Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Σταύρος Σπηλιόπουλος Επ. Καθηγητής ΕΚΠΑ Επεμβατικός Ακτινολόγος
Ενδαγγειακές τεχνικές για την αντιμετώπισης της απόφραξης της άνω κοίλης φλέβας Σταύρος Σπηλιόπουλος Επ. Καθηγητής ΕΚΠΑ Επεμβατικός Ακτινολόγος

2
Ανατομία ΑΚΦ Υποκλείδιος φλέβα Ανώνυμες φλέβες Ανω κοίλη φλέβα
Η ΑΚΦ σχηματίζεται από την εκβολή των 2 ανωνύμων φλεβών όπσθεν της 1ης δεξιάς στερνοπλευρικής αρθρώσεως. Φερόμενη προς τα κάτω, όπισθεν του 1ου και 2ου μεσοχονδρίου διαστήματος εκβάλλει στο άνω τοίχωμα του δεξιού κόλπου ισουψώς με τον 3ο δεξιό πλευρικό χόνδρο. Υποκλείδιος φλέβα Ανώνυμες φλέβες Ανω κοίλη φλέβα

3
ΑΝΑΤΟΜΙΑ Έσω σφαγίτιδα φλέβα ----αρθροίζει το αίμα της κεφαλής και εν μέρει του τραχήλου Υποκλείδιος φλέβα--αρθροίζει το αίμα του άνω άκρου, άνω θώρακα, και επιπολής φλεβικού δικτύου κεφαλής τραχήλου.

4
Ανατομία ΑΚΦ και φλεβών μεσοθωρακίου
Άζυγος φλέβα ΑΚΦ Μεσοπλεύριες Φλέβες Μαστικές φλέβες Ανώνυμες φλέβες ΑΚΦ Στο επίπεδο του 2ου δεξιού πλευρικού χόνδρου διατιτραίνει το περικάρδιο αφού πρώτα δέχεται την εκβολή της αζύγου φλέβας οπισθίως άνωθεν του δεξιού βρόγχου Η άζυγος φλέβα αρθροίζει το αίμα από τον θώρακα και τη σπονδυλική στήλη.

5
Η ΑΚΦ στερείται βαλβίδων
Μήκος: εκ. Διάμετρος χιλ. Φλεβική πίεση: -5 έως 5 mmHg

6
Σύνδρομο άνω κοίλης φλέβας (ΑΚΦ)
Σημαντική στένωση/απόφραξη της ΑΚΦ Σύνδρομο ΑΚΦ: Aποτελεί επείγουσα και απειλητική για τη ζωή κατάσταση κατά την οποία η σύμπιεση της ΑΚΦ από διάφορα αίτια επιφέρει σημαντικά κλινικά συμπτώματα όπως δύσπνοια, κυάνωση, οίδημα προσώπου/άνω κορμού και αίσθημα πνιγμού. Χαρακτηριστική η εμφάνιση παράπλευρου φλεβικού δικτύου στο θώρακα.

7
Σύνδρομο άνω κοίλης φλέβας (ΑΚΦ)
Αφορά σε 15,000 ασθενείς ετησίως στις ΗΠΑ. Τα συμπτώματα αναπτύσονται εντός 2 εβδομάδων στο 1/3 των ασθενών και σε μεγαλύτερο χρονικό διάστημα στους υπόοιπους.

8
Αιτιολογία συνδρόμου ΑΚΦ
Κακοήθειες Καρκίνος πνεύμονος 72% Λέμφωμα 12% Μεταστατικοί όγκοι 9% Θύμωμα Μεσοθηλίωμα Λειομυοσάρκωμα και αγγειοσάρκωμα Νεοπλαστικοί θρόμβοι Αναπλαστικό Ca θυρεοειδούς Ν Eng J Med: ;18

9
Καλόηθες Σύνδρομο ΑΚΦ (10%)
Καλόηθες Σύνδρομο ΑΚΦ (10%) Λεμφαδενοπάθειες Σαρκοείδωση Σύνδρομο Behçet’s Ινωδοποιός μεσοθωρακίτιδα (ιδιοπαθής ή μετακτινική) Νόσος Castelman’s Μεταδοτικές ασθένειες– Αορτικά ανευρύσματα Φυματίωση Ιστοπλάσμωση Καταδυόμενη βρογχοκήλη Εχινοκοκκίαση Περικαρδιακές, βρογχογενείς κύστεις Σύφιλη Ασπεργίλωση Βλαστομυκητίαση Ιατρογενείς Φιλαρίαση Απινιδωτές και βηματοδότες Νοκαρδίωση Κεντρικοί φλεβικοί καθετήρες Θρόμβωση (μη νεοπλαστικής αιτιολογίας) Μετεγχειρητικές στενώσεις
 Λεμφαδενοπάθειες. Σαρκοείδωση. Σύνδρομο Behçet’s. Ινωδοποιός μεσοθωρακίτιδα (ιδιοπαθής ή μετακτινική) Νόσος Castelman’s. Μεταδοτικές ασθένειες– Αορτικά ανευρύσματα. Φυματίωση. Ιστοπλάσμωση. Καταδυόμενη βρογχοκήλη. Εχινοκοκκίαση. Περικαρδιακές, βρογχογενείς κύστεις. Σύφιλη. Ασπεργίλωση. Βλαστομυκητίαση. Ιατρογενείς. Φιλαρίαση. Απινιδωτές και βηματοδότες. Νοκαρδίωση. Κεντρικοί φλεβικοί καθετήρες. Θρόμβωση (μη νεοπλαστικής αιτιολογίας) Μετεγχειρητικές στενώσεις.")
10
Μόνιμοι κεντρικοί φλεβικοί καθετήρες
Μόνιμοι κεντρικοί φλεβικοί καθετήρες 40% των ασθενών παρουσιάζει στένωση/απόφραξη κεντρικής φλέβας

11
Απόφραξη ΑΚΦ Η απόφραξη της άνω κοίλης φλέβας είναι σχετικά σπάνια επιπλοκή παθήσεων που αφορούν το μεσοθωράκιο. Τα κυριότερα αίτια είναι: 1. Όγκοι του μεσοθωρωκίου ή καρκίνος του πνεύμονα που επεκτείνεται σ' αυτό 2. Χρόνια μεσοθωρακίτιδα ιδιοπαθής ή δευτεροπαθής σε φυματίωση, ιστοπλάσμωση ή άλλες λοιμώξεις. 3. Θρομβοφλεβίτιδα της άνω κοίλης φλέβας συνήθως σαν επιπλοκή καθετηριασμού των μεγάλων αγγείων. 4. Ανεύρυσμα της αορτής

12
ΣΥΝΔΡΟΜΟ ΑΝΩ ΚΟΙΛΗΣ ΦΛΕΒΑΣ (ΑΚΦ)
Παθοφυσιολογία Διήθηση / εξωτερική συμπίεση από βλάβες: Δεξιού πνεύμονα Λεμφαδένες Λοιπές μεσοθωρακικές δομές In situ θρόμβωση Αύξηση φλεβικών πιέσεων στα άνω άκρα Διάταση παράπλευρου φλεβικού δικτύου Διάμεσο οίδημα-στένωση ανωτέρων αεραγωγών Εγκεφαλικό οίδημα => ισχαιμία => εγκολεασμός => Θάνατος Οξεία ελάττωση καρδιακής παροχής

13
ΣΥΝΔΡΟΜΟ ΑΝΩ ΚΟΙΛΗΣ ΦΛΕΒΑΣ (ΑΚΦ)
Παθοφυσιολογία Στο επίπεδο εισόδου της ΑΚΦ στον Δε κόλπο Άνωθεν της συμβολής αζύγου-ΑΚΦ Πιο έντονα συμπτώματα Χαρακτηριστικά συμβατά με απόφραξη σε άπω θέση σε σχέση με την εκβολή της άνω κοίλης Διατεταμένα παράπλευρα αγγεία προσθίου-οπισθίου κοιλιακού τοιχώματος => ΚΚΦ => καρδιά Διάταση φλεβών τραχήλου-άνω άκρων Οίδημα τραχήλου, προσώπου, άνω άκρων Οιδηματώδης στοματικός βλεννογόνος Οφιοειδώς διατεταμένα παράπλευρα αγγεία ανώτερου θώρακα-ράχης

14
Αύξηση πιέσεων της ΑΚΦ, μείωση της φλεβικής επιστροφής
Σημαντική στένωση >60% ΑΚΦ ενεργοποίηση της παράπλευρη κυκλοφορίας Sy WM, Lao RS. Collateral pathways in superior vena cava obstruction as seen on gamma images. Br J Radiol 1982; 55: Ο χρόνος ανάπτυξης της απόφραξης καθορίζει την κλινική εικόνα

15
Επί οξείας αποφράξεως: Μη αναπτυγμένο παράπλευρο δίκτυο= έντονη συμπτωματολογία
Αργά εξελισσόμενη νόσος= παράπλευρη κυκλοφορία και σταδιακή επιδείνωση

16
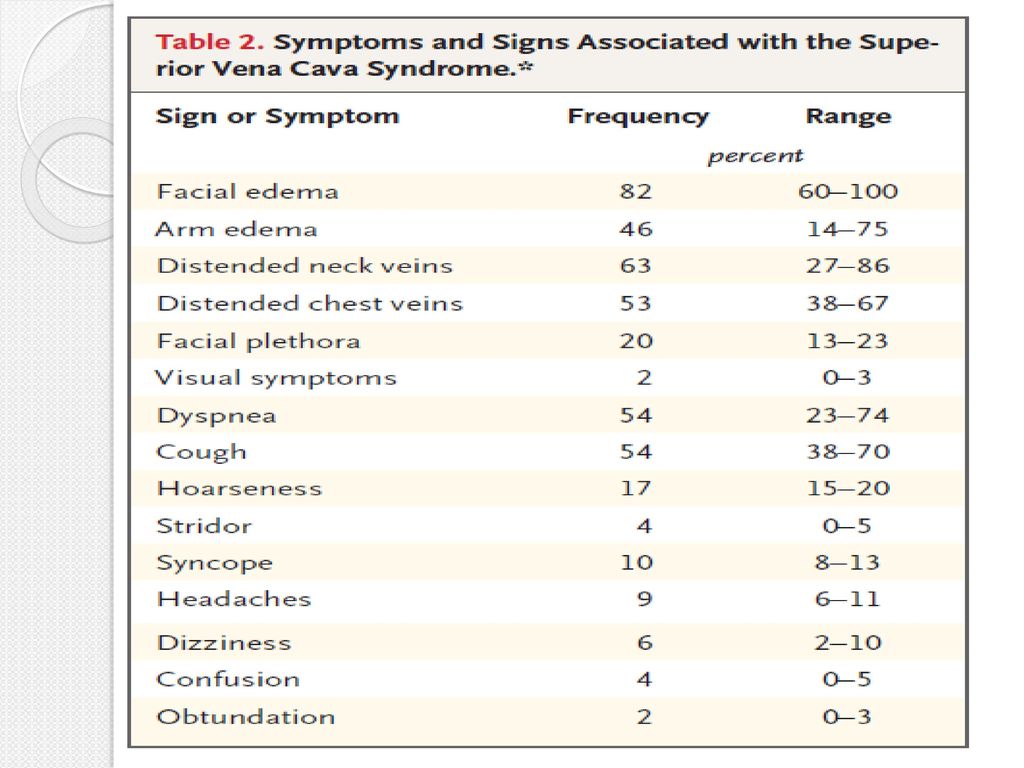
Κλινική εικόνα οσώπου ~ 80% Δύσπνοια ~ 63% Βήχας ~ 55%
οσώπου ~ 80% Δύσπνοια ~ 63% Βήχας ~ 55% Κεφαλαλγία ~ 20% Δυσφαγία ~ 12% Συγκοπή ~ 7% Οίδημα άνω άκρων ~ 3% Ορθόπνοια ~ 2% Θόλωση ~ 2% Ληθαργικότητα ~ 1% Συριγμός ~ 1% ΣΥΜΠΤΩΜΑΤΑ Συμφόρηση προσώπου Διάταση φλεβών τραχήλου, θώρακα, κοιλιακού τοιχώματος Οίδημα άνω άκρων, κυάνωση ΣΗΜΕΙΑ

17
Κλινική εικόνα Βαθμός βαρύτητας Κατηγορία Συχνότητα (%) Ορισμός
Ασυμπτωματικό 10 Ακτινολογική εικόνα χωρίς συμπτώματα 1 Ήπιο 25 Οίδημα κεφαλής ή τραχήλου, διάταση φλεβών, κυάνωση 2 Μέτριο 50 Οίδημα κεφαλής ή τραχήλου με λειτουργική διαταραχή: Ήπια δυσφαγία, βήχας Ήπιος ή μέτριος περιορισμός κινητικότητας κεφαλής, σιαγόνας, βλεφάρων Οπτικές διαταραχές λόγω οιδήματος οφθαλμών 3 Σοβαρό Μέτριο ή ήπιο εγκεφαλικό οίδημα (κεφαλαλγία, ζάλη) Ήπιο/ μέτριο οίδημα λάρυγγα Επηρεασμένες καρδιακές εφεδρείες (συγκοπή μετά από κάμψη) 4 Απειλητικό για τη ζωή 5 Σημαντικό εγκεφαλικό οίδημα (σύγχυση, διαταραχή συνείδησης) Σημαντικό οίδημα λάρυγγα (συριγμός) Σημαντική αιμοδυναμική επιβάρυνση (συγκοπή, υπόταση, νεφρική ανεπάρκεια) Θανατηφόρο <1 Θάνατος
 Ήπιο/ μέτριο οίδημα λάρυγγα. Επηρεασμένες καρδιακές εφεδρείες (συγκοπή μετά από κάμψη) 4. Απειλητικό για τη ζωή. 5. Σημαντικό εγκεφαλικό οίδημα (σύγχυση, διαταραχή συνείδησης) Σημαντικό οίδημα λάρυγγα (συριγμός) Σημαντική αιμοδυναμική επιβάρυνση (συγκοπή, υπόταση, νεφρική ανεπάρκεια) Θανατηφόρο. <1. Θάνατος.")
18
Αντιμετώπιση ΣΤΟΧΟΙ Ανακούφιση συμπτωμάτων
Θεραπεία υποκείμενου νοσήματος ΚΑΘΟΡΙΣΤΙΚΟΙ ΠΑΡΑΓΟΝΤΕΣ Τύπος κακοήθειας Έκταση νόσου Συνολική πρόγνωση Ιστολογία Προηγηθείσα ΧΜΘ

19
Αντιμετώπιση Straka et al. SpringerPlus (2016) 5:229
 5:229")
20
Ακτινοθεραπεία (ΑΚΘ) Σε SCLC ΧΜΘ και/ή ΑΚΘ ανακουφίζουν τα συμπτώματα του συνδρόμου ΑΚΦ σε ποσοστό ≈77%. ≈17% παρουσιάζουν υποτροπή. Σε NSCLC: 60% ≈19% παρουσιάζουν υποτροπή.

21
ΑΚΘ/ΧΜΘ Αποτελεσματική σε περίπου 90% των περιπτώσεων.
20% υποτροπή ακόμα και σε περιπτώσεις όπου χρησιμοποιήθηκε η μέγιστη επιτρεπτή δόση Σχετικές αντνδείξεις ΑΚΘ: Προηγηθείσα ΑΚΘ Ακτινο-ανθεκτικοί τύποι κακοήθειας π.χ. σάρκωμα Σκληρόδερμα Σε grade 4 η άμεση ΑΚΘ δεν ενδείκνυται ως θεραπεία 1ης γραμμής αν υπάρχει η δυνατότητα τοποθέτησης στεντ, καθώς το τελευταίο παρέχει ταχύτερη ανακούφιση από τα συμπτώματα. Nicholson AA, Ettles DF, Arnold A, Greenstone M, Dyet JF (1997) Treatment of malignant superior vena cava obstruction: metal stents or radiation therapy. J Vasc Interv Radiol 8:781–788
 Treatment of malignant superior vena cava obstruction: metal stents or radiation therapy. J Vasc Interv Radiol 8:781–788.")
22
Χημειοθεραπεία (ΧΜΘ) Λέμφωμα, όγκοι εκ γεννητικών κυττάρων : Ιδιαίτερα χημειοευαίσθητοι. ΧΜΘ ανακουφίζει τα συμπτώματα σε ποσοστό 80% σε λέμφωμα ΝΗ και 77% σε SCLC. Απόκριση: 7-15 ημέρες (όπως και η ακτινοΘεραπεία).
.")
23
Ενδαγγειακή αντιμετώπιση (Stenting)
Άμεση ανακούφιση: ώρες. Ενδείκνυται σε: Ασθενείς χωρίς ιστολογική διάγνωση Προηγηθείσα ΑΚΘ ΧΜΘ- και ΑΚΘ-ανθεκτικούς όγκους. Καλοήθειες Θρομβόλυση: επικουρικά επί παρουσίας θρόμβου Η χορήγηση θρομβόλυσης αυξάνει τη περιεπεμβατική θνητότητα Αντιθρομβωτική αγωγή

24
Σύνδρομο ΑΚΦ κακοήθους αιτιολογίας
Το όφελος της ακτινοθεραπείας μπορεί να είναι βραχυπρόθεσμο με αποτέλεσμα τη υποτροπή των συμπτωμάτων πριν ο ασθενής καταλήξει λόγω της νόσου. Επί έντονης συμπτωματολογίας ταχύτερη ανακούφιση μπορεί να επιτευχθεί με τη διαδερμική τοποθέτηση ενδαγγειακού στεντ και εν συνεχεία ακτινοθεραπεία για την αντιμετώπιση της υποκείμενης νόσου. Η διαδερμική τοποθέτηση στεντ είναι αποτελεσματική και σε περιπτώσεις ασθενών που δεν ανταποκρίθηκαν στην ακτινοθεραπεία.

25
Σύγκριση ΑΚΘ, ΧΜΘ και Στεντ
Δεν υπάρχουν τυχαιοποιημένες μελέτες Straka et al. SpringerPlus (2016) 5:229
 5:229.")
26
Ενδείξεις τοποθέτησης μεταλλικής ενδοπρόθεσης
Οξύ σύνδρομο ΑΚΦ κακοήθους αιτιολογίας που δεν ανταποκρίνεται στη ακτινοθεραπεία Οξύ σύνδρομο ΑΚΦ λόγω θρόμβωσης καλοήθους αιτιολογίας. Χρόνια καλοήθης απόφραξη με συμπτώματα συνδρόμου ΑΚΦ Δεν απαιτείται ιστολογική διάγνωση

27
ΑΚΤΙΝΟΒΟΛΗΣΗ ΜΕΣΟΘΩΡΑΚΙΟΥ (+ STENT)
Ενδείξεις: Βαρύτητα συμπτωμάτων Grade 4 Βαρύτητα συμπτωμάτων Grade 3 σε: Μέτρια χημειο-, ακτινοευαίσθητους όγκους (π.χ. NSCLC) Κακή λειτουργική κατάσταση (performance status) Mεσοθηλίωμα Βαρύτητα συμπτωμάτων με Grade 2-4 που εμμένουν ή υποτροπιάζουν παρά την ΧΜΘ και/ή την ακτινοβόληση Συνδυασμός με ακτινοβόληση ΑΚΤΙΝΟΒΟΛΗΣΗ ΜΕΣΟΘΩΡΑΚΙΟΥ (+ STENT) Απόλυτες ενδείξεις: Σοβαρή απόφραξη ανώτερων αεραγωγών => Συριγμός Εγκεφαλικό οίδημα => Κώμα Προέχει η ιστολογική διάγνωση
 Κακή λειτουργική κατάσταση (performance status) Mεσοθηλίωμα. Βαρύτητα συμπτωμάτων με Grade 2-4 που εμμένουν ή υποτροπιάζουν παρά την ΧΜΘ και/ή την ακτινοβόληση. Συνδυασμός με ακτινοβόληση. ΑΚΤΙΝΟΒΟΛΗΣΗ ΜΕΣΟΘΩΡΑΚΙΟΥ (+ STENT) Απόλυτες ενδείξεις: Σοβαρή απόφραξη ανώτερων αεραγωγών => Συριγμός. Εγκεφαλικό οίδημα => Κώμα. Προέχει η ιστολογική διάγνωση.")
28
Προ-επεμβατική Απεικόνιση
CT Θώρακος με σκιαγραφικό Εκτίμηση της ΑΚΦ και ΚΚΦ (στένωση απόφραξη, παρουσία θρόμβου, προσβασιμότητα) Εκτίμηση landing zone Μετρήσεις διαστάσεων
 Εκτίμηση landing zone. Μετρήσεις διαστάσεων.")
29
Προετοιμασία ασθενούς
Γεν αίματος Νεφρική λειτουργία PT, PTT, INR Δυνατότητα του ασθενούς να ξαπλώσει (αρκετά μαξιλάρια και Ο2) για τουλάχιστον 30’ Αναισθησιολογική κάλυψη
 για τουλάχιστον 30’ Αναισθησιολογική κάλυψη.")
30
Τεχνική Υπό τοπική αναισθησία
Ενδαγγειακοί καθετήρες και σύρμάτινοι οδηγοί. Έως και 10Fr θηκάρι Υδρόφυλο σύρμα για τη προσέλαση της βλάβης Σκληρό Amplatz-type σύρμα για την τοποθέτηση του στεντ.

31
Τεχνική Επί αμφιβολίας: Αρχική φλεβογραφία από τη βασιλική ή βραχιόνιο φλέβα. Παρακέντηση της κοινής μηριαίας ή έσω σφαγίτιδας ή βασιλικής ή βραχιόνιας φλέβας Ταυτόχρονη παρακέντηση κοινής μηριαίας και βασιλική/βραχιόνιας φλέβας σε περίπτωση αποτυχίας προσπέλασης

32
Τεχνική Υπερηχογραφική καθοδήγηση Micropuncture set

33
ΣΥΝΔΡΟΜΟ ΑΝΩ ΚΟΙΛΗΣ ΦΛΕΒΑΣ (ΑΚΦ)
Αρχική φλεβογραφία

36
High pressure 8 mm

37
Καλοήθους αιτιολογίας σύνδρομο ΑΚΦ
Στεντ: μη ικανοποιητική πρωτογενής βατότητα. Αssisted patency: 33-56% στο έτος

44
16x80 venous direct SelfX stent
10x60mm PTA

46
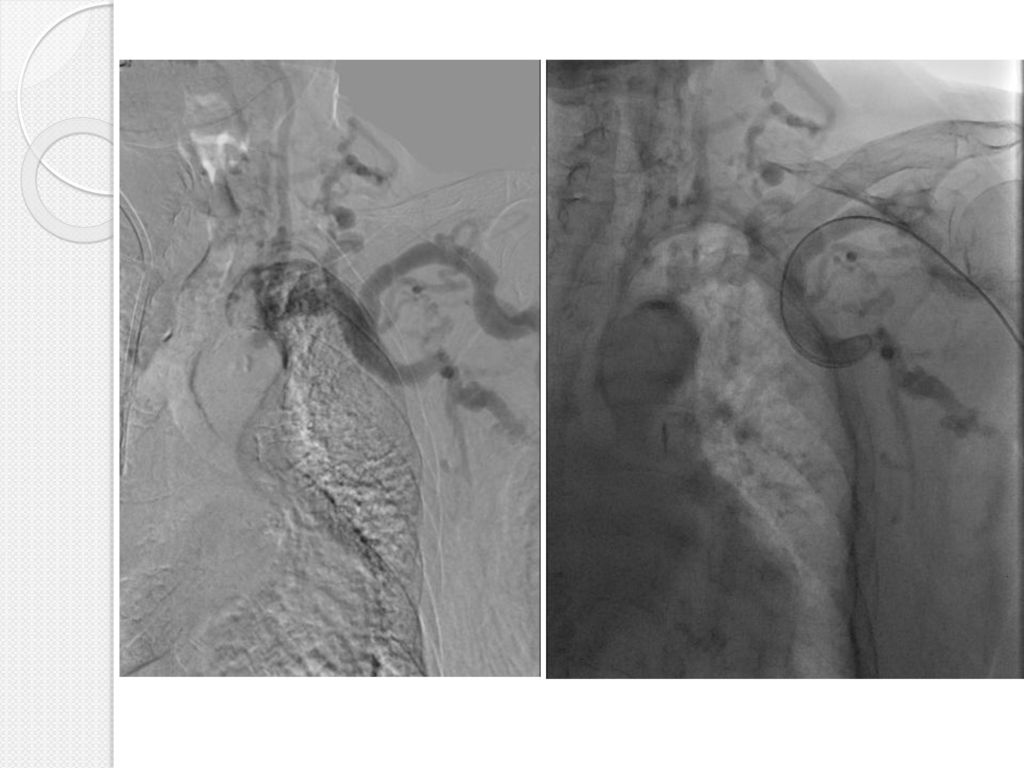
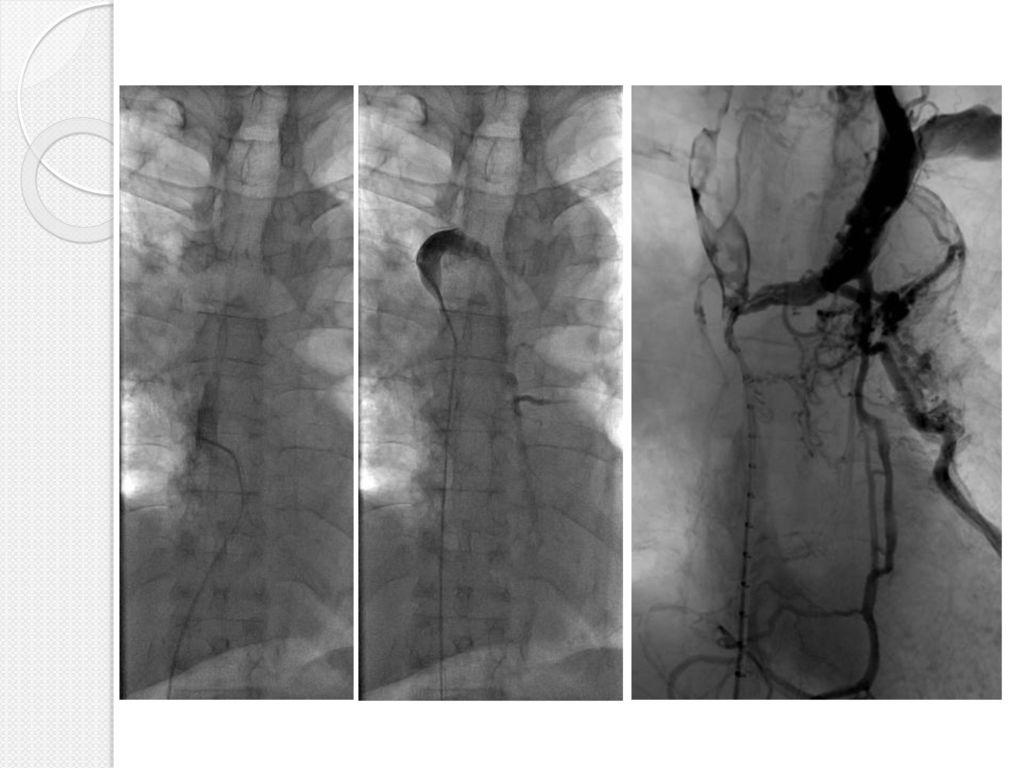
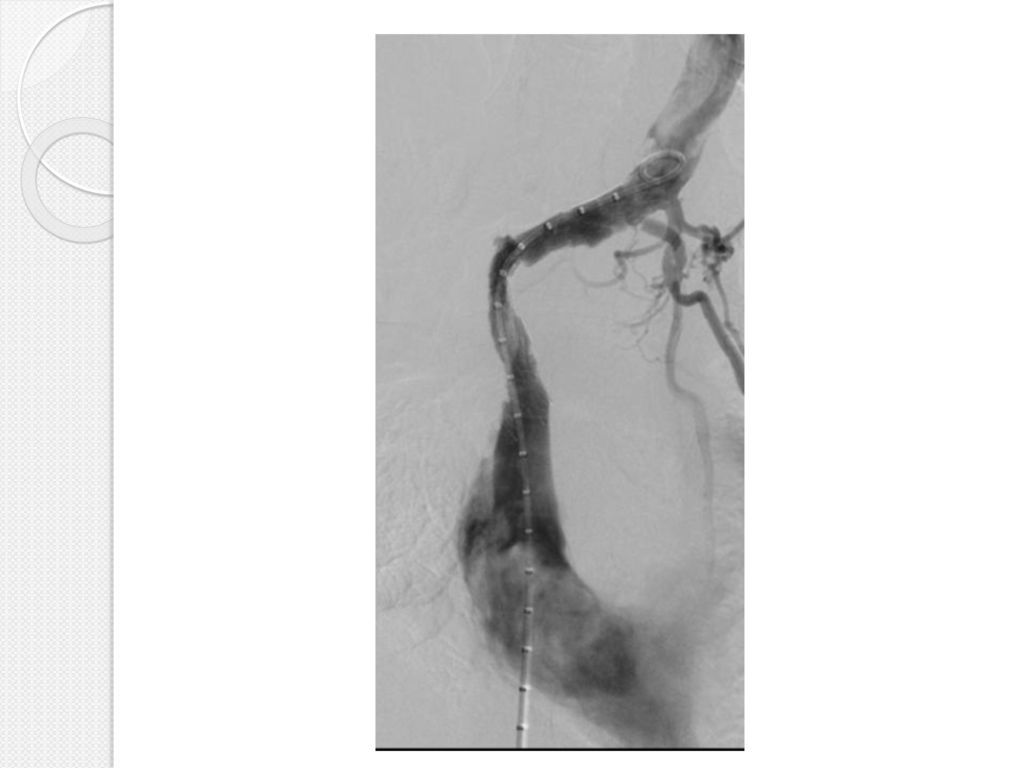
Καλοήθης απόφραξη από βηματοδότη-Θρόμβος
Θρομβόλυση Στεντ και μεταδιαστολή 14μμ

47
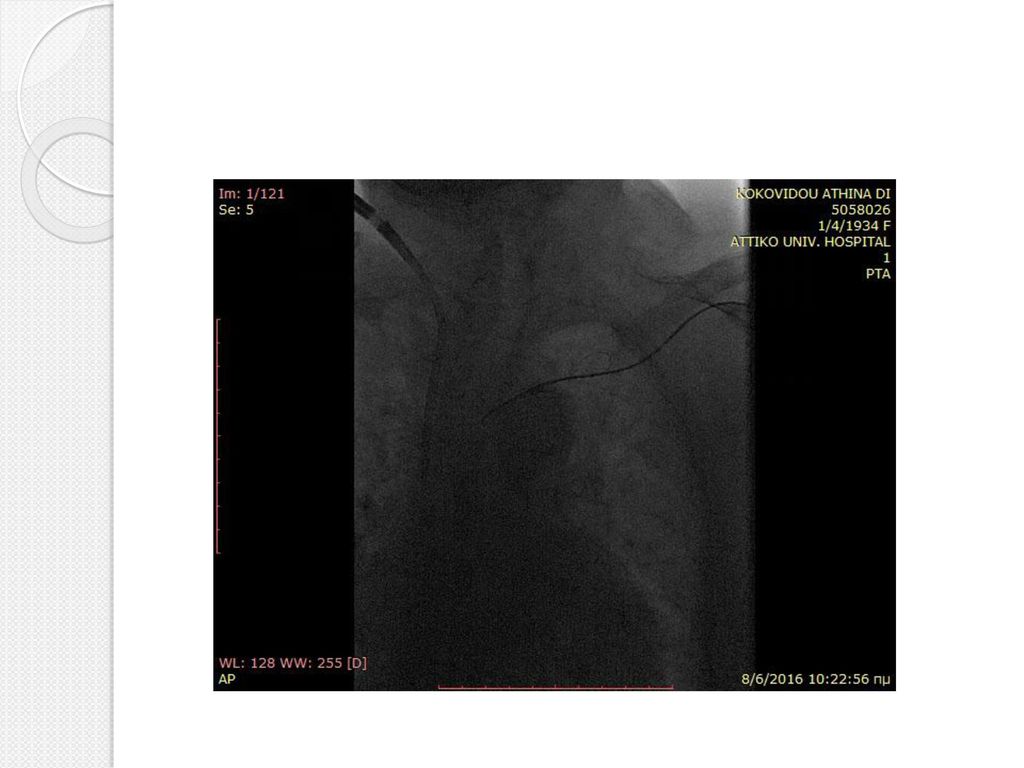
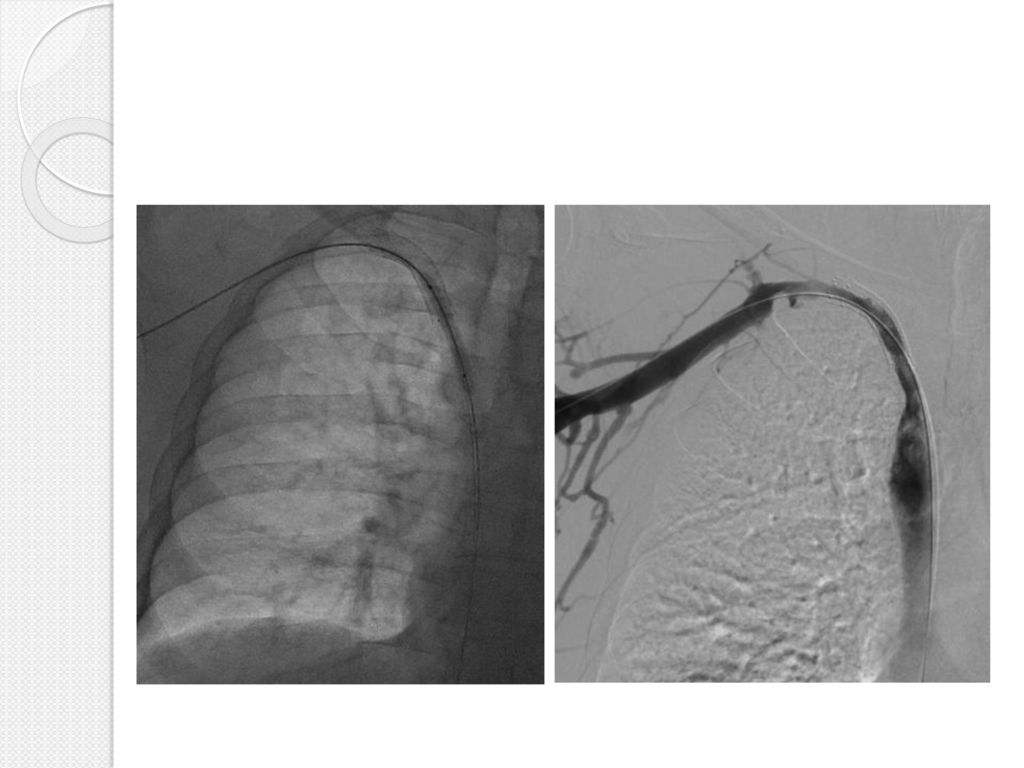
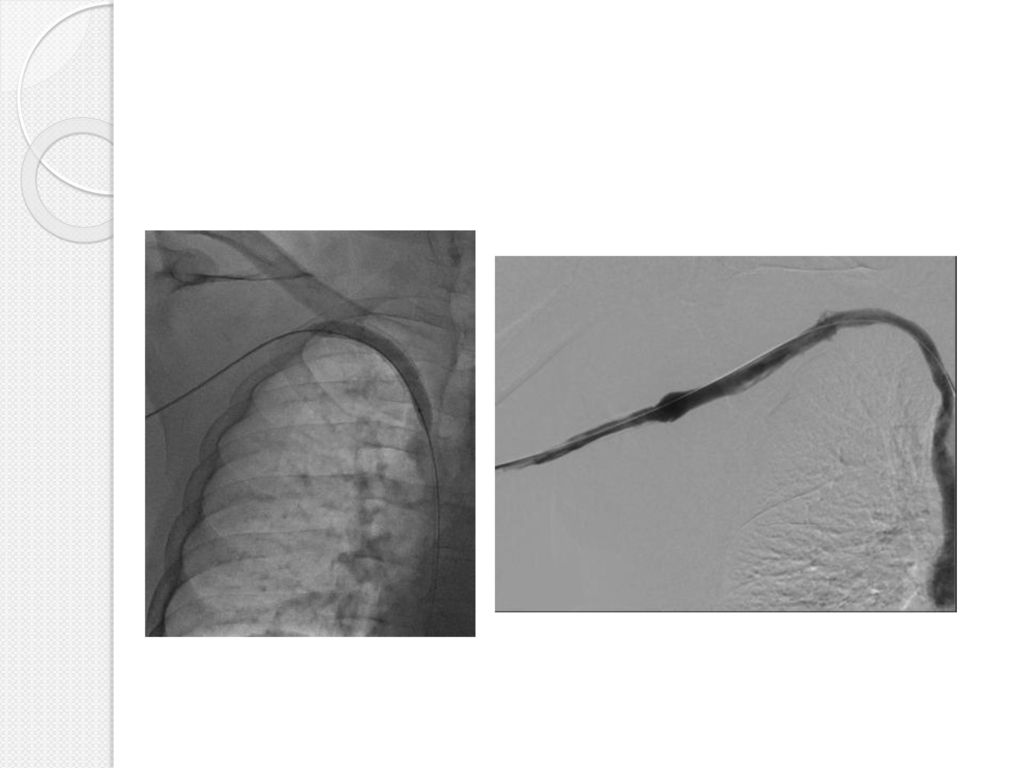
Απόφραξη μετά από τοποθέτηση Μόνιμου Κεντρικού Φλεβικού Καθετήρα

48
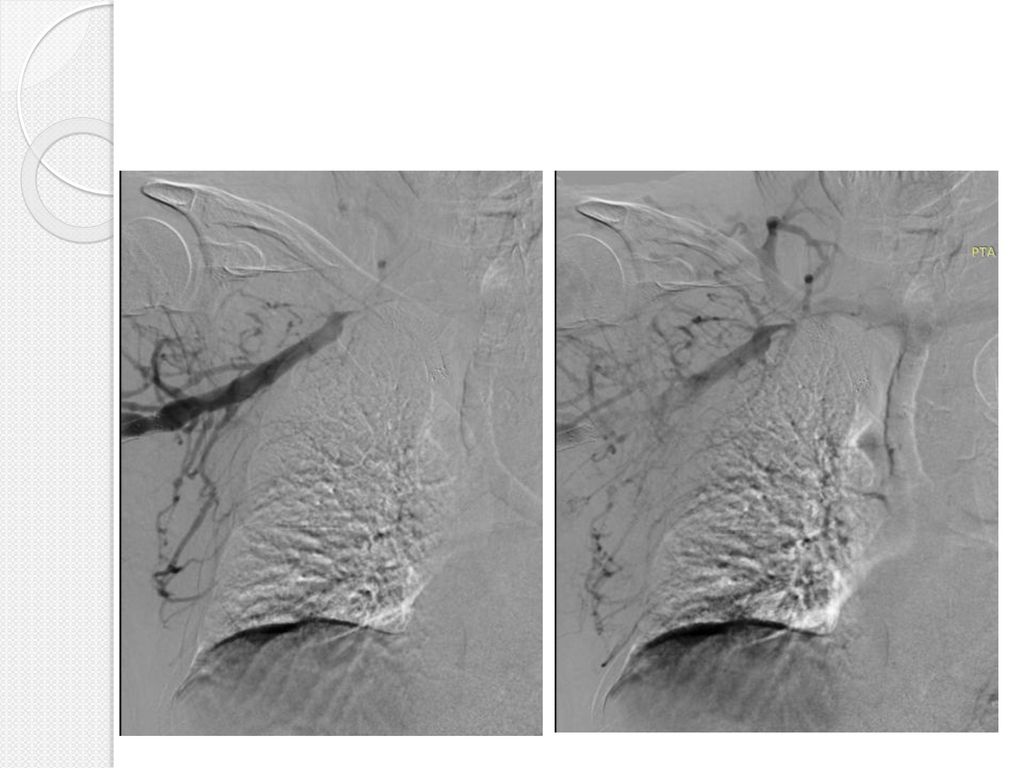
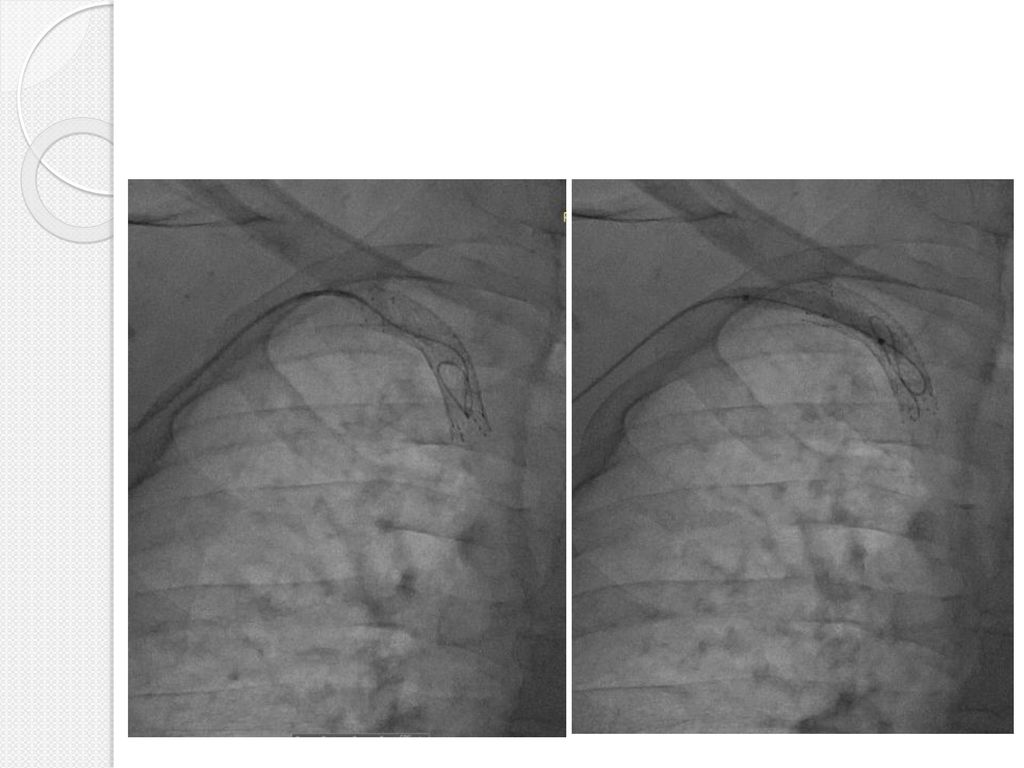
Επιπλοκή αγγειοπλαστικής

49
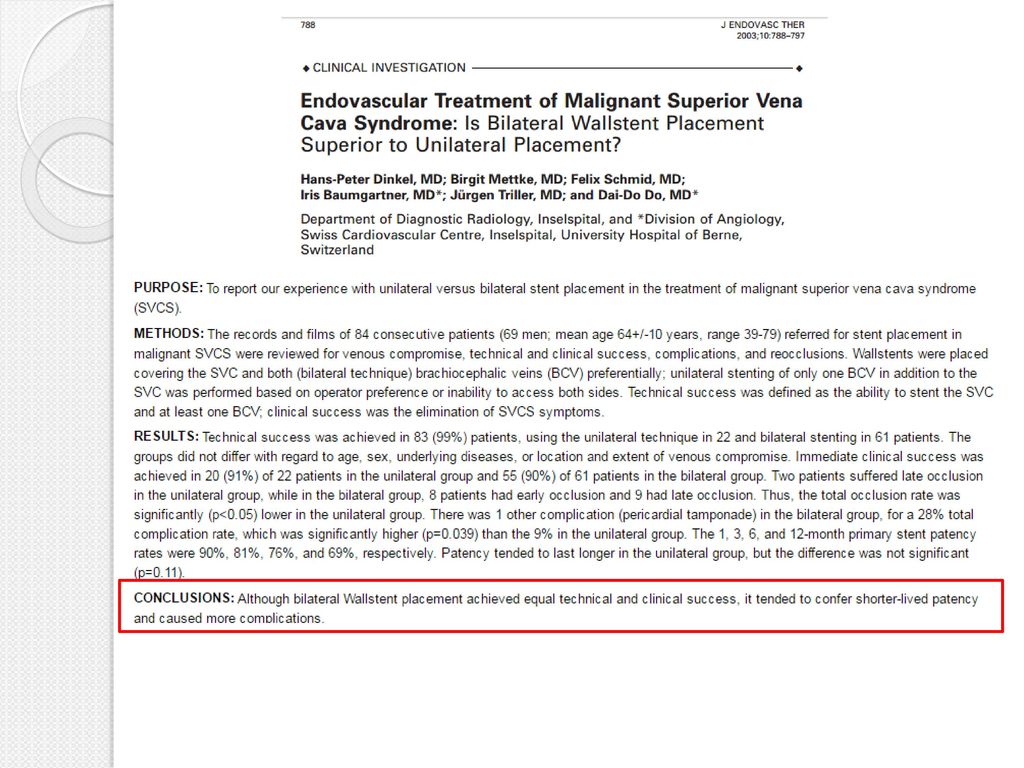
Αμφοτερόπλευρο stenting

51
Αποτελέσματα Τεχνική επιτυχία %, με 97–99 % άμεση ανακούφιση από τα συμπτώματα (Maleux et al. 2013; Gwon et al. 2013). Πρωτογενής βατότητα 64–95 %, Δευτερογενής βατότητας 93–100 %, Υποτροπή 0–40 % Επιπλοκές 0–25 % Θνητότητα 3–4 % Uberoi R (2006) Quality assurance guidelines for superior vena cava stenting in malignant disease. Cardiovasc Intervent Radiol 29:319–322
 Quality assurance guidelines for superior vena cava stenting in. malignant disease. Cardiovasc Intervent Radiol 29:319–322.")
52
Επιπλοκές Πρώιμες Επιμόλυνση Πνευμονική εμβολή Μετανάστευση του στεντ
Αιμάτωμα στην περιοχή παρακέντησης Αιμορραγία Ρήξη ΑΚΦ

53
Όψιμες επιπλοκές: Αιμορραγία (1 – 14%) Θάνατος(1 -2%) λόγω αντιπηκτικής αγωγής Απόφραξη του στεντ: Θρόμβωση ή διήθηση καρκινικού ιστού (tumor ingrowth).
.")
54
Μετεπεμβατική αγωγή Συνιστάται βραχυπρόθεσμη αντιπηκτική/αντιαιμοπεταλιακή αγωγή Μακροπρόθεσμα? Επανεπέμβαση: stent/θρομβόλυση

55
Extreme cases Οπίσθιο μέρος του υδρόφιλου σύρματος
Οπίσθιο μέρος του υδρόφιλου σύρματος Re-entry arterial devises Βελόνα TIPS Ειδικά σύρματα αποφράξεων

56
Extreme cases E. N. Brountzos et al. CVIR 2011
Οίδημα άνω άκρου, άλγος, εξέλκωση 14mm Stent in stent (substent technique) Μεταδιαστολή 14mm Outback LTD re-entry catheter
 Μεταδιαστολή 14mm. Outback LTD re-entry catheter.")
57
Extreme cases McGuckin, et al. Endvascular Today 2009
Υποκλείδιος φλέβα Βηματοδότης ΕΣΦ θήκη ινώδους ιστού

58
Extreme cases McGuckin, et al. Endvascular Today 2009
Snare από την ΕΣΦ Baylis RF PowerWire from the subclavian

59
Extreme cases Επανασυραγγοποίηση με αιχμηρή βελόνη TIPS
Αεροθάλαμος για στοχευόμενη επανείσοδο

60
Trans-septal needle (BRKTM-1, 71 cm; St Jude Medical, MN, USA

61
Extreme cases Επανασυραγγοποίηση με αιχμηρή βελόνη TIPS

62
Ευχαριστώ για τη προσοχή σας

63
Venographic Classification of SVC Syndrome
STANFORD ET AL. AJR 148: , February 1987

64
Venographic Classification of SVC Syndrome-Contd.
AJR 148: , February 1987 STANFORD ET AL.

65
CT Diagnosis of Superior Vena Cava Syndrome: Importance of Collateral Vessels
It was believed at that time that CT diagnosis of obstruction of the superior vena cava (SVC) or its major tributaries required at least two findings: One was lack of (or decreased) opacification of central venous structures distal to the site of obstruction. (This may be associated with a visible, obstructing lesion or intraluminal filling defects.) The other CT finding was opacification of collateral venous vessels. The fulfillment of either criterion alone was insufficient for an accurate CT diagnosis of venous obstruction. Results of their study: The presence of collateral vessels, regardless of the number and location of the vessels shown on CT scans, was highly accurate as a predictor of superior vena cave syndrome, with a sensitivity of 96% and a specificity of 92%. The most common site of venous obstruction seen on CT scans was the SVC (n = 41), followed by the brachiocephalic vein (n = 20) and the jugular vein (n = 2). KIM ET AL. AJA:161, September1993
 or its major tributaries required at least two findings: One was lack of (or decreased) opacification of central venous structures distal to the site of obstruction. (This may be associated with a visible, obstructing lesion or intraluminal filling defects.) The other CT finding was opacification of collateral venous vessels. The fulfillment of either criterion alone was insufficient for an accurate CT diagnosis of venous obstruction. Results of their study: The presence of collateral vessels, regardless of the number and location of the vessels shown on CT scans, was highly accurate as a predictor of superior vena cave syndrome, with a sensitivity of 96% and a specificity of 92%. The most common site of venous obstruction seen on CT scans was the SVC (n = 41), followed by the brachiocephalic vein (n = 20) and the jugular vein (n = 2). KIM ET AL. AJA:161, September1993.")
66
Clinical and Radiological Grading of Superior Vena Cava Obstruction
Plekker et al Respiration 2008;76:69–75

67
Clinical and Radiological Grading of Superior Vena Cava Obstruction-Contd.
Plekker et al Respiration 2008;76:69–75

68
Clinical and Radiological Grading of Superior Vena Cava Obstruction-Contd.
Plekker et al Respiration 2008;76:69–75

69
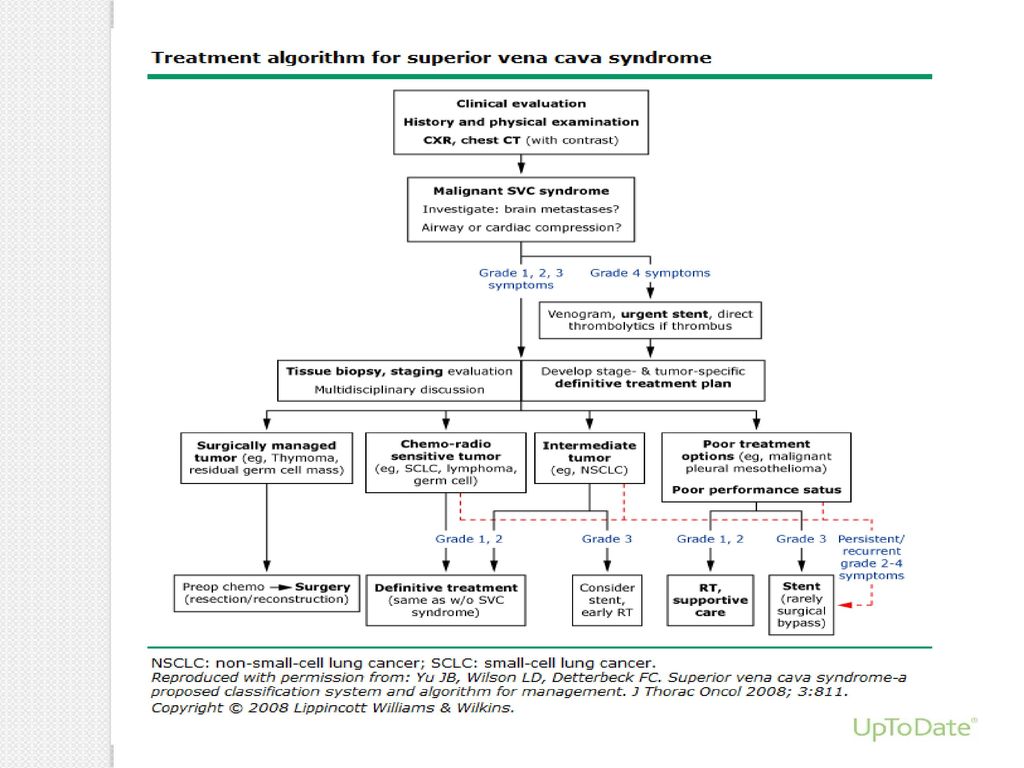
Treatment Algorithm for Malignant Causes

70
There are four possible collateral systems which were first described in 1949 by McIntire and Sykes.
They are represented by Azygos venous system, Internal thoracic venous system, Vertebral venous system and External thoracic venous system. McIntire FT, Sykes EM jr. Obstruction of the superior vena cava: Ann Intern Med 1949; 30:925. 1.

71
Azygos venous system is the only direct path into the SVC.
Internal thoracic vein is the collector between SVC and inferior vena cava (IVC) via epigastric and iliac veins. Vertebral veins with intercostals, lumbar and sacral veins, represent the posterior network between SVC and IVC. External thoracic vein system is the most superficial and it is represented by axillary, lateral thoracic and superficial epigastric veins.
 via epigastric and iliac veins. Vertebral veins with intercostals, lumbar and sacral veins, represent the posterior network between SVC and IVC. External thoracic vein system is the most superficial and it is represented by axillary, lateral thoracic and superficial epigastric veins.")
72
Etiology May be related to various etiological factors.
Malignancies are predominant (95%) while, in the past, infectious diseases used to be common. During the last century, progression in anti-bacterial therapies and improvement in social conditions have led to a consistent decrease in the benign origin. Incidence of iatrogenic SVCS is currently increasing. Wan JF, Bezjak A. Superior vena cava syndrome. Hematol Oncol Clin North Am. 2010;24:501-13
 while, in the past, infectious diseases used to be common. During the last century, progression in anti-bacterial therapies and improvement in social conditions have led to a consistent decrease in the benign origin. Incidence of iatrogenic SVCS is currently increasing. Wan JF, Bezjak A. Superior vena cava syndrome. Hematol Oncol Clin North Am. 2010;24:")
73
Pathophysiology Pathogenetic basis of SVCS is obstruction to the blood flow. It can result from intrinsic or extrinsic obstacles. Intrinsic—uncommon, caused by thrombosis or invading tissue. Extrinsic factors develop from compression or stricture of the vein. In physiologic conditions, blood return to the right atrium is facilitated by the pressure gradient between the right atrium and venae cavae.

74
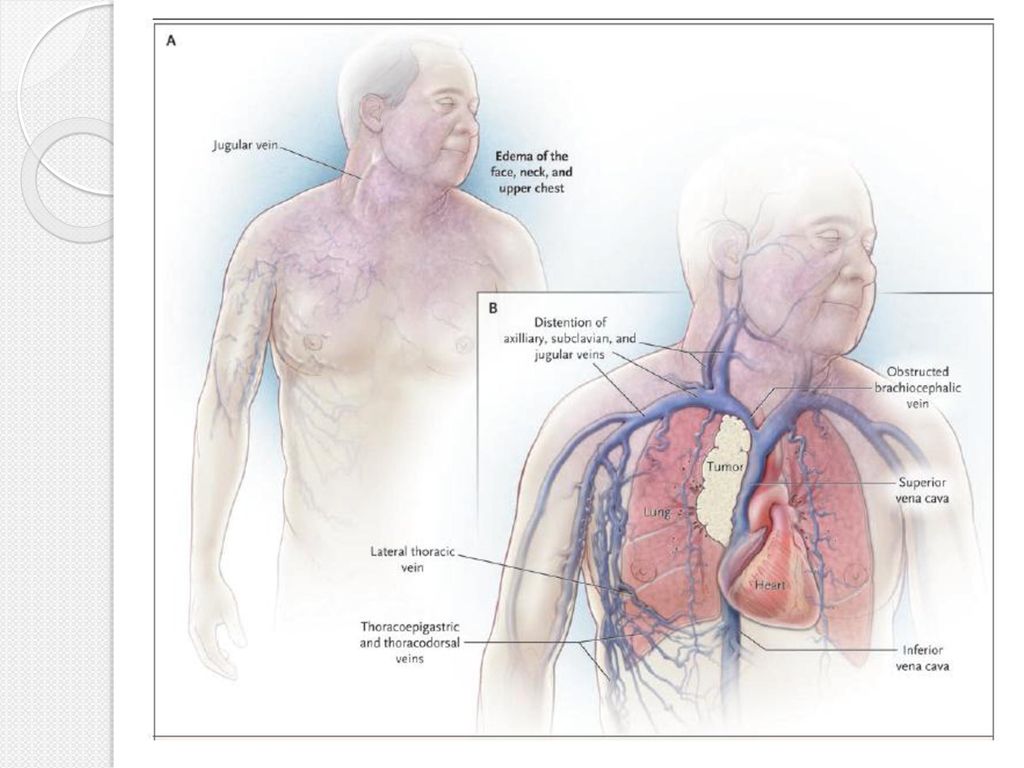
Clinical presentation
The SVC wall does not offer resistance to compression. When SVC lumen reduction is greater than 60%, hemodynamic changes occur: Proximal dilatation, Congestion and Flow slowdown. The clinical signs of this condition are mainly represented by Cyanosis (due to venous stasis with normal arterial oxygenation) and Edema of the upper chest, arms, neck and face (periorbital initially).
 and. Edema of the upper chest, arms, neck and face (periorbital initially).")
75
Swelling is usually more important on the right side, because of the better possibility of collateral circulation in the left brachiocephalic vein compared to the contralateral. Vein varicosities of the proximal tongue and dark purple ears are also typical. Other signs or symptoms are: Coughing, Epistaxis, Hemoptysis, Dysphagia, Dysphonia and Hoarseness (caused by vocal cord congestion), Esophageal, Retinal and Conjuntival bleeding.
, Esophageal, Retinal and Conjuntival bleeding.")
78
The clinical seriousness is related to several factors:
Level of obstruction and rapidity of development, determining the effectiveness of collateral circulation Impairment of lymphatic drainage (pulmonary interstitial edema or pleural effusion) Involvement of other mediastinal structures (compression or invasion of heart, pulmonary artery and central airways, phrenic nerve paralysis…)
 Involvement of other mediastinal structures (compression or invasion of heart, pulmonary artery and central airways, phrenic nerve paralysis…)")
79
Superficial dilated vascular routes are the main sign of collateral circulation and appear swollen and non-pulsating. In case of marked obesity, superficial veins can be missing at inspection. Variety of collateral circulation and the differences in the venous rearrangement are expression of the SVC obstruction site. Anatomic classification includes three levels of obstruction: Obstruction of the upper SVC, proximal to the azygos entry point. Obstruction with azygos involvement. Obstruction of the lower SVC, distal to the azygos entry point.

80
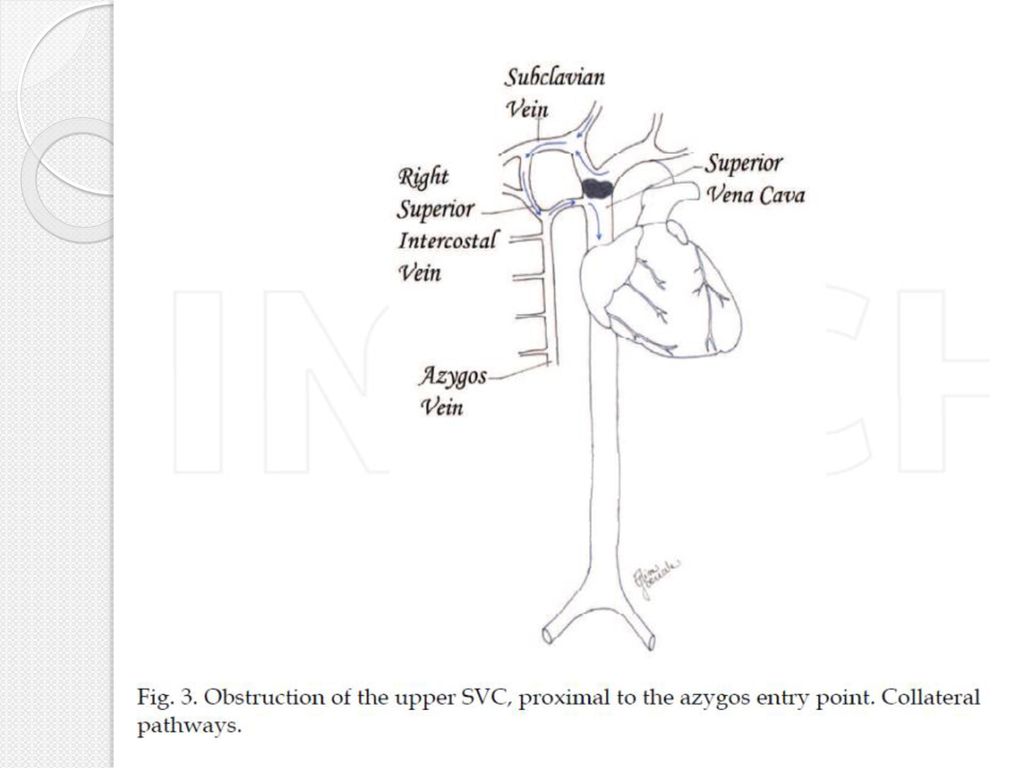
Obstruction of the upper SVC, proximal to the azygos entry point.
In this situation, there is no impediment to normal blood flow through the azygos vein which opens into the patent tract of the SVC. Venous drainage coming from the head neck, shoulders and arms cannot directly reach the right atrium. A longer but effective way is provided by several veins, the most important being the right superior intercostal vein.

81
From the superior tract of the SVC, blood flow is reversed and directed to the azygos, mainly through the right superior intercostal vein. Azygos collateral system is eminently deep; therefore the presence of superficial vessels is usually lacking, even if possible in the area of the internal thoracic vein’s superficial tributaries. Volumetric increase of the vessels can be consistent and capacity may increase up to 8 times. The efficiency of this collateral route is reliable, thus the clinical compensation is unbalanced only in the case of a rapid development of the obstruction or if the stenosis is more than 90%.

83
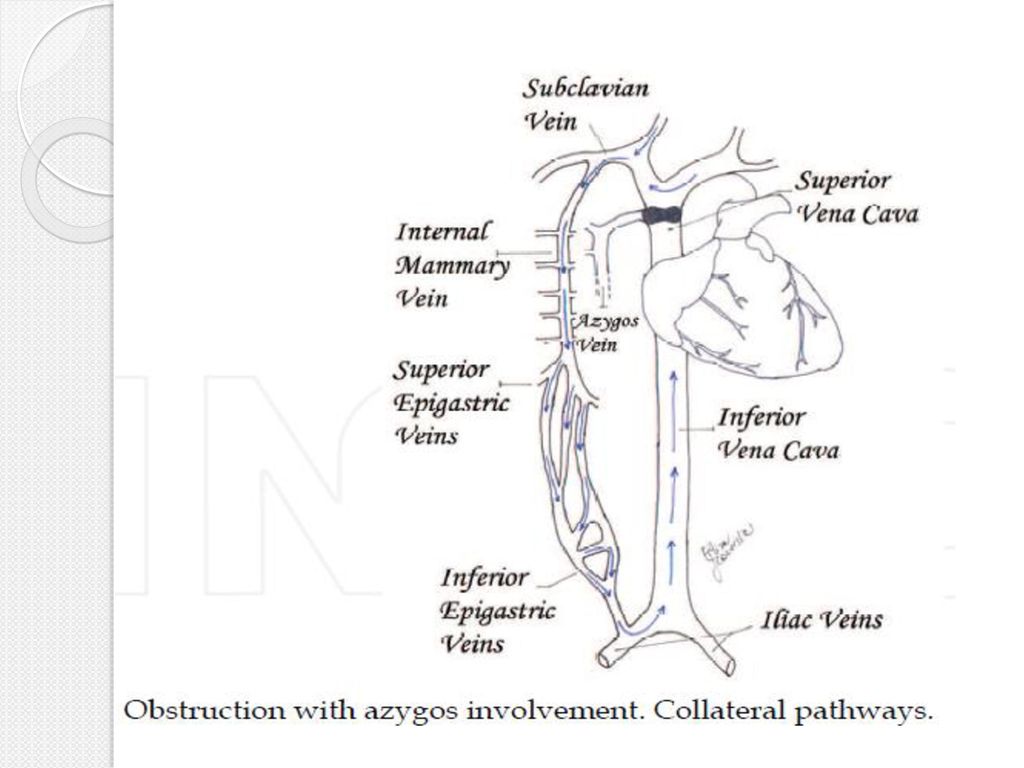
Obstruction with azygos involvement.
In this case, the azygos vein cannot be available as collateral pathway and the only viable blood return is carried by minor vessels to IVC (cava-cava or anazygotic circulation). From the internal thoracic veins, blood is forced to the intercostal veins, then to azygos and hemiazygos veins. The flow is thus reversed into the ascending lumbar veins to the iliac veins.
. From the internal thoracic veins, blood is forced to the intercostal veins, then to azygos and hemiazygos veins. The flow is thus reversed into the ascending lumbar veins to the iliac veins.")
84
Direct anastomosis between the azygos’ origin and the IVC and between hemiazygos and left renal vein are also active. In addition, the internal thoracic veins can flow into the superior epigastric veins. From the superior epigastric veins, blood is carried to the inferior epigastric veins across the superficial system of the cutaneous abdominal veins and finally to the iliac veins. Another course is between the thoraco-epigastric vein (collateral of the axillary vein) and the external iliac vein.
 and the external iliac vein.")
85
In these conditions, the collateral circulation is partly deep and partly superficial.
Physical examination often reveals SVC obstruction. The reversed circulation through the described pathways, remains less efficient than the azygos system and venous hypertension is usually more severe. For this reason, this kind of SVC obstruction is often related to important symptoms, dyspnea and pleural effusion. The ensuing slow blood flow may be responsible for superimposed thrombosis.

87
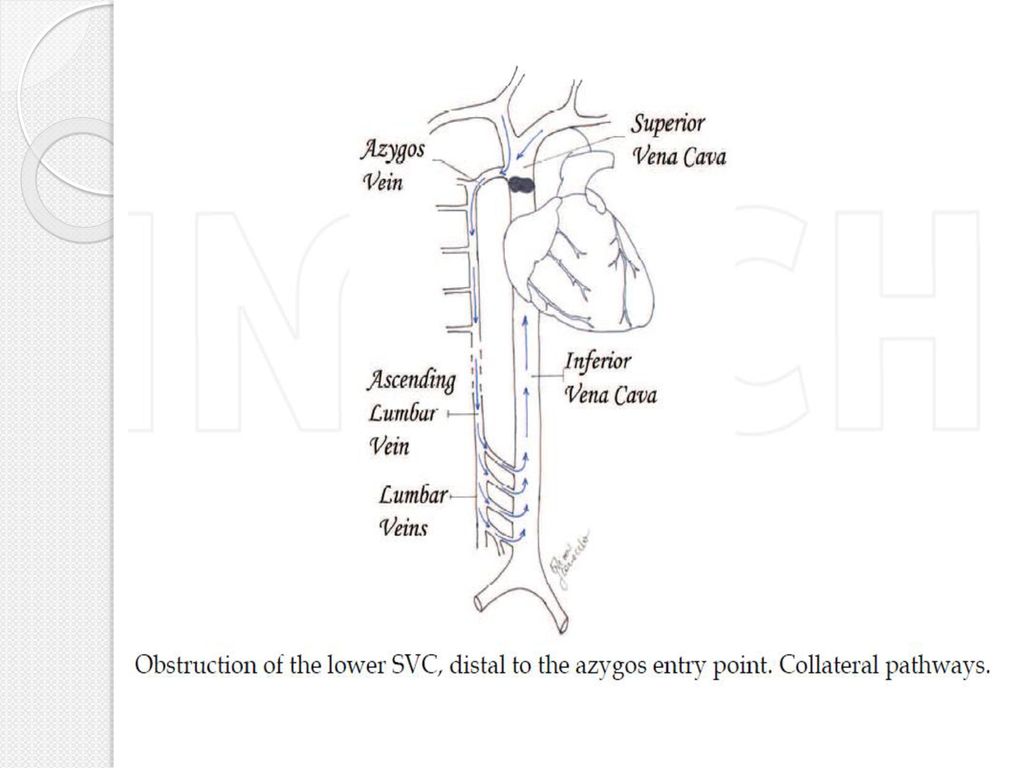
Obstruction of the lower SVC, distal to the azygos entry point.
In this condition, the obstruction is just below the azygos arch. The blood flow is distributed from the superior body into the azygos and hemiazygos veins, in which the flow is inverted, to the IVC tributaries.

88
In this type of case, the superficial collateral system is not always evident but the azygos and hemiazygos congestion and dilatation are usually important. The hemodynamic changes lead to edema and cyanosis of the upper chest and pleural effusion. Pleural effusion is often slowly-growing and rightsided, probably due to anatomical reasons: There is a wider anastomosis between hemiazygos and IVC than between azygos and IVC.

90
Classification of SVCS
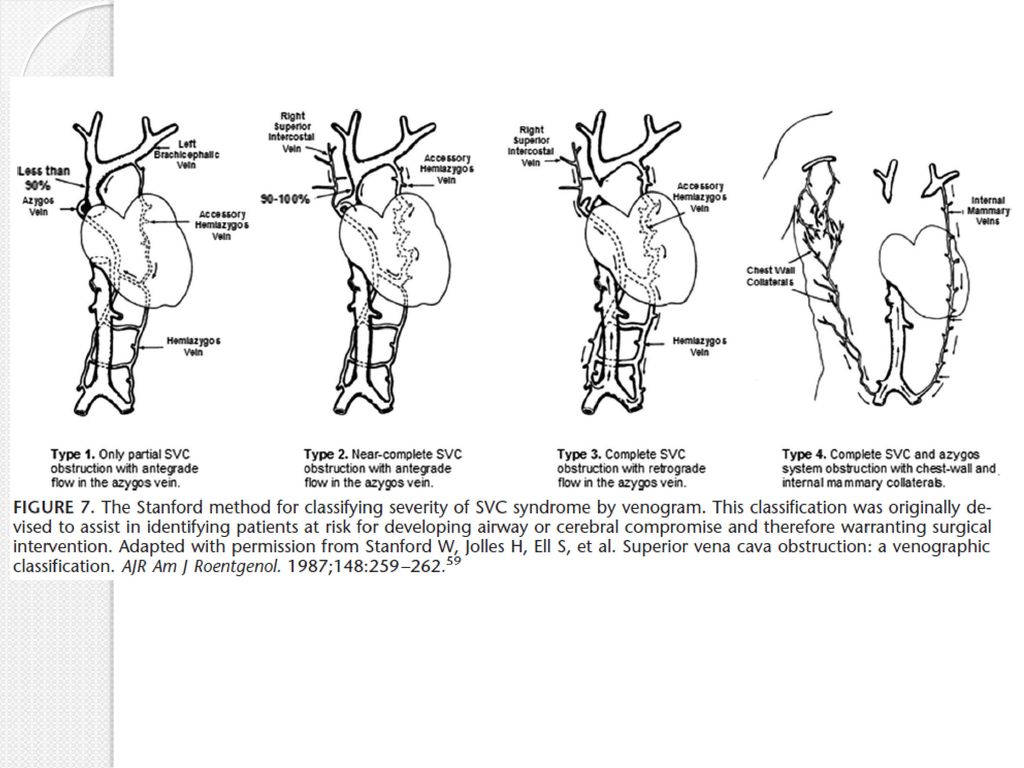
There are three main classification proposals which follow different methods of categorization. Doty and Standford’s classification (anatomical) Type I: stenosis of up to 90% of the supra-azygos SVC Type II: stenosis of more than 90% of the supra-azygos SVC Type III: complete occlusion of SVC with azygos reverse blood flow Type IV: complete occlusion of SVC with the involvement of the major tributaries and azygos vein
 Type I: stenosis of up to 90% of the supra-azygos SVC. Type II: stenosis of more than 90% of the supra-azygos SVC. Type III: complete occlusion of SVC with azygos reverse blood flow. Type IV: complete occlusion of SVC with the involvement of the major tributaries and azygos vein.")
92
Yu’s classification (clinical)
Grade 0: asymptomatic (imaging evidence of SVC obstruction) Grade 1: mild (plethora, cyanosis, head and neck edema) Grade 2: moderate (grade 1 evidence + functional impairment) Grade 3: severe (mild/moderate cerebral or laryngeal edema, limited cardiac reserve) Grade 4: life-threatening (significant cerebral or laryngeal edema, cardiac failure) Grade 5: fatal
 Grade 1: mild (plethora, cyanosis, head and neck edema) Grade 2: moderate (grade 1 evidence + functional impairment) Grade 3: severe (mild/moderate cerebral or laryngeal edema, limited cardiac reserve) Grade 4: life-threatening (significant cerebral or laryngeal edema, cardiac failure) Grade 5: fatal.")
93
Bigsby’s classification (operative risk)
Low risk High risk The low risk patients present: No dyspnea at rest, No facial cyanosis in the upright position, No change of dyspnea and No worsening of facial edema and Cyanosis, during the supine position. The high risk patients present facial cyanosis or dyspnea at rest in the sitting position.

94
Diagnosis Physical examination is often crucial:
Presence of edema and superficial venous network of the upper chest may support the clinical diagnosis. Imaging studies are however required. Most cases are suspected at the standard chest X-ray and the most common radiological findings are right mediastinal widening and pleural effusion.

95
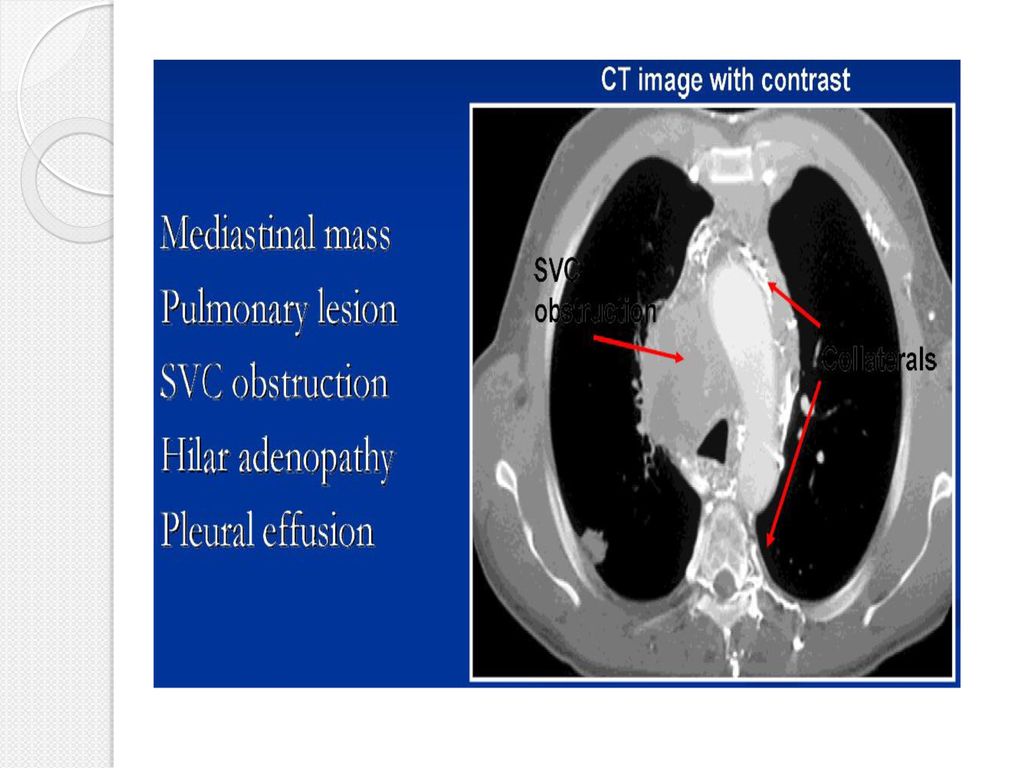
CT with multislice detector is the most useful tool in the evaluation of the mediastinal syndromes.
Intravenous contrast should be administered, in order to provide high-quality vascular imaging. Contrast enhanced multidetector CT may show Site of the obstruction, Some aspects of the primary disease and Eventual intraluminal thrombi. The contrast flow can also help to distinguish the extent of the collateral network

98
MRI plays a side role; it is indicated when CT cannot be performed (e
MRI plays a side role; it is indicated when CT cannot be performed (e.g. pregnancy, endovenous contrast intollerance). Invasive venography – Now ραely used due to the huge improvement in vascular CT imaging. It is currently performed only as a preliminary to operative procedures such as stent placement. Once the thoracic imaging is obtained, the work-up should include brain, abdominal and bone studies in view of the probable malignant nature of the primary lesion. Recently Fluorodeoxyglucose-Positron Emission Tomography has gained an important role.
. Invasive venography – Now ραely used due to the huge improvement in vascular CT imaging. It is currently performed only as a preliminary to operative procedures such as stent placement. Once the thoracic imaging is obtained, the work-up should include brain, abdominal and bone studies in view of the probable malignant nature of the primary lesion. Recently Fluorodeoxyglucose-Positron Emission Tomography has gained an important role.")
99
The histological diagnosis remains the key factor for the causative treatment, in the case of neoplastic etiology. Superficial adenopathies have to be carefully investigated in order to find a possible source of tissue and the easiest target for biopsy. The invasive diagnostic procedure varies largely depending on the suspected malignancy and its site.

100
The biopsy can be obtained through
Traditional bronchoscopy or Echo-guided endoscopy, Superficial node biopsy, Mediastinoscopy, Mediastinotomy, Transthoracic needle biopsy, Thoracoscopy, Cervical or supraclavicular biopsies; Thoracotomy and sternotomy are rarely indicated.

101
Treatment Therapy should be causative.
Syndrome management recognizes different levels of priority depending on the Severity of symptoms, Etiology and Prognosis. The therapeutic plan is usually targeted to clinical palliation. In fact, most cases are diagnosed as advanced-stage malignancies.

102
Supportive Care Elevate the patient’s head to decrease the hydrostatic pressure and thereby the edema. Oxygen, Glucocorticoid therapy (dexamethasone, 4 mg every 6 hours) is commonly prescribed, although its effects have not been formally well studied, Glucocorticoids reduce the tumor burden in lymphoma and thymoma and are therefore more likely to reduce the obstruction in pts with lymphoma or thymoma than in those with other types of tumor.
 is commonly prescribed, although its effects have not been formally well studied, Glucocorticoids reduce the tumor burden in lymphoma and thymoma and are therefore more likely to reduce the obstruction in pts with lymphoma or thymoma than in those with other types of tumor.")
103
Loop diuretics are also commonly used, but it is unclear whether venous pressure distal to the obstruction is affected by small changes in right atrial pressure. In malignancy, the treatment can have palliative or, rarely, curative intent. Chemotherapy is usually employed in lymphomas, small- cell lung cancer and germ cell tumors. Besides chemotherapy, radiotherapy is widely used in the treatment of non-small cell lung cancer.

104
Some cases must be approached as an emergency.
In this type of situation, the treatment of choice is usually endovascular with the aim of restoring blood flow as soon as possible. Acute lifethreatening presentation is the only situation in which radiotherapy before histological diagnosis can be considered. However, this approach should be avoided, whenever possible. RT prior to biopsy may obscure the histologic diagnosis.

105
Current guidelines stress the importance of accurate histologic diagnosis prior to starting therapy, and the upfront use of endovascular stents in severely symptomatic patients to provide more rapid relief than can be achieved using RT. Kvale PA, Selecky PA, Prakash UB, American College of Chest Physicians. Palliative care in lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007; 132:368S.
. Chest 2007; 132:368S.")
106
Important exceptions to this general approach are pts who present with stridor due to central airway obstruction or severe laryngeal edema, and those with coma from cerebral edema. These situations represent a true medical emergency, and these patients require immediate treatment (stent placement and RT) to decrease the risk of sudden respiratory failure and death.
 to decrease the risk of sudden respiratory failure and death.")
107
For pts who have obstruction of the SVC resulting from intravascular thrombus associated with an indwelling catheter, removal of the catheter is indicated, in conjunction with systemic anticoagulation to limit extension of thrombus. Radiation therapy — RT provides considerable relief by reducing tumor burden Symptomatic improvement is usually apparent within 72 hours. Relief of symptoms may not be achieved for up to four weeks, and approximately 20 percent of pts do not obtain symptomatic relief from RT

108
Surgical intervention
Although effective and a/w relatively few complications, surgical bypass is rarely performed in pts with malignant cause of SVC syndrome because of the success of endovascular stenting. Surgical management is more often undertaken in patients with benign causes of SVC syndrome. Surgical resection of mediastinal tumor and reconstruction of the SVC is rarely considered in view of its morbidity and mortality and the limited life expectancy of most pts who present with this complication.

109
One possible exception is malignant thymoma and thymic carcinoma, which are relatively resistant to chemotherapy and radiation The main proposal for SVC resection is direct infiltration in thymomas or in N0-N1 non-small cell lung cancer. In case of infiltration of < 30% of the SVC circumference, direct suture is favored

110
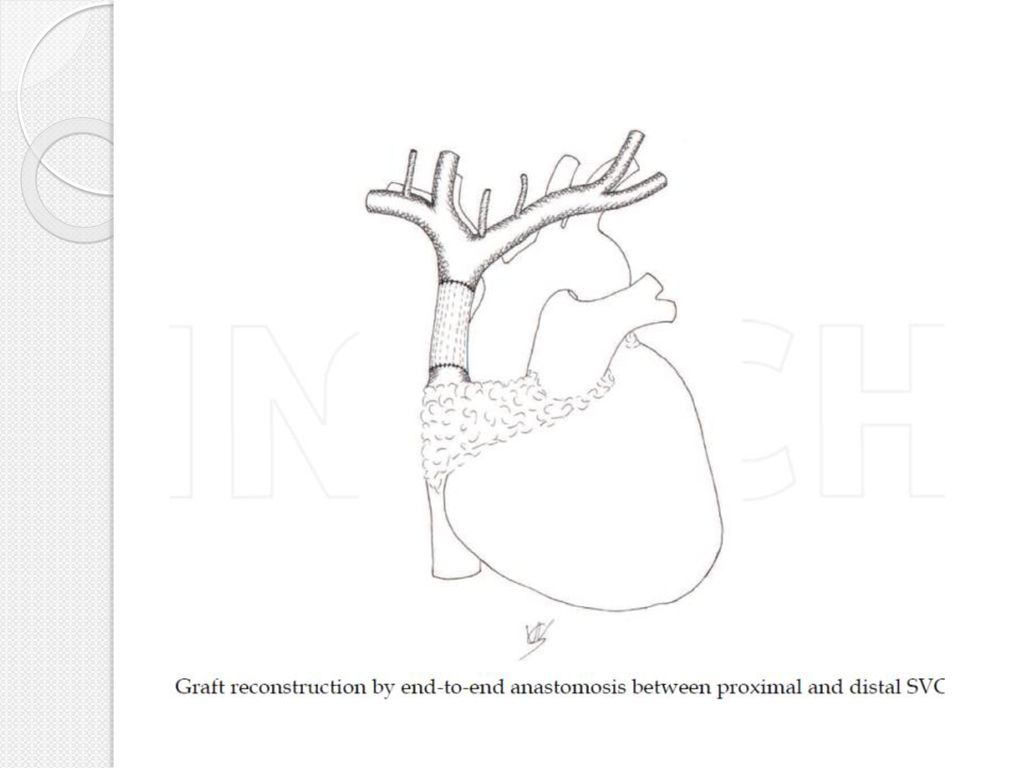
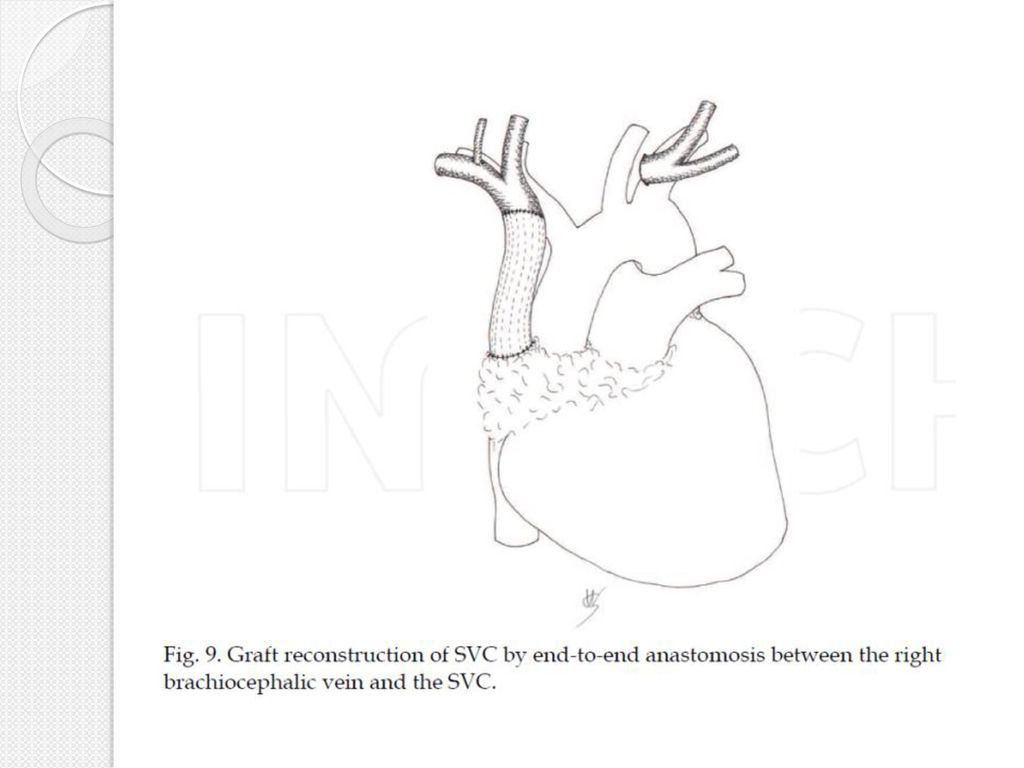
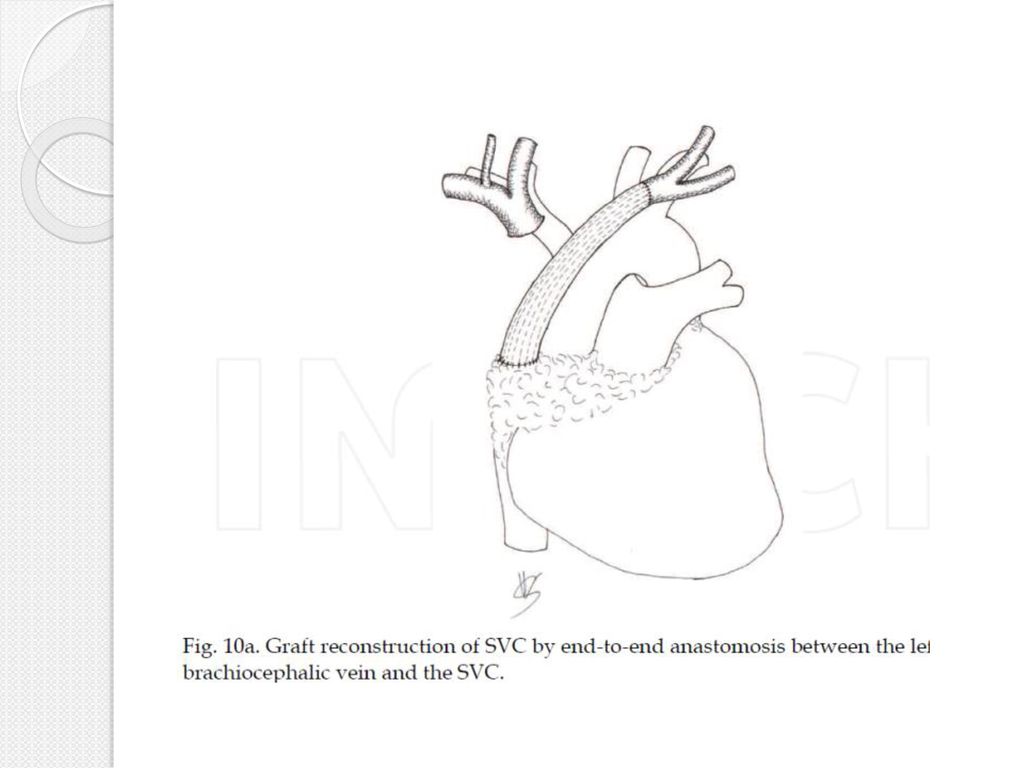
Larger involvements require a prosthetic repair.
Armoured PTFE grafts and biologic material are the preferred choices. Morbidity after SVC surgical procedures is high and the post-operative care must be intensive. Long-term patency of a SVC by-pass graft is uncertain but, usually, the slow onset of the graft thrombosis favors the development of effective collateral circulation.

Παρόμοιες παρουσιάσεις


 ΕΝΔΟΑΥΛΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΣΤΑΥΡΟΣ ΓΑΛΑΝΗΣ ΕΙΔΙΚΕΥΟΜΕΝΟΣ ΑΚΤΙΝΟΔΙΑΓΝΩΣΤΙΚΗΣ ΤΜΗΜΑ ΕΠΕΜΒΑΤΙΚΗΣ.>")



 : ΑΝΟΙΧΤΩΝ Vs ΚΛΕΙΣΤΩΝ ΚΥΨΕΛΩΝ>")






, Performance Indicators (PIs), Key Performance Indicators (KPIs)>")



. ΣΥΓΚΟΠΤΙΚΗ ΚΡΙΣΗ Αιφνίδια και σύντομη απώλεια συνείδησης που προκαλείται από ανεπαρκή εγκεφαλική αιμάτωση λόγω μειωμένης.>")



