Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Expanding the biomarker toolbox: BRAF in mCRC September 2015

2
2 Content Outline mCRC Distinct Molecular Phenotypes in mCRC44 The Role of BRAF in mCRC1111 ESMO/NCCN Recommendations for BRAF MT Patients2222 Prognosis of BRAF MT Tumours2424 Treatment Options for BRAF MT Patients2727 FOLFOXIRI + Bev BRAF Inhibitors BRAF + EGFR +/– MEK or PI3K Inhibitors Market Research Results3636 Beyond RAS – Summary and Future Directions4040 Upcoming Trials Assessing BRAF MT4848 NOTE: Complete slide references are contained within the notes.

3
3 CRC Biomarker Funnel – Distinct Molecular Phenotypes Guide Treatment Decisions KRAS NRAS BRAF PTEN PIK3CA EGFR AKT TP53 CTNNB1 BRAF MT NRAS MT RAS WTKRAS MT TP53 MT EGFR MT mCRC AKT, protein kinase B; mt, mutant; PTEN, phosphatase and tensin homolog.

4
4 *KRAS WT tumours. NOTE: Informal comparison as these are not head-to-head clinical trials. 5-FU, 5-fluorouracil; FOLFIRI, 5-FU + LV + irinotecan; FOLFOX, 5-FU + LV + oxaliplatin; FOLFOXIRI, 5-FU + LV + oxaliplatin + irinotecan; IFL, irinotecan/bolus 5-FU/LV; LV, leucovorin; XELOX, capecitabine + oxaliplatin. 1. Saltz. 2000; 2. Douillard. 2000; 3. Goldberg. 2004; 4. Hurwitz. 2004; 5. Saltz. 2008; 6. Falcone. 2007; 7. Bokemeyer. 2011; 8. Van Cutsem. 2011; 9. Douillard. 2011; 10. Passardi. 2013; 11. Heinemann. 2013; 12. Venook. 2014; 13. Loupakis. 2015. VEGF and EGFR Inhibitors in Combination with Chemotherapy Have Substantially Altered mCRC Outcome

5
5 Any RAS MT Disease Results in Shorter Survival Compared with KRAS WT KRAS WT Any/Other* RAS MT CRYSTAL 3,4 CALGB* 10 OPUS 1,2 PRIME 5,6 FIRE-3 7,8 TRIBE 9 FOLFOX FOLFOX + cetuximab FOLFIRI FOLFIRI + cetuximab FOLFOX FOLFOX + panitumumab FOLFIRI + bevacizumab FOLFIRI + cetuximab FOLFIRI + bevacizumab FOLFOXIRI + bevacizumab Chemo + bevacizumab Chemo + cetuximab 18.5 22.8 20.0 23.5 19.7 23.9 25.0 28.7 26.8 29.0 29.9 37.1 KRAS WT Any/Other* RAS MT Overall Survival (months) 22.3* 28.7* 23.9 20.2 20.6 15.6 19.2 16.4 17.7 13.5 17.8 27.3 Only phase III trials with data for patients with any RAS MT are shown. *Data for KRAS exon 2 WT, MT in KRAS exon 3, 4, or NRAS exon 2, 3, or 4. 1. Bokemeyer. 2011; 2. Bokemeyer. 2014; 3. Van Cutsem. 2011; 4. Ciardiello. 2014; 5. Douillard. 2011; 6. Douillard. 2013; 7. Heinemann. 2013; 8. Stintzing. 2014; 9. Loupakis. 2015; 10. Lenz. 2014.

6
6 Douillard. 2013. EXON 1EXON 2**EXON 3EXON 4 EXON 1EXON 2*EXON 3EXON 4 KRAS NRAS 40% 1213 1213 5961 5961 117146 117146 4%6% 3%4%NT BRAF 600 EXON 15 8% *Prevalence is defined as mutations detected in a population of patients with WT KRAS exon 2 tumours whose tissues were deemed evaluable for RAS testing. **The KRAS exon 2 data are from the overall population Old test New, extended test Extended Testing Identified Prevalence of New Mutations Beyond KRAS Exon 2

7
7 Realisation of Other RAS Mutations = Shifted Frequency and Further Limits Population Eligible for Anti-EGFR mAbs Peeters. 2015. KRAS WT KRAS MT RAS WT RAS MT Meta-Analysis of >3,000 Patients from Randomised Clinical Trials The proportion of RAS WT patients has decreased 13.7% have other RAS mutations (KRAS exon 3 and 4, and NRAS mutations)
.")
8
8 Beyond KRAS: There Are Myriad Genes Involved in CRC 1. Sorich. 2015; 2. Sayar. 2008. RAS/ BRAF WT RAS/ BRAF MT Approximately 8% have BRAF mutations Meta-Analysis of >3,000 Patients from Randomised Clinical Trials 1 KRAS WT KRAS MT 13.7% have other RAS mutations (KRAS exon 3 and 4, and NRAS mutations) A myriad of additional gene mutations known to exist in mCRC 2 may have prognostic and/or predictive utility PIK3CA PTEN FGFR3 ERBB2
 A myriad of additional gene mutations known to exist in mCRC 2 may have prognostic and/or predictive utility PIK3CA PTEN FGFR3 ERBB2.")
9
9 Most Mutations Are Mutually Exclusive; However, Some May Co-Exist Tumours traditionally denoted KRAS WT (based on mutations in KRAS exon 2; codon 12 or 13) may have been carrying an NRAS, BRAF, PIK3CA, or PTEN mutation, or a mutation in another codon of KRAS (61 or 146) 1,2 *Exons 9 and 20. 1. De Roock. 2010; 2. Sartore-Binache. 2009. PTEN loss BRAF PIK3CA* KRAS MT n = 132 mCRC treated patientsn = 773 mCRC treated patients 23 12 1 2 2 5 1 3 6 1 21

10
10 The BRAF Story BRAF is a downstream effector of activated KRAS –KRAS and BRAF mutations tend to be mutually exclusive 1,2 –>95% of BRAF mutations are in the V600E kinase activation domain of the protein 3,4 –Major negative prognosticator in CRC 1. Lievre. 2006; 2. Benventui. 2007; 3. Di Nicolantonio. 2008; 4. Laurent-Puig. 2009. BRAF

11
11 Mutation Status Is Prognostic in CRC: Wildtype > RAS MT > BRAF MT Sinicrope. 2015. Stage III Colon Cancer Treated with 5-FU-based Adjuvant Chemotherapy (n = 737) 0 10 20 30 40 50 60 70 80 90 100 012 347311265236215197 270233187163148140 28 22 18 15 13 13 33 27 26 23 19 19 59 5146 44 40 39 24364860 5-yr DFS Rate(95% CI)P-value Non mutated BRAF V600E & KRAS, pMMR65.3%(65.3-70.6)REF Mutant KRAS, pMMR57.7%(60.3-73-9).0265 Mutant BRAF V600E, pMMR49.2%(33.6-72.1).1770 Sporadic dMMR71.0%(56.4-89.1).2940 Familial dMMR70.9(60.1-83.6).1857 Months Since Diagnosis Event-Free Survival, % Overall P-value =.0142
 yr DFS Rate(95% CI)P-value Non mutated BRAF V600E & KRAS, pMMR65.3%( )REF Mutant KRAS, pMMR57.7%( ).0265 Mutant BRAF V600E, pMMR49.2%( ).1770 Sporadic dMMR71.0%( ).2940 Familial dMMR70.9( ).1857 Months Since Diagnosis Event-Free Survival, % Overall P-value =")
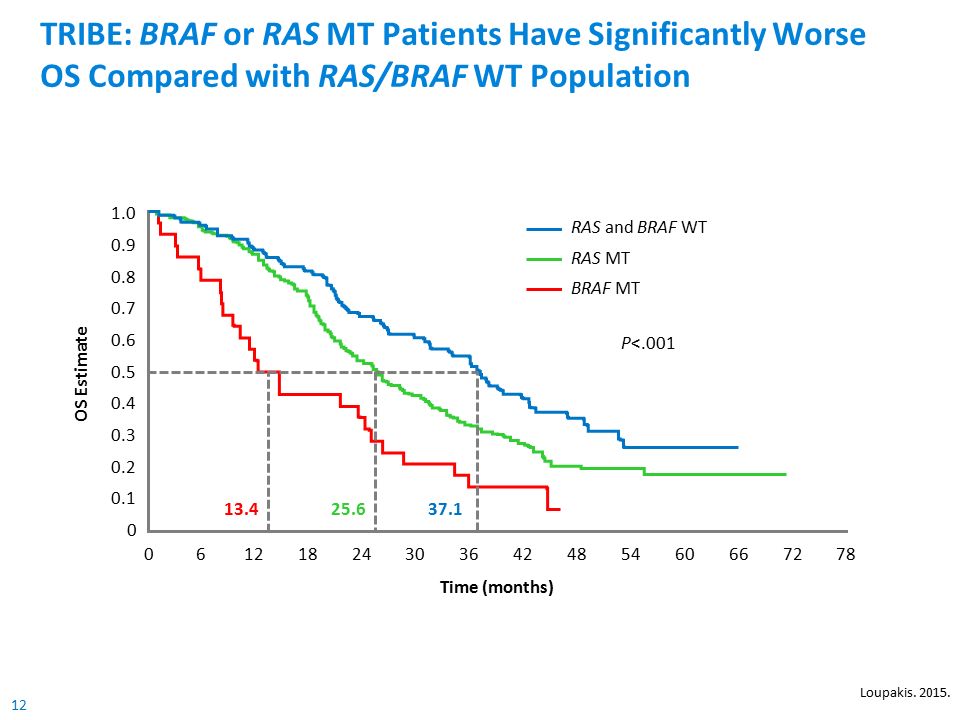
12
12 TRIBE: BRAF or RAS MT Patients Have Significantly Worse OS Compared with RAS/BRAF WT Population P<.001 OS Estimate 1.0 0.9 0.7 0.5 0.2 0 Time (months) 0.8 0.6 0.3 0.4 0.1 06121824303642485460667278 RAS and BRAF WT RAS MT BRAF MT 25.637.113.4 Loupakis. 2015.
13
13 TRIBE: OS 1 and PFS 2 According to Molecular Subgroups A multivariate model accounting for factors significantly associated with shorter OS was developed 1 –Treatment effect on OS: Adjusted HR = 0.79 (95% CI: 0.61–1.04), P =.087 –Effect of BRAF mutation: HR = 2.24 (95% CI: 1.32–3.81), P =.003 –Effect of RAS mutation: HR = 1.30 (95% CI: 0.94–1.79), P =.113 The benefit of bevacizumab + FOLFOXIRI is consistent across all molecular subgroups *P for interaction. 1. Loupakis. 2015; 2. Cremolini. 2015. Median OS, monthsMedian PFS, months n FOLFIRI + Bevacizumab FOLFOXIRI + Bevacizumab HRP Value FOLFIRI+ Bevacizumab FOLFOXIRI + Bevacizumab HRP Value ITT population50825.829.80.80.0309.712.30.77.006 RAS and BRAF evaluable 35724.928.60.84.1599.812.10.80.042 RAS and BRAF WT9333.541.70.77.522* 12.213.70.85.679* RAS MT23623.927.30.889.512.00.78 BRAF MT2810.719.00.545.57.50.57 RAS WT12126.837.10.78.658* 11.012.80.84.767* RAS MT23623.927.30.889.512.00.78

14
14 Exploring Outcomes of BRAF MT Advanced CRC Patients Analysis Design GenotypingKRAS c.12–13,61,146, NRAS c.12–13,61, and BRAF V600E Study populationTreated with chemotherapy alone (n = 2,530) Phase III RCTCOIN: 1L OxFp either continuously or with planned CT-free intervals FOCUS: Sequencing trial of 1L and planned 2L treatment with 5-FU alone, or IrFU or OxFp PICCOLO: 2L treatment with irinotecan alone EndpointsOS, PFS, P-PS, and response rate ObjectiveAnalysis of individual patient data to compare outcomes of BRAF MT and WT patients; analysis adjusted for relevant prognostic factors, eg, primary tumour site Arm B Cont. OxFp + Cmab (n = 662) Arm C Intermittent OxFp (n = 652) Strategy A: 5-FU; Ir on prog FOCUS – 1L aCRC ISRTN 79877428 Sponsor: MRC CTU (N = 2,135) COIN – 1L aCRC ISRTN 27286448 Sponsor: MRC CTU Funder: CRUK, UK MRC, Merck (N = 2,445) PICCOLO – 2L aCRC ISRTN 79877428 Sponsor: University of Leeds Funder: CRUK, Amgen Inc (N = 1,196) BRAF status available (n = 787) BRAF status available (n = 1,946) KRAS MT BRAF available (n = 477) KRAS WT BRAF available (n = 591) Trial arm(s) included in RR, PFS, P-PS, and OS analysis Trial arm(s) included in RR and OS analysis Trial arm(s) excluded from all analysis Strategy B: 5-FU; IrFU or OxFU on prog (n = 371) Strategy C: IrFU or OxFU until prog (n = 357) Arm A Cont. OxFp (n = 632) Ir (n = 189) IrCs (n = 288) IrPan (n = 321) Ir (n = 270) Cmab, cetuximab; Cs, cyclosporine; Fp, fluoropyrimidine; FU, fluorouracil; Ir, irinotecan; Ox, oxaliplatin; Pan, panitumumab; P-PS, post-progression survival; RCT, randomised controlled trial. Seligmann. 2015.
 Arm C Intermittent OxFp (n = 652) Strategy A: 5-FU; Ir on prog FOCUS – 1L aCRC ISRTN Sponsor: MRC CTU (N = 2,135) COIN – 1L aCRC ISRTN Sponsor: MRC CTU Funder: CRUK, UK MRC, Merck (N = 2,445) PICCOLO – 2L aCRC ISRTN Sponsor: University of Leeds Funder: CRUK, Amgen Inc (N = 1,196) BRAF status available (n = 787) BRAF status available (n = 1,946) KRAS MT BRAF available (n = 477) KRAS WT BRAF available (n = 591) Trial arm(s) included in RR, PFS, P-PS, and OS analysis Trial arm(s) included in RR and OS analysis Trial arm(s) excluded from all analysis Strategy B: 5-FU; IrFU or OxFU on prog (n = 371) Strategy C: IrFU or OxFU until prog (n = 357) Arm A Cont. OxFp (n = 632) Ir (n = 189) IrCs (n = 288) IrPan (n = 321) Ir (n = 270) Cmab, cetuximab; Cs, cyclosporine; Fp, fluoropyrimidine; FU, fluorouracil; Ir, irinotecan; Ox, oxaliplatin; Pan, panitumumab; P-PS, post-progression survival; RCT, randomised controlled trial. Seligmann")
15
15 BRAF MT patients have a significantly shorter median OS in first line; although nonsignificant, a similar trend is observed in second line BRAF MT patients had a lower probability of receiving second-line CT Exploring Outcomes of BRAF MT Advanced CRC Patients: OS in First-Line and Second-Line Treatment First-Line Treatment OS for BRAF MT vs BRAF WT OS Estimate Time (months) No. at risk: 1880 191 1610 147 1217 82 765 38 413 16 197 7 93 3 33 1 06121824303642 0 0.25 0.50 0.75 1.00 BRAF WT BRAF MT HR = 1.48 P<.001 10.8 16.4 OS Estimate Time (months) No. at risk: 419 40 036912151824 0 0.25 0.50 0.75 1.00 BRAF WT BRAF MT HR = 1.17 P =.33 21 372 33 302 22 241 17 172 16 132 13 103 12 54 5 74 8 6.910.2 Second-Line Treatment OS for BRAF MT vs BRAF WT Seligmann. 2015.
 No. at risk: BRAF WT BRAF MT HR = 1.17 P = Second-Line Treatment OS for BRAF MT vs BRAF WT Seligmann")
16
16 Exploratory cohort September 2008–May 2010 BREAC: Impact of BRAF Mutational Status on Outcome in Patients Treated with Anti-EGFR mAb Multicentre, retrospective study to investigate novel biomarkers of anti- EGFR mAb therapy in mCRC patients PFS, OS, and response rate were evaluated according to expanded RAS and BRAF mutational status Inference cohort June 2010–June 2012 Super-responder (CR, PR, long SD) Nonresponder (PD at first evaluation) Patients with KRAS exon 2 WT or unknown mutation status mCRC with fluoropyrimidine, irinotecan, and oxaliplatin failure Further samples collected and candidate target genes sequenced Yuki. 2015. Anti-EGFR mAb (N = 184)
.")
17
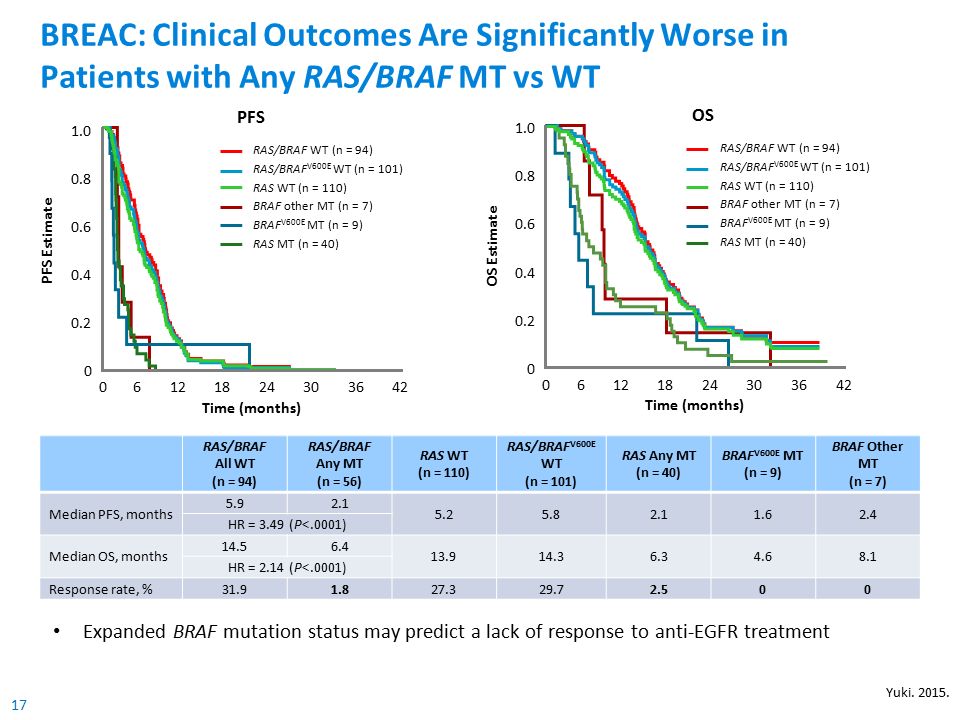
17 BREAC: Clinical Outcomes Are Significantly Worse in Patients with Any RAS/BRAF MT vs WT RAS/BRAF All WT (n = 94) RAS/BRAF Any MT (n = 56) RAS WT (n = 110) RAS/BRAF V600E WT (n = 101) RAS Any MT (n = 40) BRAF V600E MT (n = 9) BRAF Other MT (n = 7) Median PFS, months 5.92.1 5.25.82.11.62.4 HR = 3.49 (P<.0001) Median OS, months 14.56.4 13.914.36.34.68.1 HR = 2.14 (P<.0001) Response rate, %31.91.827.329.72.500 PFS 06121842 PFS Estimate Time (months) 24 1.0 0.8 0.6 0.4 0.2 0 3630 RAS/BRAF WT (n = 94) RAS/BRAF V600E WT (n = 101) RAS WT (n = 110) BRAF other MT (n = 7) BRAF V600E MT (n = 9) RAS MT (n = 40) OS 012182442 Time (months) OS Estimate 30366 1.0 0.8 0.6 0.4 0.2 0 RAS/BRAF WT (n = 94) RAS/BRAF V600E WT (n = 101) RAS WT (n = 110) BRAF other MT (n = 7) BRAF V600E MT (n = 9) RAS MT (n = 40) Expanded BRAF mutation status may predict a lack of response to anti-EGFR treatment Yuki. 2015.
18
18 High BRAF Mutation Frequency in a Scandinavian Population-Based mCRC Cohort 1,2 Prospective, unselected population of unresectable mCRC patients (N = 798) –Tissue microarray for mutational analysis was possible in 446 cases (56%) 1,2. Sorbye. 2015. BRAF MT (21%) BRAF WT/ KRAS MT (40%) BRAF WT/ KRAS WT (39%) Unknown* (<1%) BRAF and KRAS Mutation Status (n = 446) 1,2 OS in Patients Receiving Chemotherapy OS Estimate 605448423630 Time (months) 24181260 KRAS/BRAF WT KRAS MT BRAF MT P<.001 0.0 0.2 0.4 0.6 0.8 1.0 121821 The observed 21% BRAF mutation incidence is higher than the previously reported incidence of 5%–12% in mCRC 2 BRAF MT patients had a significantly poor prognosis compared with KRAS/BRAF WT patients *BRAF status unknown.
 BRAF WT/ KRAS MT (40%) BRAF WT/ KRAS WT (39%) Unknown* (<1%) BRAF and KRAS Mutation Status (n = 446) 1,2 OS in Patients Receiving Chemotherapy OS Estimate Time (months) KRAS/BRAF WT KRAS MT BRAF MT P< The observed 21% BRAF mutation incidence is higher than the previously reported incidence of 5%–12% in mCRC 2 BRAF MT patients had a significantly poor prognosis compared with KRAS/BRAF WT patients *BRAF status unknown..")
19
19 However... Not All BRAF Mutations Are Created Equal: BRAF 594 and BRAF 596 BRAF 594 and BRAF 596 mutations occur in <1% of CRCs Cremolini. 2015. NMedian OSHR for death BRAF 594/596 vs BRAF V600E 1062.0 mos0.36 (0.20–0.64) P =.002 BRAF 594/596 vs BRAF WT54035.9 mos0.55 (0.29–1.05) P =.081 BRAF V600E vs BRAF WT7712.6 mos5.70 (3.74–8.69) P<.001 BRAF 594 or BRAF 596 MT mCRC differs from BRAF V600E MT mCRC in terms of clinical outcome, consistent with preclinical evidence of a kinase-inactivating effect of these mutations The role of CRAF in intracellular signal transduction warrants further preclinical investigation Log-rank test, p<.001 Months 7550100125150175250 0 50 75 100 Overall Survival, %
 P =.002 BRAF 594/596 vs BRAF WT mos0.55 (0.29–1.05) P =.081 BRAF V600E vs BRAF WT mos5.70 (3.74–8.69) P<.001 BRAF 594 or BRAF 596 MT mCRC differs from BRAF V600E MT mCRC in terms of clinical outcome, consistent with preclinical evidence of a kinase-inactivating effect of these mutations The role of CRAF in intracellular signal transduction warrants further preclinical investigation Log-rank test, p<.001 Months Overall Survival, %.")
20
20 ESMO and NCCN Recommendations for the Treatment of BRAF MT Patients 1. Van Cutsem. 2014; 2. NCCN Guidelines. 2015. ESMO says 1 “Evidence is accumulating that patients with a BRAF mutant tumor do not benefit from anti-EGFR antibodies alone or in combination with cytotoxics” “It may be beneficial to use more intensive regimens, eg FOLFOXIRI/ bev to obtain a maximal benefit in this poor prognosis group” NCCN says 2 “Patients with a V600E BRAF mutation appear to have a poorer prognosis. There are insufficient data to guide the use of anti-EGFR therapy in the first- line setting with active chemotherapy based on BRAF V600E mutation status. Limited available data suggest lack of antitumor activity from anti- EGFR monoclonal antibodies in the presence of a V600E mutation when used after a patient has progressed on first-line therapy.”

21
21 Treatment Choice: Molecular Testing Based on RAS/BRAF Mutation Status PD, progressive disease; VEGF inhibitor, bevacizumab or aflibercept. Adapted from Sridharan. 2014. Any RAS mutation (55%) All RAS wildtype (40%) BRAF mutation (5%) Metastatic colorectal cancer with unresectable metastases PD1 PD2 PD3 PD4 Bevacizumab + CT doublet Bevacizumab + FOLFOXIRI Bevacizumab + CT doublet EGFR inhibitor + CT doublet EGFR inhibitor ± CT EGFR inhibitor ± irinotecan VEGF inhibitor + CT doublet Regorafenib Consideration of reintroduction of antitumour therapy, clinical trial, or BSC Molecular biomarker testing
 All RAS wildtype (40%) BRAF mutation (5%) Metastatic colorectal cancer with unresectable metastases PD1 PD2 PD3 PD4 Bevacizumab + CT doublet Bevacizumab + FOLFOXIRI Bevacizumab + CT doublet EGFR inhibitor + CT doublet EGFR inhibitor ± CT EGFR inhibitor ± irinotecan VEGF inhibitor + CT doublet Regorafenib Consideration of reintroduction of antitumour therapy, clinical trial, or BSC Molecular biomarker testing.")
22
22 BRAF Mutation Confers a Poor Prognosis in mCRC Irrespective of Biologic Treatment Evaluated First-Line StudyBiologic All WTBRAF MT OS months (n) OS months (n) COIN 1 Cetuximab 20.1 (n = 581) 8.8 (n = 102) OPUS/CRYSTAL 2 Cetuximab 23.0 # (n = 730) 12.0 # (n = 70) PRIME 3 Panitumumab 24.6 # (n = 446) 9.9 # (n = 53) 20050181 4 (2nd Line) Panitumumab 17.1 # (n = 376) 5.2 # (n = 45) AGITG MAX 5 Bevacizumab 20.8 (n = 280*) 8.6 (n = 33) TRIBE 6,7 Bevacizumab 37.6 # (n = 93 ǂ ) 14.9 # (n = 28) FIRE-3 8,9 Cetuximab 33.1 (n = 199) 12.3 (n = 23) Bevacizumab 25.0 (n = 201) 13.7 (n = 25) *BRAF WT only; ǂ RAS and BRAF WT. # Mean OS calculated from all treatment groups. 1. Maughan. 2011; 2. Bokemeyer. 2012; 3. Douillard. 2013; 4. Peeters. 2014; 5. Price. 2011; 6. Cremolini. 2014; 7. Loupakis. 2015; 8. Stintzing. 2014; 9. Stintzing. 2015.

23
23 BRAF Mutations Do Not Appear to Predict for Lack of Benefit with EGFR mAbs or Bevacizumab *Second-line study. a Chemotherapy is oxaliplatin-based or irinotecan-based, not a combination of both. 1. Bokemeyer. 2012; 2. Peeters. 2014; 3. Douillard. 2013; 4. Price. 2011. OPUS/CRYSTAL 1 BRAF MT subset Chemotherapy a (n = 38) Chemotherapy + Cetuximab (n = 32) P Value OS months9.914.1.08 PFS months3.77.1.23 20050181 2 * BRAF MT subset Chemotherapy a (n = 23) Chemotherapy + Panitumumab (n = 22) P Value OS months5.74.7.20 PFS months1.82.5.34 PRIME 3 BRAF MT subset Chemotherapy a (n = 29) Chemotherapy + Panitumumab (n = 24) P Value OS months9.210.5.76 PFS months5.46.1.12 AGITG MAX 4 BRAF MT subset (n = 33) Chemotherapy a Chemotherapy + BevacizumabP Value OS months6.39.2.34 PFS months2.55.5.71 Cetuximab Panitumumab Bevacizumab
 Chemotherapy + Cetuximab (n = 32) P Value OS months PFS months * BRAF MT subset Chemotherapy a (n = 23) Chemotherapy + Panitumumab (n = 22) P Value OS months PFS months PRIME 3 BRAF MT subset Chemotherapy a (n = 29) Chemotherapy + Panitumumab (n = 24) P Value OS months PFS months AGITG MAX 4 BRAF MT subset (n = 33) Chemotherapy a Chemotherapy + BevacizumabP Value OS months PFS months Cetuximab Panitumumab Bevacizumab.")
24
24 In RAS & BRAF WT mCRC, Intensive Therapy with FOLFOXIRI + Either EGFR Inhibitors or Bevacizumab Results in High ORR TRIP Study 1 BRAF WT (n = 37) TRIP + MACBETH Study 2 BRAF WT (n = 37 + 64) TRIBE 2 BRAF WT (n = 62) FOLFOXIRI + Panitumumab FOLFOXIRI + Anti-EGFR FOLFOXIRI + Bevacizumab CR04%3% PR86.5%78%71% SD10.8%13%27% PD2.7%5%2% Overall response rate*86%82%71% *P =.120, Fisher’s exact test. CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; Pani, panitumumab; Bev, bevacizumab. 1. Lonardi. 2012; 2. Salvatore. 2014.

25
25 Intensive Therapy with FOLFOXIRI + Bevacizumab May Partially Offset the Negative Prognosis of BRAF MT mCRC 1. Cremolini. 2014; 2. Loupakis. 2015. Phase III trial of first-line FOLFOXIRI + bevacizumab vs FOLFIRI + bevacizumab The benefit of FOLFOXIRI + bevacizumab is independent of BRAF or RAS mutation status FOLFOXIRI + bevacizumab may provide the longest OS opportunity for BRAF MT mCRC FOLFIRI + Bevacizumab HR = 0.77 n = 508 HR = 0.78 n = 236 HR = 0.57 n = 28 HR = 0.80 n = 508 HR = 0.88 n = 236 HR = 0.54 n = 28 FOLFOXIRI + Bevacizumab

26
26 BRAF MT Population AGITG MAX 1 Phase III Cape +/– Bev* FIRE-3 Phase III 2 FOLFIRI + Cetux or Bev TRIBE Phase III 3,4 FOLFIRI or FOLFOXIRI + Bev Phase II Single-Arm Experience 5,6 FOLFOXIRI + Bev Sample size n = 33n = 23n = 25n = 28 Phase II n = 10 Phase II n = 15 Pooled n = 25 CapeCape/Bev FOLFIRI Cetux FOLFIRI Bev FOLFIRI Bev FOLFOXIRI Bev FOLFOXIRI Bev OS months6.39.212.313.710.719.023.824.1 PFS months2.55.54.96.05.57.512.89.211.8 Overall response rate 25%42.9%52.2%40%--90%60%72% FOLFOXIRI + Bevacizumab Singlet or Doublet + Biologic Body of Evidence with FOLFOXIRI + Bevacizumab in BRAF MT mCRC Suggests Improved Outcomes with Intensive Therapy *Includes patients receiving capecitabine + bevacizumab +/– mitomycin. 1. Price. 2011; 2. Stintzing. 2014; 3. Cremolini. 2014; 4. Loupakis. 2015; 5. Masi. 2010; 6. Loupakis. 2014.

27
27 MAPK Pathway Suppression via BRAF Inhibition in BRAF MT CRC Models Shows Antiproliferative & Antitumour Activity The BRAF V600E mutant kinase constitutively activates the mitogen-activated cascade of the mitogen-activated protein kinase (MAPK) pathway, resulting in deregulation of MAPK target genes and oncogenic cellular behaviours –Pleiotropic functions, resistance to apoptosis, genetic instability, senescence and independence from extracellular growth signals 1 1. Hirschi. 2014; 2. Yang. 2011. Preclinical BRAF V600E-expressing CRC xenograft model (HT29) demonstrates antiproliferative and antitumour activity of vemurafenib, suggesting that BRAF V600E is a viable therapeutic target in CRC 2 0 200 400 600 800 1,000 1,200 1,400 1,600 1,800 2,000 1214161820 Days Post Tumor Cell Implant 222426283032 Mean Tumor Volume (mm 3 ) ± SEI HT29: BRAF V600E % TGIPRCR% ILS Vehicle b.i.d. Vemurafenib 25 mg/kg b.i.d.710045 Vemurafenib 50 mg/kg b.i.d.830071 Vemurafenib 75 mg/kg b.i.d. 951090 Vemurafenib 100 mg/kg b.i.d.985090
 demonstrates antiproliferative and antitumour activity of vemurafenib, suggesting that BRAF V600E is a viable therapeutic target in CRC ,000 1,200 1,400 1,600 1,800 2, Days Post Tumor Cell Implant Mean Tumor Volume (mm 3 ) ± SEI HT29: BRAF V600E % TGIPRCR% ILS Vehicle b.i.d. Vemurafenib 25 mg/kg b.i.d Vemurafenib 50 mg/kg b.i.d Vemurafenib 75 mg/kg b.i.d Vemurafenib 100 mg/kg b.i.d")
28
28 -100 Single-Agent Vemurafenib in BRAF MT Patients Has Not Been as Promising as in BRAF MT Melanoma Patients 1,2 PR, partial response; MR, minor response (≥10% shrinkage); CR, complete response. 1. Flaherty. 2010; 2. Kopetz. 2010. Antitumour Response in Metastatic Melanoma 81% response rate 1 n = 32 Evaluable Patients Antitumour Response in mCRC ~5% response rate 2 24 PR and 2 CR 125 100 75 50 25 0 -25 -50 -75 Threshhold for response according to RECIST % Change from Baseline Best Overall Response Melanoma stage M1a Melanoma stage M1b Melanoma stage 1c 100 75 50 25 0 -25 -50 -75 -100 % Change from Baseline (Sum of Lesion Size) n = 19 Evaluable Patients (RECIST cutoff for PR, 30%) 1 PR and 4 MRs (≥10% shrinkage) Interim – 12/31/09
 n = 19 Evaluable Patients (RECIST cutoff for PR, 30%) 1 PR and 4 MRs (≥10% shrinkage) Interim – 12/31/09.")
29
29 The Addition of a MEK Inhibitor to a BRAF Inhibitor Modestly Increases Antitumour Activity in BRAF MT mCRC 1. Corcoran. 2014. Dabrafenib + Trametinib in BRAF MT mCRC (n = 43) Waterfall Plot of Investigator-Assessed Best Response Preclinical data suggest improved MAPK pathway suppression with combined inhibition of BRAF and MEK may improve efficacy 12% Response Rate
 Waterfall Plot of Investigator-Assessed Best Response Preclinical data suggest improved MAPK pathway suppression with combined inhibition of BRAF and MEK may improve efficacy 12% Response Rate.")
30
30 Preclinical Models Favour the Use of EGFR Inhibitors Plus BRAF Inhibitors in BRAF MT Patients Low response rates of BRAF mutant mCRC tumours to the BRAF inhibitor, vemurafenib, may be explained by the rapid EGFR-mediated reactivation of the MAPK pathway 1, 2 Preclinical models in vitro and in vivo have demonstrated that blockade of EGFR receptor with cetuximab is strongly synergistic with BRAF inhibition 2 1. Corcoran. 2012; 2. Prahallad. 2012.

31
31 Ongoing Clinical Trials are Assessing the Efficacy of BRAF and EGFR Inhibitors in BRAF MT Patients NCT 01524978 Phase II (BASKET): BRAF/EGFR (Roche) 1 –BRAFi vemurafenib +/- cetuximab NCT 01791309 pilot study: BRAF/EFGR (Genentech/Roche) 2 –Vemurafenib + panitumumab NCT 01719380 Phase I: BRAF/EGFR/PI3K (Novartis) 3 –BRAFi encorafenib + cetuximab +/- PI3Ki BLY719 NCT 01750918 Phase I/II: BRAF/EGFR/MEK (GSK) 4 –BRAFi dabrafenib + panitumumab +/- MEKi trametinib –MEKi trametinib + panitumumab BRAFi, BRAF inhibitor; MEKi, MEK inhibitor. 1. Tabernero. 2014; 2. Yaeger. 2015; 3. Van Geel. 2014; 4. Bendell. 2014.

32
32 Vemurafenib + Cetux 1 (n = 21)* # Vemurafenib + Pani 2 (n = 12) Encorafenib + Cetux +/- BLY719 3 (n = 51) Dabrafenib + Pani +/- Trametinib 4† (n = 30) Encorafenib + Cetux (n = 26) Encorafenib + Cetux + BLY719 (n = 25) Dabrafenib + Pani (n = 15) Dabrafenib + Pani + Trametinib (n = 15) CR000006.7% PR013%29.2%30%13.3%33.3% SD19%53%50%60%73.3%40% PD33%13%12.5%0%13.3%20% *Dose level 3 in study; 960 mg VEM. # Preliminary data; †Preliminary data best unconfirmed response in response-evaluable patients. Cetux, cetuximab; Pani, panitumumab. CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease. 1. Tabernero. 2014; 2. Yaeger. 2015; 3. Van Geel. 2014; 4. Bendell. 2014. Preliminary Evidence of Stable Disease is Promising in BRAF + EGFR (+/- MEK) Inhibitor Combinations, Suggests Additional Research may be Warranted
 Inhibitor Combinations, Suggests Additional Research may be Warranted.")
33
33 To Date, Activity of BRAF-Targeted Approach Alone or in Combination Is Modest Relative to FOLFOXIRI + Bevacizumab FOLFOXIRI + Bevacizumab ORR = 60%–90% PFS = 7.5 – 12.8 months OS = 19.1 – 24.1 months BRAF +/– MEK and/or EGFR ORR = 5%–40% BRAF MT mCRC First Line Various Lines

34
34 Benefit of bevacizumab maintained irrespective of RAS, BRAF, PIK3CA mutational status, or PTEN loss Prognostic Predictive* Anti-EGFR mAbsBevacizumab RAS No – Maybe YesNo BRAFYes NoMaybe No – MaybeNo PIK3CANo Yes Maybe Yes – MaybeNo PTENNoYesNo *Of resistance or lack of response Beyond RAS – Summary

35
35 Beyond RAS: Future Biomarkers of Relevance for Treatment Selection? 1. Sorich. 2014; 2. De Roock. 2010; 3. Sartore-Binachi. 2009. RAS/ BRAF MT Approximately 7% have BRAF mutations 1 11% have other RAS mutations (KRAS exon 3 and 4, and NRAS mutations) 1 RAS/ BRAF WT Approximately 4.5% have PIK3CA mutations 2,3 Approximately 15% have PTEN loss 2,3 RAS/ BRAF/ PIK3CA/ PTEN WT Appropriate candidates for anti-EGFR mAbs?
 1 RAS/ BRAF WT Approximately 4.5% have PIK3CA mutations 2,3 Approximately 15% have PTEN loss 2,3 RAS/ BRAF/ PIK3CA/ PTEN WT Appropriate candidates for anti-EGFR mAbs .")
36
36 BRAF mutation has strong negative prognostic value –Treatment with FOLFOXIRI + bevacizumab may provide optimal outcomes in this aggressive disease subset PIK3CA mutations and PTEN loss may confer resistance to anti-EGFR mAbs Bevacizumab benefit appears retained in the presence of RAS, BRAF, PI3K and PTEN mutations BRAF PIK3CA Beyond RAS: BRAF, PIK3CA, and PTEN Mutations PTEN

37
37 Treatment Choice: More than Efficacy Treatment decisions should take into account patient preference, and patient and tumour characteristics 1L treatment Expectations Toxicity profile Flexibility Socioeconomic factors Quality of life Expectations Toxicity profile Flexibility Socioeconomic factors Quality of life Age Performance status Prior adjuvant treatment Comorbidities Age Performance status Prior adjuvant treatment Comorbidities Tumour characteristics Patient preference Patient characteristics Clinical presentation Tumour biology RAS mutation status BRAF mutation status Clinical presentation Tumour biology RAS mutation status BRAF mutation status

38
38 1L treatment Tumour characteristics Clinical presentation Tumour biology RAS mutation status BRAF mutation status Clinical presentation Tumour biology RAS mutation status BRAF mutation status Molecular biomarker testing is of utmost importance to treatment choice Patient preference Patient characteristics Treatment Choice: The Role of Molecular Testing

39
39 Treatment Choice: Molecular Testing Based on RAS/BRAF Mutation Status PD, progressive disease; VEGF inhibitor, bevacizumab or aflibercept. Adapted from Sridharan. 2014. Any RAS mutation (55%) All RAS wildtype (40%) BRAF mutation (5%) Metastatic colorectal cancer with unresectable metastases PD1 PD2 PD3 PD4 Bevacizumab + CT doublet Bevacizumab + FOLFOXIRI Bevacizumab + CT doublet EGFR inhibitor + CT doublet EGFR inhibitor ± CT EGFR inhibitor ± irinotecan VEGF inhibitor + CT doublet Regorafenib Consideration of reintroduction of antitumour therapy, clinical trial, or BSC Molecular biomarker testing
 All RAS wildtype (40%) BRAF mutation (5%) Metastatic colorectal cancer with unresectable metastases PD1 PD2 PD3 PD4 Bevacizumab + CT doublet Bevacizumab + FOLFOXIRI Bevacizumab + CT doublet EGFR inhibitor + CT doublet EGFR inhibitor ± CT EGFR inhibitor ± irinotecan VEGF inhibitor + CT doublet Regorafenib Consideration of reintroduction of antitumour therapy, clinical trial, or BSC Molecular biomarker testing.")
40
40 Treatment Algorithm for the Practical Medical Management of mCRC Based on Extended Molecular Testing Adapted from Sridharan. 2014. Any RAS mutation (55%) All RAS wildtype (40%) BRAF mutation (5%) Metastatic colorectal cancer with unresectable metastases PD1 PD2 PD3 PD4 Bevacizumab + CT doublet Bevacizumab + FOLFOXIRI Bevacizumab + CT doublet EGFR inhibitor + CT doublet EGFR inhibitor ± CT EGFR inhibitor ± Irinotecan VEGF inhibitor + CT doublet Regorafenib Consideration of reintroduction of antitumour therapy, clinical trial, or BSC Molecular biomarker testing Bevacizumab is the only biologic than can be used front line in all mCRC patient populations independent of mutational status
 All RAS wildtype (40%) BRAF mutation (5%) Metastatic colorectal cancer with unresectable metastases PD1 PD2 PD3 PD4 Bevacizumab + CT doublet Bevacizumab + FOLFOXIRI Bevacizumab + CT doublet EGFR inhibitor + CT doublet EGFR inhibitor ± CT EGFR inhibitor ± Irinotecan VEGF inhibitor + CT doublet Regorafenib Consideration of reintroduction of antitumour therapy, clinical trial, or BSC Molecular biomarker testing Bevacizumab is the only biologic than can be used front line in all mCRC patient populations independent of mutational status.")
Παρόμοιες παρουσιάσεις








, Performance Indicators (PIs), Key Performance Indicators (KPIs)>")










