Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
Υπερβολική ημερήσια υπνηλία
Σοφία Ε. Σχίζα Επίκουρη Καθηγήτρια Πνευμονολογίας Υπεύθυνη Εργαστηρίου Ύπνου Ιατρική Σχολή, Παν/μίου Κρήτης

2
Υπνηλία Τι είναι υπνηλία Γιατί την εκτιμούμε Πως την εκτιμούμε Αίτια
Αντιμετώπιση

3
Υπνηλία-ορισμός Sleepiness
A state of decreased ability to maintain wakefulness or increased propensity to fall asleep A normal biologic need or drive; sleep is to sleepiness as food is to hunger Krieger J. Sleep 2000:15;23(suppl 4):S95-98. Η Υπερβολική υπνηλία (ΥΥ) είναι η αδυναμία επίτευξης και διατήρησης της αφύπνισης και της εγρήγορσης απαραίτητες για την εκτέλεση καθημερινών δραστηριοτήτων Lee-Chiong TL. In Sleep Medicine. Philadelphia, PA Hanley & Belfus Inc 2002 80% ασθενών με ημερήσια υπνηλία: ΣΑΥ, ναρκοληψία και ιδιοπαθή υπερυπνία Mitler MM et al. Sleep 1994;17:352-71
:S Η Υπερβολική υπνηλία (ΥΥ) είναι η αδυναμία επίτευξης και διατήρησης της αφύπνισης και της εγρήγορσης απαραίτητες για την εκτέλεση καθημερινών δραστηριοτήτων. Lee-Chiong TL. In Sleep Medicine. Philadelphia, PA Hanley & Belfus Inc % ασθενών με ημερήσια υπνηλία: ΣΑΥ, ναρκοληψία και ιδιοπαθή υπερυπνία. Mitler MM et al. Sleep 1994;17:")
4
Overlap of Symptoms of Fatigue and Sleepiness
Major Depression Chronic Fatigue Syndrome Excessive Sleepiness Parkinson’s Sleepiness MS Symptoms of ES, fatigue, and sleepiness can overlap in some disease states. Patients with sleep apnea can present with symptoms of both fatigue and ES, while Parkinson's patients are sleepy and have pathologic fatigue. Depression and CFS patients primarily are fatigued. Shift Work Sleep Disorder Sleep Deprivation Narcolepsy Sleep Apnea

5
Υπερβολική υπνηλία (ΥΥ)-ένα σύνηθες πρόβλημα
NSF, p. 11, ¶ 1. 40 37% 30 Ενήλικες στις ΗΠΑ αναφέρουν (%) 20 16% 10 Τουλάχιστον κάποιες ημέρες κάθε μήνα Τουλάχιστον κάποιες ημέρες κάθε εβδομάδα Η υπνηλία επηρεάζει τις καθημερινές δραστηριότητες National Sleep Foundation “Sleep in America” Poll. March 2002.
 % 10. Τουλάχιστον κάποιες ημέρες κάθε μήνα. Τουλάχιστον κάποιες ημέρες κάθε εβδομάδα. Η υπνηλία επηρεάζει τις καθημερινές δραστηριότητες. National Sleep Foundation Sleep in America Poll. March")
6
+ The “Sleep Switch” TMN LC/DR PPT/LDT Hist NE/5-HT ACh Arousal
Saper CB, Chou TC, Scammell TE. Trends Neurosci. 2001(Dec);24(12):
;24(12):")
7
Physiologic Determinants of Sleepiness
Normal Sleepiness Sleep Drive Wake Propensity Work Seep Sleep load → homeostat increases wake dissipates sleep Accumulates across day CR governed by SCN-light-dark OUTPUT ALERTING PULSE Sum = wake sleep propensity Direction of up down alertness MWT/MSLT = wake propensity Kryger MH, Thomas R, Dement WC, editors. Principles and Practices of Sleep Medicine. 3rd edition. Philadelphia: W.B. Saunders Circadian Drive for Wakefulness 9 a.m. 3 p.m. 9 p.m. 3 a.m. 9 a.m. Awake Asleep Kryger MH et al. (2000), Principles and Practices of Sleep Medicine, 3rd ed. Philadelphia: W.B. Saunders
, Principles and Practices of Sleep Medicine, 3rd ed. Philadelphia: W.B. Saunders.")
8
Γιατί την εκτιμούμε Κλινική απόφαση Ερευνητικοί λόγοι Νομικοί λόγοι
Οι ασθενείς θεωρούν απαραίτητη την αντιμετώπιση της ημερήσιας υπνηλίας τους για την κοινωνική, επαγγελματική και προσωπική τους ζωή

9
Υπερβολική υπνηλία (YY)- κλινική εικόνα
Aldrich, p. 100, col. 1, ¶ 3 & col. 2, ¶ 3. Shneerson, p. 128, col. 1, ¶ 2. Κόπωση Έλλειψη ενεργητικότητας Δυσκολία συγκέντρωσης Απουσία κινήτρων Έλλειψη αισθήματος ευεξίας Aldrich MS. Obstructive Sleep Apnea Syndrome. In: Sleep Medicine. New York, NY: Oxford University Press, Inc.; 1999:

10
Υπερβολική υπνηλία (YY)- επιπτώσεις
Shneerson, p. 127, Table 6.2. Ατυχήματα (ταξίδια, σπίτι, εργασία) Διαταραχές διάθεσης, ευερεθιστότητα Έλλειψη διανοητικής προσαρμογής Μειωμένη απόδοση στην εργασία Μειωμένη σωματική απόδοση Μειωμένη εγρήγορση και προσοχή Διαταραγμένες κοινωνικές αλληλεπιδράσεις Shneerson JM. Sleep Medicine: A Guide to Sleep and Its Disorders. 2nd ed. Malden, Mass: Blackwell Science Ltd; 2005.
 Διαταραχές διάθεσης, ευερεθιστότητα. Έλλειψη διανοητικής προσαρμογής. Μειωμένη απόδοση στην εργασία. Μειωμένη σωματική απόδοση. Μειωμένη εγρήγορση και προσοχή. Διαταραγμένες κοινωνικές αλληλεπιδράσεις. Shneerson JM. Sleep Medicine: A Guide to Sleep and Its Disorders. 2nd ed. Malden, Mass: Blackwell Science Ltd;")
11
Πώς την εκτιμούμε Υποκειμενικές μετρήσεις: ESS (φυσιολογικές τιμές 6±2) Αντικειμενικές μετρήσεις: MSLT (παθολογικές τιμές< 8 min), MWT
 Αντικειμενικές μετρήσεις: MSLT (παθολογικές τιμές< 8 min), MWT.")
12
Υπερβολική υπνηλία (YY)-Αίτια Ι
A Sleep-related Breathing Disorders Hypersomnias Circadian Rhythm Sleep Disorders (eg, Narcolepsy) (eg, OSAHS) (eg, SWSD) Υπερβολική υπνηλία Insomnias Psychiatric/ Behavioral Disorders* Parasomnias Other Sleep Disorders Sleep-related Movement Disorders ANIMATION PROGRESSION B *Non-sleep disorders included in the ICSD due to their frequent association with sleep disorders. OSAHS = obstructive sleep apnea/hypopnea syndrome; SWSD = shift work sleep disorder; ICSD = The International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
 (eg, OSAHS) (eg, SWSD) Υπερβολική. υπνηλία. Insomnias. Psychiatric/ Behavioral Disorders* Parasomnias. Other Sleep Disorders. Sleep-related Movement Disorders. ANIMATION PROGRESSION. B. *Non-sleep disorders included in the ICSD due to their frequent association with sleep disorders. OSAHS = obstructive sleep apnea/hypopnea syndrome; SWSD = shift work sleep disorder; ICSD = The International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine;")
13
Υπερβολική υπνηλία (YY)-Αίτια ΙΙ
Increased Sleep Drive Sleep Disruption Disorders of Sleep/Wake Regulation Disorders of Sleep Disruption Narcolepsy Obstructive Sleep Apnea/Hypopnea Syndrome Disorders of Circadian Alignment SWSD

14
Σύνδρομο Απνοιών Υποπνοιών στον Ύπνο (ΣΑΥΥ)
Επαναλαμβανόμενα επεισόδια απόφραξης ανώτερου αεραγωγού κατά τον ύπνο Μείωση εύρους ανώτερου αεραγωγού Μείωση τόνου μυών ανώτερων αεραγωγών κατά τον ύπνο

15
Cardiovascular Stressors
Επιπτώσεις ΣΑΥΥ Sleep Arrhythmia Systemic hypertension Chronic hypercapnia Pulmonary hypertension Cor pulmonale Loss of airway tone Airway obstruction Hypoxia Hypercapnia Acidosis Cardiovascular Stressors This slide depicts the cycle of events that occurs in a patient with OAS. Loss of airway tone during sleep leads to obstruction, resulting in hypoxia, hypocapnia, and acidosis Patient then becomes aroused, leading to patency of the airway The metabolic changes that occur can lead to cardiac symptoms and oftentimes hypertension The constant cycle of sleep and arousal leads to hypersomnolence and impaired cognition Arousal Sleepiness, impaired cognition Fragmented sleep Increase in airway tone Patent airway Adapted from: Rapoport DM. Mt Sinai J Med

16
CPAP: επίδραση CPAP στην ημερήσια λειτουργία
Αρκετές RCT επιβεβαιώνουν την αποτελεσματικότητα του CPAP στην ημερήσια λειτουργία ασθενών με ΣΑΥΥ 2.91 4.75 AHI>30/hour of sleep Patel Arch Intern Med 2003;163:565-71

17
1.6 s Mazza S et al, ERJ 2007 0.98 s * 0.6 seconds: 22 m at 130km/h
0,2 0,4 0,6 0,8 1 1,2 1,4 1,6 1,8 2 Simple Distraction CONTROLS n=10 OSAS n=10 * 0.98 s 1.6 s 0.6 seconds: 22 m at 130km/h Διαταραχές προσοχής, αντίδρασης σε ασθενείς με ΣΑΥΥ (ESS, Osler) επηρεάζουν την ικανότητα οδήγησης Mazza S et al, ERJ 2007
 επηρεάζουν την ικανότητα οδήγησης. Mazza S et al, ERJ")
18
Διάσπαση της προσοχής, ικανότητα οδήγησης βελτιώνονται μετά CPAP
OSA before CPAP OSA on CPAP Διάσπαση της προσοχής, ικανότητα οδήγησης βελτιώνονται μετά CPAP Mazza S et al, ERJ 2007

19
Παρόλα αυτά υπάρχουν ασθενείς με ΣΑΥΥ υπό θεραπεία με CPAP που αναφέρουν υπολειμματική ημερήσια υπνηλία: Epworth sleepiness scale (ESS>10) Τι ορίζουμε όμως ως υπολειμματική υπνηλία???

20
Τι εννοούμε με τον όρο «υπολειμματική υπνηλία»? I
Στην υπνηλία όπως στην πείνα και στη δίψα: δύσκολος ο ορισμός και η μέτρηση Βελτίωση υπνηλίας λόγω και βελτίωσης διάθεσης (κατάθλιψη/άγχος) Guilleminaut et al Sleep 1996;19:117-22 Επίδραση του λεγόμενου “placebo effect” ή του τέλους της “honeymoon” περιόδου Engleman et al Am Respir Crit Care Med 1999;159:461-7 Η βαρύτητα της υπολειμματικής υπνηλίας μετά θεραπεία με PAP < αυτής του αθεράπευτου ΣΑΥΥ ή της υπό θεραπεία ναρκοληψίας
 Guilleminaut et al Sleep 1996;19: Επίδραση του λεγόμενου placebo effect ή του τέλους της honeymoon περιόδου. Engleman et al Am Respir Crit Care Med 1999;159: Η βαρύτητα της υπολειμματικής υπνηλίας μετά θεραπεία με PAP < αυτής του αθεράπευτου ΣΑΥΥ ή της υπό θεραπεία ναρκοληψίας.")
21
Τι εννοούμε με τον όρο «υπολειμματική υπνηλία»? II
Το ΣΑΥΥ είναι μάλλον παράγοντας κινδύνου για υπνηλία και όχι άμεση αιτία: Επιπολασμός ΑΗΙ>5/ώρα: 17-24% Επιπολασμός ΣΑΥΥ (ΑΗΙ+υπνηλία): 3-4% Pack A et al Am J Respir Crit Care Med 2006;173:7-15 Ροχαλητό και παχυσαρκία συσχετίζονται με υπνηλία ανεξάρτητα του ΑΗΙ Vgontzas A et al Arch Intern Med 1998;158:1333-7 Gottbier DJ et al Am Respir Crit Care Med 2000;162:1512-7 Υπνηλία συχνό σύμπτωμα του γενικού πληθυσμού σαν αποτέλεσμα περιορισμένης διάρκειας ύπνου Stradling JR et al J Sleep Res 2007;16:436-8
: 3-4% Pack A et al Am J Respir Crit Care Med 2006;173:7-15. Ροχαλητό και παχυσαρκία συσχετίζονται με υπνηλία ανεξάρτητα του ΑΗΙ. Vgontzas A et al Arch Intern Med 1998;158: Gottbier DJ et al Am Respir Crit Care Med 2000;162: Υπνηλία συχνό σύμπτωμα του γενικού πληθυσμού σαν αποτέλεσμα περιορισμένης διάρκειας ύπνου. Stradling JR et al J Sleep Res 2007;16:")
22
Επίπτωση ???

23
Residual sleepiness at 1 year in CPAP treated OSA (n=502)
For the whole group after one year of CPAP use: ESS 5.9 ± 4 ESS>10 60/502 patients remained sleepy on CPAP (ESS=14.3±2.5) Prevalence rate of RES of 12.0% (CI %) Pépin et al Eur Respir J
 Prevalence rate of RES of 12.0% (CI %) Pépin et al Eur Respir J.")
24
Prevalence rate of residual excessive sleepiness
RLS, major depression and narcolepsy were identified in respectively 25, 17 and 2% of the sleepy patient group versus 11, 4 and 1% in non sleepy OSA CPAP users (p<0.001) Considering all these diseases or situations as potential confounding factors for excessive daytime sleepiness these subjects were excluded for further analysis The prevalence rate of RES, without any explanation or associated disease was then of 6.0% (CI 3.9–8.01%) Pépin et al Eur Respir J
 Considering all these diseases or situations as potential confounding factors for excessive daytime sleepiness these subjects were excluded for further analysis. The prevalence rate of RES, without any explanation or associated disease was then of 6.0% (CI 3.9–8.01%) Pépin et al Eur Respir J.")
25
Impact of residual excessive sleepiness on quality of life
Pépin et al Eur Respir J

26
Conclusions of the prevalence study
First study establishing the prevalence rate of RES in a large group of 502 patients coming both from private and hospital practice As 230,000 OSA patients are currently treated in France by CPAP, one can estimate that more than 13,800 of them suffer from RES. As they generally complain from their sleepiness and exhibit altered quality of life, appropriate pharmacological therapy should be proposed to these patients

27
Post-CPAP sleepiness – a specific syndrome. Stradling JR et al J
Post-CPAP sleepiness – a specific syndrome? Stradling JR et al J. Sleep Res. (2007) 16, 436–438
 16, 436–438.")
28
Design: Multicenter, quasi-experimental study.
Relationship Between Hours of CPAP Use and Achieving Normal Levels of Sleepiness and Daily Functioning TE Weaver et al SLEEP 2007;30(6): Design: Multicenter, quasi-experimental study. Setting: Seven sleep centers in the United States and Canada. Conclusions: Our analyses suggest that a greater percentage of patients will achieve normal functioning with longer nightly CPAP durations, but what constitutes adequate use varies between different outcomes.
: Design: Multicenter, quasi-experimental study. Setting: Seven sleep centers in the United States and Canada. Conclusions: Our analyses suggest that a greater percentage of patients will achieve normal functioning with longer nightly CPAP durations, but what constitutes adequate use varies between different outcomes.")
29
Γιατί σε ορισμένους ασθενείς εμφανίζεται υπολειμματική υπνηλία???

30
Μακράς διάρκειας διακοπτόμενη οξυγόνωση (long term intermittent hypoxia)
Σε πειραματικό μοντέλο: προκαλεί αλλαγές σε κέντρα του εγκεφάλου μέσω φλεγμονώδους ενεργοποίησης, εξωκυττάριων επιπέδων ντοπαμίνης, οξειδωτικού stress, απόπτωσης. Μέσω αυτού του μηχανισμού εξηγείται πιθανά και η δράση της μοδαφιλίνης Cozal et al J Neurosci 2001;21: Zhian et al Am J Respir Crit Care Med 2005;172:921-9 Ωστόσο: Ασθενείς με σοβαρού βαθμού ΣΑΥΥ και απουσία υπνηλίας ή ηπίου βαθμού Ασθενείς με πλήρη υποχώρηση υπνηλίας μετά θεραπεία με PAP

31
Joo E etal Sleep 2010 Feb 1;33(2):235-41.
Υπολειμματική υπνηλία: A brain Hypoxic insult? Macey AJRCCM 2002 Reduced brain gray matter concentration in patients with obstructive sleep apnea syndrome. Joo E etal Sleep 2010 Feb 1;33(2): Alchanatis ERJ 2004
: Alchanatis ERJ")
32
Persistent sleepiness in CPAP treated obstructive sleep apnea patients: Evaluation and treatment Clinical Review Joan Santamaria et al Sleep Medicine Reviews (2007) 11, 195–207
 11, 195–207")
33
Persistent sleepiness in CPAP treated obstructive sleep apnea patients: Evaluation and treatment Clinical Review Joan Santamaria et al Sleep Medicine Reviews (2007) 11, 195–207 Δύο κατηγορίες ασθενών με ΣΑΥΥ, υπό θεραπεία με CPAP και υπολειμματική υπνηλία: Ασθενείς χωρίς καμία μεταβολή στην υπνηλία μετά την εφαρμογή CPAP Ασθενείς με αρχική βελτίωση της υπνηλίας μετά την εφαρμογή CPAP, αλλά μετά από κάποιο χρονικό διάστημα επανεμφάνιση υπνηλίας

34
Persistent sleepiness in CPAP treated obstructive sleep apnea patients: Evaluation and treatment Clinical Review Joan Santamaria et al Sleep Medicine Reviews (2007) 11, 195–207 Ασθενείς χωρίς καμία μεταβολή στην υπνηλία μετά την εφαρμογή CPAP. Αίτια: Εσφαλμένη διάγνωση ΣΑΥΥ Ανεπαρκής θεραπεία με CPAP Αδιάγνωστα συνοδά νοσήματα (κατάθλιψη, κακή υγειινή ύπνου, κ.λ.π) Άλλοι άγνωστοι παράγοντες
 Άλλοι άγνωστοι παράγοντες.")
35
Bilevel PAP: για ασθενείς με obesity hypoventilation syndrome
REM sleep hypoventilation

36
Ανεπαρκής πίεση του CPAP Περιοδικές κινήσεις ποδών
Αιτίες υπολειμματικής υπνηλίας: : κατακερματισμός ύπνου Ανεπαρκής πίεση του CPAP υπολειμματικό νόσημα Περιοδικές κινήσεις ποδών

37
Persistent sleepiness in CPAP treated obstructive sleep apnea patients: Evaluation and treatment Clinical Review Joan Santamaria et al Sleep Medicine Reviews (2007) 11, 195–207 Ασθενείς με αρχική βελτίωση της υπνηλίας μετά την εφαρμογή CPAP, αλλά μετά από κάποιο χρονικό διάστημα επανεμφάνιση υπνηλίας. Αίτια: Απώλεια προηγούμενης καλής συμμόρφωσης στη θεραπεία (νεοεγκατασταθείσα ρινίτιδα, νέος σύντροφος κρεβατιού….) Πρόσληψη κιλών Ανάπτυξη συνοδών νοσημάτων (κακή υγιεινή ύπνου, κατάθλιψη, άλλες διαταραχές ύπνου, κ.λ.π.) Απώλεια του «μήνα μέλιτος»/placebo effect (υποδηλώνει συνήθως ύπαρξη μη διαγνωσμένων νοσημάτων)
 Πρόσληψη κιλών. Ανάπτυξη συνοδών νοσημάτων (κακή υγιεινή ύπνου, κατάθλιψη, άλλες διαταραχές ύπνου, κ.λ.π.) Απώλεια του «μήνα μέλιτος»/placebo effect (υποδηλώνει συνήθως ύπαρξη μη διαγνωσμένων νοσημάτων)")
38
Αιτίες υπολειμματικής υπνηλίας: Κακή συνεργασία με το CPAP

39
Αιτίες υπολειμματικής υπνηλίας: κατακερματισμός ύπνου λόγω διαφυγών

40
Chen R et al Daytime sleepiness and its determining factors in Chinese obstructive sleep apnea patients. Sleep Breath 2010 Feb 20 CONCLUSION: EDS is correlated with the severity of OSAHS. More severe patients are characterized by higher ESS score, higher BMI, and progressive worsening of nocturnal hypoxemia. Nocturnal hypoxemia is a major determinant of EDS in Chinese OSAHS patients Koutsourelakis I., Predictors of residual sleepiness in adequately treated obstructive sleep apnoea patients. Eur Respir J 2009; 34: 687–693 In conclusion, predictors of residual excessive sleepiness in adequately CPAP-treated OSAS: were a history of depression, diabetes and heart disease, and a higher ESS score and lower RDI on initial assessment. Koutsourelakis I., Determinants of subjective sleepiness in suspected obstructive sleep apnoea J. Sleep Res. (2008) 17, 437–443 Primarily depression and diabetes, but also COPD, stroke, heart disease, alcohol use and increased BMI may contribute to increased subjective sleepiness.
 17, 437–443. Primarily depression and diabetes, but also COPD, stroke, heart disease, alcohol use and increased BMI may contribute to increased subjective sleepiness.")
43
What Keep us awake? DISCOVERING TREATMENTS TO FIGHT EFFICIENTLY AGAINST EXCESSIVE DAYTIME SLEEPINESS IS A CHALLENGE FOR BOTH SLEEP MEDICINE AND BASIC SCIENCE Boutrel B, Koob G. Sleep 2004(15);27(6):
;27(6):")
45
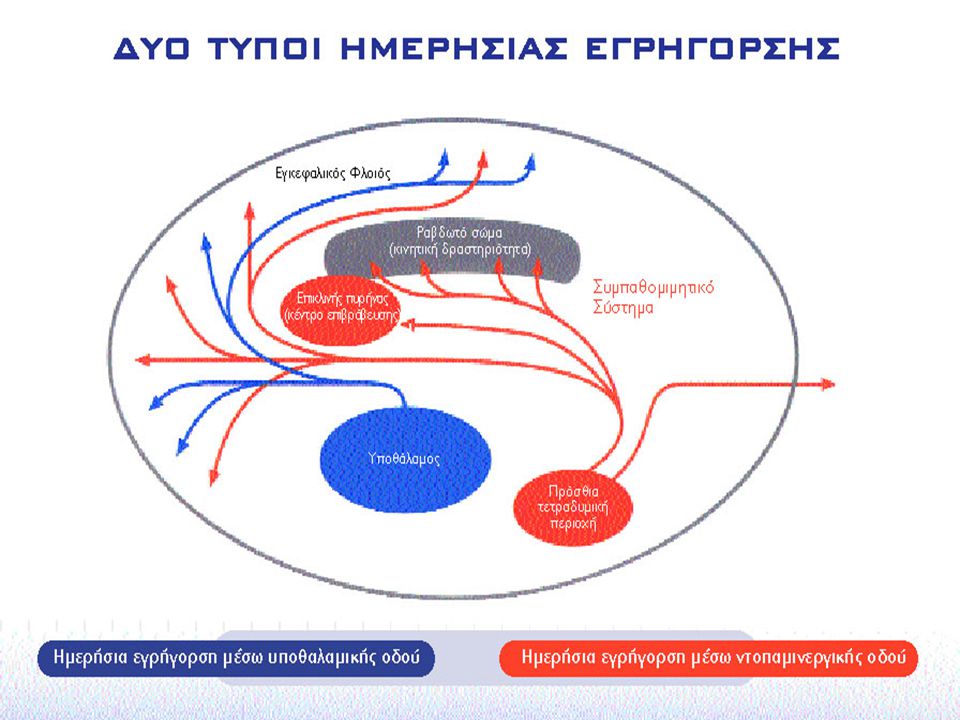
Φαρμακολογία Τα διεγερτικά του ΚΝΣ αυξάνουν την απελευθέρωση και μπλοκάρουν την αντλία επαναπρόσληψης ντοπαμίνης Δράση: στον εγκεφαλικό φλοιό στα ντοπαμινεργικά μονοπάτια όπως τον επικλινή πυρήνα (κέντρο επιβράβευσης) και στο ραβδωτό σώμα (κινητική δραστηριότητα)
 και στο ραβδωτό σώμα (κινητική δραστηριότητα)")
46
Ευγρηγορικά φάρμακα- Μοδαφιλίνη
Modafinil: A Pack et al Am J Respir Crit Care Med 2001;164: Kingshott R et al Am J Respir Crit Care Med 2001;163:918-23 Schwartz JRL et al Chest 2003;124: Black JE et al Sleep 2005;28(4):464-71 Hirshkowitz M et al CNS Drugs 2007;21(5):407-16 Armodafinil: Roth T et al Clin Ther 2006;28(5): Roth T et al Sleep Breath 2007; Sep 15 Hirshkowitz M et al Respiratory Medicine 2007;101:616-27 Use: in pts with OSA/HS who ahere to nCPAP therapeutic use prescription, properly titrated to an effective pressure, maintain adequate sleep schedule
: Hirshkowitz M et al CNS Drugs 2007;21(5): Armodafinil: Roth T et al Clin Ther 2006;28(5): Roth T et al Sleep Breath 2007; Sep 15. Hirshkowitz M et al Respiratory Medicine 2007;101: Use: in pts with OSA/HS who ahere to nCPAP therapeutic use prescription, properly titrated to an effective pressure, maintain adequate sleep schedule.")
48
Μηχανισμός δράσης Moδαφινίλης (ΙΙ)
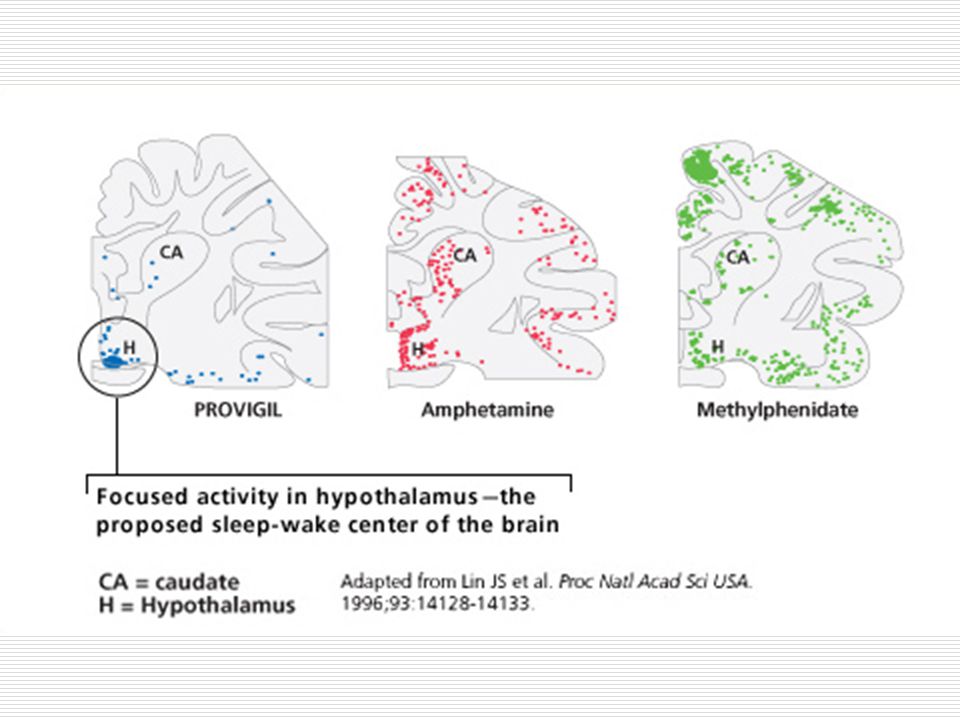
Η μοδαφινίλη όπως φαίνεται από μελέτες που χρησιμοποιούν την τεχνική της c-Fos ανοσοϊστοχημείας: αυξάνει την δραστηριότητα του φυματοθυλοειδή πυρήνα (κέντρο εγρήγορσης) ο οποίος και προεκτείνεται ως τον εγκεφαλικό φλοιό επιτυγχάνοντας εγρήγορση μειώνει την δραστηριότητα της προσθιοπλάγιας προ-οπτικής περιοχής (κέντρο ύπνου) Ishizuka 339 (2003)
 ο οποίος και προεκτείνεται ως τον εγκεφαλικό φλοιό επιτυγχάνοντας εγρήγορση. μειώνει την δραστηριότητα της προσθιοπλάγιας προ-οπτικής περιοχής (κέντρο ύπνου) Ishizuka 339 (2003)")
49
Φαρμακολογικές δράσεις Μοδαφινίλης, μεθυλφαινιδάτης και αμφεταμίνης
Modafinil Methylphenidate Amphetamine Εγρήγορση ↑↑ Κινητική δραστηριότητα 0/↑ Αγχώδης διαταραχή Αρτηριακή πίεση/καρδιακή συχνότητα ↑ ΝREM ύπνος από ανάδραση Ο ακριβής μηχανισμός δράσης του Modiodal δεν είναι γνωστός 0 δεν έχει επίδραση 0/↑ μικρή επίδραση ↑ μέτρια δράση ↑ ↑ εμφανή αύξηση

50
Ενδείξεις μοδαφινίλης
PROVIGIL PI, p. 12, ¶ 1-3. Ναρκοληψία συνοδευόμενη ή όχι με καταπληξία. Υπολειμματική υπνηλία σε έδαφος ΣΑΥΥ υπό θεραπεία με CPAP και της μέτριας έως σοβαρής χρόνιας διαταραχής του ύπνου σχετιζόμενης με εναλλασσόμενα ωράρια εργασίας (SWSD)
")
51
Υπολειμματική υπνηλία σε ασθενείς με ΣΑΥΥ υπό θεραπεία με CPAP : χορήγηση Modafinil
Kingshott AJRCCM 2001 15 11 Pack AJRCCM 2001 Schwartz Chest 2003

52
Υπολειμματική υπνηλία σε ασθενείς με ΣΑΥΥ υπό θεραπεία με CPAP : χορήγηση Modafinil
Black Sleep 2005

53
Υπολειμματική υπνηλία σε ασθενείς με ΣΑΥΥ υπό θεραπεία με CPAP : χορήγηση Modafinil
Kingshott AJRCCM 2001 Black Sleep 2005

54
Υπολειμματική υπνηλία σε ασθενείς με ΣΑΥΥ υπό θεραπεία με CPAP : χορήγηση Modafinil
Black Sleep 2005

55
Υπολειμματική υπνηλία σε ασθενείς με ΣΑΥΥ υπό θεραπεία με CPAP : Modafinil, χρήση CPAP
During 4 wk of treatment, the mean time of CPAP use was 6.2 h per night in each group, with no significant change from baseline between the two groups and no significant change from baseline to Week 4 within each group Pack AJRCCM 2001 Kingshott AJRCCM 2001

56
* * * * *p <0.001 Μεταβολή από την γραμμή αναφοράς n=230 n=235
Schwartz; Presented at the 100th International conference of the American Thoracic Society, May 2004, Orlando, FL

57
Ανεπιθύμητες ενέργειες
PROVIGIL PI, p. 29, Table 3. Ναρκοληψία, OSAHS, and SWSD Studies Ανεπιθύμητες ενέργειες Μοδαφινίλη (%) (n=934) Placebo (%) (n=567) Κεφαλαλγία 34 23 Ναυτία 11 3 Ανησυχία 7 Ρινίτιδα 6 Back Pain 5 Διάρροια Άγχος 1 Ίλιγγος 4 Δυσπεψία Αυπνία
 (n=934) Placebo (%) (n=567) Κεφαλαλγία Ναυτία Ανησυχία. 7. Ρινίτιδα. 6. Back Pain. 5. Διάρροια. Άγχος. 1. Ίλιγγος. 4. Δυσπεψία. Αυπνία.")
58
Αλληλεπιδράσεις με άλλα φάρμακα
Η μοδαφινίλη ίσως να αλληλεπιδρά με φάρμακα που αναστέλλουν, επάγουν ή μεταβολίζονται από τα ισοένζυμα του κυτοχρώματος P450 Η αποτελεσματικότητα στεροειδών αντισυλληπτικών ίσως μειώνεται κατά τη διάρκεια χρήσης μοδαφινίλης αλλά και ένα μήνα μετά τη διακοπή της θεραπείας

59
Υπέρ-Κατά της χρήσης Μοδαφινίλης στο ΣΑΥ
Black J. Pro: Modafinil has a role in management of sleep apnea. Am J Respir Crit Care Med 2003;167: Pollack CP. Con: Modafinil has no role in management of sleep apnea. Am J Respir Crit Care Med 2003;167:

60
Πραγματικές ή όχι οι αντιθέσεις;
Black J. Stanford University (response): Σαφώς τίθεται θέμα χρήσης CPAP. Λύση: κατανόηση νοσήματος και επιπτώσεων, εξήγηση αναγκαιότητας εφαρμογής θεραπείας του ΣΑΥ, συνεπής παρακολούθηση θεραπείας και λύση προβλημάτων που προέρχονται από εφαρμογή της Σε υπολειμματική υπνηλία η συγχορήγηση Μοδαφινίλης δε φαίνεται να μειώνει χρήση CPAP Pack AI et all Am J Respir Crit Care Med 2001 Black JE et al Sleep 2002 Schwartz JRL et al Chest 2003 Απαιτείται συνεπής και συνεχής παρακολούθηση ασθενούς
: Σαφώς τίθεται θέμα χρήσης CPAP. Λύση: κατανόηση νοσήματος και επιπτώσεων, εξήγηση αναγκαιότητας εφαρμογής θεραπείας του ΣΑΥ, συνεπής παρακολούθηση θεραπείας και λύση προβλημάτων που προέρχονται από εφαρμογή της. Σε υπολειμματική υπνηλία η συγχορήγηση Μοδαφινίλης δε φαίνεται να μειώνει χρήση CPAP. Pack AI et all Am J Respir Crit Care Med Black JE et al Sleep Schwartz JRL et al Chest Απαιτείται συνεπής και συνεχής παρακολούθηση ασθενούς.")
61
Συμπεράσματα (I) Modafinil has a role in the treatment of residual sleepiness in patients with OSA: After the institution of proper primary upper airway management of sleep related obstruction As is always the case in medicine, judicious prescribing is imperative

62
Σύσταση Πρώτης επιλογής θεραπεία για την αντιμετώπιση της υπερβολικής ημερήσιας υπνηλίας και των ακατανίκητων επεισοδίων ύπνου αποτελεί η μοδαφινίλη mg/ημερησίως First-line pharmacological treatment of excessive daytime sleepiness and irresistible episodes of sleep should rely on modafinil, 100–400 mg/day, given in two doses, one in the morning and one early in the afternoon (level A).
.")
63
Διαταραχή του ύπνου λόγω εργασίας σε εναλλασσόμενα ωράρια (SWSD)
")
64
Διαγνωστικά κριτήρια: Διαταραχή του ύπνου λόγω εργασίας σε εναλλασσόμενα ωράρια (SWSD)(ICSD ) A primary complaint of insomnia or excessive sleepiness The primary complaint is temporally associated with a work period (usually night work) that occurs during the habitual sleep phase Evidence of disturbed chronobiological rhythmicity by demonstration of the loss of a normal sleep/wake pattern by polysomnography and by the MSLT SWSD is not the same as shift work. In fact is this study not all SR with SWSD were critical they had to complain of ES. Minimal Criteria: A+B MSLT = Multiple Sleep Latency Test; ICSD = International Classification of Sleep Disorders: Diagnostic and Coding Manual. Rochester, Minn.: American Sleep Disorders Association. 1990
 that occurs during the habitual sleep phase. Evidence of disturbed chronobiological rhythmicity by demonstration of the loss of a normal sleep/wake pattern by polysomnography and by the MSLT. SWSD is not the same as shift work. In fact is this study not all SR with SWSD were critical they had to complain of ES. Minimal Criteria: A+B. MSLT = Multiple Sleep Latency Test; ICSD = International Classification of Sleep Disorders: Diagnostic and Coding Manual. Rochester, Minn.: American Sleep Disorders Association")
65
Διαγνωστικά κριτήρια: Διαταραχή του ύπνου λόγω εργασίας σε εναλλασσόμενα ωράρια (SWSD)(ICSD ) D. Absence of a psychiatric or medical disorder that could account for the symptoms E. Does not meet criteria for any other sleep disorder producing insomnia or excessive sleepiness SWSD is not the same as shift work. In fact is this study not all SR with SWSD were critical they had to complain of ES. ICSD = International Classification of Sleep Disorders: Diagnostic and Coding Manual. Rochester, Minn.: American Sleep Disorders Association. 1990

66
Διαταραχή του ύπνου λόγω εργασίας σε εναλλασσόμενα ωράρια- επιπολασμός
Υπολογίζεται πως περίπου 15 εκατομμύρια εργαζόμενοι στις ΗΠΑ δουλεύουν σε εναλλασσόμενα ωράρια1 15% των εργαζομένων με πλήρες ωράριο εργάζονται σε βάρδιες1 Περίπου το 15% με 25% των ατόμων που δουλεύουν νυχτερινό ωράριο πάσχουν από SWSD2,3 Συχνό νόσημα αλλά υποδιαγνωσμένο!!!!!! 1. US Dept of Labor. Bureau of Labor Statistics. Workers on flexible and shift schedules. May Available at: Accessed March 23, 2007. 2. Drake CL, et al. Sleep. 2004;27: 3. Ohayon MM, et al. J Psychosom Res. 2002;53:

67
Διαταραχή του ύπνου λόγω εργασίας σε εναλλασσόμενα ωράρια-Συμπτώματα
Η υπνηλία είναι κυρίαρχο σύμπτωμα της SWSD Συμπεριλαμβάνονται επίσης τα ακόλουθα συμπτώματα: Αυπνία Μειωμένη διάρκεια ύπνου και κακή ποιότητα ύπνου Μειωμένη εγρήγορση και διαταραγμένη συγκέντρωση Μειωμένη απόδοση Ευερεθιστότητα και καταθλιπτική διάθεση The International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.

68
Πιθανές συνέπειες σχετιζόμενες με SWSD
Drake, p. 1458, Table 3. 35 * * Νύχτα - χωρίς SWSD Νύχτα - SWSD 30 Εναλλασσόμενα - χωρίς SWSD Εναλλασσόμενα - SWSD Ημέρα – χωρίς συμπτώματα Ημέρα – χωρίς συμπτώματα 25 20 Respondents (%) * 15 * 10 5 έλκος Καρδιαγγειακές διαταραχές κατάθλιψη Excluded individuals who were: evening shift workers, not working, retired, or unemployed. N=2,449. Day – Symptoms = day workers with symptoms of ES or insomnia; SWSD = shift work sleep disorder. *P<0.05 for those individuals who met criteria for SWSD vs those who did not. Drake CL, et al. Sleep. 2004;27:
 * 15. * έλκος. Καρδιαγγειακές διαταραχές. κατάθλιψη. Excluded individuals who were: evening shift workers, not working, retired, or unemployed. N=2,449. Day – Symptoms = day workers with symptoms of ES or insomnia; SWSD = shift work sleep disorder. *P<0.05 for those individuals who met criteria for SWSD vs those who did not. Drake CL, et al. Sleep. 2004;27:")
69
SWSD: Missed Work During the Past 3 Months
Day Shift Night Shift Rotating Shift 10 p<0.05 8 6 Days 4 Sleep Dec 15;27(8): Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Henry Ford Hospital Sleep Disorders and Research Center, Detroit, MI 48202, USA. STUDY OBJECTIVES: Although there are considerable data demonstrating the impact of shift work on sleep and alertness, little research has examined the prevalence and consequences of shift work sleep disorder in comparison to the difficulties with insomnia and excessive sleepiness experienced by day workers. The present study was designed to determine the relative prevalence and negative consequences associated with shift work sleep disorder in a representative sample drawn from the working population of metropolitan Detroit. DESIGN: Random-digit dialing techniques were used to assess individuals regarding their current work schedules and a variety of sleep- and non-sleep-related outcomes. SETTING: Detroit tricounty population. PARTICIPANTS: A total of 2,570 individuals aged 18 to 65 years from a representative community-based sample including 360 people working rotating shifts, 174 people working nights, and 2036 working days. MEASUREMENTS AND RESULTS: Using standardized techniques, individuals were assessed for the presence of insomnia and excessive sleepiness, based on DSM-IV and ICSD criteria. Those individuals with either insomnia or excessive sleepiness and who were currently working rotating or night schedules were classified as having shift work sleep disorder. Occupational, behavioral, and health-related outcomes were also measured. Individuals who met criteria for shift work sleep disorder had significantly higher rates of ulcers (odds ratio = 4.18, 95% confidence interval = ), sleepiness-related accidents, absenteeism, depression, and missed family and social activities more frequently compared to those shift workers who did not meet criteria (P < .05). Importantly, in most cases, the morbidity associated with shift work sleep disorder was significantly greater than that experienced by day workers with identical symptoms. CONCLUSION: These findings suggest that individuals with shift work sleep disorder are at risk for significant behavioral and health-related morbidity associated with their sleep-wake symptomatology. Further, it suggests that the prevalence of shift work sleep disorder is approximately 10% of the night and rotating shift work population. PMID: [PubMed - indexed for MEDLINE] 2 No Insomnia, No Insomnia, Yes Insomnia, Yes Insomnia, No ES Yes ES No ES Yes ES *The relationship is an association, not causality; Drake CL et al. (2004), Sleep 27(8):
: Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Henry Ford Hospital Sleep Disorders and Research Center, Detroit, MI 48202, USA. STUDY OBJECTIVES: Although there are considerable data demonstrating the impact of shift work on sleep and alertness, little research has examined the prevalence and consequences of shift work sleep disorder in comparison to the difficulties with insomnia and excessive sleepiness experienced by day workers. The present study was designed to determine the relative prevalence and negative consequences associated with shift work sleep disorder in a representative sample drawn from the working population of metropolitan Detroit. DESIGN: Random-digit dialing techniques were used to assess individuals regarding their current work schedules and a variety of sleep- and non-sleep-related outcomes. SETTING: Detroit tricounty population. PARTICIPANTS: A total of 2,570 individuals aged 18 to 65 years from a representative community-based sample including 360 people working rotating shifts, 174 people working nights, and 2036 working days. MEASUREMENTS AND RESULTS: Using standardized techniques, individuals were assessed for the presence of insomnia and excessive sleepiness, based on DSM-IV and ICSD criteria. Those individuals with either insomnia or excessive sleepiness and who were currently working rotating or night schedules were classified as having shift work sleep disorder. Occupational, behavioral, and health-related outcomes were also measured. Individuals who met criteria for shift work sleep disorder had significantly higher rates of ulcers (odds ratio = 4.18, 95% confidence interval = ), sleepiness-related accidents, absenteeism, depression, and missed family and social activities more frequently compared to those shift workers who did not meet criteria (P < .05). Importantly, in most cases, the morbidity associated with shift work sleep disorder was significantly greater than that experienced by day workers with identical symptoms. CONCLUSION: These findings suggest that individuals with shift work sleep disorder are at risk for significant behavioral and health-related morbidity associated with their sleep-wake symptomatology. Further, it suggests that the prevalence of shift work sleep disorder is approximately 10% of the night and rotating shift work population. PMID: [PubMed - indexed for MEDLINE] 2. No Insomnia, No Insomnia, Yes Insomnia, Yes Insomnia, No ES. Yes ES. No ES. Yes ES. *The relationship is an association, not causality; Drake CL et al. (2004), Sleep 27(8):")
70
SWSD: Missed Family and Social Activities During the Past 3 Months
Insomnia and/or ES No Insomnia or ES 12 * 10 * 8 Days 6 4 Sleep Dec 15;27(8): Related Articles, Links Comment in: Sleep Jan 1;28(1):9-11. Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Henry Ford Hospital Sleep Disorders and Research Center, Detroit, MI 48202, USA. STUDY OBJECTIVES: Although there are considerable data demonstrating the impact of shift work on sleep and alertness, little research has examined the prevalence and consequences of shift work sleep disorder in comparison to the difficulties with insomnia and excessive sleepiness experienced by day workers. The present study was designed to determine the relative prevalence and negative consequences associated with shift work sleep disorder in a representative sample drawn from the working population of metropolitan Detroit. DESIGN: Random-digit dialing techniques were used to assess individuals regarding their current work schedules and a variety of sleep- and non-sleep-related outcomes. SETTING: Detroit tricounty population. PARTICIPANTS: A total of 2,570 individuals aged 18 to 65 years from a representative community-based sample including 360 people working rotating shifts, 174 people working nights, and 2036 working days. MEASUREMENTS AND RESULTS: Using standardized techniques, individuals were assessed for the presence of insomnia and excessive sleepiness, based on DSM-IV and ICSD criteria. Those individuals with either insomnia or excessive sleepiness and who were currently working rotating or night schedules were classified as having shift work sleep disorder. Occupational, behavioral, and health-related outcomes were also measured. Individuals who met criteria for shift work sleep disorder had significantly higher rates of ulcers (odds ratio = 4.18, 95% confidence interval = ), sleepiness-related accidents, absenteeism, depression, and missed family and social activities more frequently compared to those shift workers who did not meet criteria (P < .05). Importantly, in most cases, the morbidity associated with shift work sleep disorder was significantly greater than that experienced by day workers with identical symptoms. CONCLUSION: These findings suggest that individuals with shift work sleep disorder are at risk for significant behavioral and health-related morbidity associated with their sleep-wake symptomatology. Further, it suggests that the prevalence of shift work sleep disorder is approximately 10% of the night and rotating shift work population. PMID: [PubMed - indexed for MEDLINE] 2 Day Shift Night Shift Rotating Shift *p<0.05 vs. day shift; The relationship is an association, not causality; Drake CL et al. (2004), Sleep 27(8):
: Related Articles, Links. Comment in: Sleep Jan 1;28(1):9-11. Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Henry Ford Hospital Sleep Disorders and Research Center, Detroit, MI 48202, USA. STUDY OBJECTIVES: Although there are considerable data demonstrating the impact of shift work on sleep and alertness, little research has examined the prevalence and consequences of shift work sleep disorder in comparison to the difficulties with insomnia and excessive sleepiness experienced by day workers. The present study was designed to determine the relative prevalence and negative consequences associated with shift work sleep disorder in a representative sample drawn from the working population of metropolitan Detroit. DESIGN: Random-digit dialing techniques were used to assess individuals regarding their current work schedules and a variety of sleep- and non-sleep-related outcomes. SETTING: Detroit tricounty population. PARTICIPANTS: A total of 2,570 individuals aged 18 to 65 years from a representative community-based sample including 360 people working rotating shifts, 174 people working nights, and 2036 working days. MEASUREMENTS AND RESULTS: Using standardized techniques, individuals were assessed for the presence of insomnia and excessive sleepiness, based on DSM-IV and ICSD criteria. Those individuals with either insomnia or excessive sleepiness and who were currently working rotating or night schedules were classified as having shift work sleep disorder. Occupational, behavioral, and health-related outcomes were also measured. Individuals who met criteria for shift work sleep disorder had significantly higher rates of ulcers (odds ratio = 4.18, 95% confidence interval = ), sleepiness-related accidents, absenteeism, depression, and missed family and social activities more frequently compared to those shift workers who did not meet criteria (P < .05). Importantly, in most cases, the morbidity associated with shift work sleep disorder was significantly greater than that experienced by day workers with identical symptoms. CONCLUSION: These findings suggest that individuals with shift work sleep disorder are at risk for significant behavioral and health-related morbidity associated with their sleep-wake symptomatology. Further, it suggests that the prevalence of shift work sleep disorder is approximately 10% of the night and rotating shift work population. PMID: [PubMed - indexed for MEDLINE] 2. Day Shift. Night Shift. Rotating Shift. *p<0.05 vs. day shift; The relationship is an association, not causality; Drake CL et al. (2004), Sleep 27(8):")
71
Διαταραχή του ύπνου λόγω εργασίας σε εναλλασσόμενα ωράρια-θεραπεία
Βελτίωση υγιεινής του ύπνου Βέλτιστο περιβάλλον για ύπνο Αποφυγή καφεΐνης και αλκοόλ Φωτοθεραπεία Καθορισμένος και προγραμματισμένος χρόνος ύπνου Άσκηση Φαρμακευτική θεραπεία Kryger MH, et al. Principles and Practices of Sleep Medicine. Philadelphia: WB Saunders; 2005.

72
U.S. Modafinil Shift Work Sleep Disorders Study Group
Shift-Work Sleep Disorder (SWSD) Treatment: Modafinil 200 mg of modafinil or placebo before the start of each shift U.S. Modafinil Shift Work Sleep Disorders Study Group N Engl J Med 2005;353:476-86
 Treatment: Modafinil. 200 mg of modafinil or placebo before the start of each shift. U.S. Modafinil Shift Work Sleep Disorders Study Group. N Engl J Med 2005;353:")
73
SWSD were extremely sleepy
Shift-Work Sleep Disorder (SWSD) Treatment: Modafinil 1 (very alert) to 9 (very sleepy) Improvement on CGI-C was seen in 74% of patients with modafinil compared with 36% with placebo (p < 0.001). SWSD were extremely sleepy 7.3±0.1 Vs 5.8±0.2 (P<0.001) U.S. Modafinil Shift Work Sleep Disorders Study Group N Engl J Med 2005;353:476-86
 Treatment: Modafinil. 1 (very alert) to 9 (very sleepy) Improvement on CGI-C was seen in 74% of patients with modafinil compared with 36% with placebo (p < 0.001). SWSD were extremely sleepy. 7.3±0.1 Vs 5.8±0.2. (P<0.001) U.S. Modafinil Shift Work Sleep Disorders Study Group N Engl J Med 2005;353:")
74
Shift-Work Sleep Disorder (SWSD)
Treatment: Modafinil Sleep latency during laboratory night shifts Shift work sleep disorder had excessive sleepiness during night work, similar to that seen during the day in patients with narcolepsy SOLs were significantly greater with modafinil than with placebo at 2:00am (p = 0.02) and 4:00am (p < 0.001), but not at 6:00am or 8:00am Czeisler CA N Engl J Med 2005;353:476-86
 and 4:00am (p < 0.001), but not at 6:00am or 8:00am. Czeisler CA N Engl J Med 2005;353:")
75
Shift-Work Sleep Disorder (SWSD) Treatment: Modafinil
Fewer patients had accidents or near accidents on the commute home (54% with placebo vs 29% with modafinil; p < 0.001) Significant reduction of attention lapses U.S. Modafinil Shift Work Sleep Disorders Study Group N Engl J Med 2005;353:476-86
 Significant reduction of attention lapses. U.S. Modafinil Shift Work Sleep Disorders Study Group. N Engl J Med 2005;353:")
76
Shift-Work Sleep Disorder (SWSD) Treatment: Modafinil 12 weeks
U.S. Modafinil Shift Work Sleep Disorders Study Group Prim Care Companion J Clin Psychiatry 2007;9:188–194

77
Shift-Work Sleep Disorder (SWSD) Treatment: Modafinil 12 weeks
U.S. Modafinil Shift Work Sleep Disorders Study Group Prim Care Companion J Clin Psychiatry 2007;9:188–194

78
Συμπερασματικά Η μοδαφινίλη φαίνεται να είναι ασφαλής και αποτελεσματική Δοσολογία???? ( mg) Τρόπος χορήγησης???? Εφάπαξ? Δις ημερησίως? Ανάλογα με το νόσημα? Εξατομικευμένο σχήμα??? Τρόποι αξιολόγησης??? (μέθοδος, διάρκεια)
")
79
Thank you Medical School, University of Crete 79

Παρόμοιες παρουσιάσεις
 5 1 ( ) ( ) ( /cm 2 ) 0.2 /30min·φ90 (5 /m 3 ) 0.4 /30min·φ90 (10 /m 3 ) 5 100 1000 0.75 /30min·φ90 (25 /m 3 )>")









>")






: - Υπνος.>")

