Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
ΠΡΟΣΦΑΤΕΣ ΜΕΛΕΤΕΣ ΣΤΗΝ ΥΠΟΛΙΠΙΔΑΙΜΙΚΗ ΑΓΩΓΗ
Ευάγγελος Λυμπερόπουλος Λέκτορας Παθολογίας Ιατρικής Σχολής Παν/μίου Ιωαννίνων

2
ΕΠΙΔΡΑΣΗ ΤΟΥ EZETIMIBE ΣΤΗΝ ΑΘΗΡΟΣΚΛΗΡΩΣΗ

3
LRC-CCPT 19% p<0.05 JAMA 1984;251:351-64

4
Cholesterol lowering and cardiovascular events:
Program on surgical control of the Hyperlipidemias (POSCH) 35% p<0.001 Myocardial Infarction or death Reduction of LDL cholesterol POSCH trial; New Engl J Med 1990; 323:94
 35% p< Myocardial Infarction. or death. Reduction of. LDL cholesterol. POSCH trial; New Engl J Med 1990; 323:94.")
5
ENHANCE (Ezetimibe and Simvastatin in Hypercholesterolemia Enhances Atherosclerosis Regression): Σχεδιασμός της μελέτης Ασθενείς (n=720) Οικογενής ετερόζυγος υπερχοληστερολαιμία LDL-C = 319 mg/dl EZE 10 mg + SIMVA 80 mg (n=357) SIMVA 80 mg (n=363) METEOR is a randomised, double-blind, placebo-controlled, parallel-group, multicentre phase III study of rosuvastatin 40 mg in the prevention of atherosclerosis among asymptomatic patients assessed as being at low risk of CHD. Patients are asymptomatic for atherosclerosis and are considered at low risk of CHD according to conventional risk factors; 10-year CHD risk is assessed using the Framingham Risk Index. 984 patients were recruited from approximately 30 US and European centres and randomised to receive rosuvastatin or placebo in a 5:2 ratio. The 5:2 randomisation ratio in METEOR is due to the primary endpoint consisting of a two-stage test. See the following slide. Reference Crouse III JR et al. Measuring Effects on Intima Media Thickness: an Evaluation of Rosuvastatin in Subclinical Atherosclerosis – The Rationale and Methodology of the METEOR Study. Cardiovasc Drugs Ther 2004; 18: 231–238. Adapted from Cardiovasc Drugs Ther 2004; 18: 231–238, with permission from Springer. Επίσκεψη: Εβδομάδα: 1 –6 2 –4 3 –2 4 5 6 6 13 7 26 8 39 9 52 10 65 11 78 12 91 13 104 Run in / eligibility CIMT Lipids Safety Lipids Safety CIMT Safety CIMT Safety Lipids Safety CIMT Safety CIMT Lipids Safety CIMT=Πάχυνση Έσω και Μέσου Χιτώνα Καρωτίδας Kastelein JP, et al. Am Heart J 2005;149:234-9.
 Οικογενής ετερόζυγος υπερχοληστερολαιμία. LDL-C = 319 mg/dl. EZE 10 mg + SIMVA 80 mg (n=357) SIMVA 80 mg (n=363) METEOR is a randomised, double-blind, placebo-controlled, parallel-group, multicentre phase III study of rosuvastatin 40 mg in the prevention of atherosclerosis among asymptomatic patients assessed as being at low risk of CHD. Patients are asymptomatic for atherosclerosis and are considered at low risk of CHD according to conventional risk factors; 10-year CHD risk is assessed using the Framingham Risk Index. 984 patients were recruited from approximately 30 US and European centres and randomised to receive rosuvastatin or placebo in a 5:2 ratio. The 5:2 randomisation ratio in METEOR is due to the primary endpoint consisting of a two-stage test. See the following slide. Reference. Crouse III JR et al. Measuring Effects on Intima Media Thickness: an Evaluation of Rosuvastatin in Subclinical Atherosclerosis – The Rationale and Methodology of the METEOR Study. Cardiovasc Drugs Ther 2004; 18: 231–238. Adapted from Cardiovasc Drugs Ther 2004; 18: 231–238, with permission from Springer. Επίσκεψη: Εβδομάδα: 1. –6. 2. –4. 3. – Run in / eligibility. CIMT. Lipids. Safety. Lipids Safety. CIMT Safety. CIMT Safety. Lipids Safety. CIMT Safety. CIMT. Lipids. Safety. CIMT=Πάχυνση Έσω και Μέσου Χιτώνα Καρωτίδας. Kastelein JP, et al. Am Heart J 2005;149:")
6
Baseline characteristics
Simvastatin Monotherapy Simvastatin plus Ezetimibe All randomized patients n=363 n=357 P-value Age (yr) 45.710.0 46.19.0 0.69 Male sex no. (%) 179(49%) 191 (54%) 0.26 Body-mass index 26.74.4 27.44.6 0.047 History of diabetes 5(1%) 8 (2%) 0.38 Hypertension 51 (14%) 67 (19%) 0.09 Current smoking 104 (29%) 102 (29%) 0.98 History of MI 26 (7%) 14 (4%) 0.06 Prior use of statins 297 (82%) 286 (80%) 0.56 Systolic mm Hg 12415 12515 0.31 Diastolic mm Hg 7810 789 0.41
 45.7 Male sex no. (%) 179(49%) 191 (54%) Body-mass index. 26.7 History of diabetes. 5(1%) 8 (2%) Hypertension. 51 (14%) 67 (19%) Current smoking. 104 (29%) 102 (29%) History of MI. 26 (7%) 14 (4%) Prior use of statins. 297 (82%) 286 (80%) Systolic mm Hg. 124 Diastolic mm Hg. 7810. 78")
7
Percentage change from baseline -16.5 % incremental reduction
LDL-cholesterol Baseline (mg/dL) 24 months (mg/dL) Simva 318 ± 66 193 ± 60 Eze-Simva 319 ± 65 141 ± 53 10 -10 -20 -30 P<0.01 Percentage change from baseline -40 -16.5 % incremental reduction -50 -60 -70 6 12 18 24 Simva Eze-Simva Months ENHANCE Kastelein JP, et al. N Engl J Med 2008;358:
 24 months (mg/dL) Simva. 318 ± ± 60. Eze-Simva. 319 ± ± P<0.01. Percentage change from baseline % incremental reduction Simva. Eze-Simva. Months. ENHANCE. Kastelein JP, et al. N Engl J Med 2008;358:")
8
Other Lipids and Apolipoproteins
Percent Change From Baseline Simvastatin 80 EZE/simva 10/80 P value Total Cholesterol -31.9±0.8 -45.3±0.8 <0.01 LDL-cholesterol -39.1±0.9 -55.6±0.9 Triglycerides (median) -23.2 -29.8 HDL-cholesterol 7.8±0.9 10.2±1.0 0.05 Apo B -33.1±0.9 -46.7±0.9 Apo A1 6.9±0.8 6.3±0.8 0.56 ENHANCE
 HDL-cholesterol. 7.8± ± Apo B ± ±0.9. Apo A1. 6.9± ± ENHANCE.")
9
-26 % incremental reduction
Kastelein JP, et al. N Engl J Med 2008;358: hsCRP Baseline months (mg/L) (mg/L) Simva ( ) ( ) Eze-Simva ( ) ( ) Median percent change from Baseline p < 0.01 3 6 12 18 24 Months 10 -10 -20 -30 -40 -50 -60 -70 -80 -26 % incremental reduction Simva Eze-Simva ENHANCE 9
 (mg/L) Simva 1.7( ) 1.2( ) Eze-Simva 1.7( ) 0.9( ) Median percent change from Baseline. p < Months % incremental reduction. Simva. Eze-Simva. ENHANCE. 9.")
10
Mean cIMT during 24 months of therapy Longitudinal, repeated measures analysis
6 12 18 24 0.60 0.70 0.75 0.80 0.65 Months P=0.88 Mean IMT (mm) Simva Eze-Simva ENHANCE Kastelein JP, et al. N Engl J Med 2008;358:
 Simva. Eze-Simva. ENHANCE. Kastelein JP, et al. N Engl J Med 2008;358:")
11
ΕΡΜΗΝΕΙΑ ΤΩΝ ΑΠΟΤΕΛΕΣΜΑΤΩΝ ΤΗΣ ΜΕΛΕΤΗΣ ENHANCE
Αξιόπιστη μεθοδολογία; Πλειοτροπικές δράσεις του ezetimibe vs στατίνη σε υψηλές δόσεις; Πληθυσμός (ασθενείς με FH που ελάμβαναν ήδη θεραπεία με στατίνες);
;")
12
ENHANCE cIMT Methodology Carotid Intima-Media thickness (cIMT) measurements
Measurements were made at a predefined angle of insonation Only the far-walls of all segments were imaged Images were stored in DICOM for offline image analyses ENHANCE de Groot E, et al. Circulation. (2004) 109[Suppl III]:III-33-III-38.
 109[Suppl III]:III-33-III-38.")
13
ΕΡΜΗΝΕΙΑ ΤΩΝ ΑΠΟΤΕΛΕΣΜΑΤΩΝ ΤΗΣ ΜΕΛΕΤΗΣ ENHANCE
Αξιόπιστη μεθοδολογία; Πλειοτροπικές δράσεις του ezetimibe vs στατίνη; Πληθυσμός (ασθενείς με FH που ελάμβαναν ήδη θεραπεία με στατίνες);
;")
14
The Compound Ezetimibe no pleiotropic effects?
P= n.s. Chronic heart failure patients (NYHA III), n=10 per group LDL-c reduction similar in both groups. Simvastatin: 15.6 % Ezetimibe: 15.4% P<0.01 12 12 9 9 Flow dependent dilation (percent change of diameter) Flow dependent dilation (percent change of diameter) 6 6 3 3 Baseline 4 weeks Baseline 4 weeks Simvastatin 10 mg group Ezetimibe 10 mg group ENHANCE Landmesser et al, Circulation 2005; 111(18):
, n=10 per group. LDL-c reduction similar in both groups. Simvastatin: 15.6 % Ezetimibe: 15.4% P< Flow dependent dilation. (percent change of diameter) Flow dependent dilation. (percent change of diameter) Baseline 4 weeks. Baseline 4 weeks. Simvastatin 10 mg group. Ezetimibe 10 mg group. ENHANCE. Landmesser et al, Circulation 2005; 111(18):")
15
ΠΛΕΙΟΤΡΟΠΙΚΕΣ ΔΡΑΣΕΙΣ
ΤΟΥ EZETIMIBE Αντιφλεγμονώδης δράση ( hs CRP, Lp-PLA2) Αντιοξειδωτική δράση: Παράταση λανθάνοντος χρόνου για την οξείδωση της LDL από 144 min σε 195 min (p<0.001) Αντιαιμοπεταλιακή δράση: Μείωση της συσσώρευσης των αιμοπεταλίων από 83±15% σε 60±36% (p=0.04) Br J Clin Pharmacol 2008;65:637-45
 Αντιοξειδωτική δράση: Παράταση λανθάνοντος χρόνου για την οξείδωση της LDL από 144 min σε 195 min (p<0.001) Αντιαιμοπεταλιακή δράση: Μείωση της συσσώρευσης των αιμοπεταλίων από 83±15% σε 60±36% (p=0.04) Br J Clin Pharmacol 2008;65:")
16
Endothelial function (FMD)
High dose Statin vs. Low dose Statin + Ezetimibe on endothelial function: Study-design Randomisation of 39 patients with CAD and dysglycemia to 6 weeks: Simvastatin (80 mg/day) Simvastatin + Ezetimibe ( mg/day) Analysis of: Endothelial function (FMD) Settergren et al.; Eur Heart J. 2008; 29:
 Simvastatin + Ezetimibe ( mg/day) Analysis of: Endothelial function (FMD) Settergren et al.; Eur Heart J. 2008; 29:")
17
Serum LDL-cholesterol - change after 6 weeks -
51.6% 30.0 57% 60.0 P=n.s. Simvastatin (80 mg/d) n=20 Simvastatin +Ezetimibe ( mg/d) n=19 Settergren et al.; Eur Heart J. 2008; 29:
 n=20. Simvastatin +Ezetimibe. ( mg/d) n=19. Settergren et al.; Eur Heart J. 2008; 29:")
18
Endothelial function - flow-mediated dilation (FMD)
P= n.s. 1.5 Change in FMD (%) SIMVA (80 mg/d) n = 16 SIMVA + EZE ( mg/d) n = 18 Settergren et al.; Eur Heart J. 2008; 29:
 SIMVA. (80 mg/d) n = 16. SIMVA + EZE. ( mg/d) n = 18. Settergren et al.; Eur Heart J. 2008; 29:")
19
ΕΡΜΗΝΕΙΑ ΤΩΝ ΑΠΟΤΕΛΕΣΜΑΤΩΝ ΤΗΣ ΜΕΛΕΤΗΣ ENHANCE
Αξιόπιστη μεθοδολογία; Πλειοτροπικές δράσεις του ezetimibe vs στατίνη σε υψηλές δόσεις; Πληθυσμός (ασθενείς με FH που ελάμβαναν ήδη θεραπεία με στατίνες);
;")
20
Baseline cIMT in LIPID (pediatric), ASAP and ENHANCE
Normal value (40-49 years)= mm 0.4 0.8 1.2 1.6 2.0 ENHANCE ASAP Frequency Mean CIMT (mm) 2.4 LIPID (pediatric) Baseline mean cIMT (mm) LIPID (pediatric) 0.495±0.050 ASAP 0.920±0.200 ENHANCE 0.695±0.130 ENHANCE
= mm ENHANCE. ASAP. Frequency. Mean CIMT (mm) 2.4. LIPID (pediatric) Baseline mean cIMT. (mm) LIPID (pediatric) 0.495± ASAP ± ENHANCE ± ENHANCE.")
21
Επέκταση ASAP: Η Ατορβαστατίνη Σταμάτησε Μακροπρόθεσμα την Εξέλιξη της Καρωτιδικής Αθηροσκλήρυνσης
Μεταβολή στο μέσο ΙΜΤ καρωτίδας ASAP Επέκταση ASAP 0.8 0.9 1.0 Σε ασθενείς που λάμβαναν ατορβαστατίνη για ένα επιπρόσθετο χρονικό διάστημα 2 ετών κατά τη διάρκεια της επέκτασης της μελέτης, η εξέλιξη του μέσου IMT των σταμάτησε διεκόπη πλήρως (0,89 mm στα 2 έτη έναντι 0,90 mm στο τέλος της μελέτης, P=0,58). Ωστόσο, το μέσο IMT των καρωτίδων μειώθηκε σημαντικά σε ασθενείς που άλλαξαν από σιμβαστατίνη 40 mg σε ατορβαστατίνη 80 mg (0,95 mm στα 2 έτη έναντι των 0,92 mm στο τέλος της μελέτης, P=0,01).1 Το συνολικό ποσοστό ανεπιθύμητων ενεργειών ήταν συγκρίσιμο μεταξύ των ομάδων και δεν σημειώθηκαν σημαντικές διαφορές στις εργαστηριακές παραμέτρους.1 Οι van Wissen et al συμπέραναν ότι η βέλτιστη θεραπεία για ασθενείς με FH είναι η ατορβαστατίνη υψηλής δόσης, καθώς αυτή η θεραπεία επιτυγχάνει μείωση της αθηροσκλήρυνσης και είναι ασφαλής και καλά ανεκτή.1 Βιβλιογραφική Αναφορά: 1. van Wissen S, Smilde TJ, Trip MD, et al. Long-term safety and efficacy of high-dose atorvastatin treatment in patients with familial hypercholesterolemia. Am J Cardiol. 2005;95: IMT (mm) 1 2 3 4 Έτη Ατορβαστατίνη 80 mg Σιμβαστατίνη 40 mg van Wissen S et al. Am J Cardiol. 2005;95:
. Ωστόσο, το μέσο IMT των καρωτίδων μειώθηκε σημαντικά σε ασθενείς που άλλαξαν από σιμβαστατίνη 40 mg σε ατορβαστατίνη 80 mg (0,95 mm στα 2 έτη έναντι των 0,92 mm στο τέλος της μελέτης, P=0,01).1. Το συνολικό ποσοστό ανεπιθύμητων ενεργειών ήταν συγκρίσιμο μεταξύ των ομάδων και δεν σημειώθηκαν σημαντικές διαφορές στις εργαστηριακές παραμέτρους.1. Οι van Wissen et al συμπέραναν ότι η βέλτιστη θεραπεία για ασθενείς με FH είναι η ατορβαστατίνη υψηλής δόσης, καθώς αυτή η θεραπεία επιτυγχάνει μείωση της αθηροσκλήρυνσης και είναι ασφαλής και καλά ανεκτή.1. Βιβλιογραφική Αναφορά: 1. van Wissen S, Smilde TJ, Trip MD, et al. Long-term safety and efficacy of high-dose atorvastatin treatment in patients with familial hypercholesterolemia. Am J Cardiol. 2005;95: IMT (mm) Έτη. Ατορβαστατίνη 80 mg. Σιμβαστατίνη 40 mg. van Wissen S et al. Am J Cardiol. 2005;95:")
22
SANDS JACC 2008;52:

23
SANDS Reducing LDL-C to aggressive targets resulted in similar
regression of carotid IMT in patients who attained equivalent LDL-C reductions from a statin alone or statin plus ezetimibe. Common carotid artery IMT increased in those achieving standard targets. LDL-C fall: ezetimibe +statin = 31 mg/dl (n=69) statin only = 32 mg/dl (n=154) standard treatment = 1 mg/dl (n=204)
 statin only = 32 mg/dl (n=154) standard treatment = 1 mg/dl (n=204)")
24
SANDS Changes in HDL and TG were also similar between the
ezetimibe + statin and statin alone groups. BUT, what was the baseline carotid IMT? 0.819 and in the ezetimibe + statin and statin alone groups, respectively. Change in carotid IMT at 36 months: – (95% CI: – 0.05 to 0.003) and – (0.03 to 0.008) in the ezetimibe + statin and statin alone groups, respectively. JACC 2008;52:
 and – (0.03 to 0.008) in the ezetimibe. + statin and statin alone groups, respectively. JACC 2008;52:")
25
JACC 2008;52:

26
MK-0653A PN043 NOT APPROVED FOR USE
4/3/2017 7:34 PM Clinical Trials Slide Set 26

27
Patient Definition Men and Women Age 45 - 85 years Asymptomatic
Source: EZT 2005-W SS Ref 1, C1, Table 2 Men and Women Age years Asymptomatic Valvular AS: Aortic valve thickening on echocardiographic evaluation Doppler jet velocity ≥2.5 - ≤4.0 m/sec Normal LV systolic function The SEAS study is a multicenter, randomized, double-blind, placebo-controlled, 4-year (median duration) trial conducted in patients with asymptomatic and echocardiographically defined valvular AS (aortic valve thickening and Doppler-measured peak flow velocity across the valve of 2.5 m/s and 4.0 m/s).1 The goals of this study are to investigate whether aggressive cholesterol lowering in patients with moderate AS can slow the progression of AS and reduce the necessity for valve replacement and the incidence of CV events. The study will end after at least 464 patients have major CV events (MCEs).1 The primary objective is to evaluate the efficacy of ezetimibe/simvastatin therapy in reducing MCEs. These include CV death, aortic valve replacement surgery, CHF resulting from progression of AS, nonfatal MI, coronary artery bypass graft, percutaneous coronary intervention (PCI), hospitalization for unstable angina, and nonhemorrhagic stroke. The secondary objectives are to evaluate the effects of ezetimibe/simvastatin therapy on the risk of aortic valve events or ischemic CV events and time to progression of AS. The safety profile and tolerability of ezetimibe/simvastatin therapy will also be evaluated.1 Ref 1, Table 1, C1 Ref 1, C3, ¶1,3 Ref 1, Table 2 Reference Rossebø A, Pedersen T, Skjaerpe T, et al, for the SEAS Steering Committee. Design of the simvastatin and ezetimibe in aortic stenosis (SEAS) study. Presented at: XIII International Symposium on Atherosclerosis; September 28–October 2, 2003; Kyoto, Japan. Poster 3P-0870.
 trial conducted in patients with asymptomatic and echocardiographically defined valvular AS (aortic valve thickening and Doppler-measured peak flow velocity across the valve of 2.5 m/s and 4.0 m/s).1. The goals of this study are to investigate whether aggressive cholesterol lowering in patients with moderate AS can slow the progression of AS and reduce the necessity for valve replacement and the incidence of CV events. The study will end after at least 464 patients have major CV events (MCEs).1. The primary objective is to evaluate the efficacy of ezetimibe/simvastatin therapy in reducing MCEs. These include CV death, aortic valve replacement surgery, CHF resulting from progression of AS, nonfatal MI, coronary artery bypass graft, percutaneous coronary intervention (PCI), hospitalization for unstable angina, and nonhemorrhagic stroke. The secondary objectives are to evaluate the effects of ezetimibe/simvastatin therapy on the risk of aortic valve events or ischemic CV events and time to progression of AS. The safety profile and tolerability of ezetimibe/simvastatin therapy will also be evaluated.1. Ref 1, Table 1, C1. Ref 1, C3, ¶1,3. Ref 1, Table 2. Reference. Rossebø A, Pedersen T, Skjaerpe T, et al, for the SEAS Steering Committee. Design of the simvastatin and ezetimibe in aortic stenosis (SEAS) study. Presented at: XIII International Symposium on Atherosclerosis; September 28–October 2, 2003; Kyoto, Japan. Poster 3P")
28
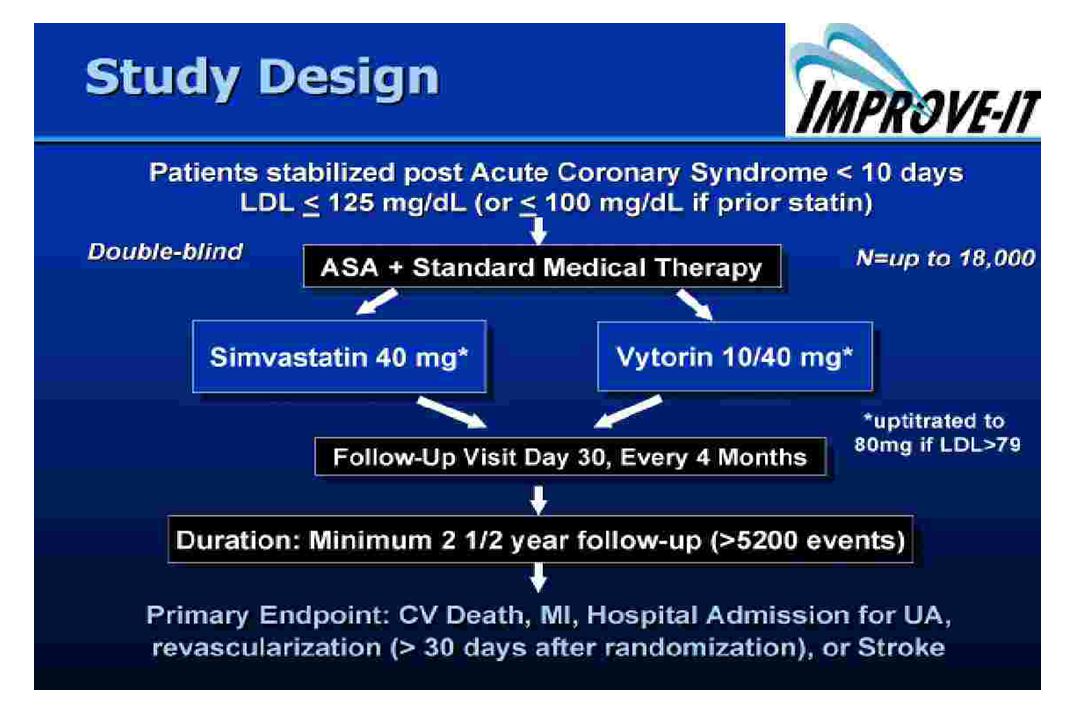
Study Design Randomized Double blind Placebo controlled Multicenter
MK-0653A PN NOT APPROVED FOR USE Study Design 4/3/2017 7:34 PM Source: EZT 2005-W SS Randomized Double blind Placebo controlled Multicenter 4 Weeks placebo/diet run-in Simvastatin 40 mg + ezetimibe 10 mg or placebo Median duration: 4.5 year (minimum follow-up 4 years) Rossebø AB, Pedersen TR, Allen C, Boman K, Chambers J, Egstrup K, Gerdts E, Gohlke-Bärwolf C, Holme I, Kesäniemi VA, Malbecq W, Nienaber C, Ray S, Skjaerpe T, Wachtell K, Willenheimer R. Design and baseline characteristics of the simvastatin and ezetimibe in aortic stenosis (SEAS) study. Am J Cardiol. 2007;99(7):970-3. Clinical Trials Slide Set 28
 Rossebø AB, Pedersen TR, Allen C, Boman K, Chambers J, Egstrup K, Gerdts E, Gohlke-Bärwolf C, Holme I, Kesäniemi VA, Malbecq W, Nienaber C, Ray S, Skjaerpe T, Wachtell K, Willenheimer R. Design and baseline characteristics of the simvastatin and ezetimibe in aortic stenosis (SEAS) study. Am J Cardiol. 2007;99(7): Clinical Trials Slide Set. 28.")
29
Baseline Characteristics
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM Baseline Characteristics Placebo Simva + Ezetimibe n= 929 n= 944 Age (years) 67.4 67.7 Women (%) 38.8 38.5 SBP (mm Hg) 144 146 DBP (mm Hg) 82 Smoker (%) 18 20 Ex-smoker (%) 37 35 Never smoker (%) 45 BMI (kg/m2) 26.8 26.9 Rossebø AB, Pedersen TR, Allen C, Boman K, Chambers J, Egstrup K, Gerdts E, Gohlke-Bärwolf C, Holme I, Kesäniemi VA, Malbecq W, Nienaber C, Ray S, Skjaerpe T, Wachtell K, Willenheimer R. Design and baseline characteristics of the simvastatin and ezetimibe in aortic stenosis (SEAS) study. Am J Cardiol. 2007;99(7):970-3. Clinical Trials Slide Set 29
 Women (%) SBP (mm Hg) DBP (mm Hg) 82. Smoker (%) Ex-smoker (%) Never smoker (%) 45. BMI (kg/m2) Rossebø AB, Pedersen TR, Allen C, Boman K, Chambers J, Egstrup K, Gerdts E, Gohlke-Bärwolf C, Holme I, Kesäniemi VA, Malbecq W, Nienaber C, Ray S, Skjaerpe T, Wachtell K, Willenheimer R. Design and baseline characteristics of the simvastatin and ezetimibe in aortic stenosis (SEAS) study. Am J Cardiol. 2007;99(7): Clinical Trials Slide Set. 29.")
30
LDL-Cholesterol 61% 150 Placebo 125 100 75 50 EZ/Simva 10/40 mg 25
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM LDL-Cholesterol Intention to Treat Population 150 61% Placebo 125 100 Rossebo et al NEJM draft manuscript 75 Mean (mg/dL) ±SE 50 EZ/Simva 10/40 mg 25 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5 Year Clinical Trials Slide Set 30
 ±SE. 50. EZ/Simva 10/40 mg Year. Clinical Trials Slide Set. 30.")
31
Percentage of Patients With First Event
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM Primary Endpoint MCE Intention to Treat Population 1 2 3 4 5 Years in Study 10 20 30 40 50 Percentage of Patients With First Event EZ/Simva 10/40 mg Placebo No. at Risk Hazard ratio: 0.96, p=0.591 906 817 713 618 53 884 791 696 586 56 Rossebo et al NEJM draft manuscript Fig 3 Clinical Trials Slide Set 31

32
2nd EP: Aortic Valve Events
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM 2nd EP: Aortic Valve Events Years in Study Placebo EZ/Simva 10/40 mg No. at Risk 914 836 732 635 55 895 814 725 611 58 Intention to Treat Population 1 2 3 4 5 10 20 30 40 50 Hazard ratio: 0.97, p=0.732 Percentage of Patients With First Event Rossebo et al NEJM draft manuscript Fig 3 Clinical Trials Slide Set 32

33
Aortic Valve Replacement
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM Aortic Valve Replacement 50 Intention to Treat Population 1 2 3 4 5 Years in Study 10 20 30 40 EZ/Simva 10/40 mg No. at risk Hazard ratio: 1.00, p=0.968 915 837 734 640 55 Percentage of Patients With First Event Placebo From Terje Pedersen Placebo 896 816 728 618 61 Clinical Trials Slide Set 33

34
Peak Aortic - Jet Velocity
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM Peak Aortic - Jet Velocity Intention to Treat Population EZ/Simva 10/40 mg Placebo Year 1 Year 2 Last Follow-up Time 0.00 0.15 0.30 0.45 0.60 0.75 Change from Baseline (m/sec) Mean (±SE) Rossebo et al NEJM draft manuscript Clinical Trials Slide Set 34
 Mean (±SE) Rossebo et al NEJM draft manuscript. Clinical Trials Slide Set. 34.")
35
2nd EP: Ischemic CV Events
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM 2nd EP: Ischemic CV Events Intention to Treat Population Years in Study Hazard ratio: 0.78, p=0.024 EZ/Simva 10/40 mg Placebo 1 2 3 4 5 10 20 30 22% Percentage of Patients With First Event ERM or Rossebo et al NEJM draft manuscript No. at risk EZ/Simva 10/40 mg 917 867 823 769 76 Placebo 898 838 788 729 76 Clinical Trials Slide Set 35

36
Coronary Artery Bypass Grafting (CABG)
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM Coronary Artery Bypass Grafting (CABG) 30 Years in Study Placebo EZ/Simva 10/40 mg No. at risk 925 909 887 862 848 819 797 761 80 Percentage of Patients With First Event Intention to Treat Population Hazard ratio: 0.68, p=0.015 1 2 3 4 5 10 20 From Terje Pedersen Clinical Trials Slide Set 36
 30. Years in Study. Placebo. EZ/Simva 10/40 mg. No. at risk Percentage of Patients With First Event. Intention to Treat Population. Hazard ratio: 0.68, p= From Terje Pedersen. Clinical Trials Slide Set. 36.")
37
Major CV Events - Components
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM Major CV Events - Components ITT Population # of Events Placebo EZ/Simva 355 56 278 23 26 100 17 8 29 333 47 267 25 69* 5 33 Endpoints Hazard Ratio (95% CI) Major CV Events CV Death AVR ERM and treatment data from Rossebo et al NEJM draft manuscript Table 2 CHF Nonfatal MI CABG PCI Hospitalized UAP Non hem. Stroke *p=0.02 vs Placebo 0.1 1.0 10.0 Favors EZ/Simva 10/40 mg Favors Placebo Clinical Trials Slide Set 37
 Major CV Events. CV Death. AVR. ERM and treatment data from Rossebo et al NEJM draft manuscript Table 2. CHF. Nonfatal MI. CABG. PCI. Hospitalized UAP. Non hem. Stroke. *p=0.02 vs Placebo Favors EZ/Simva 10/40 mg. Favors Placebo. Clinical Trials Slide Set. 37.")
38
Clinical Adverse Events (AE)
All Patients as Treated Population Placebo EZ/ Simva N=929 N=943* n p= Any serious AE (SAE) 463 468 Drug discon. due to SAE 79 77 Musculoskeletal AE 181 165 0.28 Myopathy / Rhabdo New cancer 65 102 0.01 Recurrent, same site 5 3 Cancer, total 70 105 N=944 for these D/c due to non drug related AE D/c due to drug related AE D/c due to non drug related SAE D/c due to drug related SAE ERM or Rossebo et al NEJM draft manuscript
 Drug discon. due to SAE Musculoskeletal AE Myopathy / Rhabdo. New cancer Recurrent, same site Cancer, total N=944 for these. D/c due to non drug related AE. D/c due to drug related AE. D/c due to non drug related SAE. D/c due to drug related SAE. ERM or Rossebo et al NEJM draft manuscript.")
39
Cumulative Percentage
Fatal Cancer Placebo EZ/Simva 10/40 mg No. at risk 930 916 912 890 884 865 855 835 89 94 P=0.05 Unadjusted P=0.06 With Log-rank continuity correction 1 2 3 4 5 Years in Study 10 15 20 Hazard ratio: 1.67 Cumulative Percentage Intention to Treat Population n=23 (2.5%) n=39 (4.1%)
 n=39 (4.1%)")
40
Incident Cancer All Patients as Treated Population Site
Placebo (N=929) EZ/simva (N=943) n Lip, oral pharynx, Oesophagus 1 Stomach 5 Large bowel / intestine 8 9 Pancreas 4 Liver gallbladder, bile ducts 3 2 Lung 10 7 Other respiratory Skin (any) 18 Breast Prostate 13 21 Kidney Bladder Genital Hemathological Other/unspecified 12 Rossebo et al NEJM draft manuscript All differences are non-significant
 EZ/simva (N=943) n. Lip, oral pharynx, Oesophagus. 1. Stomach. 5. Large bowel / intestine Pancreas. 4. Liver gallbladder, bile ducts Lung Other respiratory. Skin (any) 18. Breast. Prostate Kidney. Bladder. Genital. Hemathological. Other/unspecified. 12. Rossebo et al NEJM draft manuscript. All differences are non-significant.")
41
Cumulative Percentage
MK-0653A PN NOT APPROVED FOR USE 4/3/2017 7:34 PM All Cause Mortality Intention to Treat Population Placebo EZ/Simva 10/40 mg No. risk 930 916 912 890 884 865 855 835 89 94 Years in Study Hazard ratio: 1.04, p=0.799 1 2 3 4 5 10 20 30 Cumulative Percentage Rossebo et al NEJM draft manuscript Clinical Trials Slide Set 41

42
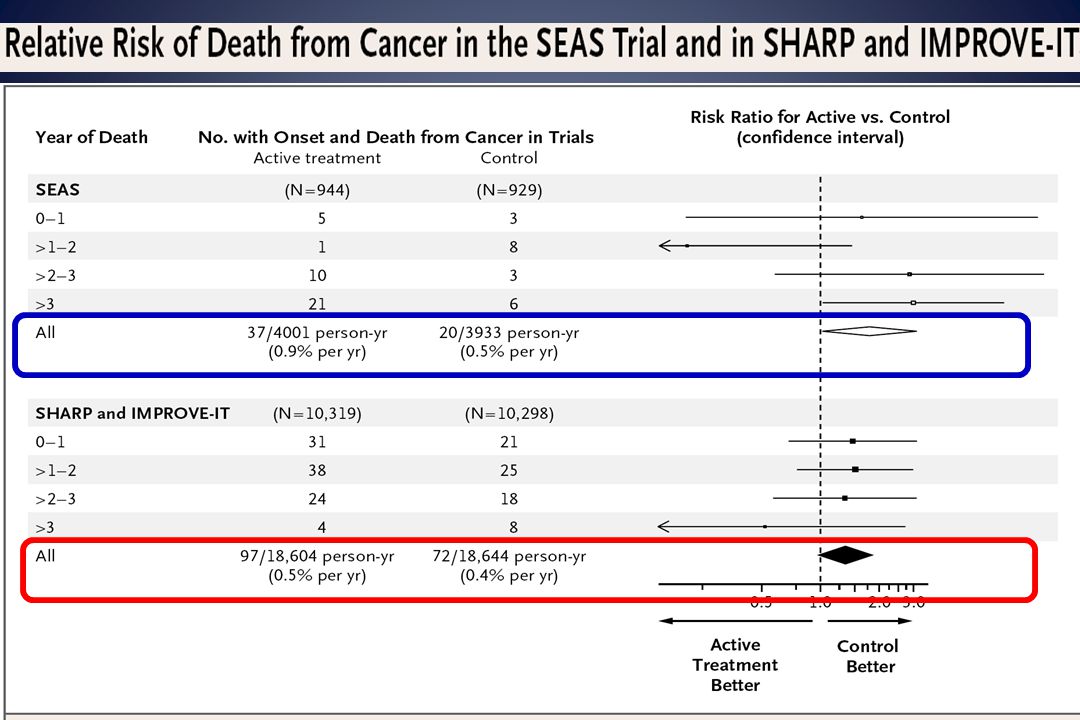
Peto R et al, N Engl J Med 2008;359

44
Comments: Carcinogens would be expected to increase cancers as time progress. The opposite was found in SEAS. The increase in cancer is across the whole range. Some cancers were less in the combination therapy. The much larger SHARP and IMPROVE-IT do not show any increase in cancer.

45
FDA ‘These findings in the SEAS trial plus the interim data from ongoing trials should not prompt patients to stop taking Vytorin or any other cholesterol lowering drug’ 21 AUG 2008

47
CRP predicts risk of MI and stroke in apparently healthy men
3.5 2.0 * *** 3.0 1.5 2.5 Relative risk of MI Relative risk of ischaemic stroke 2.0 1.0 In the epidemiological Physicians’ Health Study in 543 healthy middle-aged men, the relative risk of future MI increased significantly (p<0.001) with increasing levels of CRP. Increasing levels of CRP were also associated with significantly increased risk (p=0.02) of future thromboembolic stroke. Reference Ridker PM et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997; 336: 973–979. Abbreviations CRP=C-reactive protein; MI=myocardial infarction 1.5 1.0 0.5 0.5 1 2 3 4 1 2 3 4 Quartile of CRP Quartile of CRP CRP=C-reactive protein; MI=myocardial infarction *p=0.02 versus quartile 1; ***p<0.001 versus quartile 1 Ridker PM et al. N Engl J Med 1997; 336: 973–979
 with increasing levels of CRP. Increasing levels of CRP were also associated with significantly increased risk (p=0.02) of future thromboembolic stroke. Reference. Ridker PM et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997; 336: 973–979. Abbreviations. CRP=C-reactive protein; MI=myocardial infarction Quartile of CRP. Quartile of CRP. CRP=C-reactive protein; MI=myocardial infarction *p=0.02 versus quartile 1; ***p<0.001 versus quartile 1. Ridker PM et al. N Engl J Med 1997; 336: 973–979.")
48
AFCAPS/TexCAPS AFCAPS/TexCAPS Low LDL Subgroups Low LDL, Low hsCRP
Low LDL, High hsCRP Low LDL, Low hsCRP Low LDL, High hsCRP [A] [B] 0.5 1.0 2.0 0.5 1.0 2.0 RR Statin Effective Statin Not Effective Statin Effective Statin Not Effective However, while intriguing and of potential public health importance, the observation in AFCAPS/TexCAPS that statin therapy might be effective among those with elevated hsCRP but low cholesterol was made on a post hoc basis. Thus, a large-scale randomized trial of statin therapy was needed to directly test this hypotheses. Ridker et al, New Engl J Med 2001;344:

49
JUPITER Trial Design JUPITER Multi-National Randomized Double Blind Placebo Controlled Trial of Rosuvastatin in the Prevention of Cardiovascular Events Among Individuals With Low LDL and Elevated hsCRP MI Stroke Unstable Angina CVD Death CABG/PTCA Rosuvastatin 20 mg (N=8901) No Prior CVD or DM Men >50, Women >60 LDL <130 mg/dL hsCRP >2 mg/L Placebo (N=8901) 4-week run-in Argentina, Belgium, Brazil, Bulgaria, Canada, Chile, Colombia, Costa Rica, Denmark, El Salvador, Estonia, Germany, Israel, Mexico, Netherlands, Norway, Panama, Poland, Romania, Russia, South Africa, Switzerland, United Kingdom, Uruguay, United States, Venezuela Ridker et al, Circulation 2003;108:
 No Prior CVD or DM. Men >50, Women >60. LDL <130 mg/dL. hsCRP >2 mg/L. Placebo (N=8901) 4-week run-in. Argentina, Belgium, Brazil, Bulgaria, Canada, Chile, Colombia, Costa Rica, Denmark, El Salvador, Estonia, Germany, Israel, Mexico, Netherlands, Norway, Panama, Poland, Romania, Russia, South Africa, Switzerland, United Kingdom, Uruguay, United States, Venezuela. Ridker et al, Circulation 2003;108:")
50
JUPITER Inclusion and Exclusion Criteria, Study Flow Men > 50 years
Ridker et al NEJM 2008 89,890 Screened 89,863 Screened Reason for Exclusion (%) LDL-C > 130 mg/dL hsCRP < 2.0 mg/L Withdrew Consent Diabetes Hypothyroid <1 Liver Disease <1 TG > 500 mg/dL <1 Age out of range <1 Current Use of HRT <1 Cancer <1 Poor Compliance/Other Reason for Exclusion (%) LDL > 130 mg/dL hsCRP < 2.0 mg/L Withdrew Consent Diabetes Hypothyroid <1 Liver Disease <1 TG > 500 mg/dL <1 Age out of range <1 Current Use of HRT <1 Cancer <1 Poor Compliance/Other 3 Men > 50 years Women > 60 years No CVD, No DM LDL < 130 mg/dL hsCRP > 2 mg/L 4 week Placebo Run-In 17,802 Randomized 17,802 Randomized 8,901 Assigned to Rosuvastatin 20 mg 8,901 Assigned to Rosuvastatin 20 mg 8,901 Assigned to Placebo 8,901 Assigned to Placebo 8,600 Completed Study 120 Lost to follow-up 8,857 Completed Study 44 Lost to follow-up 8,864 Completed Study 37 Lost to follow-up 8,600 Completed Study 120 Lost to follow-up 8,901 Included in Efficacy and Safety Analyses 8,901 Included in Efficacy and Safety Analyses 8,901 Included in Efficacy and Safety Analyses 8,901 Included in Efficacy and Safety Analyses
 LDL-C > 130 mg/dL 53. hsCRP < 2.0 mg/L 37. Withdrew Consent 4. Diabetes 1. Hypothyroid <1. Liver Disease <1. TG > 500 mg/dL <1. Age out of range <1. Current Use of HRT <1. Cancer <1. Poor Compliance/Other 3. Reason for Exclusion (%) LDL > 130 mg/dL 52. hsCRP < 2.0 mg/L 36. Withdrew Consent 5. Diabetes 1. Hypothyroid <1. Liver Disease <1. TG > 500 mg/dL <1. Age out of range <1. Current Use of HRT <1. Cancer <1. Poor Compliance/Other 3. Men > 50 years. Women > 60 years. No CVD, No DM. LDL < 130 mg/dL. hsCRP > 2 mg/L. 4 week. Placebo. Run-In. 17,802 Randomized. 17,802 Randomized. 8,901 Assigned to. Rosuvastatin 20 mg. 8,901 Assigned to. Rosuvastatin 20 mg. 8,901 Assigned to. Placebo. 8,901 Assigned to. Placebo. 8,600 Completed Study. 120 Lost to follow-up. 8,857 Completed Study. 44 Lost to follow-up. 8,864 Completed Study. 37 Lost to follow-up. 8,600 Completed Study. 120 Lost to follow-up. 8,901 Included in Efficacy. and Safety Analyses. 8,901 Included in Efficacy. and Safety Analyses. 8,901 Included in Efficacy. and Safety Analyses. 8,901 Included in Efficacy. and Safety Analyses.")
51
Baseline Clinical Characteristics
JUPITER Baseline Clinical Characteristics Ridker et al NEJM 2008 Rosuvastatin Placebo (N = 8901) (n = 8901) Age, years (IQR) ( ) ( ) Female, N (%) 3,426 (38.5) 3,375 (37.9) Ethnicity, N (%) Caucasian ,358 (71.4) 6,325 (71.1) Black 1,100 (12.4) 1,124 (12.6) Hispanic 1,121 (12.6) 1,140 (12.8) Blood pressure, mm (IQR) Systolic ( ) 134 ( ) Diastolic (75-87) 80 (75-87) Smoker, N (%) 1,400 (15.7) 1,420 (16.0) Family History, N (%) 997 (11.2) 1,048 (11.8) Metabolic Syndrome, N (%) 3,652 (41.0) 3,723 (41.8) Aspirin Use, N (%) 1,481 (16.6) 1,477 (16.6) All values are median (interquartile range) or N (%)
 (n = 8901) Age, years (IQR) 66.0 ( ) 66.0 ( ) Female, N (%) 3,426 (38.5) 3,375 (37.9) Ethnicity, N (%) Caucasian 6,358 (71.4) 6,325 (71.1) Black 1,100 (12.4) 1,124 (12.6) Hispanic 1,121 (12.6) 1,140 (12.8) Blood pressure, mm (IQR) Systolic 134 ( ) 134 ( ) Diastolic 80 (75-87) 80 (75-87) Smoker, N (%) 1,400 (15.7) 1,420 (16.0) Family History, N (%) 997 (11.2) 1,048 (11.8) Metabolic Syndrome, N (%) 3,652 (41.0) 3,723 (41.8) Aspirin Use, N (%) 1,481 (16.6) 1,477 (16.6) All values are median (interquartile range) or N (%)")
52
Baseline Blood Levels (median, interquartile range)
JUPITER Baseline Blood Levels (median, interquartile range) Ridker et al NEJM 2008 Rosuvastatin Placebo (N = 8901) (n = 8901) hsCRP, mg/L ( ) ( ) LDL, mg/dL ( ) 108 ( ) HDL, mg/dL (40 – 60) 49 (40 – 60) Triglycerides, mg/L 118 ( ) ( ) Total Cholesterol, mg/dL 186 ( ) 185 ( ) Glucose, mg/dL 94 (87 – 102) 94 (88 – 102) HbA1c, % (5.4 – 5.9) (5.5 – 5.9) All values are median (interquartile range) [ Mean LDL = 104 mg/dL ]
 Ridker et al NEJM Rosuvastatin Placebo. (N = 8901) (n = 8901) hsCRP, mg/L 4.2 ( ) 4.3 ( ) LDL, mg/dL 108 ( ) 108 ( ) HDL, mg/dL 49 (40 – 60) 49 (40 – 60) Triglycerides, mg/L 118 ( ) 118 ( ) Total Cholesterol, mg/dL 186 ( ) 185 ( ) Glucose, mg/dL 94 (87 – 102) 94 (88 – 102) HbA1c, % 5.7 (5.4 – 5.9) 5.7 (5.5 – 5.9) All values are median (interquartile range). [ Mean LDL = 104 mg/dL ]")
53
JUPITER LDL (mg/dL) HDL (mg/dL) hsCRP (mg/L) TG (mg/dL) Months Months
Effects of rosuvastatin 20 mg on LDL, HDL, TG, and hsCRP Ridker et al NEJM 2008 LDL (mg/dL) HDL (mg/dL) LDL decrease 50 percent at 12 months HDL increase 4 percent at 12 months hsCRP (mg/L) TG (mg/dL) hsCRP decrease 37 percent at 12 months TG decrease 17 percent at 12 months 12 24 36 48 Months Months
 HDL (mg/dL) LDL decrease 50 percent at 12 months. HDL increase 4 percent at 12 months. hsCRP (mg/L) TG (mg/dL) hsCRP decrease 37 percent at 12 months. TG decrease 17 percent at 12 months Months. Months.")
54
- 44 % JUPITER HR 0.56, 95% CI 0.46-0.69 Placebo 251 / 8901
Primary Trial Endpoint : MI, Stroke, UA/Revascularization, CV Death Ridker et al NEJM 2008 HR 0.56, 95% CI P < Placebo 251 / 8901 0.08 Number Needed to Treat (NNT5) = 25 - 44 % 0.06 Cumulative Incidence 0.04 Rosuvastatin 142 / 8901 0.02 0.00 1 2 3 4 Follow-up (years) Number at Risk Rosuvastatin 8,901 8,631 8,412 6,540 3,893 1,958 1,353 983 544 157 Placebo 8,901 8,621 8,353 6,508 3,872 1,963 1,333 955 534 174
 = % Cumulative Incidence Rosuvastatin 142 / Follow-up (years) Number at Risk. Rosuvastatin. 8,901. 8,631. 8,412. 6,540. 3,893. 1,958. 1, Placebo. 8,901. 8,621. 8,353. 6,508. 3,872. 1,963. 1,")
55
Individual Components of the Primary Endpoint
JUPITER Individual Components of the Primary Endpoint Ridker et al NEJM 2008 Endpoint Rosuvastatin Placebo HR 95%CI P Primary Endpoint* < Non-fatal MI < Any MI <0.0002 Non-fatal Stroke Any Stroke Revascularization or Unstable Angina < MI, Stroke, CV Death < *Nonfatal MI, nonfatal stroke, revascularization, unstable angina, CV death

56
Among men and women age 50 or over:
JUPITER Implications for Primary Prevention A simple evidence-based approach to statin therapy for primary prevention. Among men and women age 50 or over: If LDL-C >Target (130 mg/dL), treat If diabetic, treat If hsCRP >2 mg/L, treat??
, treat. If diabetic, treat. If hsCRP >2 mg/L, treat")
Παρόμοιες παρουσιάσεις