Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Σχόλια – Παραδείγματα & NS πόσο NS ?
Ετήσιο Μετεκπαιδευτικό Σεμινάριο Υγρών-Ηλεκτρολυτών & Οξεοβασικής Ισορροπίας 8ο Σεμινάριο: Διαταραχές Ύδατος και νατρίου Ξενοδοχείο «Αρκαδία», Κομοτηνή 26 & 27 Σεπτεμβρίου 2014 Στρογγυλό Τραπέζι VΙ Διαταραχές ισοζυγίου του ύδατος και νατρίου στη ΜΕΘ Προεδρείο: Ν. Ζουμπαρίδης- Σ. Παναγούτσος Σάββατο, 27 Σεπτεμβρίου :30 -21:15 Καθηγητής Γεώργιος Ι. Μπαλτόπουλος Διευθυντής ΠανΜΕΘ Γενικού & Ογκολογικού Νοσοκομείου «Οι Άγιοι Ανάργυροι»

2
Δήλωση συμφερόντων για τα τελευταία 4 χρόνια (Conflict of Interest)
Υποστήριξη έρευνας /2ετία BIOTEST AG-Germany, Astellas Για υπηρεσίες συμβούλου (advisory board meetings ) 1/2ετία Astellas, Pfizer Honoraria για διαλέξεις /έτος Novartis, BIOTEST AG, Roche Diagnostics, Astellas, Pfizer
 1/2ετία. Astellas, Pfizer. Honoraria για διαλέξεις 1.5/έτος. Novartis, BIOTEST AG, Roche Diagnostics, Astellas, Pfizer.")
3
Οι τέσσαρες περίοδοι της ζωής και τα υγρά που καταναλώνουμε
Na+ ???? mEq/L Na+ 70 mEq/L 10mEq/L in 1Wk Na+ 2.3 mEq/L Na+ 10 mEq/L Na+ 0.0 mEq/L Na+ 1 mEq/L

4
ΕΡΩΤΗΣΗ 1 Πόσα υγρά θα προσλάβει ένας υγιής ενήλικας σε 177 ημέρες;
Α. 177x2.5L= L Β. 177x3L=531 L Πόσα υγρά θα προσλάβει ένας ασθενής σε 177 ημέρες; Α. 177x3L=531 L Β. 177x3.5L= L Όλα μπορεί να είναι σωστά!!!

5
Κλινική περίπτωση ♀ 80 ετών
Κλινική περίπτωση ♀ 80 ετών Αιτία εισόδου στη ΜΕΘ ΟΑΑ, ΟΝΑ, Σηπτικό shock Ερευνητική λαπαροτομία λόγω οξείας κοιλίας (κοπρανώδης περιτονίτιδα) APACHE II 41 Predicted death rate: 92,2% SAPS II 84 Predicted death rate: 94.6% Ατομικό αναμνηστικό Κακοήθης παχυσαρκία ΑΥ, ΣΝ, Αρθροπλαστική γόνατος (ΑΡ) Έξοδος από την ΜΕΘ: Μετά 177 ημέρες, Βελτιωμένη και σε καλή κατάσταση
 APACHE II 41 Predicted death rate: 92,2% SAPS II 84 Predicted death rate: 94.6% Ατομικό αναμνηστικό. Κακοήθης παχυσαρκία. ΑΥ, ΣΝ, Αρθροπλαστική γόνατος (ΑΡ) Έξοδος από την ΜΕΘ: Μετά 177 ημέρες, Βελτιωμένη και σε καλή κατάσταση.")
6
ΕΡΩΤΗΣΗ 2 Πόσα υγρά πήρε;
531 L L Πήρε: 832 L Έδωσε: 766 L Ισοζύγιο: 66 L Δέρμα 250ml x177= L Κόπρανα 250 ml x 52 = L Πνεύμονας 50 ml x 177= L Σύνολο= L

7
Daily water balance in healthy adults
Total daily water intake: ml Fluids ml Semi-solid and solid food ml Oxidation ml Total daily water output: ml Urine ml Skin ml Lungs ml Stools ml

8
Additional water requirements according to clinical conditions
Temperature elevation by 1 oC ml (0.2 cc/kg/day/1°C) Moderate sweating ml Marked sweating-high fever ml Hyperventilation ml Hyperventilation in dry surrounding ml Exposed wounds surfaces and body cavities ml
 Moderate sweating 500 ml. Marked sweating-high fever ml. Hyperventilation 500 ml. Hyperventilation in dry surrounding ml. Exposed wounds surfaces and body cavities ml.")
9
Medicine is a science of uncertainty and an art of probability Quoted by William B. Bean in Sir William Osler: Aphorisms, Ch. 5

11
Θνητότητα και Na Ασυμφωνία Wald / Chawla & Waikar
Wald και συν: συσχέτιση υποNa+ - θνητότητας → σχήμα U με Na+ ορού 140 mEq/L στη χαμηλότερη θνητότητα. Σε↓Na+ , παρατηρείται↑θνητότητας Chawla και συν, Waikar και συν : παραβολική συσχέτιση Na+ - θνητότητας με ↑ θνητότητα στα όρια mEq/L , ↓θνητότητα σε ηπιότερη ή σοβαρότερη υποNa+ : ασθενείς με σοβαρότερη υποNa+ εισάγονται μάλλον επειδή Na+ είναι τόσο↓,όχι επειδή είναι τόσο βαριά πάσχοντες Multivariable-adjusted log hazard ratios (95% confidence intervals) of all-cause mortality associated with serum sodium levels in a time-dependent Cox model with the use of restricted cubic splines, adjusted for age, gender, race, geographic location, diabetes mellitus, atherosclerotic cardiovascular disease, congestive heart failure, liver disease, malignancy, depression, Charlson comorbidity index, systolic blood pressure, estimated glomerular filtration rate, serum albumin, alkaline phosphatase, aspartate and alanine aminotransferase, total bilirubin, blood hemoglobin, glucose, and white blood cell count. The bars represent the number of deaths in patients with serum sodium levels grouped in increments of 5 mEq/L from 115 to 160 mEq/L, on a logarithmic scale. Kovesdy C P et al. Circulation. 2012;125:
 of all-cause mortality associated with serum sodium levels in a time-dependent Cox model with the use of restricted cubic splines, adjusted for age, gender, race, geographic location, diabetes mellitus, atherosclerotic cardiovascular disease, congestive heart failure, liver disease, malignancy, depression, Charlson comorbidity index, systolic blood pressure, estimated glomerular filtration rate, serum albumin, alkaline phosphatase, aspartate and alanine aminotransferase, total bilirubin, blood hemoglobin, glucose, and white blood cell count. The bars represent the number of deaths in patients with serum sodium levels grouped in increments of 5 mEq/L from 115 to 160 mEq/L, on a logarithmic scale. Kovesdy C P et al. Circulation. 2012;125:")
12
6611.5 ± 13234.45 Μεταβλητές Mean±SD ή Ν(%) Φύλο Άρρεν θήλυ 84 (60,9%)
ΤΟ ΣΥΝΟΛΙΚΟ ΙΣΟΖΥΓΙΟ ΥΓΡΩΝ ΚΑΙ Η ΕΚΒΑΣΗ ΤΩΝ ΒΑΡΕΩΣ ΠΑΣΧΟΝΤΩΝ ΑΣΘΕΝΩΝ ΜΕΘ Θεόδωρος Κατσούλας, Ελένη Μπούτζουκα, Ευδοξία Τσίγκου, Πέτρος Γαλάνης, Ναταλία Κώστα, Γεώργιος Μπαλτόπουλος Πανεπιστημιακή Μονάδα Εντατικής Θεραπείας, ΓΟΝΚ «Άγιοι Ανάργυροι» Μεταβλητές Mean±SD ή Ν(%) Φύλο Άρρεν θήλυ 84 (60,9%) 54 (39,1%) Επιβίωση Επιβίωσαν Απεβίωσαν 112 (81,2%) 26 (18,8%) Είδος εισαγωγής Παθολογικό Χειρουργικό 71 (51,4%) 67 (48,6%) Ηλικία 68,75 ± 13,93 Ημέρες Νοσηλείας 18,46 ± 29,85 APACHE II 18,64 ± 7,23 Υγρά προσλαμβανόμενα total (ml) ± Υγρά αποβαλλόμενα total (ml) ± Ισοζύγιο υγρών (ml) ± ΤΟ ΣΥΝΟΛΙΚΟ ΙΣΟΖΥΓΙΟ ΥΓΡΩΝ ΚΑΙ Η ΕΚΒΑΣΗ ΒΑΡΕΩΣ ΠΑΣΧΟΝΤΩΝ ΑΣΘΕΝΩΝ ΜΕΘ Θεόδωρος Κατσούλας1, Ελένη Μπούτζουκα1, Ευδοξία Τσίγκου1, Πέτρος Γαλάνης2, Ναταλία Κώστα1, Γεώργιος Μπαλτόπουλος1 1 Πανεπιστημιακή Μονάδα Εντατικής Θεραπείας, ΓΟΝΚ «Άγιοι Ανάργυροι» 2 Εργαστήριο Οργάνωσης και Αξιολόγησης Υπηρεσιών Υγείας, Τμήμα Νοσηλευτικής, ΕΚΠΑ Εισαγωγή: η χορήγηση υγρών παραμένει επί δεκαετίες ο θεμέλιος λίθος στην αντιμετώπιση αιμοδυναμικά ασταθών ασθενών στη Μονάδα Εντατικής Θεραπείας (ΜΕΘ). Οι ποσότητες των χορηγούμενων υγρών καθορίζονται σε μεγάλο ποσοστό εμπειρικά, παρά την εξέλιξη στη χρήση δυναμικών δοκιμασιών απόκρισης και στην παρακολούθηση των αιμοδυναμικών παραμέτρων. Η υπερφόρτωση του οργανισμού με υγρά και το αυξημένο συνολικό θετικό ισοζύγιο υγρών έχουν σχετιστεί με αυξημένες επιπλοκές και κακή πρόγνωση των βαριά πασχόντων ασθενών. Σκοπός: η διερεύνηση της επίδρασης του συνολικού ισοζυγίου υγρών στην έκβαση των βαρέως πασχόντων ασθενών. Μέθοδος: έγινε αναδρομική μελέτη των ιατρικών φακέλων όλων των ασθενών που νοσηλεύτηκαν σε γενική ΜΕΘ κατά τη διάρκεια του Καταγράφηκαν τα δημογραφικά και κλινικά χαρακτηριστικά των ασθενών, το σύνολο των προσλαμβανόμενων και αποβαλλόμενων υγρών και υπολογίστηκε το συνολικό ημερήσιο ισοζύγιο υγρών. Αποτελέσματα: νοσηλεύθηκαν συνολικά 138 ασθενείς (60,9% άνδρες, μέση ηλικία 68,75±13,93 έτη). Τα αίτια εισαγωγής ήταν παθολογικά για 71 ασθενείς (51,4%) και χειρουργικά για τους υπόλοιπους 67 (48,6%). Η βαρύτητα της νόσου κατά APACHE II score ήταν 18,64±7,23 η διάρκεια νοσηλείας ήταν 18,46±29,85 ημέρες, ενώ απεβίωσαν 26 ασθενείς (18,8%). Από τη διμεταβλητή ανάλυση με εξαρτημένη μεταβλητή τη θνητότητα προέκυψε ότι τα παθολογικά περιστατικά είχαν υψηλότερη θνητότητα (29,6%) έναντι των χειρουργικών (7,5%) (p=0,001). Επιπλέον, οι αποβιώσαντες είχαν υψηλότερη βαθμολογία βαρύτητας κατά APACHE II score (26,15±5,03 έναντι 16,89±6,52 των επιβιωσάντων, p<0,001) και έλαβαν μεγαλύτερες ποσότητες υγρών (92,81±96,196 lt έναντι 75,13±146,37 των επιβιωσάντων, p=0,002). Το συνολικό ισοζύγιο υγρών ήταν σημαντικά αυξημένο στους ασθενείς που απεβίωσαν (18,2±14,5 lt συγκριτικά με τους ασθενείς που επιβίωσαν 3,68±11,18 lt, p<0,001). Προκειμένου να βρεθούν τα σημεία διαχωρισμού (cut off points) των μεταβλητών της βαρύτητας και του ισοζυγίου υγρών, πέρα από τα οποία αυξήθηκε σημαντικά η επίπτωση θανάτου για τον πληθυσμό της μελέτης, χρησιμοποιήθηκαν οι καμπύλες ROC (Receiver Operating Characteristic curves). Ακολούθως δημιουργήθηκαν οι καμπύλες επιβίωσης με εφαρμογή της μεθόδου Kaplan Meier για κάθε μεταβλητή και για τη σύγκριση μεταξύ των καμπυλών χρησιμοποιήθηκε ο στατιστικός έλεγχος log rank (Εικόνα 1). Στο μοντέλο αναλογικών κινδύνων του Cox, επελέγησαν από τη διμεταβλητή ανάλυση με βάση τη στατιστική τους σημαντικότητα στο επίπεδο του 0,20 (p<0,20), και χρησιμοποιήθηκαν οι μεταβλητές: είδος εισαγωγής, APACHE II και συνολικό ισοζύγιο. Η ανάλυση έδειξε ότι η βαθμολογία APACHE II >24,5, αυξάνει τον κίνδυνο θανάτου κατά 4 φορές (Β=1,403, Exp(B)=4.067, CI 95%= , p=0,003) και το συνολικό θετικό ισοζύγιο υγρών >6,2 lt αυξάνει τον κίνδυνο θανάτου στον πληθυσμό της μελέτης κατά 9 φορές (Β=2,192, Exp(B)=8.954, CI 95%= , p=0.003). Συμπεράσματα: φαίνεται ότι η υπερφόρτωση με υγρά των βαριά πασχόντων ασθενών έχει σημαντική αρνητική προγνωστική αξία για την τελική έκβαση τους, ανεξάρτητα από το είδος εισαγωγής τους. Η στοχευμένη διαχείριση του ενδαγγειακού όγκου, με βάση τις αιμοδυναμικές παραμέτρους, συμβάλλει σημαντικά στη θετική έκβαση των βαρέως πασχόντων ασθενών. Βιβλιογραφία: Garcia X, Gruartmoner G, Mesquida J. Fluid optimization strategies in critical care patients. OA Critical Care 2013; 1:4 Marik PE, Monnet X, Teboul JL. Hemodynamic parameters to guide fluid therapy. Annals Intens Care 2011; 1:1 Bartels K, Thiele RH, Gan TJ. Rational fluid management in todays’ ICU practice. Critical Care 2013; 17(suppl 1):S6 Πίνακας 1. Δημογραφικά και κλινικά χαρακτηριστικά του πληθυσμού της μελέτης (Ν=138)
 Φύλο. Άρρεν. θήλυ. 84 (60,9%) 54 (39,1%) Επιβίωση. Επιβίωσαν. Απεβίωσαν. 112 (81,2%) 26 (18,8%) Είδος εισαγωγής. Παθολογικό. Χειρουργικό. 71 (51,4%) 67 (48,6%) Ηλικία. 68,75 ± 13,93. Ημέρες Νοσηλείας. 18,46 ± 29,85. APACHE II. 18,64 ± 7,23. Υγρά προσλαμβανόμενα total (ml) ± Υγρά αποβαλλόμενα total (ml) ± Ισοζύγιο υγρών (ml) ± ΤΟ ΣΥΝΟΛΙΚΟ ΙΣΟΖΥΓΙΟ ΥΓΡΩΝ ΚΑΙ Η ΕΚΒΑΣΗ ΒΑΡΕΩΣ ΠΑΣΧΟΝΤΩΝ ΑΣΘΕΝΩΝ ΜΕΘ. Θεόδωρος Κατσούλας1, Ελένη Μπούτζουκα1, Ευδοξία Τσίγκου1, Πέτρος Γαλάνης2, Ναταλία Κώστα1, Γεώργιος Μπαλτόπουλος1. 1 Πανεπιστημιακή Μονάδα Εντατικής Θεραπείας, ΓΟΝΚ «Άγιοι Ανάργυροι» 2 Εργαστήριο Οργάνωσης και Αξιολόγησης Υπηρεσιών Υγείας, Τμήμα Νοσηλευτικής, ΕΚΠΑ. Εισαγωγή: η χορήγηση υγρών παραμένει επί δεκαετίες ο θεμέλιος λίθος στην αντιμετώπιση αιμοδυναμικά ασταθών ασθενών στη Μονάδα Εντατικής Θεραπείας (ΜΕΘ). Οι ποσότητες των χορηγούμενων υγρών καθορίζονται σε μεγάλο ποσοστό εμπειρικά, παρά την εξέλιξη στη χρήση δυναμικών δοκιμασιών απόκρισης και στην παρακολούθηση των αιμοδυναμικών παραμέτρων. Η υπερφόρτωση του οργανισμού με υγρά και το αυξημένο συνολικό θετικό ισοζύγιο υγρών έχουν σχετιστεί με αυξημένες επιπλοκές και κακή πρόγνωση των βαριά πασχόντων ασθενών. Σκοπός: η διερεύνηση της επίδρασης του συνολικού ισοζυγίου υγρών στην έκβαση των βαρέως πασχόντων ασθενών. Μέθοδος: έγινε αναδρομική μελέτη των ιατρικών φακέλων όλων των ασθενών που νοσηλεύτηκαν σε γενική ΜΕΘ κατά τη διάρκεια του Καταγράφηκαν τα δημογραφικά και κλινικά χαρακτηριστικά των ασθενών, το σύνολο των προσλαμβανόμενων και αποβαλλόμενων υγρών και υπολογίστηκε το συνολικό ημερήσιο ισοζύγιο υγρών. Αποτελέσματα: νοσηλεύθηκαν συνολικά 138 ασθενείς (60,9% άνδρες, μέση ηλικία 68,75±13,93 έτη). Τα αίτια εισαγωγής ήταν παθολογικά για 71 ασθενείς (51,4%) και χειρουργικά για τους υπόλοιπους 67 (48,6%). Η βαρύτητα της νόσου κατά APACHE II score ήταν 18,64±7,23 η διάρκεια νοσηλείας ήταν 18,46±29,85 ημέρες, ενώ απεβίωσαν 26 ασθενείς (18,8%). Από τη διμεταβλητή ανάλυση με εξαρτημένη μεταβλητή τη θνητότητα προέκυψε ότι τα παθολογικά περιστατικά είχαν υψηλότερη θνητότητα (29,6%) έναντι των χειρουργικών (7,5%) (p=0,001). Επιπλέον, οι αποβιώσαντες είχαν υψηλότερη βαθμολογία βαρύτητας κατά APACHE II score (26,15±5,03 έναντι 16,89±6,52 των επιβιωσάντων, p<0,001) και έλαβαν μεγαλύτερες ποσότητες υγρών (92,81±96,196 lt έναντι 75,13±146,37 των επιβιωσάντων, p=0,002). Το συνολικό ισοζύγιο υγρών ήταν σημαντικά αυξημένο στους ασθενείς που απεβίωσαν (18,2±14,5 lt συγκριτικά με τους ασθενείς που επιβίωσαν 3,68±11,18 lt, p<0,001). Προκειμένου να βρεθούν τα σημεία διαχωρισμού (cut off points) των μεταβλητών της βαρύτητας και του ισοζυγίου υγρών, πέρα από τα οποία αυξήθηκε σημαντικά η επίπτωση θανάτου για τον πληθυσμό της μελέτης, χρησιμοποιήθηκαν οι καμπύλες ROC (Receiver Operating Characteristic curves). Ακολούθως δημιουργήθηκαν οι καμπύλες επιβίωσης με εφαρμογή της μεθόδου Kaplan Meier για κάθε μεταβλητή και για τη σύγκριση μεταξύ των καμπυλών χρησιμοποιήθηκε ο στατιστικός έλεγχος log rank (Εικόνα 1). Στο μοντέλο αναλογικών κινδύνων του Cox, επελέγησαν από τη διμεταβλητή ανάλυση με βάση τη στατιστική τους σημαντικότητα στο επίπεδο του 0,20 (p<0,20), και χρησιμοποιήθηκαν οι μεταβλητές: είδος εισαγωγής, APACHE II και συνολικό ισοζύγιο. Η ανάλυση έδειξε ότι η βαθμολογία APACHE II >24,5, αυξάνει τον κίνδυνο θανάτου κατά 4 φορές (Β=1,403, Exp(B)=4.067, CI 95%= , p=0,003) και το συνολικό θετικό ισοζύγιο υγρών >6,2 lt αυξάνει τον κίνδυνο θανάτου στον πληθυσμό της μελέτης κατά 9 φορές (Β=2,192, Exp(B)=8.954, CI 95%= , p=0.003). Συμπεράσματα: φαίνεται ότι η υπερφόρτωση με υγρά των βαριά πασχόντων ασθενών έχει σημαντική αρνητική προγνωστική αξία για την τελική έκβαση τους, ανεξάρτητα από το είδος εισαγωγής τους. Η στοχευμένη διαχείριση του ενδαγγειακού όγκου, με βάση τις αιμοδυναμικές παραμέτρους, συμβάλλει σημαντικά στη θετική έκβαση των βαρέως πασχόντων ασθενών. Βιβλιογραφία: Garcia X, Gruartmoner G, Mesquida J. Fluid optimization strategies in critical care patients. OA Critical Care 2013; 1:4. Marik PE, Monnet X, Teboul JL. Hemodynamic parameters to guide fluid therapy. Annals Intens Care 2011; 1:1. Bartels K, Thiele RH, Gan TJ. Rational fluid management in todays’ ICU practice. Critical Care 2013; 17(suppl 1):S6. Πίνακας 1. Δημογραφικά και κλινικά χαρακτηριστικά του πληθυσμού της μελέτης (Ν=138)")
13
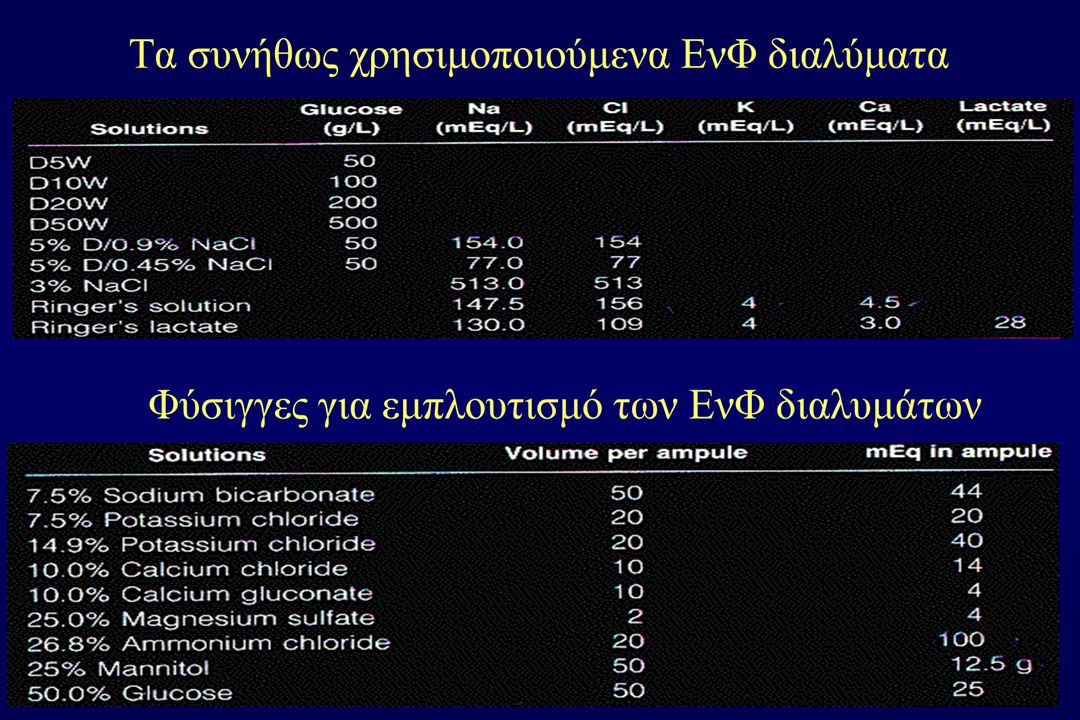
Serum values and daily requirements for of Electrolytes
Cations Concentration, mEq/L Daily Requirements ECF ICF ECF:ICF Sodium mEq/kg/d Potassium (35) mEq/kg/d Calcium <0.0002 mg/d Magnesium mg/d Anions Chloride mEq/kg/d Phosphorus mg/d Water 20% BW 40% BW :2 16% Interstitial 4% Intravascular
 mEq/kg/d. Calcium < mg/d. Magnesium mg/d. Anions. Chloride mEq/kg/d. Phosphorus mg/d. Water 20% BW 40% BW 1:2. 16% Interstitial. 4% Intravascular.")
14
ΑΙΤΙΑ & ΘΕΡΑΠΕΙΑ ΥΠΟΝΑΤΡΙΑΙΜΙΑΣ
Thompson C. Differential diagnosis of hyponatraemia. Best Practice & Research Clinical Endocrinology & Metabolism 2012; 26: S7–S15 JASN 2006; 17:1820–1832 14

15
ΕΡΩΤΗΣΗ 3 Η αιτία της υπονατριαιμίας του ασθενή είναι:
♂ 39 χρόνων προσκομίζεται στο ΤΕΠ λόγω πρόσφατης σύγχυσης, με ιστορικό ψύχωσης και κατανάλωσης νερού > 9L /ημέρα Στο ΤΕΠ: Υπνηλία και δυσκολίες προσφάτου μνήμης. Νa 110 mEq/L. a) SIADH b) Υπονατριαιμία εξ αραιώσεως /πραγματική υπονατριαιμία c) Υπογκαιμία d) Ψευδοϋπονατριαιμία e) Τίποτα από τα πιο πάνω Σωστό: b
 SIADH. b) Υπονατριαιμία εξ αραιώσεως /πραγματική υπονατριαιμία. c) Υπογκαιμία. d) Ψευδοϋπονατριαιμία. e) Τίποτα από τα πιο πάνω. Σωστό: b.")
16
Κλινική Περίπτωση 21 χρονος φοιτητής- Φοιτητική εστία
Στο happy hour της Παρασκευής ήπιε gallons νερού με μια καυτή σάλτσα!! Μετά έγινε συγχυτικός και αντιδρούσε νωθρά στα ερεθίσματα Στις 4 το πρωί ανέπτυξε επιληπτικούς σπασμούς και στις 7 μεταφέρθηκε στο νοσοκομείο

17
Κλινική Περίπτωση Ημέρα 1 στο νοσοκομείο
Κλινική Περίπτωση Ημέρα 1 στο νοσοκομείο Υπόταση/ shock δύσκολα ανταποκρινόμενο στα αγγειοδραστικά Αναπνευστική ανεπάρκεια τύπου Ι, ΜΥΑ. Διεγερτικός ΜΕΘ 100% Ο2, maximum PEEP, Μεγάλες πιέσεις, IV norepinephrine. Βαροτραύμα. Κόρες μη αντιδρώσες, Εγκεφαλικό οίδημα Μανιτόλη Νa+ 126mEq/L, Λευκοκυττάρωση, sOsmol 272, που στις 8h έγινε 263, CPK Λοιπά κ.φ. Πορεία Επιβάρυνση της ΑΑ extra-corporeal oxygenationπνευμοπεριτόναιο 3η ημέρα ηεκτρολύτες κ.φ. 4η ημέρα βελτίωση ΚΝΣ 7η ημέρα weaning 8η ημέρα πτέρυγα 10η ημέρα έξοδος κ.φ. DDAVP

18
ΕΡΩΤΗΣΗ 4 41 χρονος που πέθανε σε ένα πολύ καλό νοσοκομείο
Μετά από το βραδινό του γεύμα ανέπτυξε επιγασταλγία και ναυτία χωρίς να μπορεί να κάνει έμετο. Ήπιε 1/3 ενός μαγειρικού φλυτζανιού μαγειρικό αλάτι διαλυμένο σε νερό για να κάνει έμετο. Πέθανε 3 ημέρες μετά στο νοσοκομείο, όπου τον πήγαν γιατί έκανε και γενικευμένους σπασμούς . Ποια είναι η διάγνωση σας; Α. Οπίσθιο κατώτερο έμφραγμα αρρυθμία χαμηλή παροχή Β. Ρήξη ανευρύσματος κοιλιακής αορτής – υπογκαιμία –χαμηλή παροχή C. Διαβητική κετοξέωση D. Υπερνατριαιμία Ε. Περιτονίτιδα Hypernatremia is a common electrolyte disturbance, most often caused by volume depletion. Hypernatremia due to sodium excess occurs less frequently, and fatal hypernatremia solely from ingestion of table salt is rare. The 41-year-old man who had seizures and hypernatremia after ingestion of a supersaturated salt water solution intended for gargling. He had consumed approximately a third cup of table salt (approximately 70 to 90 g of salt or 1,200 to 1,500 meq of sodium). His initial serum sodium concentration was 209 meq/liter. Moder, K G : Hurley, D L Mayo-Clin-Proc Dec; 65(12):
. His initial serum sodium concentration was 209 meq/liter. Moder, K G : Hurley, D L Mayo-Clin-Proc Dec; 65(12):")
19
Renal losses or water restriction
HYPERNATREMIA Na+ +H2O losses H2O losses or water restriction Na+ addition Low total body sodium Normal total Increased total Renal losses Osmotic diuresis- mannitol,glucose,urea Extrarenal losses Excess sweating,diarrhea Renal losses or water restriction Nephrogenic or central diabetes Insibitus, impaired thirst sensation, unconsciousness or inability to express thirst, unavailability of water, oral trauma or inability to swallow, withholding water for therapeutic reasons Respiratory and dermal insesible losses Primary hyperaldosteronism, Cushing’s syndrome, hypertonic dialysis, rapid or excessive administration of Na+-containing parenteral or enteral solutions,sodium chloride tablets, near-drowning in salt water Iso- or hypertonic urine Urinary Na+ >20 mEq/L Hypertonic urine Urinary Na+ <10 mEq/L Urinary Na+ variable Hypo-,Iso- or hypertonic urine Iso- or hypotonic urine Hypotonic saline Water replacement Diuretics and water replacement NORMONATREMIA Modified from: Berl T et al: Kidney Int. 1976;10:117

20
Θα πιώ όλο το Βόσπορο…….. Σιγά ρε μεγάλε !!!!!! …….Καλά πιες ένα μπουκάλι!!!
If a human were to drink 1 L of sea water, there would be a net water loss of approximately 350 mL. This is why, if you're stranded at sea and severely dehydrated, you should not drink sea water as it will only worsen the situation. On the other hand, whales would show a net gain of 350 mL of pure water after ingesting 1 L of sea water, due to their powerful kidneys.

21
Κατάποση θαλασσινού Η2Ο
Σε ενήλικα, η λήψη 4-6 κουταλιών του γλυκού NaCl μπορεί να είναι θανατηφόρος Σε βρέφος, η χορήγηση ενός κουταλιού του γλυκού NaCl, αυξάνει τη συγκέντρωση του Na+ ορού κατά 70 mEq/L Κατάποση θαλασσινού Η2Ο - περιεκτικότητα Νa+: mEq/L - ωσμωτική πίεση: mOsmol/L

22
Unfortunately….

23
The history of 0.9% saline Clinical Nutrition 2008; 27:179-188
Σε ένα μήνα δημοσιεύτηκε !!! Sherif Awad, Simon P. Allison, Dileep N. Lobo* Division of Gastrointestinal Surgery, Wolfson Digestive Diseases Centre, Nottingham University Hospitals, Queen’s Medical Centre, Nottingham NG7 2UH, UK Received 12 December 2007; received in revised form 7 January 2008; accepted 15 January 2008

24
The aims of this review Ο NS χρησιμοποιείται ευρέως!!
to trace the historical origins of 0.9% saline, how it came to be used so commonly today, and to consider the justification for its continued use. Each year nearly 10 million litres of 0.9% sodium chloride (saline) are infused intravenously in the UK (data from Baxter Healthcare, UK). Από που ιστορικά ξεκίνησε η χρήση του; Υπάρχει μια καλή δικαιολογία για αυτή ;;
 are infused intravenously in the UK (data from Baxter Healthcare, UK). Από που ιστορικά ξεκίνησε η χρήση του; Υπάρχει μια καλή δικαιολογία για αυτή ;;")
25
Search strategy Ψάξανε στο Internet !!!
We performed internet-based searches of the Medline (Ovid, PubMed, Embase) and Science Citation Index databases, historical journals on ScienceDirect and the Google search engine Key words saline, physiological, salt solution, sodium chloride, 0.9%, intravenous, injection, fluid, cholera, resuscitation, parenteral, history, historical and origins in various combinations with the Boolean operators AND, OR and NOT. We also hand searched key journals, medical history textbooks and the reference lists of key articles. Ψάξανε στο Internet !!!
 and. Science Citation Index databases, historical journals on ScienceDirect and the Google search engine. Key words saline, physiological, salt solution, sodium chloride, 0.9%, intravenous, injection, fluid, cholera, resuscitation, parenteral, history, historical and origins in various combinations with the Boolean operators AND, OR and NOT. We also hand searched key journals, medical history textbooks and the reference lists of key articles. Ψάξανε στο Internet !!!")
26
Cholera 19th & 20th Century Pandemics I Ποια από όλες προτιμάτε;
First 1816–1826: The began in Bengal, and then spread across India by The cholera outbreak extended as far as China, Indonesia, Java , Caspian Sea Second 1829–1851: Russia Hungary, and Germany (in 1831); Egypt, London (in 1832) Paris, Quebec, Ontario and New York, Mecca (In 1846)] A two-year outbreak began in England and Wales in Ireland in 1849 Third 1852–1860: Russia, China and Japan in 1854, Chicago 1854, Philippines in 1858 and Korea in In 1859, Bengal Iran, Iraq, Arabia and Russia
; Egypt, London (in 1832) Paris, Quebec, Ontario and New York, Mecca (In 1846)] A two-year outbreak began in England and Wales in Ireland in Third. 1852–1860: Russia, China and Japan in 1854, Chicago 1854, Philippines in 1858 and Korea in In 1859, Bengal Iran, Iraq, Arabia and Russia.")
27
Cholera 19th & 20th Century Pandemics II Ποια από όλες προτιμάτε;
Fourth 1863–1875: Europe and Africa, Mecca , Zanzibar, Russia in 1866, Hungary and Belgium ,Netherlands, Italy Algeria 1892 cholera outbreak in Hamburg, hospital ward Fifth 1881–1896: Russia (1892), Spain, Japan Persia, Egypt, Hamburg Sixth 1899–1923: Russian cities and the Ottoman Empire, Philippines, India. Seventh 1961–1975: began in Indonesia, called El Tor, Bangladesh in 1963, India in 1964, and the Soviet Union in Baku in In 1970, Sağmalcılar district of Istanbul, then an impoverished slum, claiming more than 50 lives; eventually the incident led to the renaming of the district as present-day Bayrampaşa by the authorities who were harshly criticized.
, Spain, Japan Persia, Egypt, Hamburg. Sixth. 1899–1923: Russian cities and the Ottoman Empire, Philippines, India. Seventh. 1961–1975: began in Indonesia, called El Tor, Bangladesh in 1963, India in 1964, and the Soviet Union in Baku in In 1970, Sağmalcılar district of Istanbul, then an impoverished slum, claiming more than 50 lives; eventually the incident led to the renaming of the district as present-day Bayrampaşa by the authorities who were harshly criticized.")
28
Ουδέν καλό αμιγές κακού!!!
The use of saline is believed to have originated during the Second cholera pandemic that swept across Europe and reached England in 1831 Solutions used by Latta, Jennings and other pioneers of that era show little similarity to 0.9% saline

29
Όπου υπάρχουν πολλές θεραπείες κάτι δεν πάει καλά!
Οι Θεραπείες στη 2η Πανδημία Χολέρας και τα 3 Πουλάκια!! Blue (2nd) Cholera pandemic Reached Sunderland (northeast England) in October 1831 First development of intravenous fluid therapy. 76 different and ineffective or damaging treatments were advocated for cholera bloodletting as a means of ‘‘diminishing the venous congestion’’ emesis to rid the body of ‘‘poisons’’ and inhalation of the protoxide of azote (laughing gas, nitrous oxide) to ‘‘remedy the absence of arterialisation’’. Όπου υπάρχουν πολλές θεραπείες κάτι δεν πάει καλά!
 Cholera pandemic. Reached Sunderland (northeast England) in October First development of intravenous fluid therapy. 76 different and ineffective or damaging treatments were advocated for cholera. bloodletting as a means of ‘‘diminishing the venous congestion’’ emesis to rid the body of ‘‘poisons’’ and. inhalation of the protoxide of azote (laughing gas, nitrous oxide) to ‘‘remedy the absence of arterialisation’’. Όπου υπάρχουν πολλές θεραπείες κάτι δεν πάει καλά!")
30
2nd Cholera pandemic Moscow 1830
Hermann, a chemist at the Institute of Artificial Mineral Waters, analysing the blood of cholera patients’ found it to have lost as much as 28% of its fluidity. He concluded that ‘‘the liquids evacuated in cholera ….. form constituent parts of the blood, which is deconstituted by their disappearance . … consequently the thickening of the blood... prevents its circulation’’. He, therefore, argued for treatment to reduce the evacuations responsible for the loss of fluid. Hermann’s colleague, Jachnichen injected 6 oz of water intravenously into a cholera patient, whose pulse returned for a quarter of an hour, although he died two hours Μην αφαιρείτε αίμα. Νερό ΕνΦ κάτι κάνει!!

31
1832 William Stevens:Το χρώμα έχει την αξία του!!
Observed the blood of patients with yellow fever was darker than normal could be restored to its red colour by administering oral solutions of ‘‘non-purgative neutral salts’’. Although reported to have treated cholera patients with his ‘saline plan’ Stevens’ aim was not rehydration, but restoration of the blood to its red colour.

32
William Brooke O’Shaughnessy Lancet on 10th December 1831
Proposed a new method of treating cholera ‘‘by the injection of highly-oxygenated salts into the venous system’’. cholera ….. ‘‘universal stagnation of the venous system, and rapid cessation of the arterialisation of the blood’’. Hypothesised that ‘‘if we could bring certain salts of highly oxygenated constitution fairly into contact with the black blood of cholera, we could certainly restore its arterial properties . I therefore conceived the idea of injecting into the veins such substances . Most capable of restoring it to the arterial qualities’’. Recommended injection into the veins ‘‘of the salts which contain the greatest quantity of oxygen, and possess most powerfully the action of oxidising venous blood ….. the nitrate or chlorate of potash’’. Having trialled his proposal on a dog, with no ill effects, he recommended his method be used ‘‘in the fearful cases in which venesection is found impossible’’. O’Shaughnessy then travelled to Sunderland to study the disease and submitted a preliminary report to the Lancet detailing his experiments on the blood in cholera. His report to the Central Board of Health of London was also later reviewed by the Lancet. Having presented a critical examination of the work of Hermann and Stevens, he reached the following conclusions concerning the aim of treatment: ‘‘1st, to restore the blood to its natural specific gravity 2nd, to restore its deficient saline matters. The first of these can only be effected by absorption, by imbibition, or by the injection of aqueous fluid into the veins. The same remarks, with sufficiently obvious modifications, apply to the second.’’ He recommended injection into the veins of tepid water holding a solution of the normal salts of the blood. The reviewer went on to say of O’Shaughnessy ‘‘his experiments having, we presume, led him to abandon his former ideas respecting the superior efficacy of highly oxygenated salts’’. It was clear, therefore, that by this time O’Shaughnessy had made the intellectual leap from his oxygenation theory to realising the primacy of salt and water replacement. Ο O’Shaughnessy είπε: Αρτηριοποιείστε το αίμα δίνοντας Na2ΝΟ3+ NaCl Έδωσε σε σκύλο το διάλυμα του και όλα ΟΚ Φάση Ι και σε ασθενείς με χολέρα 7 εβδομάδες μετά Φάση ΙΙ Δημοσίευση στο Lancet

33
The evolution of saline solutions Robert Lewins Lancet 26th May 1832
Less than 7 weeks following O’Shaughnessy’s recommendations the first cases of cholera were treated with intravenous saline solutions. Robert Lewins, a physician in Leith, Edinburgh, reported the results of this new treatment to the Central Board of Health in London and published them in the Lancet of 26th May 1832. He describes witnessing this treatment in three of six patients treated by Thomas Latta to whom he ascribes the ‘‘merit of first having recourse to this practice’’. Lewins described the immediate effects of injection as ‘‘restoring the natural current in the veins and arteries, of improving the colour of the blood, and recovering the functions of the lungs’’ as ‘‘the most wonderful and satisfactory effect’’ and recommended repeated injections of large quantities of solution guided by the patient’s pulse and symptoms, thereby showing a remarkably modern understanding of the need for continuous treatment guided by physiological monitoring. The solution used by Latta, according to Lewins, consisted of ‘‘two drachms of muriate, and two scruples of carbonate, of soda, to sixty ounces of water’’, a different composition to that reported by Latta in his detailed letter to the Central Board of Health a week later, in which he outlined his rationale for using salt solutions and the results of treatment. Latta, having read O’Shaughnessy’s analyses, attempted to ‘‘restore the blood to its natural state’’ by administration of oral saline solutions only to find that this aggravated the symptoms of vomiting and purging. Robert Lewins Lancet 26th May 1832: Είδε με τα μάτια του τον Thomas Latta !! Ο Latta το έδωσε από το στόμα και……

34
Latta –Lewins- and Craigie 1832
He ‘‘proceeded to throw the fluid immediately into the circulation’’ and, with ‘‘no precedent to direct’’ him, used ‘‘two to three drachms of muriate of soda and two scruples of the subcarbonate of soda in six pints of water’’. He followed this with a description of the initial four cases treated: an aged female who had ‘‘reached the last moments of her earthly existence’’, a female of 50 and ‘‘very destitute’’ and a ‘‘delicate young female, of strumous habit’’. Three of the four patients died and Latta attributed the deaths to ‘‘deficiency in quantity’’ of saline injected, the presence of organic disease and the ‘‘late application of the remedy’’ Further reports from Lewins and Craigie detailed the treatment of more cholera patients at the Drummond Street Hospital in Edinburgh. Lewins: three of six patients survived Craigie: one of two survived Craigie’s solution: one drachm muriate of soda, ten grains carbonate of soda in two pounds aqua calid and was again different from those described previously. Murphy, Macintosh and Anderson also reported trials of intravenous salt solutions, but without describing their composition. Controversially, Murphy claimed that the idea of making ‘‘an artificial serum ... to throw ... In by the veins’’ had occurred to him three weeks prior to Latta’s seminal publication in the Lancet of 2nd June 1832 and cited two witnesses in testimony. Although the declared aim was to replace the fluid losses of cholera with solutions as close in composition as possible to that of serum, all the early solutions used were hypotonic. However, given that medical chemistry was in its infancy at that time, it is remarkable that these physicians showed such insight into the treatment of this invariably fatal illness. Lewins: Ι. το έδωσε ΡΟ ¾ πέθαναν ΙΙ 3/6 πέθαναν Craigie: ½ πέθαναν Murphy: Προηγήθηκε 3 εβδομάδες του Latta και με 2 μάρτυρες!!!!

35
Composition of salt solutions
The constituents of the solutions were described in traditional chemical terms and apothecary’s measures Final composition of Latta’s (1832) solusion: 134 mmol/l Na , 118 mmol/l Cl and 16 mmol/l HCO3 was closer to the composition of plasma and, therefore, more ‘physiological’ than 0.9% saline. Latta’s solution was not adopted by his contemporaries who made no further reference to it. Indeed, no solution of similarly physiological composition was described until that of Sydney Ringer 50 years later (Table 3). A possible explanation for this may be Latta’s death from pulmonary tuberculosis in 1833. Ο Latta ήξερε τη συνταγή και πέθανε!!!
 solusion: 134 mmol/l Na , 118 mmol/l Cl and 16 mmol/l HCO3 was closer to the composition of plasma and, therefore, more ‘physiological’ than 0.9% saline. Latta’s solution was not adopted by his contemporaries who made no further reference to it. Indeed, no solution of similarly physiological composition was described until that of Sydney Ringer 50 years later (Table 3). A possible explanation for this may be Latta’s death from pulmonary tuberculosis in Ο Latta ήξερε τη συνταγή και πέθανε!!!")
36
Solutions composition I

37
Solutions composition II

39
‘Indifferent’, ‘physiological’ or ‘normal’ saline frog nerve and muscle
Sydney Ringer (1883) led to the development and subsequent modification of Ringer’s solution, the basis of the modern solutions such as Hartmann’s. Ringer set out to ‘‘ascertain the influence each constituent of the blood exercises on the contraction of the ventricle’’ and, having bathed frog heart muscle preparations in solutions of different constituents, found that a 0.75% saline solution ‘‘makes an excellent circulating fluid in experiments with the detached heart’’. He later discovered that the saline solution previously used was made using pipe water supplied by the New River Water Company and not distilled water as intended. On repeating the experiments he found that bathing the heart muscle in saline solution made with distilled water made the ventricle grow ‘‘weaker and weaker’’ leading to cessation of contractility in about 20 min. He concluded that the effects he had previously obtained were ‘‘due to some of the inorganic constituents of the pipe water’’. Alexis Hartmann (1932) added sodium lactate to it with the aim of reducing the acidosis seen in infants suffering from diarrhoea, dehydration and oliguria. Koelliker (1857) had observed that nerve and muscle preserved their irritability and appearance for many hours in solutions of 0.5-1% sodium chloride which he therefore termed ‘ indifferent’ solutions. Nasse later determined the optimal concentration of salt for the preservation of the irritability of tissues was 0.6%. Hermann designated this solution ‘physiological water’. The term ‘physiological salt solution’ appears to have been popularised after observations that transfusions of this solution were capable of saving the lives of animals and humans after profuse haemorrhage. Sydney Ringer (1883): η καρδιά του βατράχου με 0.75%NaCl σε H2O βρύσης ΟΚ Koelliker (1857): νεύρα και μυς σε 0.5-1% NaCl σε Η2Ο ΟΚ indifferent διάλυμα Nasse: 0.6%NaCl σε Η2Ο νεύρα και μυς ΟΚ Ο Hermann αυτό το είπε physiological water
 led to the development and subsequent modification of Ringer’s solution, the basis of the modern solutions such as Hartmann’s. Ringer set out to ‘‘ascertain the influence each constituent of the blood exercises on the contraction of the ventricle’’ and, having bathed frog heart muscle preparations in solutions of different constituents, found that a 0.75% saline solution ‘‘makes an excellent circulating fluid in experiments with the detached heart’’. He later discovered that the saline solution previously used was made using pipe water supplied by the New River Water Company and not distilled water as intended. On repeating the experiments he found that bathing the heart muscle in saline solution made with distilled water made the ventricle grow ‘‘weaker and weaker’’ leading to cessation of contractility in about 20 min. He concluded that the effects he had previously obtained were ‘‘due to some of the inorganic constituents of the pipe water’’. Alexis Hartmann (1932) added sodium lactate to it with the aim of reducing the acidosis seen in infants suffering from diarrhoea, dehydration and oliguria. Koelliker (1857) had observed that nerve and muscle preserved their irritability and appearance for many hours in solutions of 0.5-1% sodium chloride which he therefore termed ‘ indifferent’ solutions. Nasse later determined the optimal concentration of salt for the preservation of the irritability of tissues was 0.6%. Hermann designated this solution ‘physiological water’. The term ‘physiological salt solution’ appears to have been popularised after observations that transfusions of this solution were capable of saving the lives of animals and humans after profuse haemorrhage. Sydney Ringer (1883): η καρδιά του βατράχου με 0.75%NaCl σε H2O βρύσης ΟΚ. Koelliker (1857): νεύρα και μυς σε 0.5-1% NaCl σε Η2Ο ΟΚ indifferent διάλυμα. Nasse: 0.6%NaCl σε Η2Ο νεύρα και μυς ΟΚ Ο Hermann αυτό το είπε physiological water.")
40
‘Indifferent’, ‘physiological’ or ‘normal’ saline
By the late 19th century, with better understanding of the principles of membrane permeability, osmosis and fluid tonicity, it was realized that for the fluid to be ‘indifferent’ it also had to be isotonic with the serum. The 0.6% solution was isotonic with the serum of the frog and was therefore only ‘indifferent’ or ‘physiological’ in this animal. Hamburger later found that a more concentrated solution was needed for isotonicity with mammalian serum. However, as Joseph and Meltzer stated in 1911, ‘‘The consequences of these new conceptions found their way into practice only slowly, and even to this day the subject is frequently handled in a loose fashion’’. The first recorded use of the term ‘normal saline’ appeared in a report published in the Lancet on 29th September 1888. This described a case of ‘scirrhus of the pylorus’ treated at Leeds General Infirmary by Dr. Churton. The patient had suffered over a month of vomiting, with minimal oral intake leading him to become ‘‘moribund ... prostrate and pulseless’’ when ‘‘he was ordered transfusion of ‘normal saline’ solution in order to replace the fluid thus lost’’. The patient was injected with 34 fluid ounces of this fluid, which bore no resemblance to 0.9% saline, with immediate improvement in his condition. Repeated injections resulted in continued improvement. Churton mentions that ‘‘the success of transfusion of the so-called normal saline solution to replace the lost water and salts of the blood was more permanent than in cholera, where there is a poison; or in cases of haemorrhage and anaemia, where blood cells are also wanting …. it is probable that by the intravenous injection of a saline solution, or a mixture of such a solution with blood, strength might be obtained to endure or to rally after an operation (of any kind) from which some exhausted patients could not otherwise recover’’. Spencer first used the term ‘normal salt’ solution in 1892, but failed to describe the composition of this fluid. These authors made no mention of the origins of the terms ‘normal saline’ or ‘normal salt’, but one may speculate that, as the terms were put in quotation marks, they may have been a colloquialism current at the time rather than having any scientific basis. The reassuring terms ‘normal’ and ‘physiological’, now commonly applied to 0.9% saline, while having no scientific validity, may have aided its widespread acceptance in practice, despite the fact that it is neither chemically normal, implying a concentration of 58.5 g NaCl/l, nor physiological, i.e. similar to extracellular fluid. 1901 Jacob Vant Hoff: τονικότητα και ωσμωτικότητατο 0.6%NaCl σε Η2Ο είναι καλό για τον βάτραχο Churton Lancet on 29th September 1888: Ο ασθενής με το έλκος στον πυλωρό και ο normal saline Spencer first used the term ‘normal salt’ solution in 1892: Δεν γνωρίζουμε τι ήθελε να πει ο ποιητής!!
 from which some exhausted patients could not otherwise recover’’. Spencer first used the term ‘normal salt’ solution in 1892, but failed to describe the composition of this fluid. These authors made no mention of the origins of the terms ‘normal saline’ or ‘normal salt’, but one may speculate that, as the terms were put in quotation marks, they may have been a colloquialism current at the time rather than having any scientific basis. The reassuring terms ‘normal’ and ‘physiological’, now commonly applied to 0.9% saline, while having no scientific validity, may have aided its widespread acceptance in practice, despite the fact that it is neither chemically normal, implying a concentration of 58.5 g NaCl/l, nor physiological, i.e. similar to extracellular fluid Jacob Vant Hoff: τονικότητα και ωσμωτικότητατο 0.6%NaCl σε Η2Ο είναι καλό για τον βάτραχο. Churton Lancet on 29th September 1888: Ο ασθενής με το έλκος στον πυλωρό και ο normal saline. Spencer first used the term ‘normal salt’ solution in 1892: Δεν γνωρίζουμε τι ήθελε να πει ο ποιητής!!")
41
Hamburger: forgotten father of 0.9% saline?
None of the intravenous saline solutions described between 1832 and 1895 bear any resemblance to 0.9% saline . The first reference to a solution similar to 0.9% saline appeared in In his article W.S. Lazarus-Barlow cites Hamburger as the main authority for suggesting that a concentration of 0.92% saline was ‘normal’ for mammalian blood. Hartog Jakob Hamburger was a Dutch physiological chemist, appointed lecturer in physiology and pathology at the Utrecht Veterinary School in 1888. Remembered for his ‘phenomenon’ (the chloride shift); his ‘interchange’ (secondary buffering), and his ‘law’ (which states that when blood is rendered acid, albumins and phosphates pass from the red blood corpuscles to the serum and the chlorides pass from the serum to the cells) no mention is made in his obituary of his role in the evolution of saline solutions. In a lecture delivered at the University of London and published in the Lancet of 19th November 1921, Hamburger refers to his own work which ‘‘alas, has of late been too often overlooked’’. He was originally inspired by the work of the botanist Hugo de Vries in 1882 on the force with which plant cells attract water. A year later Hamburger performed experiments on the effect of solutions, with varying concentrations of salt, on the escape of colouring matter from erythrocytes. He found that ‘‘for every salt a concentration could be obtained in which the least resistant blood corpuscles lost their colouring matter’’ and speculated that ‘‘the salt solutions used caused a swelling which a number of the blood corpuscles could not withstand without losing their colouring matter’’. It is accepted that the freezing point of human serum is 0.52 C. Hamburger, after comparing the ‘‘freezing points’’ of serum obtained from animals and human subjects, concluded that ‘‘the blood of the majority of warm-blooded animals, including man, was isotonic with a NaCl solution of 0.9 per cent., and not of 0.6 per cent., as was generally thought . and which had always been called the physiological NaCl solution’’. His theory linking the isotonicity of 0.9% saline to human blood, although credibly backed by his experimental evidence, was not universally accepted. The scientific evidence supporting the use of 0.9% saline in clinical practice seems to be based solely on this in vitro study. It remains a mystery how it came into general use as an intravenous fluid in vivo. Perhaps it was due to the ease, convenience and low cost of mixing common salt with water. Ο Hamburger Lancet 19th/11/1921είπε: στα θηλαστικά η ισοτονικότητα εξασφαλίζεται με NaCl 0.9 %
; his ‘interchange’ (secondary buffering), and his ‘law’ (which states that when blood is rendered acid, albumins and phosphates pass from the red blood corpuscles to the serum and the chlorides pass from the serum to the cells) no mention is made in his obituary of his role in the evolution of saline solutions. In a lecture delivered at the University of London and published in the Lancet of 19th November 1921, Hamburger refers to his own work which ‘‘alas, has of late been too often overlooked’’. He was originally inspired by the work of the botanist Hugo de Vries in 1882 on the force with which plant cells attract water. A year later Hamburger performed experiments on the effect of solutions, with varying concentrations of salt, on the escape of colouring matter from erythrocytes. He found that ‘‘for every salt a concentration could be obtained in which the least resistant blood corpuscles lost their colouring matter’’ and speculated that ‘‘the salt solutions used caused a swelling which a number of the blood corpuscles could not withstand without losing their colouring matter’’. It is accepted that the freezing point of human serum is 0.52 C. Hamburger, after comparing the ‘‘freezing points’’ of serum obtained from animals and human subjects, concluded that ‘‘the blood of the majority of warm-blooded animals, including man, was isotonic with a NaCl solution of 0.9 per cent., and not of 0.6 per cent., as was generally thought . and which had always been called the physiological NaCl solution’’. His theory linking the isotonicity of 0.9% saline to human blood, although credibly backed by his experimental evidence, was not universally accepted. The scientific evidence supporting the use of 0.9% saline in clinical practice seems to be based solely on this in vitro study. It remains a mystery how it came into general use as an intravenous fluid in vivo. Perhaps it was due to the ease, convenience and low cost of mixing common salt with water. Ο Hamburger Lancet 19th/11/1921είπε: στα θηλαστικά η ισοτονικότητα εξασφαλίζεται με NaCl 0.9 %")
42
Acceptance into routine practice and modern day problems: abnormal saline
Fluid therapy with saline solutions, in the form of proctoclysis and hypodermoclysis, became routine in the early 20th century. Evans 1911 stated his intention to ‘‘sound a note of warning against the thoughtless and indiscriminate use of this remedy’’ and to dispel the erroneous belief that the administration of ‘sodium chlorid’ solutions was harmless just because the salt was present in all foodstuffs, in body fluids, and incorrectly thought to be readily excreted by the kidneys. Having highlighted the dangers of salt overload and retention he urged restricting its use to ‘‘those conditions in which either quantitative or qualitative changes in the blood-plasma present logical indications for its application’’ and where ‘‘circulatory or renal contraindications do not exist’’. It would appear, from subsequent literature, that Evans’ plea for caution fell on deaf ears. Hartwell and Hoguet on experimental intestinal obstruction in dogs and its treatment by subcutaneous infusions of ‘normal saline’, laid the foundations for saline therapy in patients with intestinal obstruction. Trout 1913 reported a study of postoperative fluid replacement by proctoclysis in some 2000 patients treated at 232 hospitals, who were allocated to receive either tap water or ‘normal’ saline enemas. Trout study was nonetheless the first scientific study of the management of postoperative fluid balance. Trout calculated that, using normal saline,‘‘we would be forcing into an already weakened patient, in the space of 24 hours, the average amount of salt consumed as a condiment by a normal man in one month’’. He also noted transient albuminuria, using saline, which disappeared 24 h after water was substituted, returning again on further use of saline. Trout concluded ‘‘surgeons have simply drifted into employing salt solution by rectum without giving any serious consideration to what they were doing, and such is our excuse for this paper’’. A decade later Rudolph Matas, regarded as the originator of modern fluid therapy, introduced the concept of ‘the continued intravenous drip’, but also warned of the potential dangers of saline infusions. He referred to work by Roessle who showed organic changes in human heart muscle after saline infusions, by Hoeszli who noted degenerative changes in the heart and kidneys of guinea-pigs 6-7 h after massive saline infusions, and by Thiess who in 1910 pointed out ‘‘that a healthy man needs 17 gm. of salt per day, but receives 27 gm. when given 3 litres of 0.9 per cent. Salt solution . …part of the salt is eliminated by the kidneys, but some is retained in tissues, where it attracts liquids and causes oedema’’. Matas concluded for the above reasons that his preferred solution was 5% glucose rather than saline. Η Πρωκτόκληση και Υποδερμόκληση κάνουν καλό στην απόφραξη του εντέρου σε ανθρώπους και σκύλους (JAMA1912)!!!. Καθώς και σε μετεγχειρητικούς (Surg Gynecol Obstet 1913). Αλλά το πολύ αλάτι μπορεί να σας βλάψει. Δώστε καλύτερα υγρά ΕνΦ (Matas Ann Surg 1924)
!!!. Καθώς και σε μετεγχειρητικούς (Surg Gynecol Obstet 1913). Αλλά το πολύ αλάτι μπορεί να σας βλάψει. Δώστε καλύτερα υγρά ΕνΦ (Matas Ann Surg 1924)")
43
Acceptance into routine practice and modern day problems: abnormal saline
Coller et al studied three groups of postoperative patients 5% dextrose in a ‘‘solution of sodium chloride, in Ringer’s solution or in distilled water’’. Although they used a ‘physiologic solution of sodium chloride’ containing 8.5 g NaCl/l, they again found fluid retention, when saline solutions were given intravenously to sick surgical patients, in contrast to 5% dextrose which was excreted more rapidly. Fluid retention in postoperative patients, receiving crystalloid infusions, is exacerbated by their diminished ability to excrete an excess sodium and water load. This classical feature of the metabolic response to injury is unfortunately sometimes forgotten. That such fluid retention is not innocuous is shown by the work of several authors who have described an increase in postoperative complications and adverse outcomes associated with excess sodium and water administration in the perioperative period. Even healthy volunteers have difficulty with saline. When 2 l infusions administered over 1 h of either 0.9%saline or Hartmann’s solution were compared, at 6 h 56% of the infused saline was retained in contrast to only 30% of the Hartmann’s solution. A marked and sustained hyperchloraemia was also seen following saline infusion. Infusion of large volumes of saline in healthy volunteers have also been shown to produce abdominal discomfort and pain, nausea, drowsiness and decreased mental capacity to perform complex tasks. The persistent hyperchloraemia after saline infusions reflects the lower [Na ]:[Cl] ratio in saline (1:1) than in Hartmann’s solution (1.18:1) or plasma (1.38:1). While infusions of 0.9% saline produce a significant hyperchloraemic acidosis, infusions of Hartmann’s solution do not significantly alter bicarbonate and chloride concentrations or pH. Veech has emphasised that the kidney is slow to excrete an excess chloride load after the infusion of large amounts of saline. Wilcox found in animal studies : hyperchloraemia sustained renal vasoconstriction + a reduction in glomerular filtration rate. Further studies on young adult men have shown that plasma renin activity is suppressed 30 and 60 min after infusion of sodium chloride, but not after infusion of sodium bicarbonate, suggesting that both the renin and blood pressure responses to sodium chloride are dependent on chloride. Coller et al (JAMA) : Μετεγχειρητικά ο φυσιολογικός ορός σε πρήζει!! Το παθαίνουν και οι υγιείς!!!
 than in Hartmann’s solution (1.18:1) or plasma (1.38:1). While infusions of 0.9% saline produce a significant hyperchloraemic acidosis, infusions of Hartmann’s solution do not significantly alter bicarbonate and chloride concentrations or pH. Veech has emphasised that the kidney is slow to excrete an excess chloride load after the infusion of large amounts of saline. Wilcox found in animal studies : hyperchloraemia sustained renal vasoconstriction + a reduction in glomerular filtration rate. Further studies on young adult men have shown that plasma renin activity is suppressed 30 and 60 min after infusion of sodium chloride, but not after infusion of sodium bicarbonate, suggesting that both the renin and blood pressure responses to sodium chloride are dependent on chloride. Coller et al (JAMA) : Μετεγχειρητικά ο φυσιολογικός ορός σε πρήζει!! Το παθαίνουν και οι υγιείς!!!")
44
Έχει υποτιμηθεί η κακή δράση του φυσιολογικού ορού
Acceptance into routine practice and modern day problems: abnormal saline Hyperchloraemic acidosis: reduce gastric blood flow and decrease gastric intramucosal pH in elderly surgical patients In patients undergoing colonic surgery, salt and water overload delayed recovery of gastrointestinal function, increased complications and prolonged hospital stay. Acidosis also impairs cardiac contractility and may decrease the response to inotropes. At the cellular level, salt and water overload can result in cytosolic acidification, membrane hyperpolarisation, inactivation of protein kinases and disruption of phosphorylation, leading to cellular dysfunction. In addition, there is increasing evidence that 0.9% sodium chloride solution has adverse effects on immune cells. It has been suggested that the use of 0.9% sodium chloride may exacerbate injury-related neutrophil activation, thus predisposing the host to infectious complications. Alexis Hartmann, in 1934, suggested that his lactated Ringer’s solution was superior to saline infusions in the treatment of infantile diarrhoea, which may be partly due to the lower chloride concentration. Whilst there is no doubt that saline infusions have saved a number of lives in medical and surgical practice, this could well have been achieved by a balanced crystalloid, with fewer side effects. Evans put this into perspective by commenting that, ‘‘One cannot fail to be impressed with the danger . (of) the utter recklessness with which salt solution is frequently prescribed, particularly in the postoperative period.’’ and going on to state that, ‘‘. the disastrous role played by the salt solution is often lost in light of the serious conditions that call forth its use.’’ Έχει υποτιμηθεί η κακή δράση του φυσιολογικού ορού
 the utter recklessness with which salt solution is frequently prescribed, particularly in the postoperative period.’’ and going on to state that, ‘‘. the disastrous role played by the salt solution is often lost in light of the serious conditions that call forth its use.’’ Έχει υποτιμηθεί η κακή δράση του φυσιολογικού ορού.")
45
0.9% saline No EBM The attempt to find a truly physiological crystalloid preparation for both scientific and clinical work has been going on for 175 years and the results have inevitably been a compromise. In conditions of peripheral circulatory failure or liver disease, there may be increased endogenous lactate production or decreased capacity to metabolise infused lactate. On the other hand, the unphysiological proportion of chloride in 0.9% saline causes other problems as outlined. There seems to be no historical or scientific basis, except for Hamburger’s in vitro studies of red cell lysis, to support the continued use of 0.9% saline in clinical practice save in cases involving large chloride losses, e.g. due to vomiting. It is also extremely doubtful that, if a range of intravenous fluids were being designed today on evidence based principles, 0.9% saline would figure prominently. A fresh look at crystalloid formulae is overdue. In the meantime there is a strong case for using solutions nearer in composition to Ringer’s lactate or Hartmann’s solution rather than 0.9% saline, in most patients requiring more than ml of crystalloid solution per day for resuscitation or replacement. 175 χρόνια δεν αποδείξαμε ότι ο NS είναι η καλύτερη λύση!!! Σήμερα ο NS μάλλον δεν θα έπαιρνε άδεια από τον ΕΟΦ!!! Μας έφαγε το Lancet & άλλα σπουδαία περιοδικά !!!!!!! 9/1888 NS (Churton Lancet ) + 11/ % (Hamburger Lancet) = Ο φυσιολογικός ορός που χρησιμοποιούμαι σήμερα Αν ο άρρωστος σας χρειάζεται > ml κρυσταλλοειδή/ημέρα σκεφτείτε και τα διαλύματα Ringer’s lactate ή το Hartmann’s
 + 11/ % (Hamburger Lancet) = Ο φυσιολογικός ορός που χρησιμοποιούμαι σήμερα. Αν ο άρρωστος σας χρειάζεται > ml κρυσταλλοειδή/ημέρα. σκεφτείτε και τα διαλύματα Ringer’s lactate ή το Hartmann’s.")
46
Συμπεράσματα Ευχαριστώ για την προσοχή σας
Οι εκτροπές του Η2Ο & του Na πρέπει να διορθώνονται γιατί μπορούν να οδηγήσουν σε απώλεια υγείας σε υγιείς και να επιβαρύνουν την νόσο τους σε ασθενείς παρά την μεγάλη αντοχή του ανθρώπου!!! Οι εκτροπές Νa υποδηλώνουν είτε έλλειμμα είτε περίσσεια νατρίου ή νερού Οι εκτροπές των συγκεντρώσεων νατρίου μπορεί να είναι θανατηφόρες Χρειάζεται να αντιμετωπίζονται άμεσα αλλά όχι υπερβολικά!! Προηγείται η αντιμετώπιση της διαταραχής και έπεται η αντιμετώπιση της αιτίας. Συνήθως παρουσιάζονται περιπτώσεις διαταραχών Η2Ο & Na που είχαν καλή έκβαση, σπάνια όμως παρουσιάζονται περιπτώσεις που χάθηκαν που πρέπει να είναι πολλές!!! «Γρηγορείτε» ΛΟΙΠΟΝ Ο Φυσιολογικός Ορός είναι φυσιολογικός μόνο κατά το όνομα!!! Ευχαριστώ για την προσοχή σας

47
Μια πολύ συγκινητική Κινέζικη ιστορία...
朣楢琴执㝧执瑩浻牡楧㩮㔱硰执㝧执獧浻牡楧敬瑦瀰絸朣杢㑳执獧扻捡杫潲湵潣潬㩲昣昸昸㬸慢正牧畯摮椭慭敧敷止瑩札慲楤湥楬敮牡氬晥⁴潴敬瑦戠瑯潴牦浯㡦㡦㡦潴捥捥捥戻捡杫潲湵浩条㩥眭扥楫楬敮牡札慲楤湥潴昣昸昸攣散散戻捡杫潲湵浩条㩥洭穯氭湩慥牧摡敩瑮琨灯㡦㡦㡦捥捥捥㬩慢正牧畯摮椭慭敧獭氭湩慥牧摡敩瑮琨灯㡦㡦㡦捥捥捥㬩慢正牧畯摮椭慭敧楬敮牡札慲楤湥潴昣昸昸攣散散戻捡杫潲湵浩条㩥楬敮牡札慲楤湥潴昣昸昸攣散散汩整㩲牰杯摩䐺䥘慭敧牔湡晳牯楍牣獯景牧摡敩瑮猨慴瑲潃潬卲牴昣昸昸䔬摮潃潬卲牴攣散散㬩潢摲牥硰猠汯摩⌠㙣㙣㙣搻獩汰祡戺潬正潭潢摲牥爭摡畩㩳瀲㭸漭戭牯敤慲楤獵㈺硰敷止瑩戭牯敤慲楤獵㈺硰戻牯敤慲楤獵㈺硰执獧搴摻獩汰祡戺潬正瀻獯瑩潩㩮敲慬楴敶执獧搴筮楤灳慬㩹湩楬敮戭潬正漻敶晲潬 Ειδικά στο σημείο που λέει: 椭慭敧獭 … ΕΚΛΑΨΑ... Για όσους είχαν απορία! ………. η γραμματοσειρά είναι MingLiU

Παρόμοιες παρουσιάσεις






, Performance Indicators (PIs), Key Performance Indicators (KPIs)>")





 ωφελέειν ή μη βλάπτειν ωφελέειν = θεραπευτική παρέμβαση μη βλάπτειν = ασφάλεια ασθενών.>")






