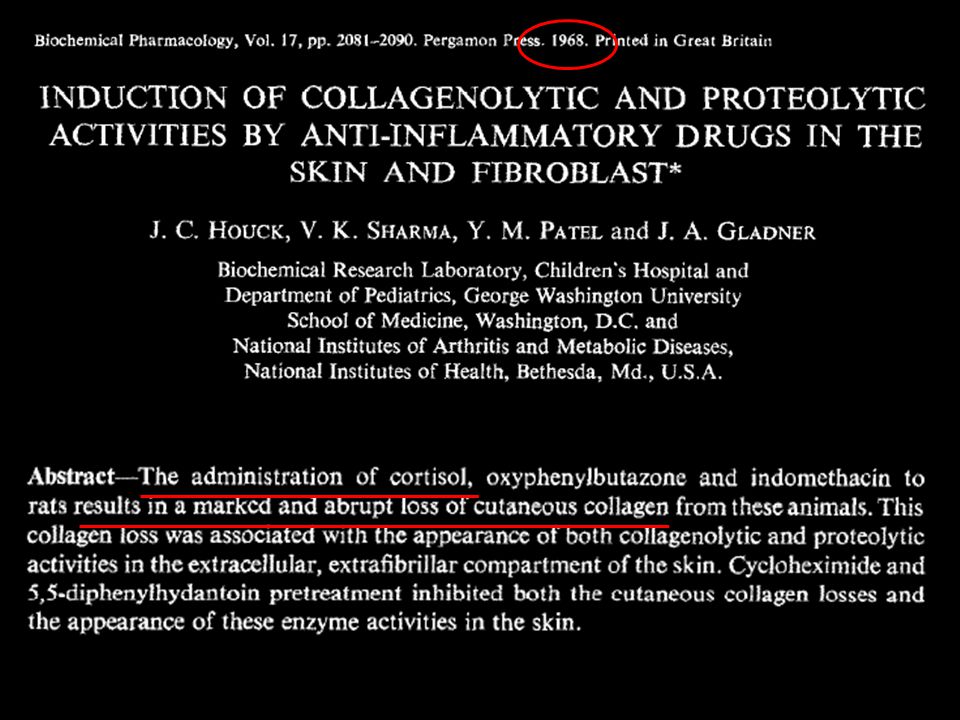
Even the protein collagen fibers in the subcutaneous tissue are diminished so that Chapter 77 Adrenocortical Hormones 959 the subcutaneous tissues tear easily, resulting in development of large purplish striae where they have torn apart.

9
Πρωτεϊνόλυση

10
Weakness and proximal muscle wasting are common in Cushing's syndrome, being induced by the catabolic effects of excess glucocorticoid on skeletal muscle (picture 11). As a result, many patients cannot rise from a squatting position without assistance; patients with more severe disease may be unable to climb stairs or get up from a deep chair. The catabolic effects of cortisol are amplified by physical inactivity [42]. (See "Glucocorticoid-induced myopathy".)
.")
13
Skin atrophy — The skin usually atrophies, the stratum corneum is thinned, and there is loss of subcutaneous fat to a sufficient degree that subcutaneous blood vessels may be seen [30]. The skin eventually becomes fragile due to these changes and, in extreme cases, peels off after being covered with adhesive tape. Minor wounds heal slowly, and surgical wounds may dehisce. Such changes should be considered in the context of gender and age differences in skin thickness, with men and younger individuals having greater skin thickness.
![Skin atrophy — The skin usually atrophies, the stratum corneum is thinned, and there is loss of subcutaneous fat to a sufficient degree that subcutaneous blood vessels may be seen [30].](http://slideplayer.gr/slide/2332874/8/images/13/Skin+atrophy+%E2%80%94+The+skin+usually+atrophies%2C+the+stratum+corneum+is+thinned%2C+and+there+is+loss+of+subcutaneous+fat+to+a+sufficient+degree+that+subcutaneous+blood+vessels+may+be+seen+%5B30%5D..jpg "The skin eventually becomes fragile due to these changes and, in extreme cases, peels off after being covered with adhesive tape. Minor wounds heal slowly, and surgical wounds may dehisce. Such changes should be considered in the context of gender and age differences in skin thickness, with men and younger individuals having greater skin thickness..")
14
Easy bruisability — Loss of subcutaneous connective tissue due to the catabolic effects of glucocorticoid results in easy bruising after minimal, often unremembered injury (picture 5). Extensive ecchymoses at venipuncture sites are also common, and it is often difficult to maintain intravenous lines without fluid infiltration into the surrounding tissues. As a result, patients with Cushing's syndrome are sometimes thought to have senile purpura or a bleeding diathesis

16
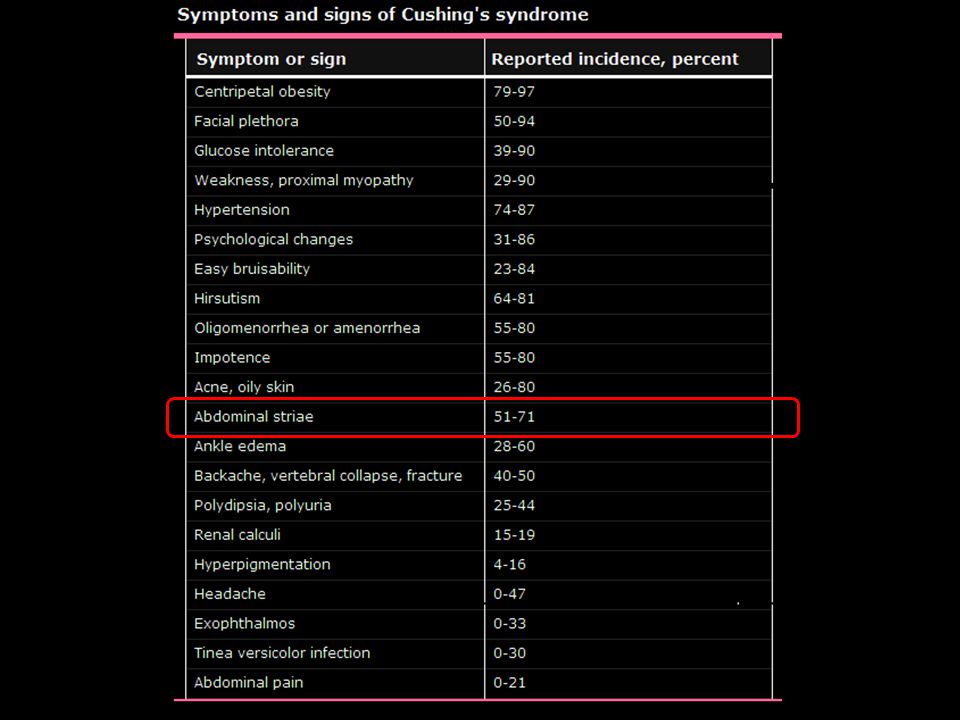
Striae — Purple striae occur as the fragile skin stretches due to the enlarging trunk, breasts, and abdomen (picture 6). The striae appear as wide, reddish-purple streaks because the increasingly thin skin does not hide the color of venous blood in the underlying dermis. Striae occur most often in younger patients, can be numerous, and are most common on the abdomen and lower flanks; however, they can also occur on the breasts, hips, buttocks, shoulders, upper thighs, upper arms, and axillae The glucocorticoid hormones responsible for the development of stretch marks affect the dermis by preventing the fibroblasts from forming collagen and elastin fibers, necessary to keep rapidly growing skin taut. This creates a lack of supportive material, as the skin is stretched and leads to dermal and epidermal tearing. Skin subjected to more stretching force than it can handle will tear. Hormonal changes and genetics influence the skin's capacity to withstand stretching forces, as do diet and (possibly) exercise
 exercise.")
18
Δράση της κορτιζόλης στον μεταβολισμό της γλυκόζης
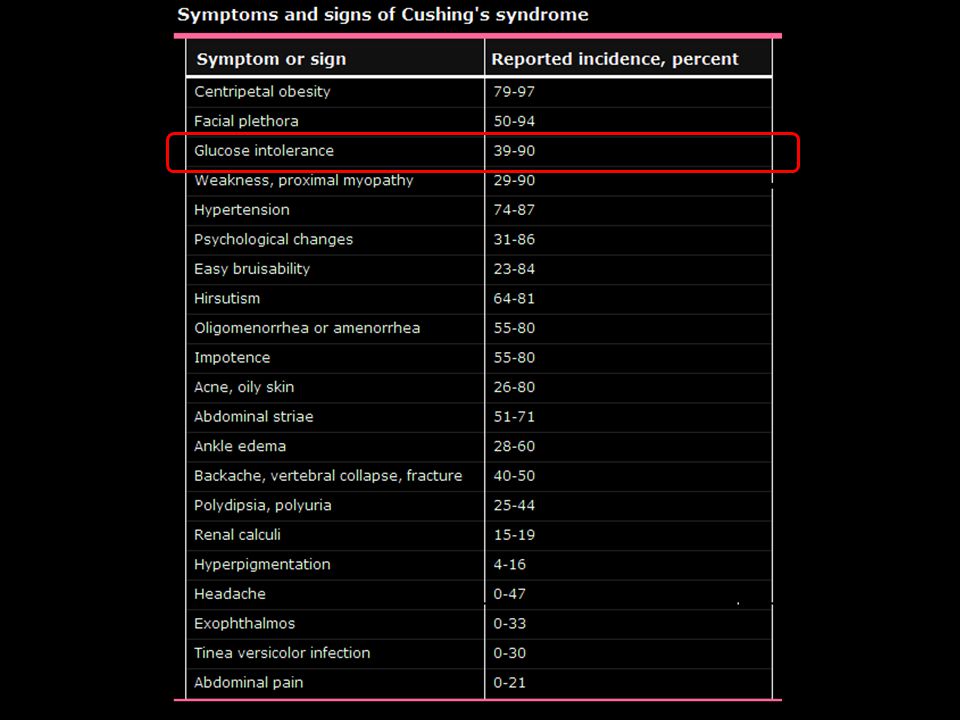
Cortisol also causes a moderate decrease in the rate of glucose utilization by most cells in the body. Although the cause of this decrease is unknown, most physiologists believe that somewhere between the point of entry of glucose into the cells and its final degradation, cortisol directly delays the rate of glucose utilization. A suggested mechanism is based on the observation that glucocorticoids depress the oxidation of nicotinamide-adenine dinucleotide (NADH) to form NAD+. Because NADH must be oxidized to allow glycolysis, this effect could account for the diminished utilization of glucose by the cells. Both the increased rate of gluconeogenesis and the moderate reduction in the rate of glucose utilization by the cells cause the blood glucose concentrations to rise. The rise in blood glucose in turn stimulates secretion of insulin. The increased plasma levels of insulin, however, are not as effective in maintaining plasma glucose as they are under normal conditions. For reasons that are not entirely clear, high levels of glucocorticoid reduce the sensitivity of many tissues, especially skeletal muscle and adipose tissue, to the stimulatory effects of insulin on glucose uptake and utilization. One possible explanation is that high levels of fatty acids, caused by the effect of glucocorticoids to mobilize lipids from fat depots, may impair insulin’s actions on the tissues. In this way, excess secretion of glucocorticoids may produce disturbances of carbohydrate metabolism very similar to those found in patients with excess levels of growth hormone. The increase in blood glucose concentration is occasionally great enough (50 per cent or more above normal) that the condition is called adrenal diabetes. Administration of insulin lowers the blood glucose concentration only a moderate amount in adrenal diabetes-not nearly as much as it does in pancreatic 0.0 3.0 2.0 1.0 Control ACE inhibitor + Ang II infusion ACE inhibitor Plasma cortisol (mg/100 ml) 20 50 40 30 Plasma aldosterone (ng/100 ml) Figure 77–4 Effects of treating sodium-depleted dogs with an angiotensinconverting enzyme (ACE) inhibitor for 7 days to block formation of angiotensin II (Ang II) and of infusing exogenous Ang II to restore plasma Ang II levels after ACE inhibition. Note that blocking Ang II formation reduced plasma aldosterone concentration with little effect on cortisol, demonstrating the important role of Ang II in stimulating aldosterone secretion during sodium depletion. (Drawn from data in Hall JE, Guyton AC, Smith MJ Jr, Coleman TG: Chronic blockade of angiotensin II formation during sodium deprivation. Am J Physiol 237:F424, 1979.) 952 Unit XIV Endocrinology and Reproduction diabetes-because the tissues are resistant to the effects of insulin.
 to form NAD+. Because NADH must be oxidized to allow glycolysis, this effect could account for the diminished utilization of glucose by the cells. Both the increased rate of gluconeogenesis and the. moderate reduction in the rate of glucose utilization. by the cells cause the blood glucose concentrations to. rise. The rise in blood glucose in turn stimulates. secretion of insulin. The increased plasma levels of. insulin, however, are not as effective in maintaining. plasma glucose as they are under normal conditions. For reasons that are not entirely clear, high levels. of glucocorticoid reduce the sensitivity of many. tissues, especially skeletal muscle and adipose tissue, to the stimulatory effects of insulin on glucose uptake. and utilization. One possible explanation is that high. levels of fatty acids, caused by the effect of glucocorticoids. to mobilize lipids from fat depots, may impair. insulin’s actions on the tissues. In this way, excess. secretion of glucocorticoids may produce disturbances. of carbohydrate metabolism very similar to those. found in patients with excess levels of growth. hormone. The increase in blood glucose concentration is occasionally. great enough (50 per cent or more above. normal) that the condition is called adrenal diabetes. Administration of insulin lowers the blood glucose. concentration only a moderate amount in adrenal. diabetes-not nearly as much as it does in pancreatic Control ACE inhibitor. + Ang II infusion. ACE. inhibitor. Plasma cortisol. (mg/100 ml) Plasma aldosterone. (ng/100 ml) Figure 77–4. Effects of treating sodium-depleted dogs with an angiotensinconverting. enzyme (ACE) inhibitor for 7 days to block formation. of angiotensin II (Ang II) and of infusing exogenous Ang II to. restore plasma Ang II levels after ACE inhibition. Note that blocking. Ang II formation reduced plasma aldosterone concentration. with little effect on cortisol, demonstrating the important role of. Ang II in stimulating aldosterone secretion during sodium depletion. (Drawn from data in Hall JE, Guyton AC, Smith MJ Jr, Coleman TG: Chronic blockade of angiotensin II formation during. sodium deprivation. Am J Physiol 237:F424, 1979.) 952 Unit XIV Endocrinology and Reproduction. diabetes-because the tissues are resistant to the effects. of insulin.")
19
Γλυκονεογένεση One of the principal effects of cortisol on the metabolic systems of the body is reduction of the protein stores in essentially all body cells except those of the liver. This is caused by both decreased protein synthesis and increased catabolism of protein already in the cells. Both these effects may result from decreased amino acid transport into extrahepatic tissues, as discussed later; this probably is not the major cause, because cortisol also depresses the formation of RNA and subsequent protein synthesis in many extrahepatic tissues, especially in muscle and lymphoid tissue. In the presence of great excesses of cortisol, the muscles can become so weak that the person cannot rise from the squatting position. And the immunity functions of the lymphoid tissue can be decreased to a small fraction of normal.

20
By far the best-known metabolic effect of cortisol and other glucocorticoids on metabolism is their ability to stimulate gluconeogenesis (formation of carbohydrate from proteins and some other substances) by the liver, often increasing the rate of gluconeogenesis as much as 6- to 10-fold. This results mainly from two effects of cortisol. 1. Cortisol increases the enzymes required to convert amino acids into glucose in the liver cells. This results from the effect of the glucocorticoids to activate DNA transcription in the liver cell nuclei in the same way that aldosterone functions in the renal tubular cells, with formation of messenger RNAs that in turn lead to the array of enzymes required for gluconeogenesis. 2. Cortisol causes mobilization of amino acids from the extrahepatic tissues mainly from muscle. As a result, more amino acids become available in the plasma to enter into the gluconeogenesis process of the liver and thereby to promote the formation of glucose. One of the effects of increased gluconeogenesis is a marked increase in glycogen storage in the liver cells. This effect of cortisol allows other glycolytic hormones, such as epinephrine and glucagon, to mobilize glucose in times of need, such as between meals.
 by the liver, often increasing the rate of gluconeogenesis as much as 6- to 10-fold. This results mainly from two effects of cortisol. 1. Cortisol increases the enzymes required to convert amino acids into glucose in the liver cells. This results from the effect of the glucocorticoids to activate DNA transcription in the liver cell nuclei in the same way that aldosterone functions in the renal tubular cells, with formation of messenger RNAs that in turn lead to the array of enzymes required for gluconeogenesis. 2. Cortisol causes mobilization of amino acids from the extrahepatic tissues mainly from muscle. As a result, more amino acids become available in the plasma to enter into the gluconeogenesis process of the liver and thereby to promote the formation of glucose. One of the effects of increased gluconeogenesis is a marked increase in glycogen storage in the liver cells. This effect of cortisol allows other glycolytic hormones, such as epinephrine and glucagon, to mobilize glucose in times of need, such as between meals.")
21
Γλυκονεογένεση Ινσουλινοαντίσταση Cell
One of the principal effects of cortisol on the metabolic systems of the body is reduction of the protein stores in essentially all body cells except those of the liver. This is caused by both decreased protein synthesis and increased catabolism of protein already in the cells. Both these effects may result from decreased amino acid transport into extrahepatic tissues, as discussed later; this probably is not the major cause, because cortisol also depresses the formation of RNA and subsequent protein synthesis in many extrahepatic tissues, especially in muscle and lymphoid tissue. In the presence of great excesses of cortisol, the muscles can become so weak that the person cannot rise from the squatting position. And the immunity functions of the lymphoid tissue can be decreased to a small fraction of normal. Cell

23
Δράση της κορτιζόλης στον μεταβολισμό του λίπους

24
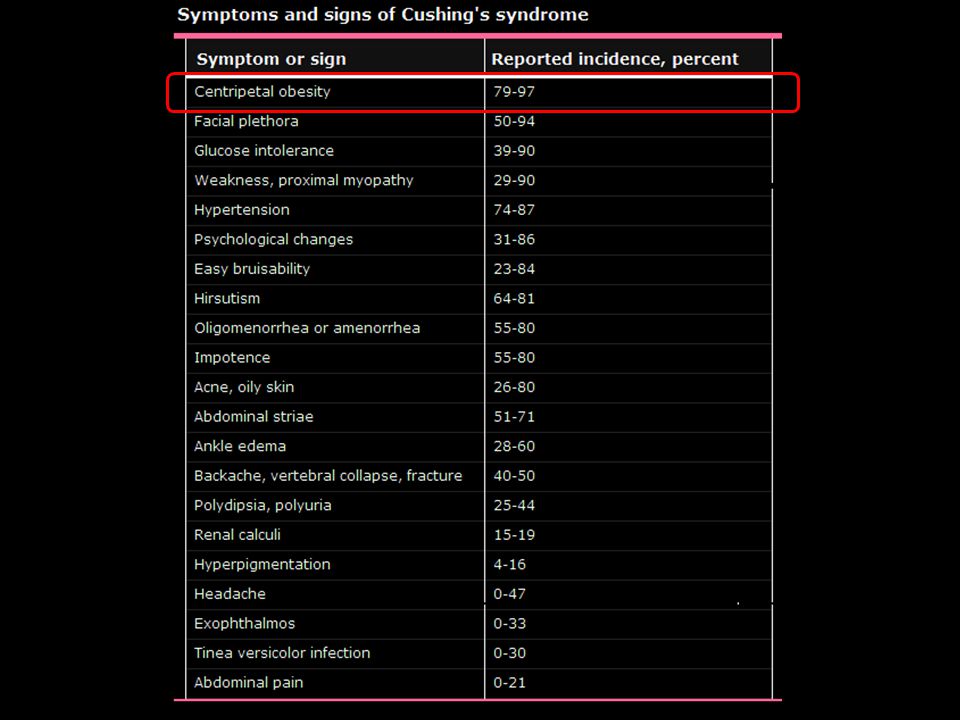
The most common feature of patients with Cushing's syndrome is progressive central (centripetal) obesity (picture 1), usually involving the face, neck, trunk, abdomen (picture 2), and, internally, spinal canal and mediastinum [21,22]. The extremities are usually spared and may be wasted. Some authors report generalized obesity in a majority of adults with Cushing’s syndrome [20].
![The most common feature of patients with Cushing s syndrome is progressive central (centripetal) obesity (picture 1), usually involving the face, neck, trunk, abdomen (picture 2), and, internally, spinal canal and mediastinum [21,22].](http://slideplayer.gr/slide/2332874/8/images/24/The+most+common+feature+of+patients+with+Cushing+s+syndrome+is+progressive+central+%28centripetal%29+obesity+%28picture+1%29%2C+usually+involving+the+face%2C+neck%2C+trunk%2C+abdomen+%28picture+2%29%2C+and%2C+internally%2C+spinal+canal+and+mediastinum+%5B21%2C22%5D..jpg "The extremities are usually spared and may be wasted. Some authors report generalized obesity in a majority of adults with Cushing’s syndrome [20]..")
26
Large doses of glucocorticoids lead to redistribution of fat to the upper trunk and face, with a concomitant loss of fat in the extremities.35 The mechanism for this effect is not understood, although these apparently paradoxical responses may result from differences in the number of glucocorticoid receptors in different types of fat cells.36 By this hypothesis, cells with fewer receptors would be spared the effects of glucocorticoids on glucose transport. Therefore, glucose and triglyceride accumulation would occur in response to the rise in insulin levels. Fat cells containing higher levels of receptor (perhaps in the periphery) would respond to the high glucocorticoid level by decreasing glucose uptake and would not accumulate triglycerides. Alternatively, cells in the extremities may be less sensitive to insulin.37 The mobilization of fat from peripheral depots by epinephrine and other lipolytics is severely blunted in the absence of glucocorticoids.38 Cortisol facilitates the response of adipocytes to the rise in cAMP induced by these agents rather than creating a larger increase in the amount of cAMP. Steroids. 1987 Jun;49(6): Differential binding of dexamethasone to ammonium sulfate precipitates of human adipose tissue cytosols. Miller LK , Kral JG , Strain GW , Zumoff B . Source Department of Medicine, Beth Israel Medical Center, New York, NY Abstract Saturation analysis of the binding of [3H]dexamethasone [( 3H]DEX) to ammonium sulfate precipitates (ASPs) confirmed the presence of a limited-capacity, high-affinity binder in human adipose tissue cytosols. Various non-radioactive steroids competed with [3H]DEX for binding to the ASPs in the following sequence: dexamethasone (DEX) approximately equal to triamcinolone acetonide (TA) greater than progesterone (P) much greater than estradiol (E2). The steroid specificity of the binder precipitated by AS was consistent with the specificities reported for glucocorticoid receptors in a number of systems. In order to investigate possible regional differences, glucocorticoid binding to ASPs derived from adipose tissues removed from two different sites in the same subject was quantitated. ASPs of human omental adipose tissue bound significantly more [3H]DEX than did similar preparations of subcutaneous adipose tissue from the abdominal wall (116 +/- 32 vs. 50 +/- 22 fmol/mg protein; mean +/- SD; p less than 0.02). The findings are consistent with reports from other laboratories suggesting that intra-abdominal fat is more responsive to glucocorticoids than is subcutaneous adipose tissue.
: Differential binding of dexamethasone to ammonium sulfate precipitates of human adipose tissue cytosols. Miller LK , Kral JG , Strain GW , Zumoff B . Source. Department of Medicine, Beth Israel Medical Center, New York, NY Abstract. Saturation analysis of the binding of [3H]dexamethasone [( 3H]DEX) to ammonium sulfate precipitates (ASPs) confirmed the presence of a limited-capacity, high-affinity binder in human adipose tissue cytosols. Various non-radioactive steroids competed with [3H]DEX for binding to the ASPs in the following sequence: dexamethasone (DEX) approximately equal to triamcinolone acetonide (TA) greater than progesterone (P) much greater than estradiol (E2). The steroid specificity of the binder precipitated by AS was consistent with the specificities reported for glucocorticoid receptors in a number of systems. In order to investigate possible regional differences, glucocorticoid binding to ASPs derived from adipose tissues removed from two different sites in the same subject was quantitated. ASPs of human omental adipose tissue bound significantly more [3H]DEX than did similar preparations of subcutaneous adipose tissue from the abdominal wall (116 +/- 32 vs. 50 +/- 22 fmol/mg protein; mean +/- SD; p less than 0.02). The findings are consistent with reports from other laboratories suggesting that intra-abdominal fat is more responsive to glucocorticoids than is subcutaneous adipose tissue.")
27
The most common feature of patients with Cushing's syndrome is progressive central (centripetal) obesity (picture 1), usually involving the face, neck, trunk, abdomen (picture 2), and, internally, spinal canal and mediastinum [21,22]. The extremities are usually spared and may be wasted. Some authors report generalized obesity in a majority of adults with Cushing’s syndrome [20].
![The most common feature of patients with Cushing s syndrome is progressive central (centripetal) obesity (picture 1), usually involving the face, neck, trunk, abdomen (picture 2), and, internally, spinal canal and mediastinum [21,22].](http://slideplayer.gr/slide/2332874/8/images/27/The+most+common+feature+of+patients+with+Cushing+s+syndrome+is+progressive+central+%28centripetal%29+obesity+%28picture+1%29%2C+usually+involving+the+face%2C+neck%2C+trunk%2C+abdomen+%28picture+2%29%2C+and%2C+internally%2C+spinal+canal+and+mediastinum+%5B21%2C22%5D..jpg "The extremities are usually spared and may be wasted. Some authors report generalized obesity in a majority of adults with Cushing’s syndrome [20]..")
28
Αναστέλλει την συσσώρευση τριγλυκεριδίων μέσα στα λιποκύτταρα
Κινητοποιεί το λίπος από τις αποθήκες

30
30-year-old woman with Cushing's disease showing round, plethoric "moon" face, facial hirsutism, and increased supraclavicular fat pads. Reprinted with permission from: Williams Textbook of Endocrinology, 8th ed, Foster, DW, Wilson, JD (Eds), WB Saunders, Philadelphia, 1996. Fat accumulation in the cheeks results in a "moon" face that sometimes obscures the ears when a patient is examined from the front (picture 3). Fat deposition in the temporal fossae also contributes to facial rounding. Enlarged fat pads that fill the supraclavicular fossae and obscure the clavicles is one of the most specific signs of Cushing's syndrome [20], although they occasionally occur in exogenous obesity. The bulging supraclavicular fat pads make the neck appear thick and shortened (picture 3). Retroorbital fat deposition may result in exophthalmos, which is present in up to 5 percent of patients [24,25].
, WB Saunders, Philadelphia, Fat accumulation in the cheeks results in a moon face that sometimes obscures the ears when a patient is examined from the front (picture 3). Fat deposition in the temporal fossae also contributes to facial rounding. Enlarged fat pads that fill the supraclavicular fossae and obscure the clavicles is one of the most specific signs of Cushing s syndrome [20], although they occasionally occur in exogenous obesity. The bulging supraclavicular fat pads make the neck appear thick and shortened (picture 3). Retroorbital fat deposition may result in exophthalmos, which is present in up to 5 percent of patients [24,25].")
31
25-year-old woman with Cushing's disease who has facial hirsutism and acne, increased supraclavicular fat pads, and a dorsocervical fat pad ("buffalo hump"). Courtesy of David N Orth, MD A "buffalo hump" or dorsocervical fat pad is common and is usually consistent with the general degree of obesity (picture 4).
.")
32
Cushing και ανάπτυξη του παιδιού

33
Chronological height and weight chart of a boy who developed overt Cushing's disease at about age seven years. He stopped growing and minimized his weight gain for about five years with a strict diet and vigorous exercise program. He was treated with conventional megavoltage pituitary irradiation at age 13 years (arrows). He resumed growth at the same velocity as boys of his age, but there was no catch-up growth. Reprinted with permission from Williams Textbook of Endocrinology, 8th ed, Foster, DW, Wilson, JD (Eds), WB Saunders, Philadelphia, 1996. Children with Cushing's syndrome almost invariably have generalized obesity and growth retardation; the latter may be the first indication of glucocorticoid excess. As a result, any child whose weight rises and height falls in percentile rank as compared with age-matched normal children should be considered to have Cushing's syndrome until proven otherwise (figure 1). These abnormalities both improve after successful treatment of patients whose bones have not yet fused [23].
, WB Saunders, Philadelphia, Children with Cushing s syndrome almost invariably have generalized obesity and growth retardation; the latter may be the first indication of glucocorticoid excess. As a result, any child whose weight rises and height falls in percentile rank as compared with age-matched normal children should be considered to have Cushing s syndrome until proven otherwise (figure 1). These abnormalities both improve after successful treatment of patients whose bones have not yet fused [23].")
34
GHRH CORTISOL GH IGF-1

35
Chronological height and weight chart of a boy who developed overt Cushing's disease at about age seven years. He stopped growing and minimized his weight gain for about five years with a strict diet and vigorous exercise program. He was treated with conventional megavoltage pituitary irradiation at age 13 years (arrows). He resumed growth at the same velocity as boys of his age, but there was no catch-up growth. Reprinted with permission from Williams Textbook of Endocrinology, 8th ed, Foster, DW, Wilson, JD (Eds), WB Saunders, Philadelphia, 1996. Children with Cushing's syndrome almost invariably have generalized obesity and growth retardation; the latter may be the first indication of glucocorticoid excess. As a result, any child whose weight rises and height falls in percentile rank as compared with age-matched normal children should be considered to have Cushing's syndrome until proven otherwise (figure 1). These abnormalities both improve after successful treatment of patients whose bones have not yet fused [23].
, WB Saunders, Philadelphia, Children with Cushing s syndrome almost invariably have generalized obesity and growth retardation; the latter may be the first indication of glucocorticoid excess. As a result, any child whose weight rises and height falls in percentile rank as compared with age-matched normal children should be considered to have Cushing s syndrome until proven otherwise (figure 1). These abnormalities both improve after successful treatment of patients whose bones have not yet fused [23].")
36
Δράση της κορτιζόλης στα χαρακτηριστικά του φύλου
The major source of androgens in women is the adrenal glands [36]. As a result, women with Cushing's syndrome often have signs of androgen excess [37]. In contrast, the major source of androgens in men is the testes [38]. Thus, men with Cushing's syndrome do not have signs of androgen excess because cortisol has no androgenic activity [39]. Signs of androgen excess in Cushing's syndrome are most common in women with adrenal carcinomas [10,15]. These tumors usually secrete large amounts of androgenic precursors because they are inefficient at converting cholesterol to cortisol [40,41]. In comparison, signs of androgen excess are usually mild in women with ACTH-dependent Cushing's syndrome and do not occur in women with adrenal adenomas [15]. Menstrual irregularities — Menstrual irregularities are common in women with Cushing's syndrome. In one series of 45 women with newly diagnosed Cushing's disease, 80 percent had abnormal menstrual cycles; 31 percent had oligomenorrhea, 33 percent had amenorrhea, and the remainder had excess or variable menses [34]. The menstrual abnormalities correlated with increased serum cortisol and decreased serum estradiol concentrations, but not with serum androgen concentrations. The menstrual irregularities may be due to suppression of secretion of gonadotropin-releasing hormone by hypercortisolemia [35].

37
Hirsutism, which is usually mild and limited to the face, but can be generalized. Downy sideburns and increased hair on the upper lip and under the chin are most common (picture 3). The scalp hair often becomes thin, but temporal balding is rare.
. The scalp hair often becomes thin, but temporal balding is rare..")
38
Amenorrhea: This dysfunction typically results from the effects of the high levels of adrenal gland hormones to suppress the normal pituitary hormones LH and FSH, that regulate reproductive function. Male incompetence: High levels of adrenal steroids such as cortisol in Cushing's syndrome can directly suppress the ability of the testes to make testosterone. In addition, high levels of cortisol and related hormones also interfere with the ability of the normal pituitary gland to secrete LH and FSH, the two pituitary hormones needed for normal male reproductive function.

39
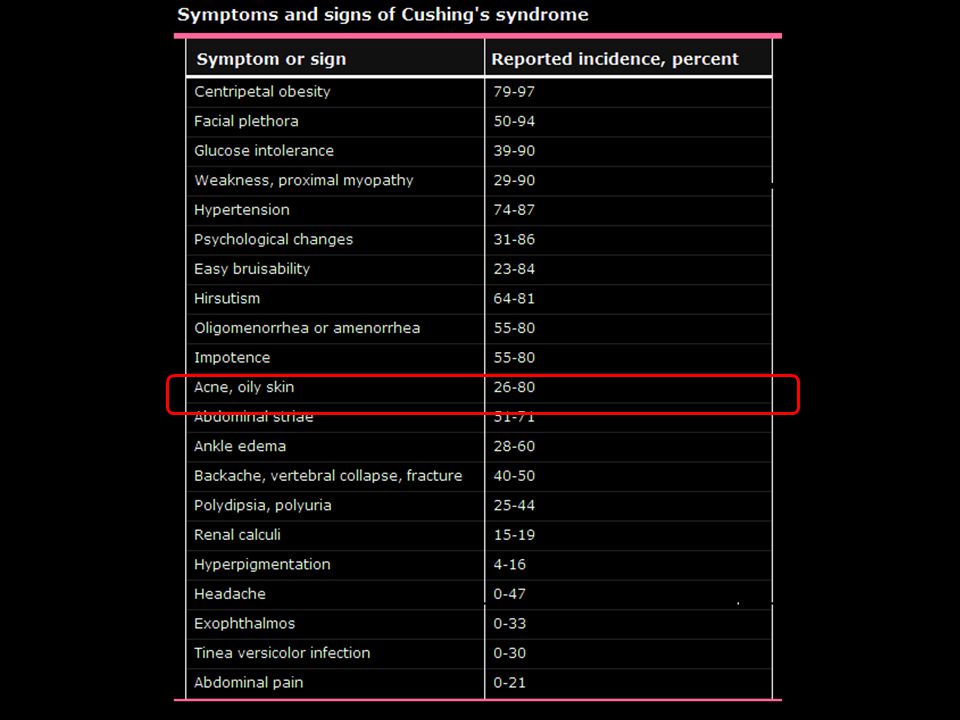
Oily facial skin and acne on the face, neck, or shoulders.

41
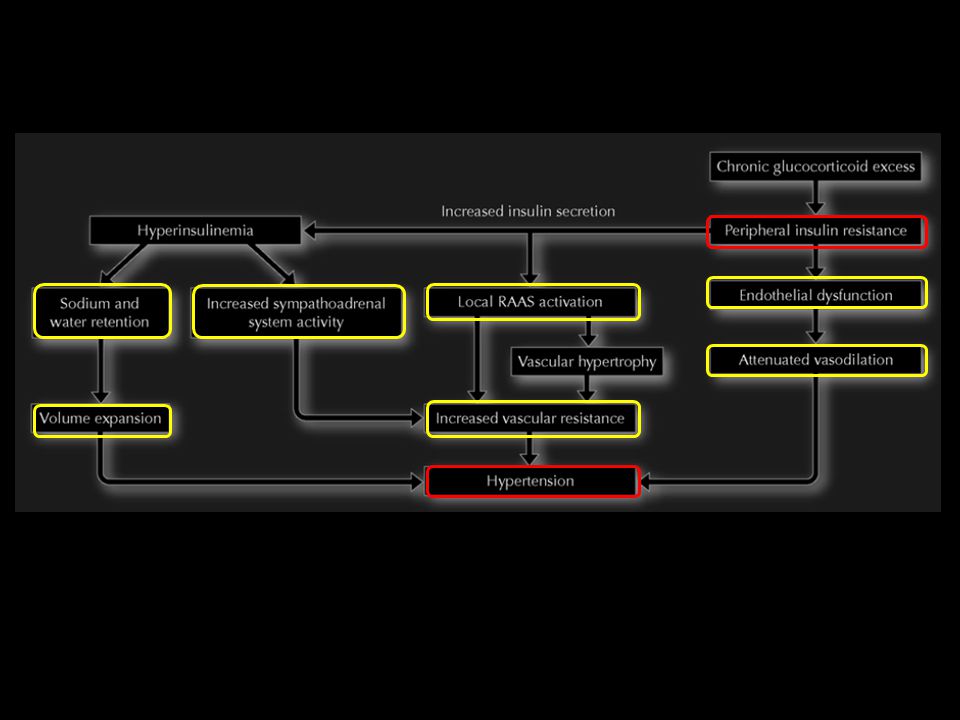
Cushing και αρτηριακή υπέρταση

42
Hypokalemia, due to increased mineralocorticoid activity, can accentuate the weakness in patients with severe hypercortisolism. On the other hand, a high-protein diet and exercise may improve muscle wasting and increase strength.

43
Excess cortisol exceeds the capacity of 11b-hydroxysteroid dehydrogenase type 2 (11b-HSD2), to convert cortisol to the inactive cortisone, making it available to bind to the mineralocorticoid receptor and behave like excess aldosterone. NAD, nicotinamide adenine dinucleotide.

44
Enzyme dependence of mineralocorticoid target tissue specificity
Enzyme dependence of mineralocorticoid target tissue specificity. In mineralocorticoid target organs, aldosterone binds to the mineralocorticoid receptor (MR), and thereafter the ligand–receptor complex is translocated into the nucleus. Binding to its hormone response element (HRE) increases the transcription of genes encoding specific aldosterone-inducible proteins, such as the rate-limiting subunits of the apical epithelial sodium channel (ENaC), sgk-1 and basolateral Na/K-ATPase. In turn, this stimulates sodium (Na+) reabsorption and potassium (K+) excretion. In vitro, aldosterone and cortisol have similar affinity to the MR, yet only aldosterone acts as the physiologic MR agonist. The enzyme 11-hydroxysteroid dehydrogenase type 2 (11HSD2) largely (90%) converts cortisol to inactive cortisone, thereby protecting the MR from activation by cortisol. Inhibition of 11HSD2 activity by glycyrrhetinic acid, the active compound of licorice, increases the intracellular cortisol level, leading to activation of the MR by cortisol. The resulting glucocorticoid activation of the MR produces the same effects as stimulation of the MR by aldosterone. NAD, nicotinamide adenine dinucleotide; NADH, reduced form of NAD.
, and thereafter the ligand–receptor complex is translocated into the nucleus. Binding to its hormone response element (HRE) increases the transcription of genes encoding specific aldosterone-inducible proteins, such as the rate-limiting subunits of the apical epithelial sodium channel (ENaC), sgk-1 and basolateral Na/K-ATPase. In turn, this stimulates sodium (Na+) reabsorption and potassium (K+) excretion. In vitro, aldosterone and cortisol have similar affinity to the MR, yet only aldosterone acts as the physiologic MR agonist. The enzyme 11-hydroxysteroid dehydrogenase type 2 (11HSD2) largely (90%) converts cortisol to inactive cortisone, thereby protecting the MR from activation by cortisol. Inhibition of 11HSD2 activity by glycyrrhetinic acid, the active compound of licorice, increases the intracellular cortisol level, leading to activation of the MR by cortisol. The resulting glucocorticoid activation of the MR produces the same effects as stimulation of the MR by aldosterone. NAD, nicotinamide adenine dinucleotide; NADH, reduced form of NAD.")
46
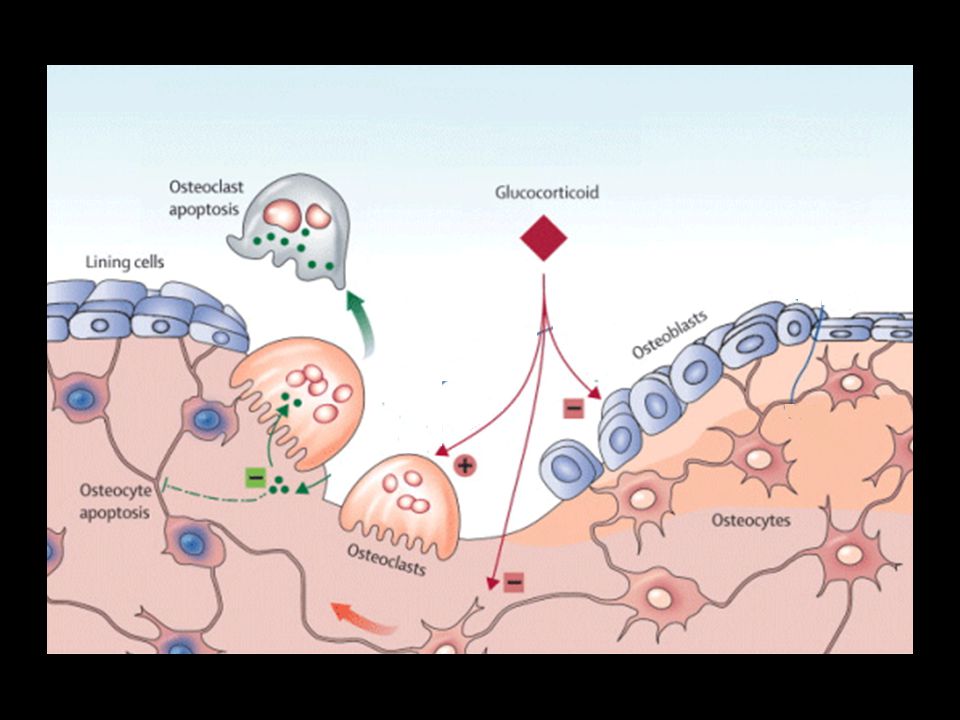
Cushing και οστικός μεταβολισμός

49
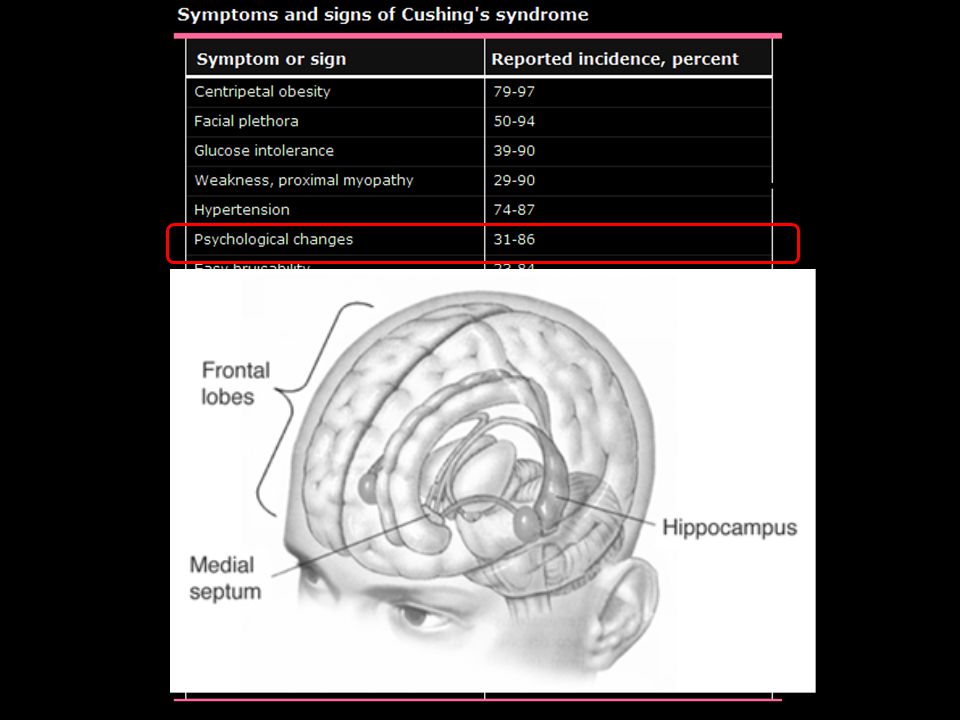
Cushing και νευροψυχιατρικά συμπτώματα

51
Cushing και ανοσιακή απάντηση

52
Lionakis. Kontoyiannis. Lancet 2003

53
In brief, NF-κB can be understood to be a protein responsible for cytokine production and cell survival. Antiinflammatory actions of cortisol. Cortisol facilitates the production of the inhibitor of NFκB (I-κB), which binds to NFκB and prevents it from entering the nucleus and activating target genes. Activated glucocorticoid receptor (GR) also interferes with NFκB binding to its response elements in deoxyribonucleic acid, thus preventing the induction of phospholipase A2, cyclooxygenase 2 (COX2), and inducible nitric oxide synthase (iNOS). By blocking further production of proinflammatory cytokines such as tumor necrosis factor-α and interleukin-1, cortisol disrupts the positive feedback cycle involving these cytokines. NO, Nitric oxide
, which binds to NFκB and prevents it from entering the nucleus and activating target genes. Activated glucocorticoid receptor (GR) also interferes with NFκB binding to its response elements in deoxyribonucleic acid, thus preventing the induction of phospholipase A2, cyclooxygenase 2 (COX2), and inducible nitric oxide synthase (iNOS). By blocking further production of proinflammatory cytokines such as tumor necrosis factor-α and interleukin-1, cortisol disrupts the positive feedback cycle involving these cytokines. NO, Nitric oxide.")
Παρόμοιες παρουσιάσεις























 Ενότητα 5: Αναιμία Χρόνιας Νόσου Αναστάσιος Κριεμπάρδης Τμήμα Ιατρικών εργαστηρίων Ανοικτά Ακαδημαϊκά Μαθήματα στο ΤΕΙ Αθήνας Το περιεχόμενο.>")