Κατέβασμα παρουσίασης
Η παρουσίαση φορτώνεται. Παρακαλείστε να περιμένετε

1
ΟΣΤΕΟΑΡΘΡΙΤΙΔΑ

2
Επιδημιολογία Η οστεοαρθρίτιδα είναι η πιο συχνή αρθρίτιδας.
Ακτινολογικά ευρήματα οστεοαρθρίτιδας είναι ορατά στην πλειοψηφία των ατόμων ηλικίας μεγαλύτερης των 75 (80%) Περίπου το 11% ατόμων με ΟΑ ηλικίας μεγαλύτερης των 65 έχουν συμπτώματα
 Περίπου το 11% ατόμων με ΟΑ ηλικίας μεγαλύτερης των 65 έχουν συμπτώματα.")
3
Ορισμός της οστεοαρθρίτιδας
“Osteoarthritis (OA) is a degenerative joint disease, occurring primarily in older persons, characterized by erosion of the articular cartilage, hypertrophy of bone at the margins (i.e., osteophytes), subchondral sclerosis, and a range of biochemical and morphologic alterations of the synovial membrane and joint capsule. Harris: Kelley's Textbook of Rheumatology, 7th ed.
 is a degenerative joint disease, occurring primarily in older persons, characterized by erosion of the articular cartilage, hypertrophy of bone at the margins (i.e., osteophytes), subchondral sclerosis, and a range of biochemical and morphologic alterations of the synovial membrane and joint capsule. Harris: Kelley s Textbook of Rheumatology, 7th ed.")
4
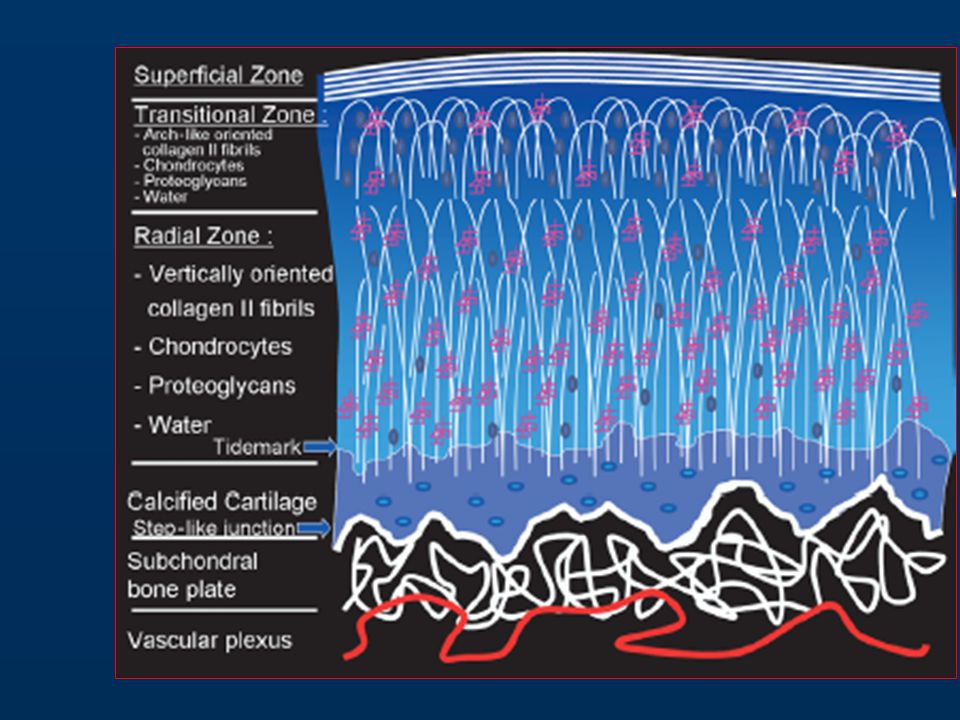
Υαλοειδής χόνδρος Ιστός που είναι σχεδιασμένος να αντιστέκεται στα φορτία και να διανέμει επίσης τα φορτία Χαμηλή μεταβολική δραστηριότητα, μειωμένη αιμέτωση, χωρίς λεμφαγγεία και νεύρωση και μειωμένη αναγενητική ικανότητα

5
ΧΟΝΔΡΟΣ Κύτταρα Εξωκυττάρια ουσία Σήματα (Signals)
")
6
ΕΞΩΚΥΤΤΑΡΙΑ ΟΥΣΙΑ Κολλαγόνο Πρωτεογλυκάνες Γλυκοπρωτείνες

7
ΤΥΠΟΙ ΚΟΛΛΑΓΟΝΟΥ Type II 95% Type IX 3% Type X 1% Type XI 1%

8
Υαλοειδής χόνδρος Core Protein-Aggrecan Hyaluronic Acid
Link Glycoprotein Chondroitin Sulfate Chain

9
SIGNALS Morphogens & Growth Factors
BMPs CDMPs FGFs IGFs IHH PTHrp WNTs

11
Αίτια πόνου Ο χόνδρος δεν περιέχει νεύρα, έτσι ο πόνος προέρχεται από:
Υποχόνδριο οστούν: μικροκατάγματα, αύξηση ενδοοστικής πίεσης Οστεόφυτα: ερεθισμός των νευρικών απολήξεων του περιοστέου Σύνδεσμοι: αυξημένη τάση Αρθρικός θύλακος: φλεγμονή Αρθρικός υμένας: φλεγμονή Περιαρθρικοί μύες: σπασμός

12
Αίτια αρθρίτιδας Ασύμμετρη φόρτιση Βιοχημικά αίτια Cytokine activation

13
Παράγοντες αυξημένου κινδύνου
Ηλικία Παχυσαρκία Επάγγελμα Αθλητικές δραστηριότητες Προηγηθείσα κάκωση Μυϊκή αδυναμία Ιδιοδεκτικότητα Εναπόθεση ασβεστίου (ψευδοουρική αρθρίτις) Up-To-Date 2005 Risk Factors for and Possible Causes of Osteoarthritis
 Up-To-Date 2005 Risk Factors for and Possible Causes of Osteoarthritis.")
14
Κλινική Εικόνα Συμπτώματα: πόνος (ηρεμίας), δυσκαμψία, κριγμός, λειτουργικά προβλήματα. Κλινικά σημεία: χωλότητα, παραμόρφωση, μυϊκή ατροφία, ύδραρθρος, κριγμός, οίδημα μαλακών μορίων.

15
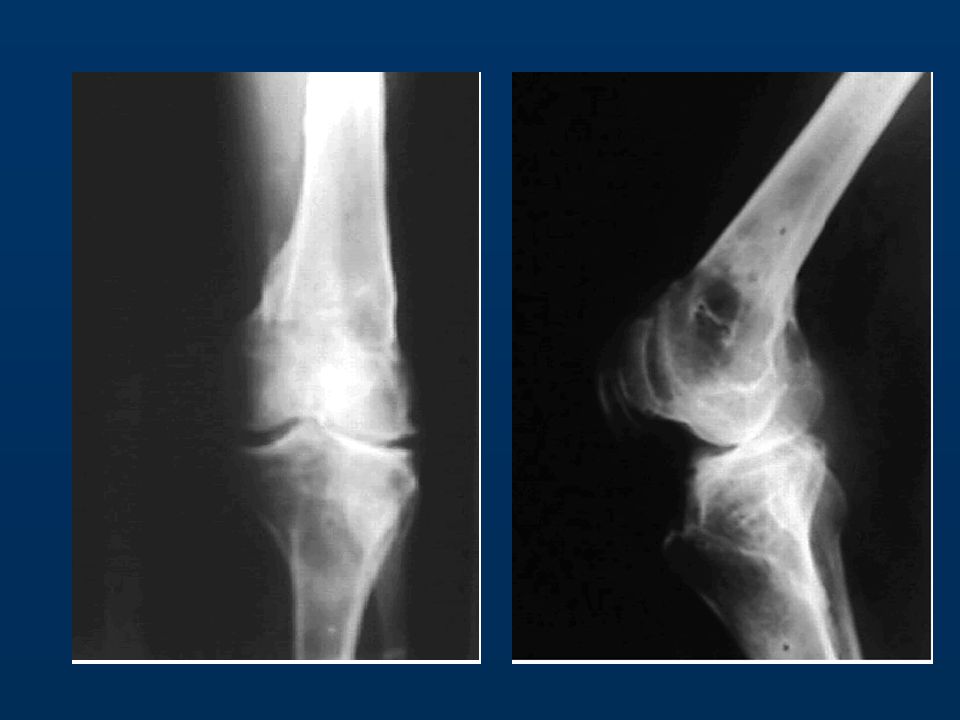
Ακτινολογική Απεικόνιση
Ακτινολογικά κριτήρια: Στένωση μεσαρθρίου Υποχόνδριες κύστεις Οστεόφυτα Οστεοπενία

16
Ακτινολογική Απεικόνιση
Kellgren and Lawrence grading system of OA of the knee. Grades: 0 (none), 1 (doubtful) 2 (minimal) 3 (moderate) 4 (severe)
, 1 (doubtful) 2 (minimal) 3 (moderate) 4 (severe)")
17
Απόκλιση του άξονα οδηγεί σε υπέρμετρη φόρτιση του ενός διαμερίσματος

18
Σκλήρυνση του υποχόνδριου οστού

19
Στένωση του μεσάρθριου διαστήματος

20
Σχηματισμός οστεοφύτων

21
Υπεξάρθρημα – Αποδιοργάνωση της άρθρωσης

22
Functional Classification System
International Classification of Functioning, Disability and Health Category 1: Mild Osteoarthritis Modest discomfort, with little or no difficulty with quality of life Category 2: Moderate Osteoarthritis Significant pain and discomfort, with impairment in normal activities or participation in aspects of life important to that individual. Category 3: Moderate with other Health Problems Same as above, combined with significant medical co-morbidities. Category 4: Severe Osteoarthritis Pain with sleep and of such severity to prevent many activities of daily living.

23
Current Guidelines American College of Rheumatology
American Academy of Orthopedic Surgery European League Against Rheumatism

24
American Academy of Orthopedic Surgery
chart_oakn.pdf Osteoarthritis of the Knee A Compendium of Evidence-based Information and Resources

25
European League Against Rheumatism
1 Treatment of knee OA* should be tailored to the individual patient, taking into account factors such as age, comorbidity, and the presence of inflammation 2 Optimal management of knee OA requires a combination of pharmacological and non-pharmacological treatment modalities 3 Intra-articular injection of long acting steroid is indicated for acute exacerbation of knee pain, especially if accompanied by effusion 4 There is evidence that SYSADOA* (glucosamine sulphate, chondroitin sulphate, diacerein, and hyaluronic acid) may possess structure modification properties, but more studies, using standardised methodology are required 5 Hyaluronic acid and other SYSADOA are probably effective in knee OA, but the size effect is relatively small, suitable patients are not well defined, and pharmacoeconomic aspects of that treatment are not well established 6 Non-pharmacological treatment of knee OA should include regular education, exercise, appliances (sticks, insoles), and weight reduction 7 Exercises, especially those directed towards increasing strength of quadriceps and/or preserving normal mobility of the knee are strongly recommended 8 Paracetamol is the oral analgesic to try first and, if successful, is the preferred long term oral analgesic 9 NSAIDs* (oral or topical) should be considered in patients (with effusion) unresponsive to paracetamol 10 Joint replacement has to be considered for refractory pain associated with disability and radiological deterioration * OA = osteoarthritis; NSAIDs = non-steroidal anti-inflammatory drugs; SYSADOA = symptomatic slow acting drugs for osteoarthritis.
 may possess structure modification properties, but more studies, using standardised methodology are required. 5. Hyaluronic acid and other SYSADOA are probably effective in knee OA, but the size effect is relatively small, suitable patients are not well defined, and pharmacoeconomic aspects of that treatment are not well established. 6. Non-pharmacological treatment of knee OA should include regular education, exercise, appliances (sticks, insoles), and weight reduction. 7. Exercises, especially those directed towards increasing strength of quadriceps and/or preserving normal mobility of the knee are strongly recommended. 8. Paracetamol is the oral analgesic to try first and, if successful, is the preferred long term oral analgesic. 9. NSAIDs* (oral or topical) should be considered in patients (with effusion) unresponsive to paracetamol. 10. Joint replacement has to be considered for refractory pain associated with disability and radiological deterioration. * OA = osteoarthritis; NSAIDs = non-steroidal anti-inflammatory drugs; SYSADOA = symptomatic slow acting drugs for osteoarthritis.")
26
Ερωτήματα Φαρμακευτικά βοηθήματα.
Μακροπρόθεσμη δράση αντιφλεγμονωδών φαρμάκων στο χόνδρο και στα οστά Αποτελεσματικότητα χειρουργικών επεμβάσεων. EULAR Recommendations

27
Διαγνωστικά Λάθη Αντανακλαστικός πόνος Άλλες μορφές αρθρίτιδας Άλλα
Ορογονοθυλακίτιδα «χηνείου ποδός» Νευροπάθεια Ριζίτιδα Άλλες μορφές αρθρίτιδας Ρευματοειδής Σηπτική Ουρική Άλλα Άσηπτη νέκρωση Όγκοι

28
Εξατομίκευση του ασθενούς
Λειτουργική ικανότητα WOMAC Pain Subscale Συνοδές παθήσεις Θυροειδής Παχυσαρκία Απαιτήσεις ασθενούς Επιλογή ασκήσεων Απώλεια βάρους Dr. St. Pierre Rule Osteoarthritis + Runner = Cyclist

29
Πόσο αποτελεσματική είναι η απώλεια σωματικού βάρους;

30
Μεγάλη ! Για μια γυναίκα κανονικού ύψους απώλεια βάρους 5kg μειώνει τον κίνδυνο ΟΑ 50%. Σημαντική απώλεια βάρους μπορεί να μειώσει τονν κίνδυνο OA κατά 33% σε γυναίκες και 20% άνδρες. Felson et al: Obesity and knee osteoarthritis. Annals of Internal Medicine 1998.

31
Αντιφλεγμονώδης αγωγή Βοηθά ή βλάπτει;
Αντιφλεγμονώδης αγωγή Βοηθά ή βλάπτει;

32
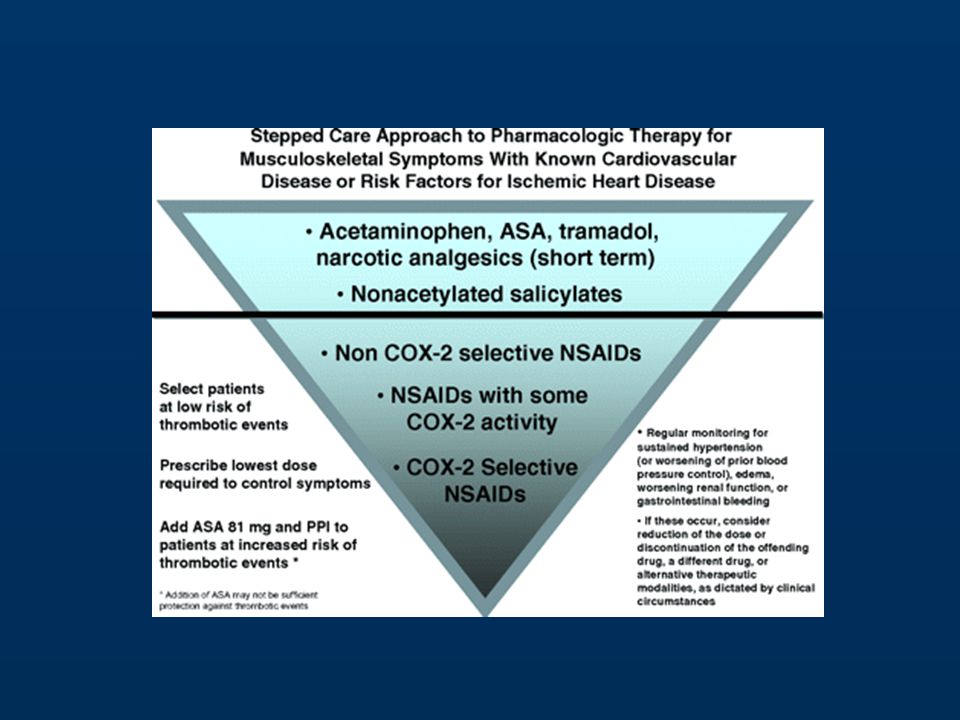
Φαρμακευτική αγωγή NSAIDs πιο αποτελεσματικά από ακεταμινοφαίνη
Coxibs για ασθενείς με προβλήματα γαστρεντερικού αλλά χωρίς καρδιαγγειακά προβλήματα Δεν υπάρχουν ενδείξεις καταστροφής ή προστασίας του χόνδρου από NSAIDs

34
Ενδαρθρικές εγχύσεις κορτιζόνης
1/10000 κίνδυνος σηπτικής αρθρίτιδας

35
Steroid Injections – The Evidence
The short-term benefit of IA corticosteroids in treatment of knee OA is well established, and few side effects have been reported. Longer term benefits have not been confirmed… “There is no clear objective evidence for intra-articular corticosteroid injections on the treatment of osteoarthritic or sports related injuries of the knee…” Snibbe, JC, Gambardella RA: Use of Injections for Osteoarthritis in Joints and Sports Activity. Clinics in Sports Medicine 24(2005);
;")
36
Κηδεμόνες - Ανυψωτικά υποδήματος
Αλλαγή φορτίων Δεν υπάρχει βιβλιογραφική υποστήριξη της χρήσης των.

37
Παράγοντες προστατευτικοί για το χόνδρο
hyaluronic acid Glucosamine

38
Glucosamine Sulfate How does it work?
Studies of radiolabeled glucoasmine do demonstrate uptake in the joint articular cartilage. Thought to stimulate chondrocytes to make proteoglycans. Thought to possibly inhibit cartilage catabolic enzymatic activity. Real mechanism of action is largely unknown.

39
Glucosamine Glucosamine sulfate setting, prevented joint structure changes in patients with knee OA, as assessed by radiographic joint space narrowing (JSN), with a significant improvement in pain and function limitation prevent TJR in an average follow-up of 5 years after drug discontinuation. Bruyere et al, Osteoarthritis and cartilage, 2007
, with a significant improvement in pain and function limitation. prevent TJR in an average follow-up of 5 years after drug discontinuation. Bruyere et al, Osteoarthritis and cartilage,")
40
Hyaluronic Acid No difference compared with steroids injections
Leopold et al, JBJS 2003

41
What’s the Role of Exercise as a Treatment? and as a Cause?

42
Does Exercise Cause Osteoarthritis?
Neuroanatomically normal joints are at increased risk of developing osteoarthritis in the absence of exercise. Neuroanatomically normal joints are not at increased risk of developing osteoarthritis upon exposure to repetitive, low impact, recreational exercise. Neuroanatomically abnormal joints are at increased risk of developing osteoarthritis upon exposure to repetitive, low impact, recreational exercise. Neuroanatomically normal joints are at increased risk of developing osteoarthritis upon exposure to repetitive, high impact.

43
Who needs to see an Orthopedic Surgeon, and When?

44
ARTHROSCOPY Classic Study: Mosely JB et al: A controlled trial of arthroscopic surgery for osteoarthritis of the knee. New England Journal of Medicine 2002. 180 pts randomly assigned to: Arthroscopic debridement Arthroscopic lavage Placebo surgery No significant benefit vs. placebo during 24 months of follow-up Most if not all of the effects of tidal irrigation can be attributed to the placebo effect

45
Ενδείξεις για αρθροσκόπηση
Συμπτωματική ΟΑ, που δεν ανταποκρίνεται σε αναλγητικά. Κλινικά ευρήματα: Ελεύθερα σώματα Μηχανικά συμπτώματα: κριγμός, αστάθεια.

46
Debridement - microfracture

47
ΜΟΝΟΔΙΑΜΕΡΙΣΜΑΤΙΚΗ ΑΡΘΡΙΤΙΔΑ
Οστεοτομία Μονοδιαμερισματική αρθροπλαστική Ολική αρθροπλαστική

48
ΕΝΔΕΙΞΕΙΣ Ιδεώδης ένδειξη για οστεοτομία κνήμης
ασθενής ηλικίας κάτω των 60 ετών με: ΟΑ έσω διαμερίσματος Συνδεσμικά σταθερό γόνατο Χωρίς σύγκαμψη Κάμψη > από 100ο Φυσιολογική επιγονατιδομηριαία Ραιβότητα < από 10ο

49
Η οστεοτομία της κνήμης απέκτησε δημοτικότητα από δημοσιεύσεις του Coventry το 1965
Coventry, M. B.: Stepped staple for upper tibial osteotomy. J.B.J.S., 51-A: 1011, July 1969.

50
Η πρώτη ανακοίνωση των αποτελεσμάτων της οστεοτομίας της κνήμης για αντιμετώπιση της μονοδιαμερισματικης οστεοαρθρίτιδας του γόνατος έγινε το 1962 από τους Jackson και Waugh J. Bone and Joint Surg., 1961

51
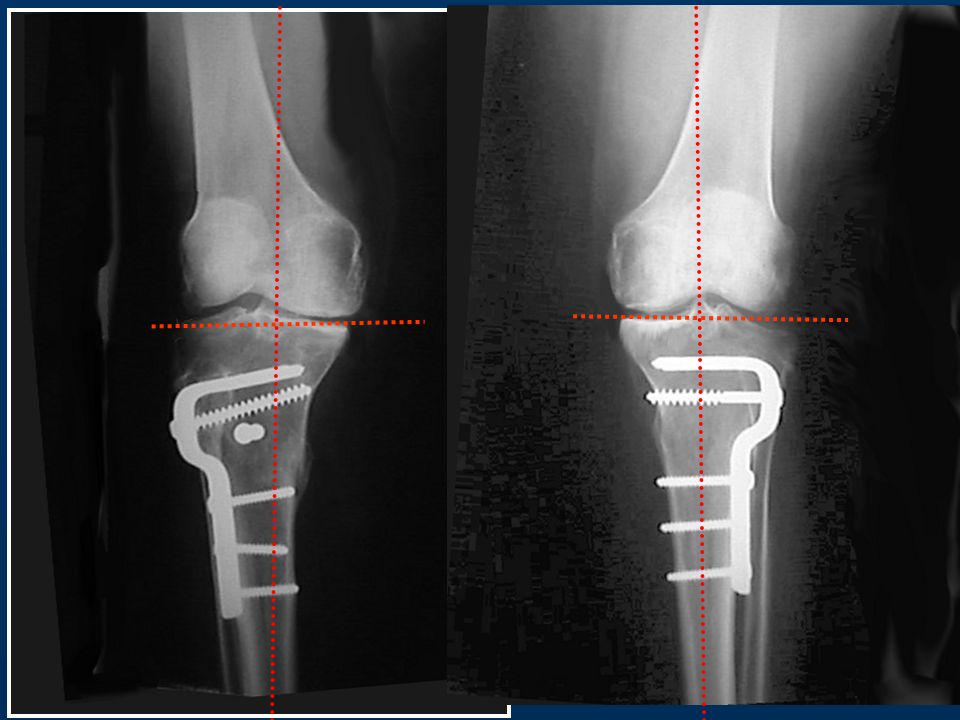
Μηχανικός Άξονας Υπάρχει 3 μοίρες απόκλιση του μηχανικού άξονα από το κάθετο επίπεδο

52
87ο 93ο

53
ΑΝΑΤΟΜΙΚΟΣ ΑΞΟΝΑΣ Μηρο-κνημιαία γωνία 175ο

55
9/10/00 9/10/00

56
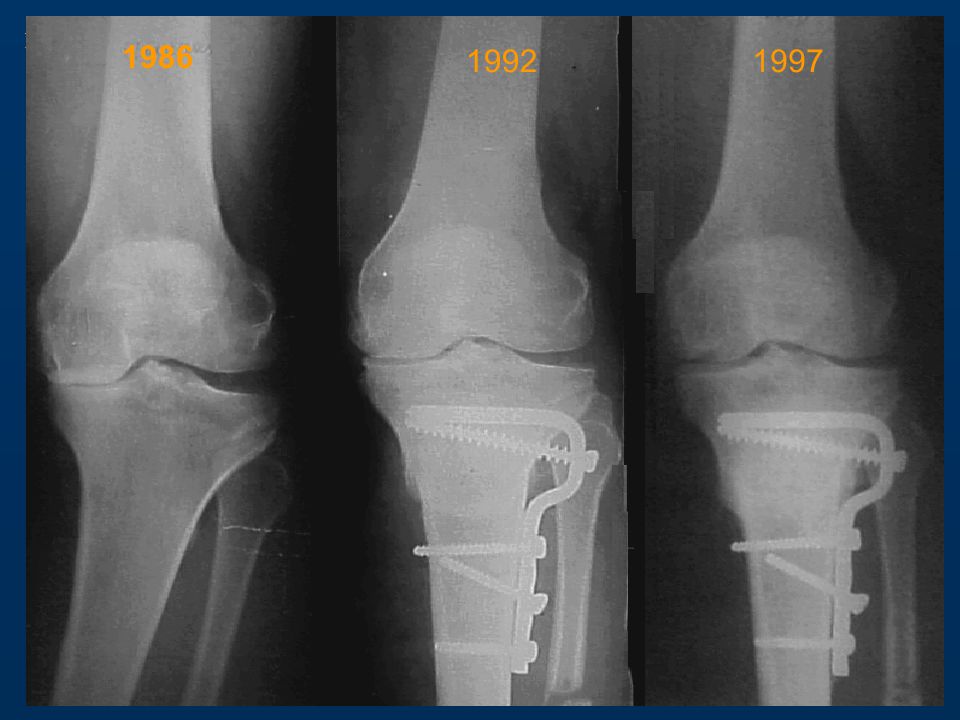
1986 1992 1997 1986 1992 1997
57
22O The patient 42 years old vas presented with severe osteoarthritis of hie lateral compartment of the right knee. 27o degrees of valgus deformity was mesured. Patelofemoral degenerated changes are also evident in the lateral view.

58
closing wedge 14o 87o The mechanical axis planing sugests that the correction of the axis and the reorientation of the knee joint can be obtaned partially by a closing supracodylar O/T, and partially by a closing high tibial O/T CLOSING WEDGE 8O

61
ΑΡΘΡΟΣΚΟΠΗΣΗ Υπάρχει ένδειξη ότι η αρθροσκόπηση σε συνδυασμό με οστεοτομία βελτιώνει το κλινικό αποτέλεσμα Akizuki S, Yasukawa Y, Takizawa T. Arthroscopy 1997;13:9-17

62
FUTURE TRENDS Human autologous culture expanded bone marrow mesenchymal cell transplantation for repair of cartilage defects in osteoarthritic knees. Wakitani S, Imoto K, Yamamoto T, Saito M, Murata N, Yoneda M. Osteoarthritis Cartilage 2002 Mar;10(3):
:")
63
Αλγόριθμος αντιμετώπισης ΟΑ πριν από αρθροπλαστική
Καλό ιστορικό και κλινική εξέταση. Ασκήσεις με προσεκτική παρακολούθηση. Επικουρική φαρμακευτική αγωγή. Χειρ/κη επέμβαση επί αποτυχίας συντηρητικής αγωγής.

Παρόμοιες παρουσιάσεις







>")













, Performance Indicators (PIs), Key Performance Indicators (KPIs)>")