Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Νεότερα στις συνιστώσες (πτυχές) του Μεταβολικού Συνδρόμου. ΛΙΠΙΔΙΑ
Νεότερα στις συνιστώσες (πτυχές) του Μεταβολικού Συνδρόμου. ΛΙΠΙΔΙΑ Ελένη Μπιλιανού Καρδιολόγος Υπεύθυνη Λιπιδαιμικού Ιατρείου Τζάνειο Νοσοκομείο
 του Μεταβολικού Συνδρόμου. ΛΙΠΙΔΙΑ. Ελένη Μπιλιανού. Καρδιολόγος. Υπεύθυνη Λιπιδαιμικού Ιατρείου. Τζάνειο Νοσοκομείο.")
2
Reaven χαρακτηριστικά μεταβολικού συνδρόμου, «Σύνδρομο Χ»
Αντίσταση στην ινσουλίνη Υπερινσουλιναιμία Υπεργλυκαιμία Υπέρταση Αυξημένα τριγλυκερίδια Μειωμένη HDL-X ADA (Banting Lecture ADA Meeting 1988)
")
3
Μεταβολικό σύνδρομο: υψηλός καρδιαγγειακός κίνδυνος
ΚΑ Θνησιμότητα RR 3,55 Μεταβολικό Σύνδρομο Καρδιαγγειακή θνησιμότητα Ομάδα ελέγχου Παρακολούθηση, έτη RR = σχετικός κίνδυνος Lakka, JAMA 2004;288:

4
Είναι ο κίνδυνος στο ΜΣ μεγαλύτερος από το άθροισμα των επιμέρους παραγόντων κινδύνου?
Επιδημιολογικά δεδομένα συνηγορούν ότι η παρουσία πολλών παραγόντων κινδύνου αυξάνει τον κίνδυνο περισσότερο από το άθροισμα τους. Ο κίνδυνος αυξάνεται γεωμετρικά και όχι γραμμικά. Το φαινόμενο καλείται πολλαπλασιαστικός κίνδυνος. Stamler J, Stamler R, Neaton JD Arch Intern Med 1993; 153: 598–615. Kannel WB, Larson M The Framingham experience. Cardiology 1993; 82: 137–52. Ferrucci L, Furberg CD, Penninx BW, et al. Circulation 2001;104:1923– 6. The question has been raised as to whether the risk for ASCVD associated with the metabolic syndrome is greater than the sum of its risk factors (44). The answer is the affirmative. First, epidemiological studies strongly suggest that multiple risk factors raise risk more than the sum of accompanying single risk factors (45–48); risk rises geometrically instead of linearly. This phenomenon is called multiplicative risk. 45. Kannel WB. Importance of hypertension as a major risk factor in cardiovascular disease. In: Genest J, Koiw E, Kuchel O, editors. Hypertension: Physiopathology and Treatment. New York, NY: McGraw-Hill Book Company, 1977:888 –910. 46. Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and diastolic, and cardiovascular risks. U.S. population data. Arch Intern Med 1993;153:598–615. 47. Kannel WB, Larson M. Long-term epidemiologic prediction of coronary disease. The Framingham experience. Cardiology 1993;82: 137–52. 48. Ferrucci L, Furberg CD, Penninx BW, et al. Treatment of isolated systolic hypertension is most effective in older patients with high-risk profile. Circulation 2001;104:1923– 6.
. The answer is the. affirmative. First, epidemiological studies strongly suggest. that multiple risk factors raise risk more than the sum of. accompanying single risk factors (45–48); risk rises geometrically. instead of linearly. This phenomenon is called multiplicative risk. 45. Kannel WB. Importance of hypertension as a major risk factor in. cardiovascular disease. In: Genest J, Koiw E, Kuchel O, editors. Hypertension: Physiopathology and Treatment. New York, NY: McGraw-Hill Book Company, 1977:888 – Stamler J, Stamler R, Neaton JD. Blood pressure, systolic and. diastolic, and cardiovascular risks. U.S. population data. Arch Intern. Med 1993;153:598– Kannel WB, Larson M. Long-term epidemiologic prediction of. coronary disease. The Framingham experience. Cardiology 1993;82: 137– Ferrucci L, Furberg CD, Penninx BW, et al. Treatment of isolated. systolic hypertension is most effective in older patients with high-risk. profile. Circulation 2001;104:1923– 6.")
5
INTERHEART: η επίδραση των παραγόντων κινδύνου στην επίπτωση του ΕΜ
Smk = κάπνισμα DM = σακχαρώδης διαβήτης HTN = υπέρταση Obes = παχυσαρκία Ps = ψυχοκοινωνικοί παράγοντες Yusuf S et al. Lancet. 2004; 364:

6
Μεταβολικό σύνδρομο-ΕΛΛΑΔΑ (NCEP definition)
Athyros VG, et al. Diabetes Obes Metab 2005;7:

7
Μεταβολικό σύνδρομο-ΕΛΛΑΔΑ (NCEP definition)
Athyros VG, et al. Diabetes Obes Metab 2005;7:

8
REVIEW: Peroxisome Proliferator-Activated Receptor
and Adipose Tissue—Understanding Obesity-Related Changes in Regulation of Lipid and Glucose Metabolism

9
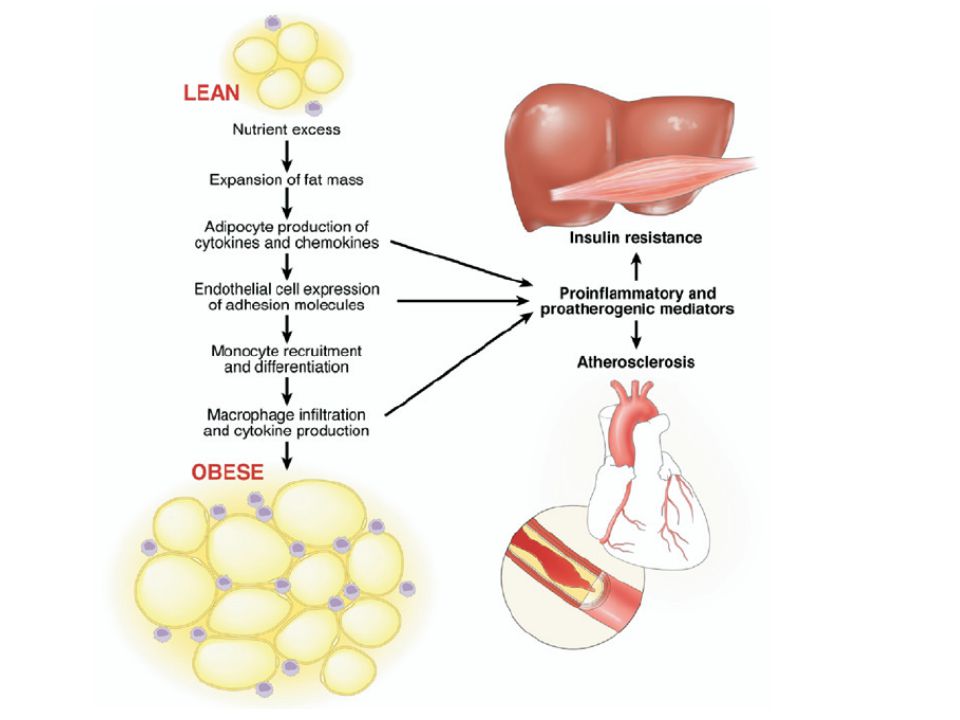
Η Παχυσαρκία Χαρακτηρίζεται
Απο Ηπια Φλεγμονώδη Αντίδραση του Λιπώδους Ιστου Ο λιπώδης ιστός πέραν του ώριμου λιποκυττάρου αποτελείται από προλιποκύτταρα, αγγεία, νεύρα και λίγα μακροφάγα. Με την προοδευτική αύξηση του βάρους, ΤΑ ΩΡΙΜΑ ΛΙΠΟΚΥΤΤΑΡΑ ΕΚΦΡΑΖΟΥΝ ΜΟΡΙΑ ΠΟΥ ΠΡΟΣΕΛΚΥΟΥΝ ΜΑΚΡΟΦΑΓΑ. ο αριθμός των μακροφάγων αυξάνεται. Τα μακροφάγα αυτά παράγοντας φλεγμονώδεις κυτταροκίνες δρουν στα γειτονικά τους λιποκύτταρα τα οποία με τη σειρά τους γίνονται λιγότερο ευαίσθητα στην ινσουλίνη και παράγουν επίσης φλεγμονώδεις κυτταροκίνες. Έτσι τα όρια ανάμεσα στα δυο κύτταρα γίνονται ασαφή.

11
ΔΡΑΣΗ ΤΗΣ ΙΝΣΟΥΛΙΝΗΣ ΣΤΟ ΛΙΠΟΚΥΤΤΑΡΟ
Αντίσταση στη δράση της ινσουλίνης σε επιπεδο λιποκυτταρου οδηγεί σε αυξημενη λιπολυση και ελευθερωση ελευθερων λιπαρων οξεων στην κυκλοφορια.

12
Συνοπτικά η παχυσαρκία μέσω ER stress oδηγεί σε ενεργοποίηση φλεγμονωδών μονοπατιών, παραγωγή ROS, αντίσταση στην ινσουλίνη και τελικά απόπτωση.

13
Ηπατική παραγωγή πλούσιων σε τριγλυκερίδια VLDL
Fig. 2. Portrayed is the metabolic model for apo B metabolism. The lipoprotein assembly is initiated by the lipidation of apo B mediated by MTP (microsomal transfer protein). Further lipids are added to the “pre” VLDL particles during its maturation first to VLDL 2 particles and finally to lipid-rich VLDL 2 particle. Apo B-containing particles released into circulation range from LDL to VLDL 1. The loading of newly formed particles with lipids determines the density of secreted particles. The production of VLDL 1 and VLDL 2 particles are regulated independently. The site of insulin action is located at the final step of lipid loading that produces VLDL 1 particles. The particles are subject to lipolysis and remodelling in the circulation and they are metabolized via two parallel cascades. The subscript shows the VLDL apo B production during saline infusion (open columns) and during an 8.5-h euglycaemic clamp (closed columns) in normal healthy men and in Type 2 diabetic subjects. Insulin suppressed the rate of VLDL 1 apo B synthesis by 50% in normal men but failed to suppress the synthesis of VLDL 1 apo B in Type 2 diabetic men. [Reproduced from references [47, 50] with permission of Diabetologia (Diabetologia 1997; 40: ) and Arteriosclerosis Thrombosis Vascular Biology (Arterioscler Thromb Vasc Biol 1997; 17: )] Malmstrom R, Packard CJ, Watson TDG et al. (1997) Metabolic basis of hypotriglyceridemic effects of insulin in normal men. Arterioscler Thromb Vasc Biol 17: Malmstrom R Arterioscler Thromb Vasc Biol 17: , 1997
. Further lipids are added to the pre VLDL particles during its maturation first to VLDL 2 particles and finally to lipid-rich VLDL 2 particle. Apo B-containing particles released into circulation range from LDL to VLDL 1. The loading of newly formed particles with lipids determines the density of secreted particles. The production of VLDL 1 and VLDL 2 particles are regulated independently. The site of insulin action is located at the final step of lipid loading that produces VLDL 1 particles. The particles are subject to lipolysis and remodelling in the circulation and they are metabolized via two parallel cascades. The subscript shows the VLDL apo B production during saline infusion (open columns) and during an 8.5-h euglycaemic clamp (closed columns) in normal healthy men and in Type 2 diabetic subjects. Insulin suppressed the rate of VLDL 1 apo B synthesis by 50% in normal men but failed to suppress the synthesis of VLDL 1 apo B in Type 2 diabetic men. [Reproduced from references [47, 50] with permission of Diabetologia (Diabetologia 1997; 40: ) and Arteriosclerosis Thrombosis Vascular Biology (Arterioscler Thromb Vasc Biol 1997; 17: )] Malmstrom R, Packard CJ, Watson TDG et al. (1997) Metabolic basis of hypotriglyceridemic effects of insulin in normal men. Arterioscler Thromb Vasc Biol 17: Malmstrom R Arterioscler Thromb Vasc Biol 17: ,")
14
Σχηματισμός μικρών και πυκνών LDL και HDL
Fig. 6. Proposed mechanisms behind the generation of small dense LDL and small dense HDL in Type 2 diabetes. The increase of TRLs due to both exaggerated postprandial lipemia and VLDL 1 overproduction in the face of low LPL activity results in the long-residence time of TRL particles in circulation. These favour the exchange of core lipids, mediated by cholesterol ester transfer protein (CETP), between both LDL and TRLs and HDL and TRLs leading to triglyceride enrichment of both LDL and HDL particles. These particles are good substrate for hepatic lipase which is commonly increased in Type 2 diabetes [14]. The hydrolysis of HDL particles produces smaller particles that have enhanced catabolic rate as shown in the subscript panel. Taken together there is a symmetry of mechanisms leading to formation of small dense LDL and HDL. Reproduced from reference [7] with permission of Elsevier (The Lancet, 1997, 350, Suppl 1, 20.23) Syvanne M, Taskinen M-R (1997) Lipids and lipoproteins as coronary risk factors in non-insulin dependent diabetes mellitus. Lancet 350 [Suppl 1]:20.23 Syvanne M, Taskinen M-R Lancet 350 [Suppl 1]:
, between both LDL and TRLs and HDL and TRLs leading to triglyceride enrichment of both LDL and HDL particles. These particles are good substrate for hepatic lipase which is commonly increased in Type 2 diabetes [14]. The hydrolysis of HDL particles produces smaller particles that have enhanced catabolic rate as shown in the subscript panel. Taken together there is a symmetry of mechanisms leading to formation of small dense LDL and HDL. Reproduced from reference [7] with permission of Elsevier (The Lancet, 1997, 350, Suppl 1, 20.23) Syvanne M, Taskinen M-R (1997) Lipids and lipoproteins as coronary risk factors in non-insulin dependent diabetes mellitus. Lancet 350 [Suppl 1]: Syvanne M, Taskinen M-R Lancet 350 [Suppl 1]:")
15
ΜΣ Πολυοργανική Παθολογική Οντότητα

16
Συσσώρευση τριγλυκεριδίων σε ιστούς εκτός του λίπους
Positive net energy balance exceeds the buffering capacity of adipose tissue, leading to glucolipotoxicity. Positive net energy balance, resulting from increased calorie intake and reduced energy expenditure, leads to an accumulation of triglyceride in many tissues, particularly in adipose tissue. The accumulation of triglyceride in adipose tissue leads to increased lipolysis by a mass effect. This, associated with the development of adipocyte insulin resistance, results in net spillover of fatty acids to nonadipose tissue, which further increases extraadipocytic triglyceride storage, leading to many of the typical features that characterize the insulin-resistant state and type 2 diabetes. Lewis GF et al. Endocrine Reviews 23: 201–229, 2002

17
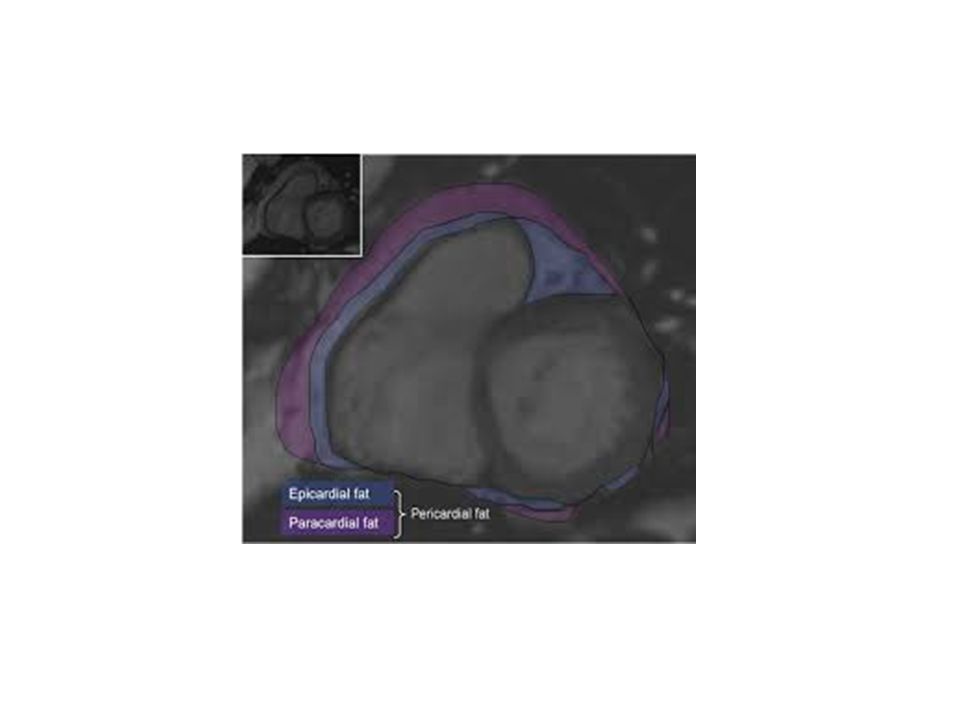
Λιπώδης ιστός της καρδιάς
Ενδοκυττάριο λίπος Εξωκυττάριο λίπος επικαρδιακό περικαρδιακό περιαγγειακό

18
Ενδοκυττάριο λίπος 1% του συνόλου της καρδιακής μάζας
Αυξάνεται με την ηλικία περισσότερο οι άνδρες και οι γυναίκες με ΣΔ

19
Παχυσαρκία, ΣΔ, ΜΣ Τα ενδοκαρδιακά τριγλυκερίδια 2πλάσια – 4πλάσια
Iacobellis G. et al J Am Soc Echocardiogr 2009

21
Εξωκυττάριο λίπος Επικαρδιακό Περικαρδιακό
εφάπτεται απευθείας στον καρδιακό μυ διάχυση ουσιών, μετανάστευση κυττάρων Περικαρδιακό ανάμεσα στις δύο περικαρδιακές μεμβράνες Περιαγγειακό περιβάλλει στεφανιαίες αρτηρίες και αρτηριόλια

24
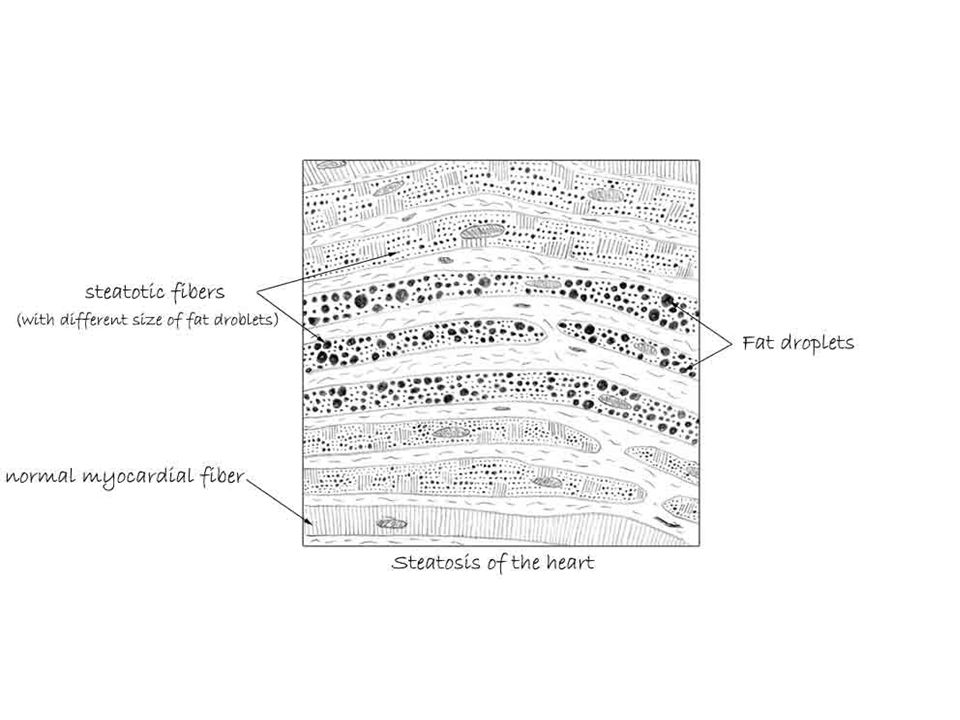
Λιπώδης καρδιά Η καρδιά προτιμά τα ΛΟ σαν πηγή ενέργειας 60%
Η περίσσεια→λιποειδή σταγονίδια στο κύτταρο Μείωση συσπαστικότητας πιθανόν μέσω μείωσης της διόδου Ca από τις κυτταρικές μεμβράνες Σε ΟΒ ΣΔ και υπερΤΓΛ υπερτροφία, λιποτοξίκωση,απόπτωση Επικαρδιακό λίπος >20% συσχέτιση με σπλαχνικό

25
Grundy SM et al. Circulation 2005;112:2735-52
Δίαιτα Ελάττωση προσλαμβανόμενων θερμίδων κατά /μέρα - στόχος απώλεια βάρους 5-10% εντός 6-12 μηνών Λίπη <25-35% των ολικών θερμίδων, κυρίως ακόρεστα Αύξηση πρόσληψης δημητριακών, φρούτων, λαχανικών, γαλακτοκομικών προϊόντων χωρίς λιπαρά Περιορισμός κατανάλωσης νατρίου (< 2,4 g/ημέρα) Περιορισμός κατανάλωσης αλκοόλ (άνδρες < 2 ποτά/ημέρα, γυναίκες < 1 ποτό/ημέρα) Grundy SM et al. Circulation 2005;112:
 Περιορισμός κατανάλωσης αλκοόλ (άνδρες < 2 ποτά/ημέρα, γυναίκες < 1 ποτό/ημέρα) Grundy SM et al. Circulation 2005;112:")
26
Grundy SM et al. Circulation 2005;112:2735-52
Άσκηση Μέτριας έντασης αερόβια άσκηση > 30 min/ημέρα Τουλάχιστον 5 μέρες την εβδομάδα και κατά προτίμηση κάθε μέρα Προοδευτική έναρξη – προοδευτική αύξηση διάρκειας άσκησης Grundy SM et al. Circulation 2005;112:

27
Walking for Health: More Is Better
8-Year follow-up n= Women Abstract/Summary: BACKGROUND: The role of walking, as compared with vigorous exercise, in the prevention of coronary heart disease remains controversial, and data for women on this topic are sparse. METHODS: We prospectively examined the associations between the score for total physical activity, walking, and vigorous exercise and the incidence of coronary events among 72,488 female nurses who were 40 to 65 years old in Participants were free of diagnosed cardiovascular disease or cancer at the time of entry and completed serial detailed questionnaires about physical activity. During eight years of follow-up, we documented 645 incident coronary events (nonfatal myocardial infarction or death from coronary disease). RESULTS: There was a strong, graded inverse association between physical activity and the risk of coronary events. As compared with women in the lowest quintile group for energy expenditure (expressed as the metabolic-equivalent [MET] score), women in increasing quintile groups had age-adjusted relative risks of 0.77, 0.65, 0.54, and 0.46 for coronary events (P for trend <0.001). In multivariate analyses, the inverse gradient remained strong (relative risks, 0.88, 0.81, 0.74, and 0.66 for women in increasing quintile groups as compared with those in the lowest quintile group; P for trend=0.002). Walking was inversely associated with the risk of coronary events; women in the highest quintile group for walking, who walked the equivalent of three or more hours per week at a brisk pace, had a multivariate relative risk of 0.65 (95 percent confidence interval, 0.47 to 0.91) as compared with women who walked infrequently. Regular vigorous exercise (> or =6 MET) was associated with similar risk reductions (30 to 40 percent). Sedentary women who became active in middle adulthood or later had a lower risk of coronary events than their counterparts who remained sedentary. CONCLUSIONS: These prospective data indicate that brisk walking and vigorous exercise are associated with substantial and similar reductions in the incidence of coronary events among women. Citation: Manson JE, Hu FB, Rich-Edwards JW, Colditz GA, Stampfer MJ, Willett WC, Speizer FE, Hennekens CH. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. N Engl J Med 1999;341(9):650-8. Risk for Coronary Heart Disease (CHD) ¯ 23% ¯ 35% ¯ 46% ¯ 54% Lowest Level of Walking Highest Level of Walking (3+ Hours of Brisk Walking) Manson JE. N Engl J Med 1999;341:
. RESULTS: There was a strong, graded inverse association between physical activity and the risk of coronary events. As compared with women in the lowest quintile group for energy expenditure (expressed as the metabolic-equivalent [MET] score), women in increasing quintile groups had age-adjusted relative risks of 0.77, 0.65, 0.54, and 0.46 for coronary events (P for trend <0.001). In multivariate analyses, the inverse gradient remained strong (relative risks, 0.88, 0.81, 0.74, and 0.66 for women in increasing quintile groups as compared with those in the lowest quintile group; P for trend=0.002). Walking was inversely associated with the risk of coronary events; women in the highest quintile group for walking, who walked the equivalent of three or more hours per week at a brisk pace, had a multivariate relative risk of 0.65 (95 percent confidence interval, 0.47 to 0.91) as compared with women who walked infrequently. Regular vigorous exercise (> or =6 MET) was associated with similar risk reductions (30 to 40 percent). Sedentary women who became active in middle adulthood or later had a lower risk of coronary events than their counterparts who remained sedentary. CONCLUSIONS: These prospective data indicate that brisk walking and vigorous exercise are associated with substantial and similar reductions in the incidence of coronary events among women. Citation: Manson JE, Hu FB, Rich-Edwards JW, Colditz GA, Stampfer MJ, Willett WC, Speizer FE, Hennekens CH. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. N Engl J Med 1999;341(9): Risk for Coronary Heart Disease (CHD) ¯ 23% ¯ 35% ¯ 46% ¯ 54% Lowest Level of Walking. Highest Level of Walking (3+ Hours of Brisk Walking) Manson JE. N Engl J Med 1999;341:")
28
Συστάσεις για φυσική δραστηριότητα
Για άτομα ηλικίας άνω των 65 ετών: Μέτριας έντασης φυσική δραστηριότητα για τουλάχιστον 30 λεπτά την ημέρα και για 5 ημέρες την εβδομάδα. ή Υψηλής έντασης άσκηση για τουλάχιστον 20 λεπτά την ημέρα και για 3 ημέρες την εβδομάδα. και Οκτώ έως 10 ασκήσεις με βάρη από 10 με 15 επαναλήψεις η κάθε άσκηση για δύο με τρεις φορές την εβδομάδα. Αν υπάρχει κίνδυνος πεσίματος, συμπεριλαμβάνονται και ασκήσεις ισορροπίας Over 65 years old Both aerobic and muscle-strengthening activity is critical for healthy aging. Moderate-intensity aerobic exercise means working hard at about a level-six intensity on a scale of 10. You should still be able to carry on a conversation during exercise. Older adults or adults with chronic conditions should develop an activity plan with a health professional to manage risks and take therapeutic needs into account. Nelson et al, Med Sci Sports Exerc, 2007 28

29
ΘΕΡΑΠΕΙΑ Χαμηλή σε θερμίδες δίαιτα και άσκηση
μειώνει το εξωκαρδιακό λίπος περισσότερο συγκριτικά με το λίπος σε άλλα μέρη του σώματος

30
Τριγλυκερίδια: Θεραπευτικές σκέψεις
Αλλαγές Τρόπου Ζωής Φαρμακοθεραπεία Μόλις αυξημένα TG: διαιτητικές αλλαγές, αύξηση άσκησης Φάρμακα που μειώνουν τα TG - Νικοτινικό οξύ - Φιμπράτες - Ω-3 ΛΟ Άσκηση: - οδηγεί σε καλλίτερη κυτταρική χρησιμοποίηση της ενέργειας στους ιστούς (↓TG, ↑HDL-C) - Σε διαβητικούς μειώνει τις ανάγκες σε ινσουλίνη - μειώνει τα TG (LDL-C) ακόμη και σε απουσία απώλειας βάρους Επιπλέον φάρμακα μείωσης TG: - γλιταζόνες - στατίνες (μέτρια δράση) - διακοπή αλκοόλ (το αλκοόλ μειώνει την β-οξείδωση των ΛΟ) Πολύ υψηλά επίπεδα TG (>500mg/dl) απαιτούν θεραπεία πρόληψης παγκρεατίτιδας
 - Σε διαβητικούς μειώνει τις ανάγκες σε ινσουλίνη. - μειώνει τα TG (LDL-C) ακόμη και σε απουσία απώλειας βάρους. Επιπλέον φάρμακα μείωσης TG: - γλιταζόνες. - στατίνες (μέτρια δράση) - διακοπή αλκοόλ (το αλκοόλ μειώνει την β-οξείδωση των ΛΟ) Πολύ υψηλά επίπεδα TG (>500mg/dl) απαιτούν θεραπεία πρόληψης παγκρεατίτιδας.")
31
Νέος ορισμός για το ΜΣ; CIRCULATORY SYNDROME
An Evolution of the Metabolic Syndrome concept Khoshdel A.Curr Cardiol Rev 2012

32
Circulatory syndrome Σκοπός Να συμπεριληφθούν νέοι δείκτες της ΚΑΝ (Νεφρική διαταραχή, μικρολευκωματινουρία, Αρτηριακή σκληρία, αναιμία κ.ά.) Και να προστεθούν στους κλασσικούς. Τελικό κοινό μονοπάτι φλεγμονή, οξειδ. Stress, υπερπηκτικότητα βλάβη ενδοθηλίου - ΚΑΝ

33
Νέες θεραπείες ΑΔΙΠΟΝΕΚΤΊΝΗ ΛΕΠΤΙΝΗ

34
ΜΕΤΑΒΟΛΙΚΟ ΣΥΝΔΡΟΜΟ ΠΟΛΥΟΡΓΑΝΙΚΟ ΝΟΣΗΜΑ ΣΕ ΣΥΝΕΧΗ ΑΝΟΔΟ ΧΡΕΙΑΖΕΤΑΙ ΕΠΕΙΓΟΥΣΑ ΜΕΡΙΜΝΑ

35
Prevalence of MetS in obesechildren
WHO NCEP CSMS HDLc % % % TG % % % HY % % % MetS prev % % % Invitti C. et al. ADA 63th

36
Child Specific criteria MS
BMI > 97th ηλικία και φύλο ΑΠ και ΤΓΛ > 95th HDLc < 5th σακχαρώδης διαβήτης ή διαταρ. γλυκόζης νηστείας ή φόρτησης ή HOMA-IR > 2.5

37
Does Treating The Metabolic Syndrome Make a Difference?
Finnish Diabetes Prevention Study Σχεδιασμός 522 μεσήλικες υπέρβαροι/παχύσαρκοι ασθενείς (μέσο BMI 31 kg/m2) 172 ♂ και 350 ♀ Μέση διάρκεια 3.2 έτη Ομάδα παρέμβασης: εξατομικευμένο σχέδιο δράσης Μείωση βάρους, συνολική πρόσληψη λίπους και κεκορεσμένων λιπαρών Αύξηση πρόσληψης φυτικών ινών και άσκηση Tuomilehto J, et al. N Engl J Med. 2001;344:
 172 ♂ και 350 ♀ Μέση διάρκεια 3.2 έτη. Ομάδα παρέμβασης: εξατομικευμένο σχέδιο δράσης. Μείωση βάρους, συνολική πρόσληψη λίπους και κεκορεσμένων λιπαρών. Αύξηση πρόσληψης φυτικών ινών και άσκηση. Tuomilehto J, et al. N Engl J Med. 2001;344:")
38
Finnish Diabetes Prevention Study
Όφελος από τη θεραπεία του μεταβολικού συνδρόμου Finnish Diabetes Prevention Study Intervention Control 0% 5% 10% 15% 20% 25% -58% Ο κίνδυνος εμφάνισης διαβήτη 4 χρόνια μετά: Tuomilehto J, et al. N Engl J Med. 2001;344:

39
ΑΣΚΗΣΗ ΚΑΙ ΥΓΕΙΑ ΝΙΗ Η κατανάλωση με άσκηση 500 -2000 kcal / w
ΑΣΚΗΣΗ ΚΑΙ ΥΓΕΙΑ Η κατανάλωση με άσκηση kcal / w ↓ έως 40% την ολική θνητότητα ( Η διακοπή του καπνίσματος 44% ) ΝΙΗ
 ΝΙΗ.")
40
Helsinki Heart Study: combined effects of BMI and dyslipidemia on response to treatment 70 BMI 26 kg/m2 BMI > 26 10 20 30 40 50 60 P G CHD events/1000 BMI > 26 kg/m2 plus dyslipidaemia 80 16% 48% 78% Tenkanen et al. Circulation, 1995

Παρόμοιες παρουσιάσεις